
Abstract
Abstract
Background:
Placement of a heat moisture exchanger (HME) between aerosol generator and patient has been associated with greatly reduced drug delivery. The purpose of this study was to evaluate the effect of filtered and nonfiltered HMEs placed between nebulizer and patient on aerosol deposition and airway resistance (Raw) in simulated ventilator-dependent adults.
Methods:
An in vitro lung model was developed to simulate a mechanically ventilated adult (Vt 500 mL, RR 15/min, and PEEP 5 cmH2O, using two inspiratory flow rates 40 and 50 L/min) using an intubated adult manikin with an endotracheal tube (8 mmID). The bronchi of the manikin were connected to a Y-adapter through a collecting filter (Respirgard II) attached to a test lung through a heated humidifier (37°C producing 100% relative humidity) to simulate exhaled humidity. For treatment conditions, a nonfiltered HME (ThermoFlo™ 6070; ARC Medical) and filtered HMEs (ThermoFlo™ Filter; ARC Medical and PALL Ultipor; Pall Medical) were placed between the ventilator circuit at the endotracheal tube and allowed to acclimate to the exhaled heat and humidity for 30 minutes before aerosol administration. Airway resistance (cmH2O/L/s) was taken at 0, 10, 20, and 30 minutes after HME placement and after each of four aerosol treatments. Albuterol sulfate (2.5 mg/3 mL) was administered with jet (Misty Max 10; Airlife) and mesh (Aerogen Solo; Aerogen) nebulizers positioned in the inspiratory limb proximal to the Y-adapter. Control consisted of nebulization with no HME. Drug was eluted from filter at the end of the trachea and measured using spectrophotometry (276 nm).
Results:
Greater than 60% of the control dose was delivered through the ThermoFlo. No significant difference was found between the first four treatments given by the jet (p = 0.825) and the mesh (p = 0.753) nebulizers. There is a small increase in Raw between pre- and post-four treatments with the jet (p = 0.001) and mesh (p = 0.015) nebulizers. Aerosol delivery through filtered HMEs was similar (<0.5%) across the four treatments. Airway resistance was similar using the ThermoFlo Filter. With the PALL Ultipor, changes in Raw increased with mesh nebulizer after treatment (p = 0.005). Changes in resistance pre- and post-treatment were similar with both filtered HMEs.
Conclusion:
The ThermoFlo™ nonfilter HME allowed the majority of the control dose to be delivered to the airway. Increases in Raw would likely not be outside of a tolerable range in ventilated patients. In contrast, filtered HMEs should not be placed between nebulizers and patient airways. Further research with other HMEs and materials is warranted.
Introduction
I
The HME is considered as a barrier to aerosol drug delivery in ventilator-dependent patients. Through the collection of medical aerosols in the HME during aerosol therapy, airway resistance may further increase during mechanical ventilation. Although the impact of aerosol drug delivery through HME has not been reported, clinicians remove HMEs from the ventilator circuit before aerosol therapy to prevent the filtering feature of the HME that acts as a barrier for the delivery of medical aerosols to the patient.
During aerosol administration, it has been speculated that a substantial amount of drug can build up within an HME, increasing resistance of gas passing through and resulting in substantial increases in work of breathing that might adversely impact ventilator-dependent patients. With the advent of modern materials and design, some HMEs may be able to effectively pass aerosol on to the patient without a substantial decrease in drug delivery to the airway or increase in airway resistance. The purpose of this study is to evaluate the effectiveness of an HME on aerosol deposition and airway resistance with delivery of an aerosolized bronchodilator using jet and mesh nebulizers during mechanical ventilation. The following questions were answered in this study:
1. What is the amount of drug deposition when aerosol is passed through filtered and nonfiltered HMEs in a simulated adult lung model receiving mechanical ventilation? 2. How does repeated administration of aerosolized medications through filtered and nonfiltered HMEs with jet and mesh nebulizers impact airway resistance in simulated ventilator-dependent adults?
Materials and Methods
Types of HMEs
Three types of HMEs tested in this study include (1) nonfiltered HME (ThermoFlo™; ARC Medical, Atlanta, GA) and (2) filtered HMEs: ThermoFlo™ filter (ARC Medical) and PALL Ultipor (PALL Medical, Port Washington, NY).
