
Abstract
Abstract
Background:
Corticosteroids play an important role in the treatment of chronic obstructive pulmonary disease (COPD) exacerbations, and a global initiative has suggested the use of inhaled corticosteroids (ICSs) as an alternative to systemic corticosteroids (SCs). Here, we report results of a meta-analysis performed to systematically compare the efficacies of ICSs and SCs in the treatment of COPD exacerbations.
Methods:
PubMed, EMBASE, and the Cochrane databases were searched for relevant human clinical trials describing the use of ICSs compared with SCs in the treatment of COPD exacerbations. We compared the results of FEV1%pred and blood gas analyses that had been calculated. Weighted mean differences and fixed effects models were applied by using Revman 5.2.
Results:
Five original studies satisfied our inclusion criteria, and no significant heterogeneity was shown. Three studies evaluated the increase of FEV1%pred after treatment for 7 days. There were three and four studies, respectively, that evaluated the increase of SaO2 and PaO2, and three reported the decrease of PaCO2 at 24 hours control, 2–4 days control, and 7–10 days control. All the results showed that both ICSs and SCs were effective in the treatment of COPD exacerbations.
Conclusion:
ICSs were not inferior to SCs when used in the treatment of COPD exacerbations.
Introduction
C
When administered by following international guidelines, systemic corticosteroids (SCs), bronchodilators, and antibacterial agents all play an important role in the management of COPD exacerbations.(5,6) However, there remain concerns about administering SCs to COPD patients because of their adverse effects such as osteoporosis and bone fractures, thinning of the skin, posterior subcapsular cataract formation, glucose intolerance, and myopathy.(7–10)
Over the years, clinicians have searched for agents that provide the same therapeutic results as SCs in treating AECOPD, but that produce fewer adverse effects. Inhaled corticosteroids (ICSs) have been used as a safe and effective treatment for COPD since 1992,(11) and they are often used either alone(12) or in combination with long-acting β2-agonists.(13–16) ICSs can be safely used for treating COPD, and they demonstrate high degrees of topical anti-inflammatory activity and low levels of systemic activity.(17,18)
The Global Initiative for COPD has suggested ICSs as an alternative to SCs for treating COPD exacerbations; however, there have been only a few published studies on this topic.(19–25) We conducted this study to systematically compare the efficacies of ICSs and SCs by using a meta-analysis.
Methods
Literature search
We performed three separate literature searches of PubMed, EMBASE, and Cochrane databases to identify all relevant human clinical trials that compared ICSs and systemic steroids in treating COPD patients, and for which the results were published between 1971 and June 2014. The search strategy utilized text words for COPD, the names of inhaled and systemic steroids used in treating COPD, and relevant keywords.
The terms used in the searches were as follows: (1) insufflation, inhalation, inhaled, inhalants, nebulized, parental, budesonide, beclomethasone, beclomethasonepropionate, fluticasonepropionate, fluticasone, and aerosols; (2) methylprednisolone, prednisolone, prednisone, hydroprednisone, veins, infusions, intravenous, systemic, oral, and parenteral; and (3) COPD, obstructive pulmonary disease, and obstructive disease of the lung. Boolean logic was used to truncate and combine terms. All article titles were reviewed for their relevance, all subject headings and abstracts were examined, and only clinical trials that involved human subjects were included in the final analysis. The search was further augmented by reviewing and scanning references cited in the retrieved papers. The literature searches were not limited by the language of the published paper or abstract.
Inclusion criteria
All studies included in the meta-analysis had to satisfy the following criteria: (1) the study had been published and showed results of a randomized, controlled clinical trial conducted in humans; (2) the study compared results obtained when treating AECOPD patients with an ICS versus an SC; (3) the diagnostic criteria for AECOPD were consistent with the criteria used by GOLD or ATS; and (4) there were sufficient data to perform a comparison of lung function, blood gas analysis, exacerbations, health-related quality of life, or adverse reactions.
