
Abstract
Abstract
Background:
Researchers, using checklists, have identified that 30%–90% of patients make errors in inhaler use. It is not certain whether these errors affect the delivery of medication. We have developed an electronic monitor (INCA™) that records audio each time an inhaler is used, providing objective information on inhaler technique. The aim of this study was to assess the effect that correctly identified inhaler errors, with the INCA device, have on drug delivery.
Methods:
This was a prospective study of healthy volunteers using a salbutamol Diskus™. The inclusion criteria allowed for the recruitment of healthy participants who were nonfrequent users of Salbutamol. Each participant was assigned to one control “phase” first and two/three subsequent error “phases.” Each phase consisted of six doses of the drug taken 6 hours apart, and the participants' blood was drawn before and 25 minutes after doses one and six. This allowed us to sample their trough and peak serum salbutamol levels.
Results:
Fourteen healthy volunteers were studied. The inhaler technique errors simulated in this study included exhaling into the device after drug priming but before inhalation, low inspiratory flow, multiple inhalations, low breath hold, missed doses, and wrong inhaler position. Only the exhalation error, low inspiratory flow, and missed doses led to a significant reduction in serum salbutamol levels. After six doses of the exhalation error, there was a 62% reduction in peak salbutamol levels. Low inspiratory flow led to a 52% reduction in peak salbutamol levels and a 78% reduction in trough levels. Missed doses led to a 37% reduction in trough salbutamol levels.
Conclusions:
These findings confirm that technique errors affect drug delivery. Furthermore, we were able to identify that the most critical technique errors with the Diskus inhaler are exhalation into the device before inhalation, poor inspiratory flow, and missing doses.
Introduction
R
Poor adherence to inhaled medications is a problem with respiratory patients, and an estimated 30%–70% of asthmatic patients are nonadherent.(4) In addition, these inhaled therapies are administered through various inhaler devices and unlike the oral route where the technique of administration does not matter, to achieve maximum drug delivery, technique is vital in inhaled therapy. Usually, when studies record adherence, they use pharmacy records or electronic diaries; however, these methods do not take into consideration the technique of the patients using inhalers. Some authors have used checklists to assess inhaler technique(5); however, these checklists only provide a snapshot of inhaler use.
To quantify both inhaler technique and adherence over time, we developed an audio recording electronic adherence monitor (INhaler Compliance Assessment, INCA™). The device records an audio file each time an inhaler is used by a patient. We have previously published the validation of this device and the methodology for correctly identifying inhaler technique errors.(6–10)
In previous studies using the INCA to record inhaler adherence in patients with respiratory disorders, we have identified several common errors in inhaler technique with the Diskus™ inhaler.(8–17) These errors include exhalation into the inhaler after drug priming but before inhalation, low peak inspiratory flow (PIF), multiple inhalations, breath hold less than 10 seconds (also seen in multiple inhalations where the patient exhales and inhales directly after the first inhalation), and missed doses.
Having described the frequency of these errors, the aim of this study is to assess their impact on drug delivery and to examine whether any of these errors should be considered “critical” technique errors. We hypothesize that previously identified, common inhaler errors lead to poor inhaled drug delivery and may, therefore, impact how we calculate adherence.
Materials and Methods
The aim of this study was to evaluate the impact of commonly observed inhaler technique errors. Trough and peak plasma salbutamol levels were compared between correctly taken events and when the inhaler was taken incorrectly.
Ethics and consent
The ethics committee of the Royal College of Surgeons in Ireland and Beaumont Hospital approved this study. All participants provided written informed consent.
Participants
Over a 3-month period, 14 healthy participants, who did not use an inhaler regularly (i.e., not on any inhaled corticosteroids and or long-acting beta agonists), were recruited. The exclusion criteria consisted of any history of sensitivity to salbutamol or refusal of consent.
Study design
All participants were instructed on the correct use of the salbutamol Diskus inhaler. Correct technique starts with opening the inhaler device, followed by priming the drug by moving the drug lever, exhaling away from the mouth piece, holding the device at a horizontal position and creating a tight seal around the mouth piece, taking a deep strong inhalation, breath holding for at least 10 seconds, and exhaling away from the inhaler and ends with closing the device. To ensure participants knew what an adequate inspiratory flow rate was, each participant demonstrated inspiratory flow with the Clement Clarke Inspiratory flow meter (set to Diskus) until they comfortably reached above 60 L/min.
Control phase (correct technique)
After ensuring adequate inhaler technique, each participant was asked to take six doses, 6 hours apart over 2 days.
Error phase (incorrect technique)
A minimum of 5 days after completing the Control Phase, participants commenced the Error Phase of the study. Participants used the salbutamol Diskus inhaler, six doses 6 hours apart over 2 days. However, in this phase, participants were asked to purposely make a consistent and predefined error each time the inhaler was used. These errors included: (1) exhaling into the device after drug blistering and before inhalation; (2) generating a low PIF (<below 35 L/min(18)); (3) taking multiple inhalations; (4) correct use but holding breath <5 seconds; (5) missing some doses (out of six doses, participants were asked to miss the fourth and fifth); and (6) wrong inhaler position.