Lung model
As shown in Figure 1, an anatomical teaching manikin was intubated with an ETT (Mallinckrodt, Covidien, Mansfield, MA) of 8 mmID. Each mainstem bronchi of the manikin was connected to a Y-adapter through a collecting filter (Respirgard II; Vital Signs, Totowa, NJ) attached to a test lung through a heated humidifier (Fisher & Paykel Healthcare, Auckland, New Zealand) to simulate a ventilator-dependent adult with exhaled humidity. The relative humidity was 100%, and temperature was kept 35 ± 2°C during each experiment. A ventilator using a standard unheated ventilator circuit was heated and humidified with each HME tested in this study. While the jet nebulizer (JN) was placed 6 in from the Y-adapter in the inspiratory limb of the ventilator circuit, the mesh nebulizer (MN) was located at the Y-adapter as per the manufacturer's recommendation. All HMEs tested in this study were kept between the ETT and the nebulizer.
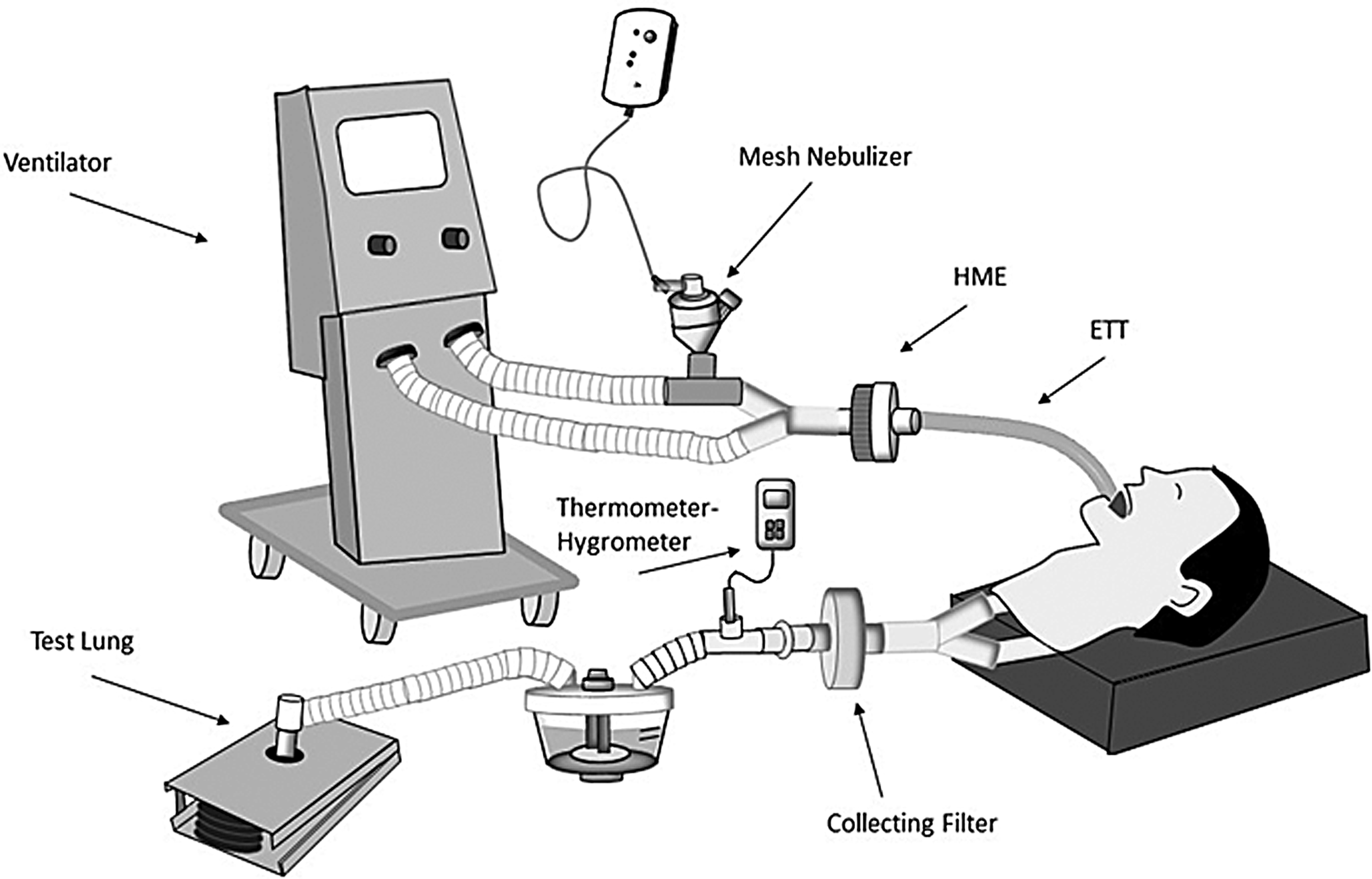
Experimental setup of the study.