Data extraction
Two investigators independently extracted data from the selected articles, after which the results were compared, and differences were resolved by discussion and consensus. The first author's surname and the year of article publication were used for identification purposes. The following study and patient characteristics were included in the extracted data: authors' names, publication year, study design, sample size, study population, patient age (mean or range), sex, number of current smokers, pack-years, GOLD classification, baseline values for lung function and blood gas analysis, duration of treatment, treatment comparisons, and other data of interest (e.g., changes in FEV1%pred, PaO2, PaCO2, and SaO2). Mean values, standard deviations, 95% confidence intervals (CIs), as well as the maximum and minimum values of study outcomes were also extracted for further analysis. Certain data were extracted by interpreting the published figures.
Methodological quality
We used the Cochrane collaboration classification scheme and the following factors to assess the quality of articles included in the meta-analysis: method of randomization; sequence generation; allocation concealment for selection bias; blinding for performance bias; whether or not lost patients were accounted for; whether the outcome assessor was blinded for detection bias; and whether there was evidence of selective reporting of outcome measures and other bias.
Statistical analysis
The meta-analysis was performed by using Review Manager 5.2 (Revman, The Cochrane Collaboration, Oxford, United Kingdom). The results were pooled by using weighted mean differences (WMDs) and corresponding 95% CIs, as all the data were in the same units and not much difference was seen between means. Q and I2 statistics were used to examine statistical heterogeneity among individual studies. Pheterogeneity >0.10 or I2 < 50 indicated no significant heterogeneity. If significant heterogeneity was observed, we used a random-effects model to analyze the pooled results; otherwise, a fixed-effects model was used. Basic statistical formulas were used to calculate the data for final analysis, such as mean values, standard deviations, 95% CIs, as well as the maximum and minimum values of FEV1%pred, SaO2, PaO2, and PaCO2.
Results
Search results
The initial search yielded 427 unique titles and abstracts from PubMed, Cochrane, and EMBASE databases; however, after reading them, only seven satisfied our inclusion criteria.(19–25) After reviewing the articles and bibliographies, five articles were included in the final meta-analysis.(21–25) Two articles were excluded, as we were unable to extract data from the text of the manuscripts. Details of the study selection process are shown in Figure 1.