Blood sampling
Serum salbutamol samples were taken before (time zero) and after (25 minutes after dose) dose one and dose six of each phase (totaling four samples per phase). The timing of blood sampling allowed for measurement of trough (time zero before dose six) and peak (time 25 minutes after dose one and dose six). See Figure 1 for the blood sampling schedule. Samples at time zero before dose one acted as a further control. Samples were initially collected in an ethylenediaminetetraacetic acid blood bottle. Each sample sat vertically for at least 30 minutes after venipuncture. Samples were then placed in a centrifuge and spun for 10 minutes at 1500 g. After this, 1 mL samples of plasma were pipetted out of the blood bottle into 1 mL capsules and frozen at −30°C. Each sample was labeled with a unique identifier and coded information on the subject number, the dose, the time taken of the sample, and the error (or no error for control samples).
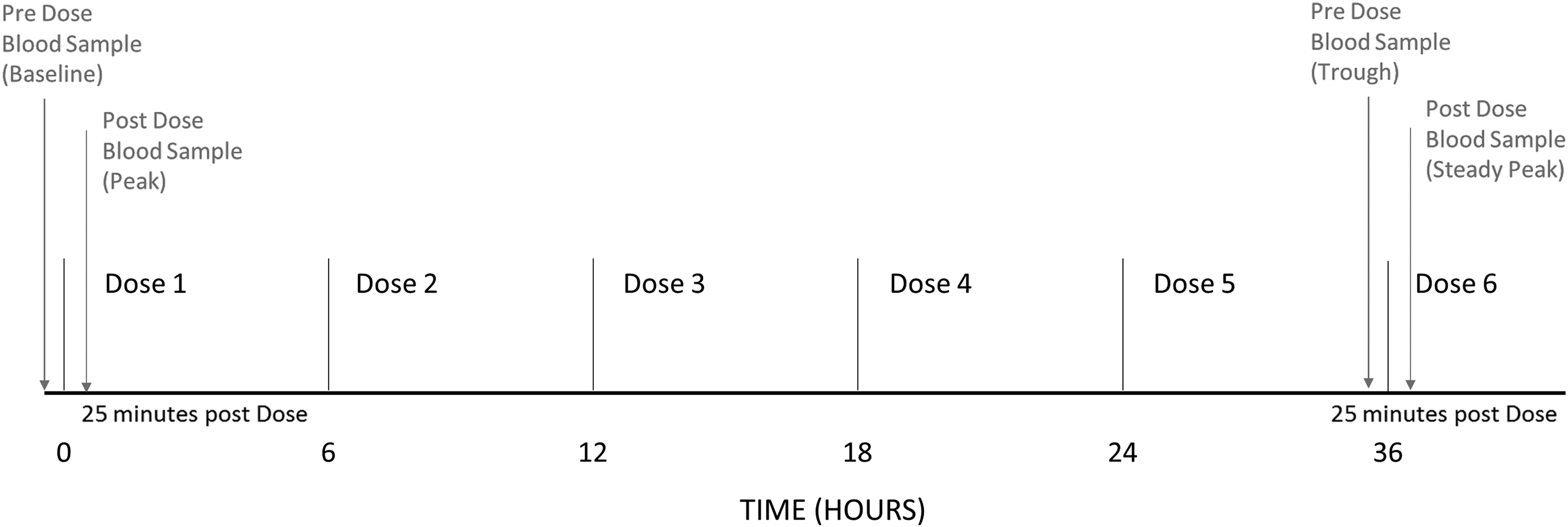
Blood sampling schedule: This figure illustrates the blood sampling schedule for this study. Based on the results of the pilot study, participants had a blood sample taken before dose one (a predose baseline level) and then a sample taken 25 minutes later (a peak level). Participants then took five more doses of salbutamol. Before the sixth dose, another sample was collected (a trough level) and then, a final sample was taken 25 minutes after dose six (a steady peak level). This blood-sampling schedule was the same for the control phase and error phase of the study.
Salbutamol assay—external
Serum salbutamol concentration was measured by using a published and widely used method adapted from Sidler-Moix et al.(19) Salbutamol sulfate was purchased from Sigma Aldrich (St. Louis, MO) and salbutamol-d4, the internal standard, was purchased from Toronto Research Chemicals (Toronto, Ontario, Canada). All chemicals and solvents were of analytical grade and used as received. A full description of the assay can be seen in the online supplement (Supplementary Data are available online at www.liebertpub.com/jamp).