Ventilator settings
Standard adult ventilator settings were used with volume control ventilation (tidal volume: 500 mL, respiratory rate: 15 bpm, PEEP: 5 cmH2O, and inspiratory flow 40 L/min) when testing the nonfiltered HME. The following breathing parameters were used with filtered HMEs: Vt 500 mL, RR 15/min, PEEP 5 cmH2O, and inspiratory flow 50 L/min. Before each experiment, the ventilator circuit and lung model were checked to ensure connection integrity and proper functionality.
Study variables
The independent variables of this study include the delivery of albuterol sulfate through the nonfiltered HME (ThermoFlo HME) and filtered HMEs (ThermoFlo Filter HME and PALL Ultipor Filter HME) using JN and MN against control (without HME in place). Inhaled mass and airway resistance are the primary outcome variables of this study. Inhaled mass was obtained with each aerosol treatment after each run. Airway resistance was measured via the ventilator, using the resident software to determine inspiratory resistance. The values on resistance were taken from the display on the ventilator monitor.
Study design
As shown in Figure 2, this study has a control and a treatment group. In all experiments, albuterol sulfate (2.5 mg/3 mL) was delivered via JN (Misty Max 10; Carefusion, Yorba Linda, CA) and MN (Aerogen Solo, Galway, Ireland) placed between the inspiratory limb and Y-piece. For control, no HME was placed in the circuit, while treatment group had HMEs placed between ventilator circuit and airway.
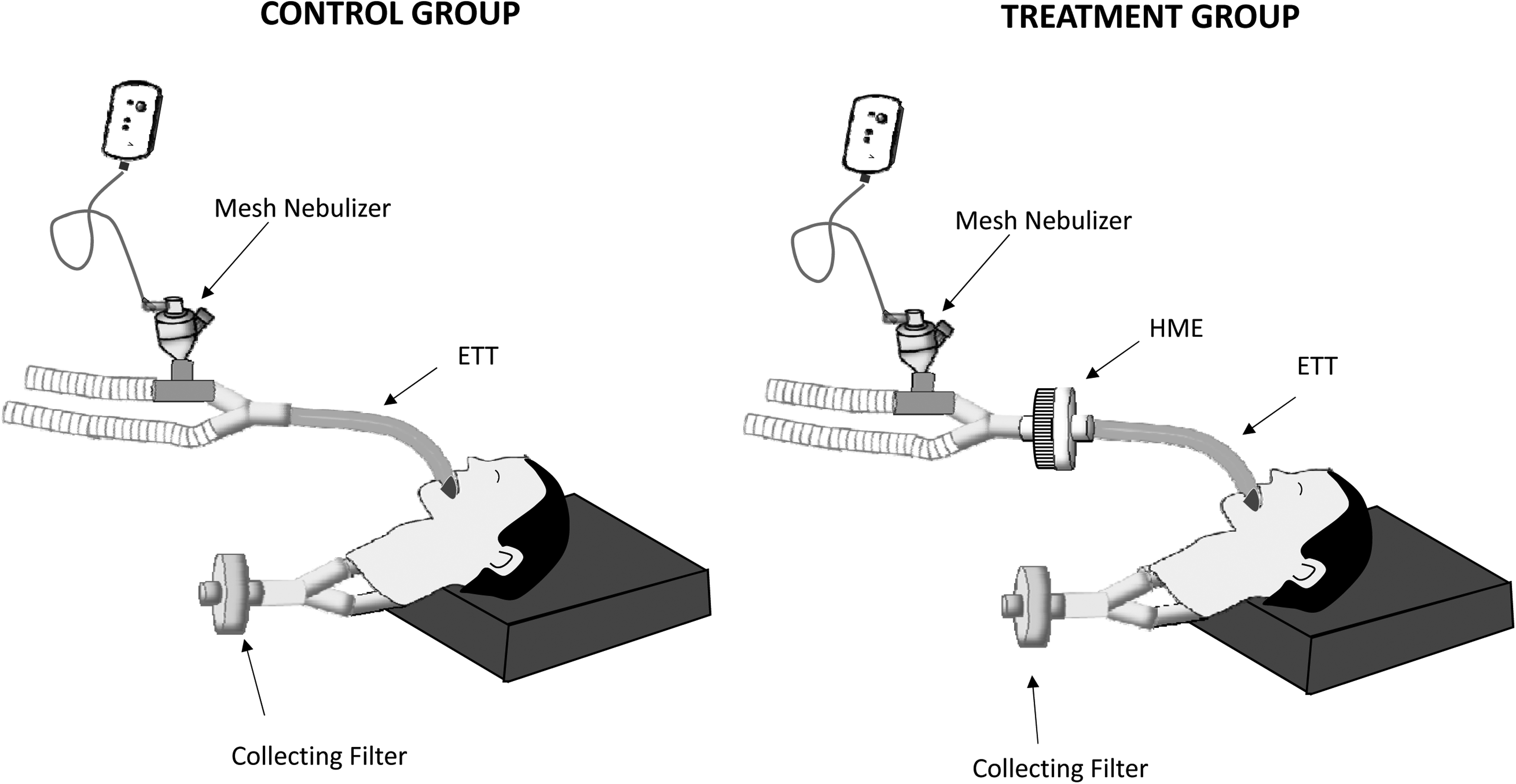
Setup for testing without HME (Control) and with HME (Treatment) in the circuit.
Aerosol particle size distribution, expressed as volume median diameter (VMD) and geometric standard deviation (GSD), was determined via laser diffraction (Spraytec, Malvern) for each nebulizer alone and in series with each HME type.