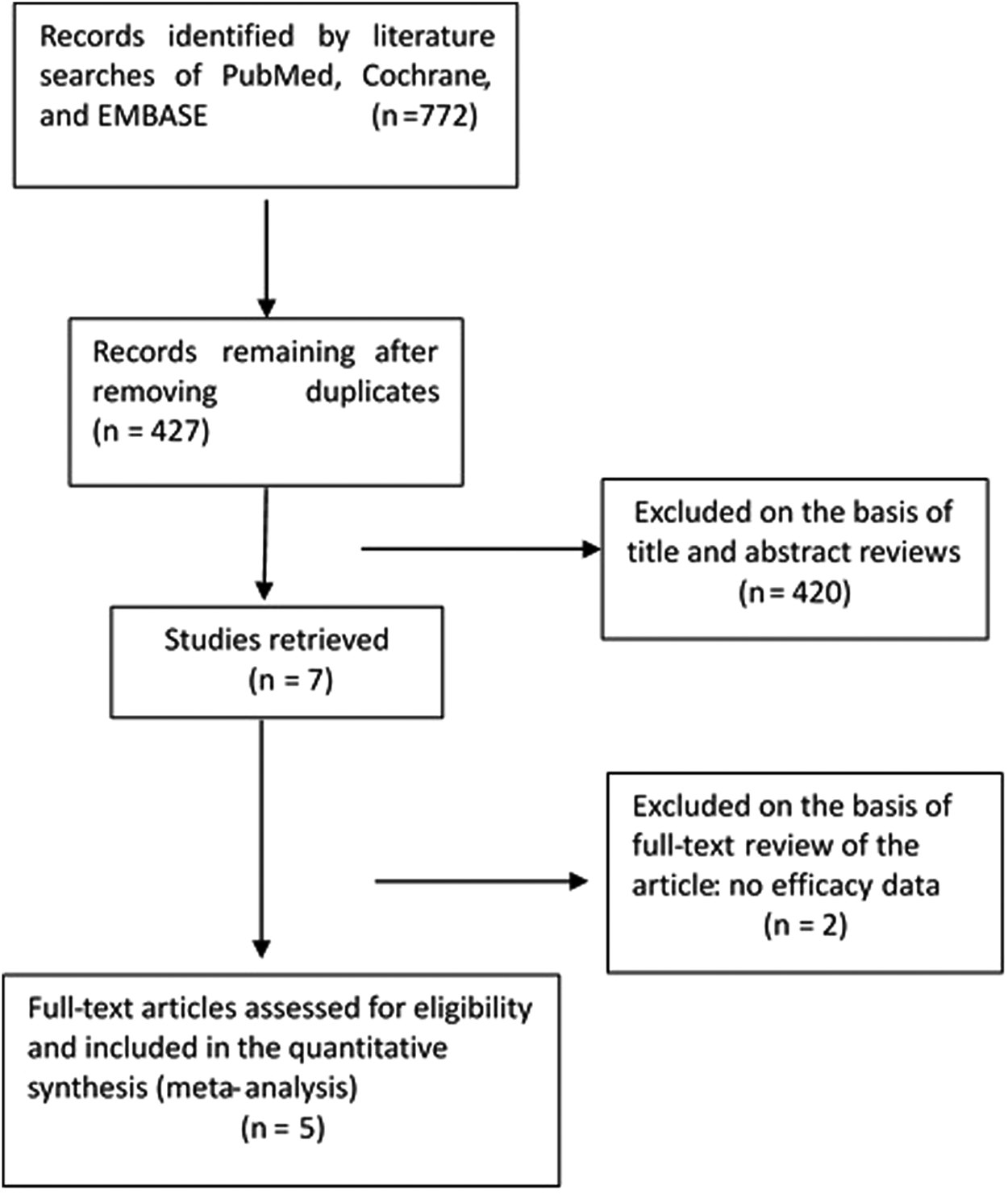
Study flow diagram of the meta-analysis.
Study characteristics
Various characteristics of the included trials and patients are shown in Tables 1 and 2, respectively.
COPD, chronic obstructive pulmonary disease; /, not mentioned in the included studies.
The included studies enrolled a total of 343 participants with a mean age of 65.3 years, and all subjects were aged >40 years. Only one study used both SCs and ICSs (>1500 μg/d) therapy in preceding months as an exclusion criterion, whereas others were based on the SCs therapy as an exclusion criterion. All study subjects were current or ex-smokers, and the majority had moderate or severe COPD. The included studies had a treatment duration of ∼10 days. Four studies used different doses (that were significantly higher compared with the dose used in stable patients) of nebulized budesonide, which is mentioned in Table 1 as a comparator to SCs,(21,22,24,25) and one study used a budesonide inhaler.(23) All studies reported changes in lung function, health-related quality of life, arterial blood gases, and any adverse events in the Results section of the paper or abstract.
Our current meta-analysis focused on changes in lung function (FEV1%pred) and the results of arterial blood gas analyses (PaO2, PaCO2, and SaO2). Our analysis of FEV1%pred utilized data obtained from 179 patients after 7 days of treatment.(22,23,25) The SaO2 analysis included data obtained from 208 patients(21,22,24) after 24 hours, 2–4 days, and 10 days of treatment. The PaO2 analysis utilized data gathered from 238 patients(21,22,24,25) after 24 hours, 2–4 days, and 10 days of treatment. The PaCO2 analysis included data obtained from 152 patients(21,22,25) after 24 hours, 2–4 days, and 7–10 days of treatment.
Methodological quality of the included studies
The five parallel trials all had an acceptable level of bias as reflected by satisfying ≥2 bias criteria (Fig. 2). Two of the included studies(21,24) clearly utilized a randomization sequence, and two other included studies(21,23) employed methods for allocation concealment. All included studies utilized a double-blind protocol design and accounted for lost patients (no loss of patients),(25) and no study showed evidence of reporting bias.

Quality of the included studies.
Results of pooled analysis
When compared with SCs, the pooled results showed a noninferiority trend for ICSs regarding changes in FEV1%pred, SaO2, PaO2, and PaCO2 during their use in the treatment of COPD exacerbations. Detailed results of the pooled analysis are presented in Figures 3–6.