Inhaler Compliance Assessment
The inhaler device used in this study was the DPI Diskus inhaler, and the drug administered to the participants was salbutamol. Salbutamol was chosen for this study, as measuring blood levels were previously tested and validated.(19–22) The INCA device was used to ensure that participants used the inhaler as directed and to provide an accurate measure of PIF.(14–17) The audio was downloaded and analyzed for each participant.
Outcomes measured
Plasma salbutamol levels for each time point (predose, peak dose, trough steady state, and peak steady state) were measured, and control levels were compared with each specific predefined error.
Statistical analysis
Descriptive statistics were used to present basic patient details for those included in this analysis. Means and standard deviations (SD) are presented for continuous variables. Paired T-tests were used to compare the means of salbutamol levels at different times between the different error phases and the control phase. All statistical analysis was conducted by using Stata Release 13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).
Results
Participants
Between June 2015 and August 2015, 14 healthy volunteers (not on any inhaled therapy) were recruited. Ten participants were men, whereas the remaining 4 were female. The mean (95% confidence interval) age for these participants was 25.8 (20.7, 30.8).
Control phase
All 14 participants completed the control phase of the study. Two runs of the salbutamol assay were completed for each sample received. For dose one, all participants had a baseline salbutamol level of near 0 (mean = 0.01). Twenty-five minutes after the dose, there was an increase in salbutamol levels for all participants, with a mean (SD) increase of 0.50 (0.14) ng/mL for the first run and 0.54 (0.16) ng/mL in the second run. This was not significantly different (p = 0.51).
By dose six, the mean (SD) trough level for all participants was 0.82 (0.11) ng/mL. Twenty-five minutes after dose six, all patients' plasma salbutamol levels increased by mean (SD) 0.58 (0.30) ng/mL for run 1 and 0.61 (0.26) ng/mL for run 2. Two patients had a decrease in salbutamol levels. Despite a good inhaler technique, these subject data were removed from all subsequent analyses. Due to the nonsignificant difference between run 1 and run 2, the mean of the two assessments was used for the rest of the analysis.