Aerosol deposition was measured at the end of each run. In the treatment group, aerosolized albuterol was administered through filtered and nonfiltered HMEs that were placed between ETT and the nebulizer. Before administering aerosol treatment, each HME was exposed to simulated exhaled humidity allowed to become saturated for >30 minutes before aerosol administration. Airway resistance was measured immediately after the placement of each HME in the ventilator circuit. To represent daily delivery of aerosolized albuterol sulfate, a series of four repeated doses were administered with the same HME in place. Both filtered and nonfiltered HMEs were tested five times (n = 5).
Data collection
Aerosol drug that is deposited on an absolute filter placed at the end of the trachea was eluted with 0.1 molar N hydrochloric acid for 3 minutes and measured using a spectrophotometric technique (Beckman Instruments, Fullerton, CA), at a wavelength of 276 nm. The drug was reported as a percentage of the dose placed in the nebulizer. Airway resistance (cmH2O/L/s) was determined using the resident ventilator software for inspiratory resistance. Values were collected from the resistance display reported on the patient data section of the ventilator monitor. Inspiratory resistance was recorded immediately and at 10, 20, and 30 minutes after placement of the HME in the ventilator circuit for both control and treatment groups. Airway resistance was also recorded at the end of each treatment.
Data analysis
The means and standard deviations were calculated for total inhaled mass and airway resistance. Differences between the inhaled mass percent obtained with the control and treatment were compared with the Mann–Whitney U statistical analysis. Data on airway resistance were analyzed with the Kruskal–Wallis analysis of variance. Differences were considered statistically significant when p < 0.05.
Results
Aerosol deposition through HME
As shown in Table 1, greater than 62% of the control dose was delivered through the ThermoFlo nonfiltered HME regardless of the type of nebulizer tested in this study. No significant difference was found between the first four treatments given by the JN (p = 0.825) and the MN (p = 0.753) nebulizers. Aerosol drug delivery with the MN was twofold greater than with the JN (p < 0.05).
Delivered dose greater than treatment with same nebulizer (p = 0.001).
HME, heat moisture exchanger.