Analysis of FEV1pred data
Both ICSs and SCs produced salutary effects on lung function, and the pooled result for FEV1%pred showed a nonsignificant difference in both groups (ICS and SC). As compared with the SC group, the weighted mean difference in patients treated with ICSs was 1.84% predicted (95% CI: −1.60 to 5.28; Fig. 3) and was without significant heterogeneity (Pheterogeneity = 0.72, I2 = 0.0%). This result was consistent across all three RCTs included in this meta-analysis.(22,23,25)

Effects of ICSs on FEV1%pred in the treatment of COPD exacerbations compared with the effects of SC after treatment for 7 days. CI, confidence interval; COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; IV, inverse variance; SC, systemic corticosteroid.
Analysis of blood gases
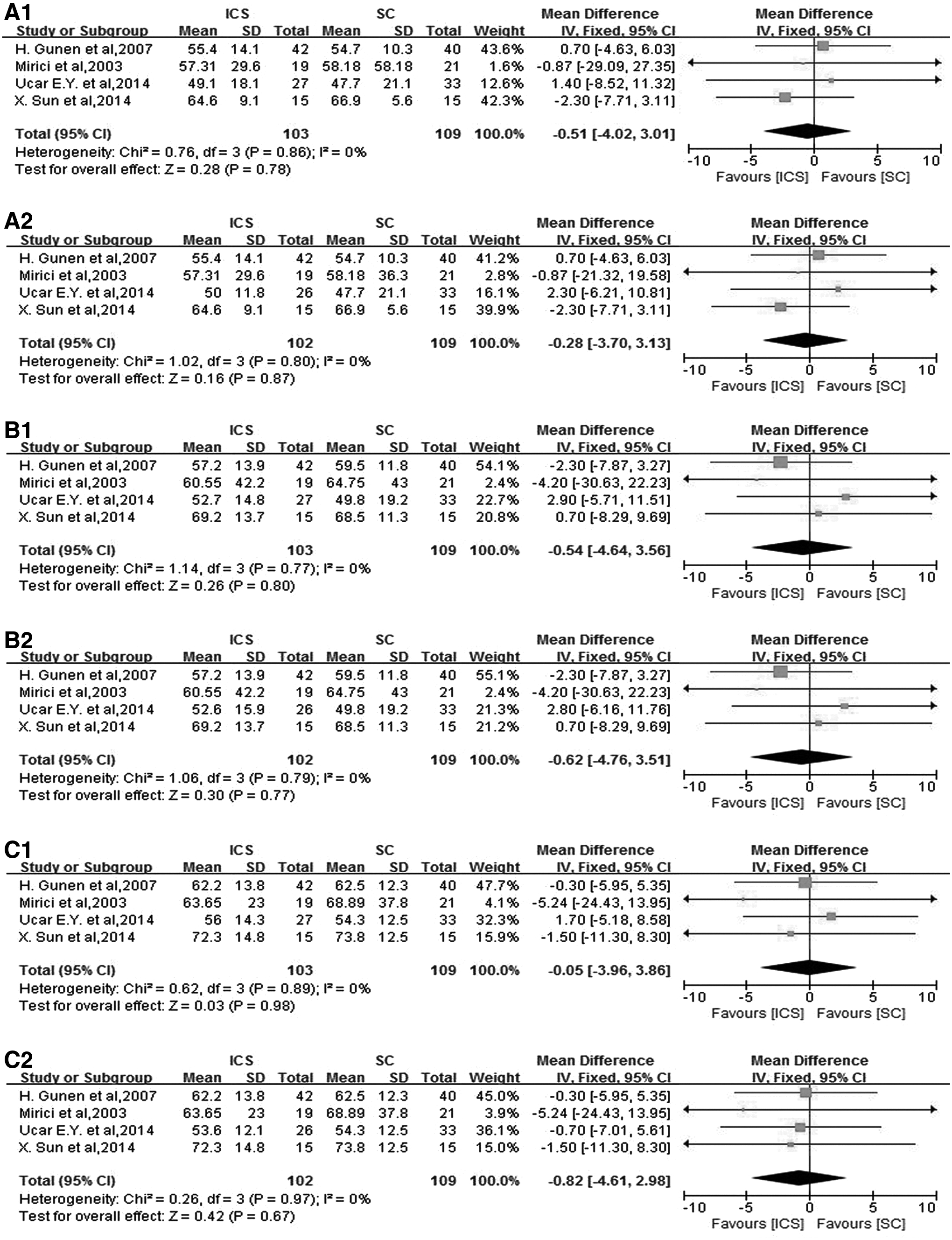
We next investigated changes in the results of blood gas analyses in four RCTs,(21,22,24,25) and we separated the pooled results for PaO2, PaCO2, and SaO2. We divided the data into three groups that were designated as “results after treatment” for 24 hours, 2–4 days, and 7–10 days, respectively. As the therapeutic dose of ICS was divided into categories of 4 mg and 8 mg in the RCTs reported by Yilmazel Ucar et al.,(24) the analyses of SaO2 and PaO2 were separated as shown in Figures 4 and 5.