See Figure 2 for a summary of the control phase results.

Control-phase salbutamol level changes: All 14 participants completed the control phase. All samples were assessed with two sample runs.
Error phase
All participants completed both control phase (correct technique) and at least one error phase (technique error) (Fig. 3).
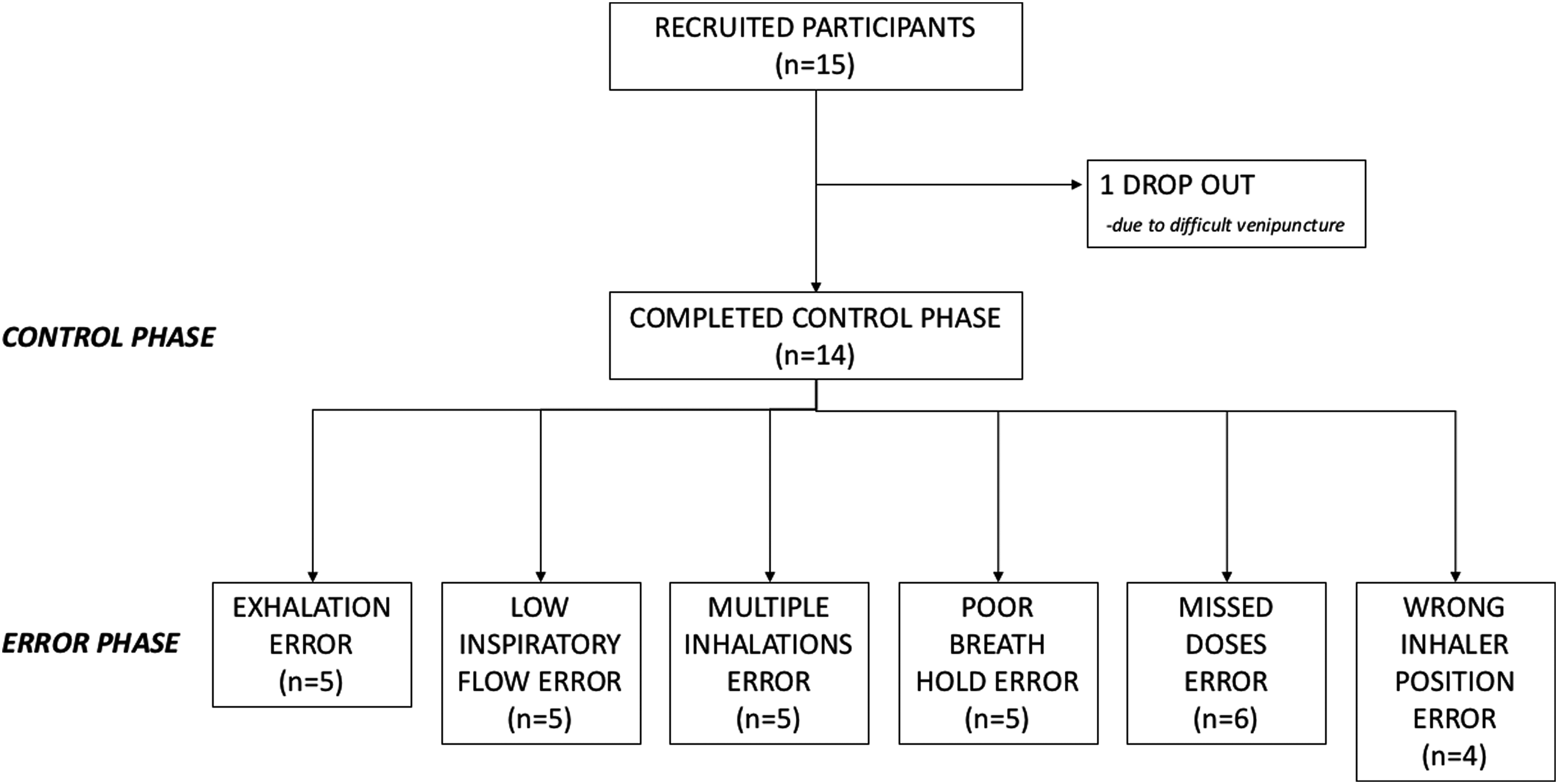
Study flow: This is a diagram of the study flow. Fifteen participants were recruited overall, with just one dropout. All 14 participants completed the control phase. Five participants completed the exhalation error, low inspiratory flow error, multiple inhalations error, and poor breath hold error. Six participants completed the missed doses error, and only four participants completed the wrong inhaler position error. Due to low recruitment, some participants completed more than one error; however, between errors, there was always a minimum 5-day gap to allow enough time for salbutamol levels to return to normal/not detectable.
Exhalation error
The mean (SD) baseline salbutamol level for patients performing this error was 0.00 (0.00). Participants (n = 5) then performed the exhalation inhaler error, described earlier (Fig. 4a, b), and a blood sample was taken 25 minutes later. Salbutamol levels rose to a mean (SD) 0.21 (0.29) ng/mL. This was not significantly different from the control phase, 0.53 (0.25) ng/mL (p = 0.12). Participants continued to make this error for the next four doses. Before taking dose six, the mean (SD) salbutamol level was 0.44 (0.35) ng/mL. This trough level was lower than the matched control phase, 0.79 (0.05) ng/mL; however, this was not significant (p = 0.10). Participants then took dose six with an exhalation error, and 25 minutes later the mean (SD) peak salbutamol level was 0.53 (0.40). This final peak level was significantly lower than the matched control (p < 0.01) (Fig. 5a and Table 1).
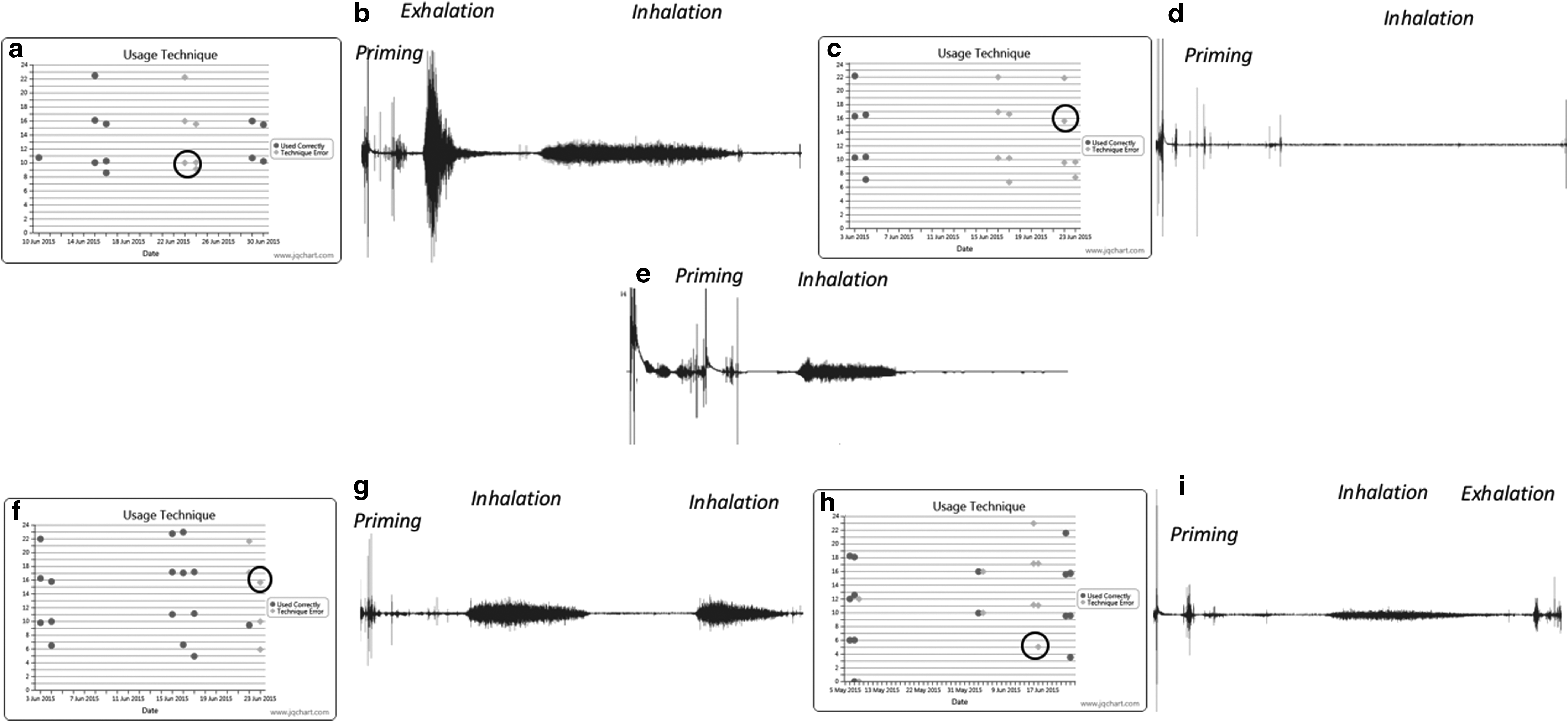