Aerosol delivery through both filtered HMEs (ThermoFlo Filter and PALL Ultipor) was similar and <0.5% (Table 2). No significant difference was found in percentage of dose delivered across the four treatments given by JN and MN, using the ThermoFlo Filter (p = 0.98 and p = 0.99, respectively), and the PALL Ultipor (p = 0.69 and p = 0.98, respectively).
The particle size distribution of aerosol produced by Misty Max at 8 L/min was 3.56 μm with a GSD of 2.2, and the Aerogen Solo was 4.42 μm and 1.6, respectively. Particle size of aerosol passing through the ThermoFlo ranged from 0.57 to 1.5 μm with MN and 1.18 to 1.32 μm with the JN.
Administration duration of the Misty Max 10 to one minute past sputter was 8 minutes ±9 seconds versus 6 minutes ±20 seconds to end of aerosol generation with the Aerogen Solo.
Effect of repeated aerosol administration on airway resistance
The measured airway resistance in cmH2O/L/s with nonfiltered HMEs using JN and MN with peak flows of 40 L/min before and after treatments (Table 3) and at peak flows of 50 L/min with all three HMEs (Table 4) increased over 30 minutes of HME exposure to exhaled humidity (p = 0.02). However, Raw did not increase with individual or with the four cumulative aerosol treatments with either JN (p = 0.99) or MN (p = 0.25).
Airway resistance was similar with JN (p = 0.63) and MN (p = 0.11) using the ThermoFlo Filter. With the PALL Ultipor, changes in Raw was similar with JN (p = 0.13), but Raw increased with MN after treatment (p = 0.005). Changes in resistance pre- and posttreatments were similar with both filtered HMEs.
Discussion
This is the first study reporting that aerosol can be delivered through a nonfilter HME to a simulated intubated adult without increasing airway resistance with serial doses of aerosol. While many authors have recommended removing an HME from between the aerosol generator and the patient airway, we could find no published evidence supporting that practice.(9) Our findings suggest that when using the ThermoFlo HME, the moderate reduction in aerosol delivery (<40% vs. control) with both JN and MN with no significant increase in Raw with four treatments may provide a reasonable alternative to removing and replacing this HME with each aerosol administration. This finding is in stark contrast to aerosol delivery through the filtered HMEs (ThermoFlo Filter and PALL Ultipor Filter), which reduced delivered dose to <0.5%, demonstrating that not all HMEs are created equal and filtered HMEs should always be removed from that pathway between the aerosol generator and the patient's airway.
Our findings confirm that reports of Raw increase with exposure to exhaled humidity over time. Use of HME has been associated with an increase in airway resistance due to saturation and occlusion of the filter medium during mechanical ventilation, and continuous monitoring has been advocated.(5,10–12) The findings of this study show simulated use of HME with exhaled humidity in a ventilator-dependent adult lung model resulted in a moderate increase in measured airway resistance over the first 30 minutes of exposure, to a level that would likely not be outside of an acceptable tolerable range during mechanical ventilation. This simulates the type of Raw changes during the first 30 minutes of HME use.
We chose four doses of aerosol, as this reflects a common QID administration of aerosol four times a day. The proportion of aerosol passing through the HME through the airways compared with control values (with no HME inline) were consistent with both JN and MN at 63.78% and 62.12%, respectively. This similarity despite the manufacturer claims of a twofold difference in particle size distribution of the two types of nebulizers used. This level of delivery efficiency did not change between any of the four serial doses, suggesting that any loading of the HME was not reducing filtering of the aerosol. This corresponds to the lack of Raw increase across doses.
We did not observe linear effect on airway resistance with each treatment administered with both JN and MN due to continuous nebulization and the volume of medication trapped by any of HMEs during aerosol therapy.
The lung model used in this study uses a heated humidifier to simulate exhaled humidity by the lung model, which is essential to load the HME with heat and humidity before measuring resistance changes pre- and postaerosol administration. The resistance to gas flow through an HME changes with exposure to humidity over time during mechanical ventilation. Our previous research(13) showed aerosol delivery with JN and MN ranged from 9.7% to 30.2% with the nonhumidified ventilator circuit, respectively, as opposed to the findings of this study, in which aerosol delivery efficiency was 5.4% with the JN and 10.6% with the MN in the control group. The differences in deposition can be explained by the exhaled humidity simulated in the current study.