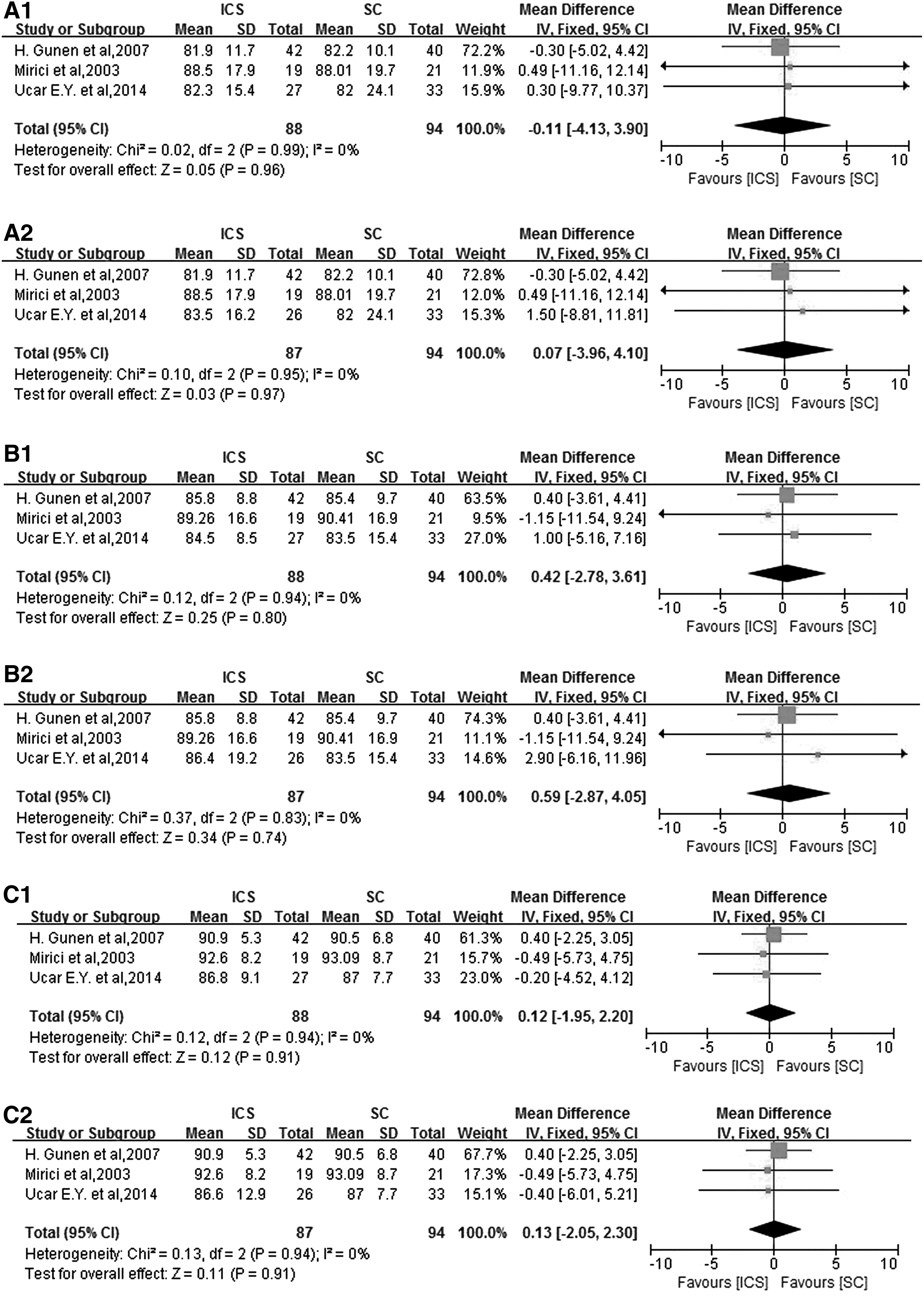
Effects of ICSs on SaO2 in the treatment of COPD exacerbations compared with SCs at 24 hours control
Effects of ICSs on PaO2 in the treatment of COPD exacerbations compared with SCs at 24 hours control
Three(21,22,24) out of the five RCTs reported an increase in SaO2 after treatment with either an ICS or an SC. The pooled result for SaO2 showed a non-significant difference in both groups in a fixed-effects model without significant heterogeneity. The final results are shown in Figure 4.