Examples of different inhaler technique errors in this figure,
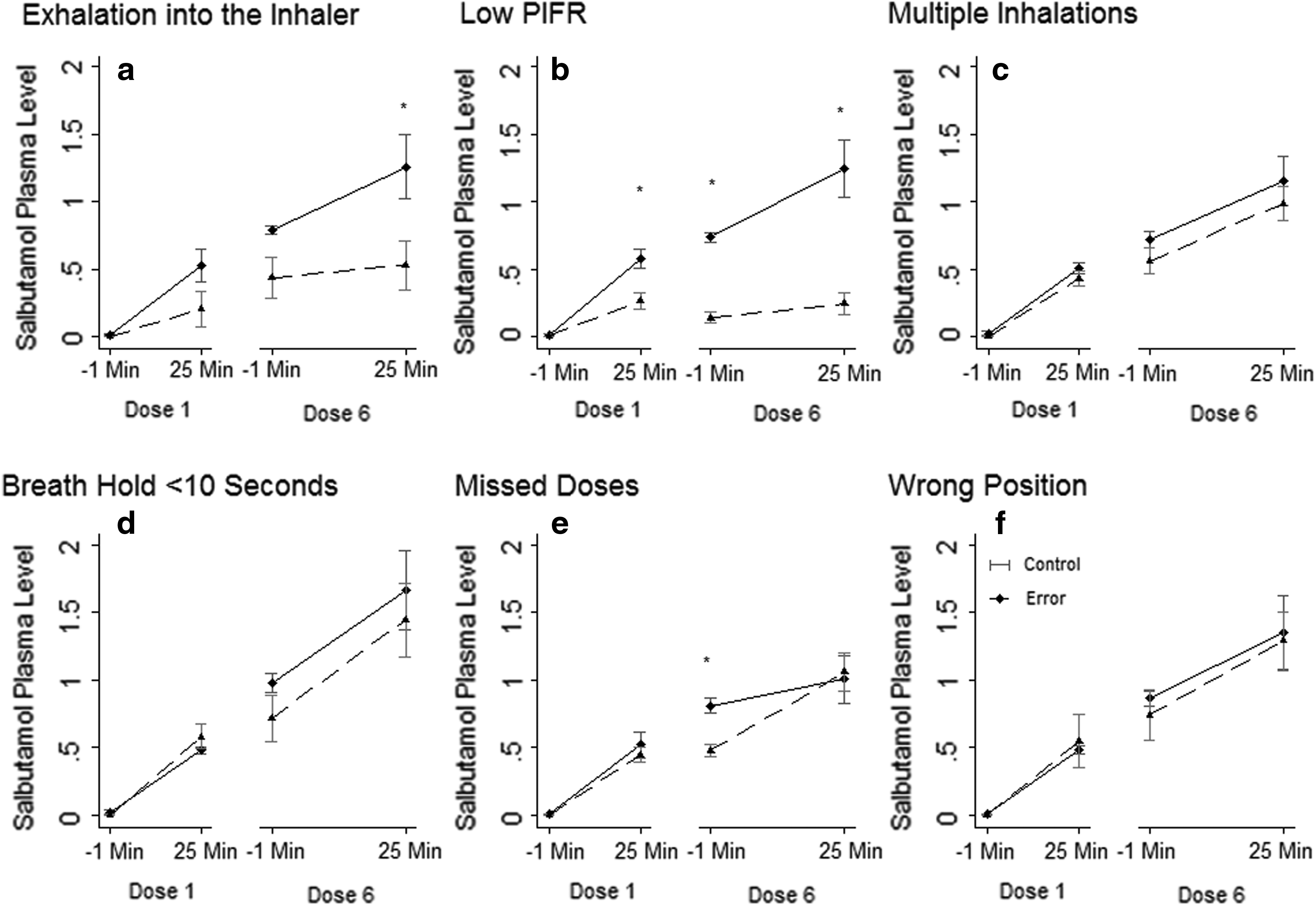
Comparing salbutamol levels for each inhaler error: Six inhaler errors [exhalation into the inhaler
All values are presented as mean (SD) ng/mL salbutamol levels. Fourteen participants were recruited to this study in total; all completed the control phase of the study. Five patients performed the exhalation error phase, five patients performed the low inspiratory flow error, five performed the multiple inhalation error, five performed the poor breath hold, six missed doses, and four participants used their inhaler in the wrong position. All baseline levels, dose 0 time 0, were near to zero. Exhalation into the inhaler after drug priming and before inhalation leads to a low level of salbutamol over time, only significant at 25 minutes after dose six. Low inspiratory flow error had a consistently low level of salbutamol throughout the study. Missed doses error lead to a low trough level before dose six was taken. *p < 0.05 compared with matched control levels. The difference in numbers between the matched control and errors in the exhalation error, missed doses error, and wrong position error is due to dropping the two participants whose salbutamol level fell 25 minutes after dose six.
SD, standard deviations.
Poor inspiratory flow
The baseline level of salbutamol was near zero in this error phase. Participants (n = 5) generated a low inspiratory flow (Fig. 4c, d) and 25 minutes after completing this error, the mean (SD) salbutamol level was 0.27 (0.13) ng/mL. This was significantly lower than the matched control of 0.58 (0.12) ng/mL (p = 0.02). Before the sixth dose, the mean (SD) salbutamol level was 0.14 (0.09) ng/mL. This trough level was also significantly lower than the matched control, 0.74 (0.06) ng/mL (p < 0.01). The peak salbutamol level at 25 minutes after dose six was 0.25 (0.18) ng/mL, and this also was significantly lower than the matched control of 1.24 (0.36) ng/mL (p < 0.01) (Fig. 5b and Table 1). Analysis of the acoustic properties of inhalation allowed the calculation of the PIF.(14,16) All participants who performed the low inspiratory flow error were shown to have generated a low flow with each inhalation.