According to previous research, heat and humidity reduce the amount of drug delivered distal to the trachea up to 50%.(14–18) However, it is important to note that previous in vitro studies did not take exhaled humidity into account. A recently published in vitro study(19) reported that simulating exhaled humidity in a lung model decreased the delivery of albuterol sulfate by 44% compared with the lung model without exhaled humidity.
Ari et al.(13) found aerosol deposition with heated/humidified ventilator circuit during mechanical ventilation was 3.6% to 16.8% with JN and MN, respectively. The amount of aerosol delivered with the JN in this study ranged from 3.4% to 3.6% with the first four treatments while aerosol deposition with the MN was ∼6.6%. The reduced delivery of aerosol passing through the HME without increasing Raw may be justified as an alternative to interrupting ventilation to remove and replace an HME before and after each treatment. In 2010, Ari et al. used similar ventilator parameters but a more conventional model without simulated exhaled humidity. Simulated exhaled humidity appears to reduce aerosol drug delivery distal to the airway compared with nonheated humidified conditions.
Current recommendations for aerosol delivery include removing the HME from between the aerosol generator and the patient airway.(20–22) Our findings suggest that not all HMEs act as filters to the same level. Even the filtered HMEs, which have been described as absolute filters, allowed 0.4% of the aerosol to pass through, despite the particle sizes being below the level of quantification of the laser diffraction method we used.
Limitations of the study and further research
In this model, aerosol passes through the HME during inspiration and again as a portion is exhaled. A greater proportion of aerosol inhaled during mechanical ventilation is exhaled in vivo than in vitro models, in which the aerosol is collected on an absolute filter. Consequently, our model underestimates the aerosol load on the HME by as much as 5%.(16) Therefore, the amount of drug collected in the HME during this bench study would be less than a similar in vivo study that may lead to a greater impact of drug collected in the HME on airway resistance. While we did not leave the HME in the circuit for 24 hours, the accelerated schedule for treatments most likely would increase the load on the HMEs, with less time for the liquid load on the filter to be redistributed.
Changes in inspiratory resistance as measured through the ventilator were evaluated in this study based on the assumption that changes in inspiratory resistance in the steady state in vitro model would reflect changes in resistance through HME during mechanical ventilation. Currently, many ventilators provide dynamic measurements of inspiratory resistance that are readily available to the clinicians at the bedside. Although algorithms to determine this parameter may vary between models of ventilator, similar changes in inspiratory resistance would be demonstrated regardless of the brand of mechanical ventilator used. While it might be more precise to measure the change in filter resistance by measuring changes in pressure by passing a constant flow of gas through the HME, this type of measurement is not performed at the bedside. In addition, it is not practical to do manual calculations based on airway pressure and inspiratory flow because of descending flow patterns used in ventilator-dependent patients. However, further research with different ventilators is warranted to confirm this.
It must be emphasized that this study represents one specific type of HME and our findings should not be generalized to other HME types or materials. Previous research reported that each type, design, and brand of HME makes a difference on the amount of moisture collected within HME that affects airway resistance.(23–25) Therefore, future research testing a variety of HMEs available on the market is necessary for understanding the impact of different HMEs on airway resistance and aerosol deposition. Albuterol sulfate was used in this study, it is also important to determine the impact of viscous medications such as mucomyst on Raw and HME performance in ventilator-dependent patients.
Conclusion
Placement of a ThermoFlo HME between the aerosol generator and ETT resulted in the majority of aerosol depositing distal the airway compared with control. Raw increased with exposure to exhaled humidity, but increased secondary to a series of four treatments that were not significant and stayed within a tolerable range in ventilated patients. These findings cannot be generalized to other HME designs and materials such as the two filtered HMEs tested. Further research with other HMEs and materials is warranted. Filtered HMEs allowed <0.5% of aerosol drug to reach the airway. Our findings support recommendations that filtered HMEs should not be placed between nebulizers and patient airways.
Footnotes
Author Disclosure Statement
This study was funded with an unrestricted research grant from ARC Medical. Dr. A.A. has a relationship with Bayer Pharmaceuticals, ARC Medical, and Aerogen. Dr. J.B.F. is CSO of Aerogen Pharma Corp. The rest of the authors have no conflict of interest to disclose.