Both ICSs and SCs increased the PaO2 of patients included in the RCTs.(21,22,24,25) After treatment for 24 hours, 2–4 days, and 7–10 days, the heterogeneity for PaO2 was statistically nonsignificant, and the same increasing trends were found in a fixed-effects model. The exact results are shown in Figure 5.
Our analysis showed that PaCO2 decreased and non-revealed heterogeneous effects (Pheterogeneity = 0.82, I2 = 0% vs. Pheterogeneity = 0.95; I2 = 0% vs. Pheterogeneity = 0.92, I2 = 0%) in three RCTs.(21,22,25) When using a fixed-effects model, the pooled result failed to show differences in PaCO2 after treatment for 24 hours, 2–4 days or 7–10 days. The exact results are shown in Figure 6.
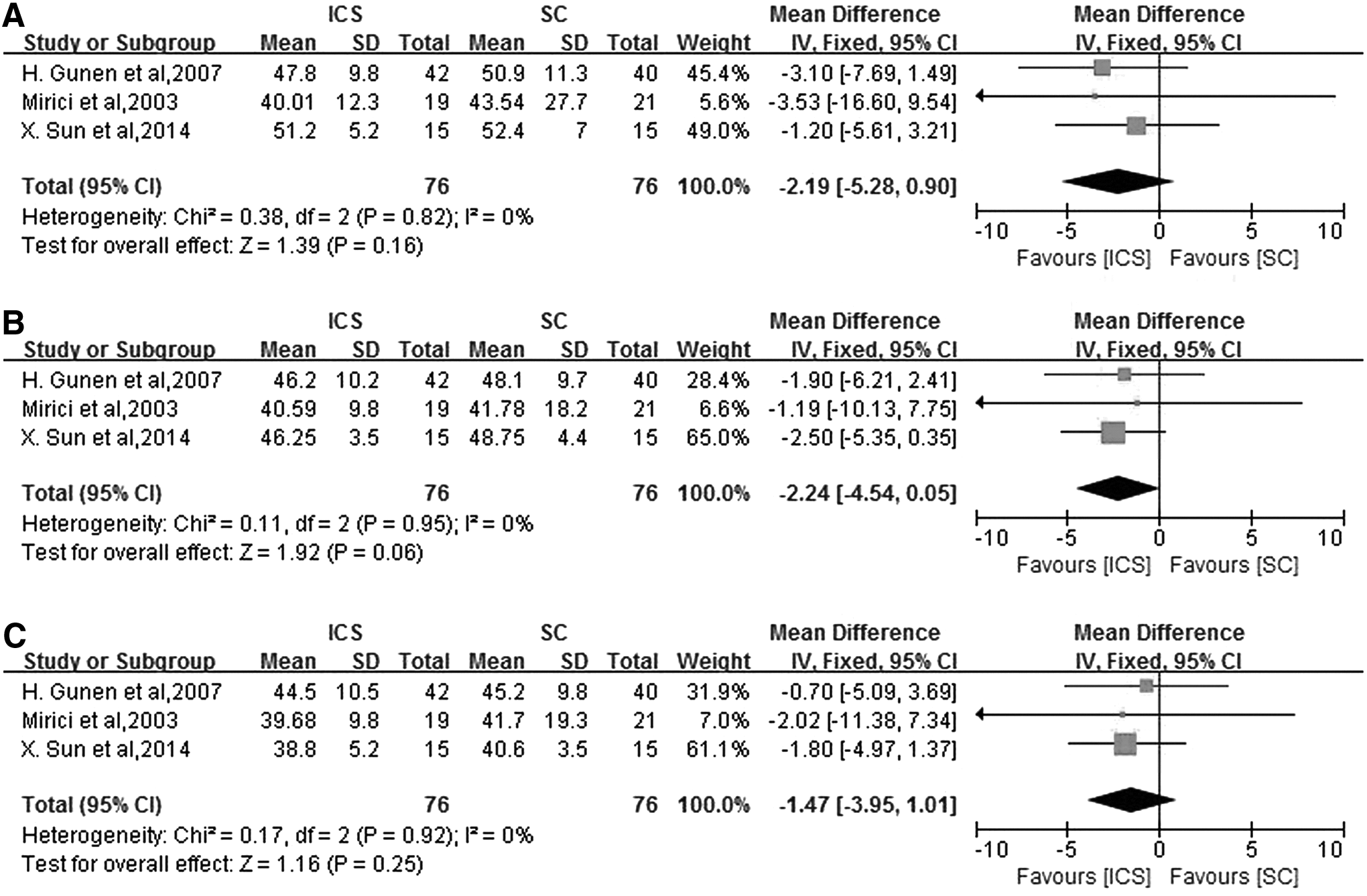
Effects of ICSs on PaCO2 in the treatment of COPD exacerbations compared with SCs at 24 hours control
Because a maximum of four studies were included in our analysis for FEV1%pred and blood gas analyses, further analyses for publication bias and sensitivity were not performed, as the information would not be meaningful.
Discussion
Our meta-analysis showed that ICSs were noninferior to SCs in the treatment of COPD exacerbations. No significant differences regarding the effects of ICSs and SCs were seen in our analyses of SaO2, PaO2, PaCO2, or FEV1%pred. Lung function blood gas analyses are important indicators of respiratory function.
In addition to the indicators cited earlier, other relevant markers were also examined in the included studies. Morice et al. showed that there were no differences in the improvement of FEV1 between budesonide and prednisolone (1.8–2.1 and 1.9–2.0 L for SC and ICS, respectively) after treatment for 5 days.