Multiple inhalations
For this error, participants (n = 5) took their first dose with more than one inhalation (Fig. 4f, g) and 25 minutes later, their mean (SD) salbutamol level was 0.44 (0.13) ng/mL. This was very similar to the control phase of 0.51 (0.08) ng/mL and not statistically significant (p = 0.36). The trough level before dose six was 0.56 (0.21) ng/mL, again not significantly different from the control phase of 0.72 (0.12) ng/mL (p = 0.16). The mean (SD) peak salbutamol level 25 minutes after dose six was 0.99 (0.27) ng/mL. This was not significantly different from the control phase of 1.15 (0.37) ng/mL (p = 0.28) (Fig. 5c and Table 1).
Breath holding less than 5 seconds
For this error, participants (n = 5) took their first dose correctly but only held their breath for four or less seconds before exhaling fully (Fig. 4d, h). Twenty-five minutes later, the mean (SD) salbutamol level was 0.58 (0.20) ng/mL, and this was not significantly different than the control phase, 0.48 (0.06) ng/mL (p = 0.37). Continuing this error for the next four doses, before dose six, the mean (SD) salbutamol level was 0.54 (0.29) ng/mL, again not different from the control phase, 0.74 (0.11) ng/mL (p = 0.42). Twenty-five minutes later, the mean (SD) peak salbutamol level was 1.10 (0.46) ng/mL, and not significantly different from the control phase, 1.25 (0.44) ng/mL (p = 0.61) (Fig. 5d and Table 1).
Missing doses
Participants (n = 6) took their first dose correctly (Fig. 4e), leading to an increase in salbutamol levels up to 0.45 (0.13) ng/mL, 25 minutes after dose one. Participants then took their second and third dose 6 hours apart but omitted the fourth and fifth dose. The mean (SD) trough level after missing two doses of salbutamol was 0.48 (0.10) ng/mL. This was significantly lower than the control phase of 0.81 (0.13) ng/mL (p = 0.02). Participants then took their sixth dose correctly and 25 minutes later, their mean (SD) peak salbutamol level measured at 1.06 (0.36) ng/mL; this was not significantly different from the control phase of 1.01 (0.39) ng/mL (p = 0.51) (Fig. 5e and Table 1).
Wrong inhaler position
The participants (n = 4) in this error phase held the Diskus inhaler vertically, as opposed to the recommended horizontal position, and took a normal dose. The mean (SD) peak level 25 minutes after dose one was 0.55 (0.40) ng/mL, not significantly different from the control phase of 0.49 (0.06) ng/mL (p = 0.77). Participants held the inhaler in this position for each subsequent dose. Before dose six, the mean (SD) trough salbutamol level was 0.74 (0.37) ng/mL and 25 minutes later, it was 1.29 (0.43) ng/mL. Neither values were significantly different from the control phase (p = 0.75 and p = 0.39, respectively) (Fig. 5f and Table 1).
Discussion
Inhaled medications may become complicated by the introduction of a device that is required to deliver the medication. Unlike pill/oral-based medication, inhaled medication requires a “device,” such as the Diskus device, to deliver the medication, which introduces the potential for human error in using these devices. Currently, there are more than 10 different inhaler devices in the market.(23,24) Each comes with its own list of instructions and potential for human error. The aim of this study was to identify which of these errors directly affected drug delivery.
In a previous work, we identified and described the frequency of several common inhaler errors made by patients using a Diskus inhaler.(8–12,14–17,25) These errors included exhaling into the inhaler after drug priming and before inhalation, poor inspiratory flow rate and multiple inhalations (which, in theory, combines the exhalation error and poor breath hold as patients exhale directly after inhaling and then inhale again without a break). Although technically not an error in technique, missed doses can be considered an error in inhaler handling, since they affect the pharmacokinetic profile of the medication. Another possible error previously reported is the specific position of the inhaler. For the Diskus inhaler, it is suggested that the inhaler be held horizontal when used.(26)
The findings of the present study show that a persistently low inspiratory flow rate resulted in a significant reduction in the trough salbutamol level. A low inspiratory flow rate also led to a significant reduction in the peak salbutamol level. Exhalation after priming, but before inhalation, led to a significant reduction in peak salbutamol levels. Missing doses only had a significant effect on trough levels. In contrast, multiple inhalations, low breath hold, and wrong inhaler position had no significant impact on salbutamol levels.
Low inspiratory flow rate had the most significant effect on plasma salbutamol levels, and it was observed that in those performing the low inspiratory flow rate error, the inhaler device was covered with a dry powdered drug residue (Fig. 6), suggesting that with poor inspiratory flow, a proportion of the drug transferred to the mouthpiece with each blister is left in the mouthpiece and with time this residue gets displaced around the inhaler. Therefore, with this inhaler error, there is a large amount of drug wasted, leading to lower levels of drug delivery.
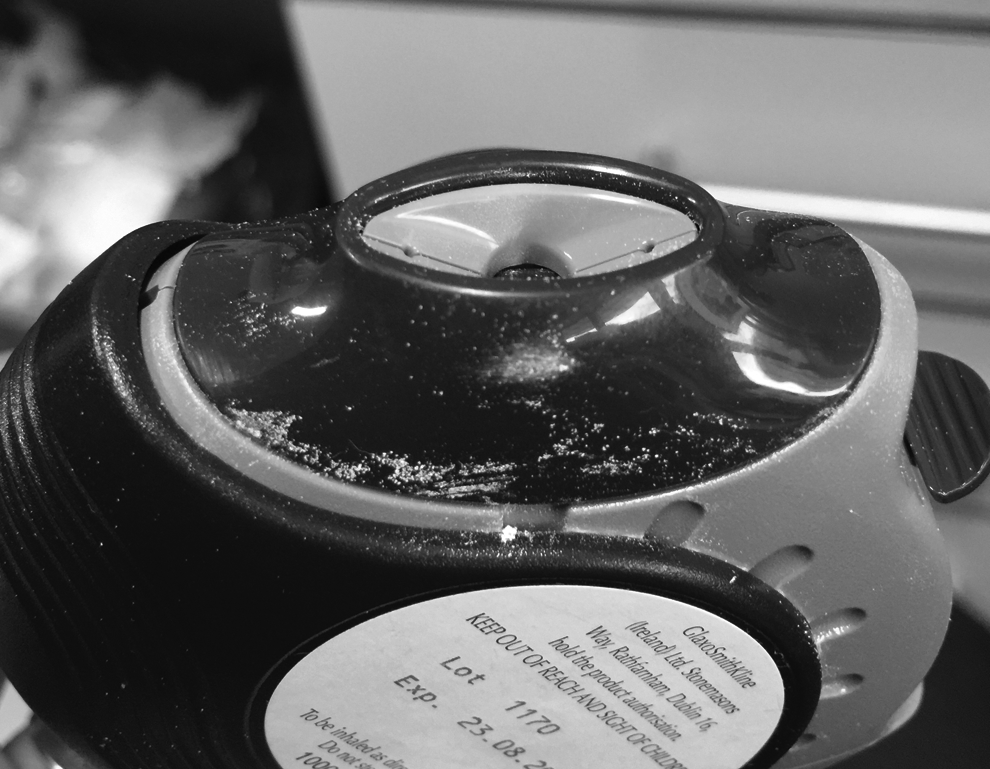
Low inspiratory flow error: This is an image of a participant's inhaler mouthpiece after performing the low inspiratory flow error for six doses. In the image, you can see the deposition of the dry powder inhaler all around the mouth piece, therefore leading to wasted drug and reduced drug delivery.