(19) FEV1 values were also measured in the study by Maltais et al. In their study, the difference in FEV1 [0.06 L; (range 0.14 L vs. 0.02 L)] after treatment with an ICS or an SC was not statistically significant,(20) which was similar to Morice et al.'s results. In the study by Mirici et al., values for PEFR (peak expiratory flow rate) and pH were measured at 30 minutes, 6 hours, 24 hours, 48 hours, and 10 days, and no significant differences were found regarding the percentage change in PEFR (p = 0.75) or pH values (p = 0.81) during the entire period of assessment.(21)
In addition to lung function and blood gas analyses, some clinical indicators also supported the noninferiority between the treatment of ICS and SC groups. In the RCTs reported by Yilmazel Ucar et al., the reductions in Borg scale ratings in both the ICS and SC groups were shown to be statistically significant; however, the difference between the two groups in a direct comparison was not statistically significant (p = 0.34). Similarly, the mean duration of hospitalization for the two groups was also not significantly different (p = 0.74).(24) Patient symptom scores and total CCQ scores were compared in the RCTs reported by Ställberg et al., and there were no statistically significant differences between the ICS group and SC group regarding total CCQ scores or subgroup scores for function, mental health, and symptoms.(23)
However, such results were only found in one or two studies, which make their value somewhat limited and contingent on further confirmation.
Exacerbation contributes to an increased inflammatory response and the levels of TNF-a, IL-8, and hs-CRP are higher in these patients. Sun et al. focused on these indicators and found that there were no significant differences in the levels of IL-8, TNF-a, and hs-CRP in ICS and SC groups (p > 0.05).(25) These data supported the non-inferiority of ICSs vs SCs when used to relieve airway inflammation.