In a Cochrane review, the authors found that only 46%–59% of patients had an efficient inhalation technique.(27) With such low levels of proper inspiratory effort, these patients are only getting a small proportion of medication into their airways. This may lead to adverse effects such as poor disease control, increased exacerbations, higher mortality,(28) and possibly oral candida and vocal cord issues, such as hoarseness.
Exhalation into the inhaler after drug priming appeared to have a cumulative effect in the present study. There was no immediate effect on salbutamol levels, but over time there was a significant reduction in salbutamol levels after dose six. By exhaling into the mouthpiece after drug priming and before inhalation, the inhaler user is blowing the dry powder away from the mouthpiece and introducing moisture into the mouthpiece, therefore wetting and clumping the dry powder. The combinations of these two events lead to a significant reduction in plasma drug levels of salbutamol. Multiple inhalations and low breath hold are common inhaler errors.(11,12) However, in this study, neither of these errors had a significant effect on the salbutamol plasma levels.
Current methods of assessing inhaler technique utilize checklists. These checklists describe what are believed to be key steps in correctly taking an inhaler and only assess inhaler technique at one point in time.(5) These checklists do not identify careless errors and give equal ratings to any error, which may not be appropriate.
With the introduction of electronic monitors, inhaler adherence can be monitored over time.(29) However, none of the current electronic monitors are able to monitor inhaler technique. In this study, we have demonstrated that inhaler technique is both a crucial, and, with some errors, a critical component of measuring inhaler use. In a previously published randomized clinical trial looking at the effectiveness of an asthma education program that included education on inhaler technique, the authors found that the group randomized to the treatment arm had fewer exacerbations and greater increases in the Mini Asthma Quality of Life Questionnaire.(30) This highlights the potential importance of monitoring inhaler technique in respiratory diseases, such as asthma, which are dependent on inhaler treatment.
In another study looking at the impact that inhaler technique has on emergency department visits, the authors found that poor inhaler device use was associated with poor asthma control and frequent emergency department visits,(31) further supporting the importance of inhaler technique.
This study has some limitations. First, the Diskus inhaler device was the only inhaler device used. As previously mentioned, there are more than 10 inhaler devices in the market, all with their own specific instructions. A study is currently underway examining the effect of these inhaler errors with different inhaler devices. However, the errors found to be significant on drug delivery in this study, exhalation and low inspiratory flow, are applicable to any dry powder-based inhaler.
For this study, we used salbutamol as the inhaled drug. There are numerous other compounds prescribed to patients with airways disease, such as salmeterol, fluticasone, and budesonide. All these different inhaled drugs have different mechanisms, and similar studies with these various inhaled medications will need to be performed. However, the principle message of this study, that poor inspiratory effort and exhalation after drug priming before inhalation lead to poor drug delivery, still remains true for any inhaled medication studied.
Participants in this study were healthy volunteers. This was a proof-of-concept study. The aim of this study was to identify which inhaler errors captured by the INCA device lead to significant reductions in drug delivery. It is not certain what impact these findings may have on patients with airways disease, such as asthma and COPD, and future studies with these patients will need to be performed. It would also be important to see how these identified inhaler errors affect clinical outcomes such as lung physiology and quality of life.
In this study, we have identified two technique errors that should be considered critical technique errors: exhalation into the device after drug priming and before inhalation and low inspiratory flow. Not surprisingly, missing doses also lead to a reduction in drug delivery. Other common errors, multiple inhalations, poor breath hold, and wrong inhaler position had no impact on drug delivery.
Footnotes
Acknowledgments
N.S., E.M., A.S.B., B.C., and M.C.M. were primarily involved in patient recruitment for this article. I.K. and R.B.R. were primarily involved in the audio analysis required for this article. F.B. was primarily involved in the statistical analysis for this article. J.S., S.G., and N.S. were involved in the salbutamol assay work. I.S. and R.W.C. were involved in all aspects required for this article, including patient recruitment, data management, and data analysis, and were the primary leads in writing this article. All co-authors were involved in writing and editing this article. This was a researcher-initiated study, funded by the Health Research Board of Ireland. The funder of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the article. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit it for publication.
Author Disclosure Statement
Authors I.K., R.B.R., and R.W.C. are named on a patent for the INCA™ device. However, this aim of this article was not to validate this technology but to quantify inhaler technique errors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.