In contrast, some indicators did show significant differences between ICS and SC groups. Sun et al. and Gunen et al. conducted studies that showed different values for FEV1/FVC. In the study conducted by Gunen et al., the rate of improvement in FEV1/FVC became statistically significant after 10 days of treatment only in the ICS group (p = 0.019), whereas there was no difference between groups in the study conducted by Sun et al.
In a study conducted by Gunen et al., values for forced vital capacity (FVC) and FEF25–75%%pred were measured at baseline and again after treatment for 24 hours, 72 hours, 7 days, and 10 days. At 24 hours, improvements in FVC became statistically significant in the ICS group (p = 0.032), whereas values for mean forced expiratory flow between 25% and 75% of FVC (FEF25–75%) in the SC group were significantly higher than those in the ICS group (p = 0.03).(22) This difference in outcomes suggests that the hypothesis that ICSs and SCs produce the same acute flares in the initial stage of COPD exacerbations remains to be confirmed.(22)
We also analyzed adverse events in our meta-analysis. Except for the study reported by Mirici et al. and Ställberg et al., data regarding adverse effects in other studies showed differences between SC and ICS groups.
The study by Morice et al. used changes in values for biochemical variables to evaluate adverse effects after treatment for 5 days. Mean values for urinary corticosteroid metabolites, serum osteocalcin, and 24-hour urinary calcium/creatinine ratios were significantly different in an ICS group compared with an SC group (p < 0.05); however, values for urinary androgen metabolites and urinary hydroxyproline-to-creatinine ratios were similar in both groups.(19)
In a study reported by Maltais et al.,(20) budesonide showed little systemic activity, whereas a higher incidence of hyperglycemia was observed in a prednisolone group.(20) Gunen et al. reported blood glucose levels in their study, and they showed that absolute blood glucose levels were significantly higher in an SC group (p < 0.05).(22) A study by Sun et al. found fewer adverse events (abnormal heart rate, blood pressure, glycemia, sleep problems, gastrointestinal symptoms) in an ICS group when compared with an SC group (p < 0.05).(25)
In addition, in the studies mentioned earlier, patients who switched from an SC to an ICS experienced fewer adverse events. Only systemic adverse effects, and not local adverse effects, were observed in the studies included in our meta-analysis. It is possible that symptoms such as cough, dry mouth, ulceration, and hoarseness were caused by overlaid ICSs.
Limitations
From a statistical standpoint, the small number of studies included in our meta-analysis eliminated the need for any additional analyses of sensitivity or publication bias, as the results would not be useful. In addition, some important data in the five studies were not directly reported in the text of the paper, and they had to be obtained by reading the figures in the manuscript. Finally, some basic statistical formulas were used to calculate the data for our analysis, and this introduces a certain amount of error.
Regarding therapeutic efficacy, many aspects of patient outcome were only mentioned in one or two studies, which makes it difficult to definitely prove a certain result. In addition, none of the five RCTs reported long-term follow-up data, and thus, the comparative long-term effects of ICSs and SCs remain unknown. Only one study(24) thoroughly addressed the dosage of ICS, thus we could not reach conclusions regarding the effects of high doses versus low doses of ICSs. Finally, different ICS formulations were used in the different studies, and it is unknown whether this may have affected the study results.
Conclusion
In summary, the present meta-analysis suggests that ICSs are not inferior to SCs when used for the treatment of COPD exacerbations. Despite the few studies analyzed and the different dosages used in these trials, the results of RCTs suggest that an ICS can be considered an alternative to an SC, because the two types of dosage forms appear equally effective, and ICSs produce fewer systemic adverse effects. Further studies should be conducted to identify the effects of ICSs on other relevant clinical and inflammation markers. The optimal dosage form for use in treating an AECOPD needs to be clarified.
Footnotes
Acknowledgment
The authors would like to thank the Health and Family Planning Commission of Liaoning Province for funding source with the No. LNCCC-D14-2015.
Authors' Contribution
Y.Z.: Study design, data acquisition, data analysis, article drafting, critical article revision, and final article approval. H.Z., T.S., and M.Y.: Data acquisition, data analysis, and final article approval. H.L.: Data analysis, critical article revision, and final article approval. R.Z.: Study design, critical article revision, and final article approval.
Author Disclosure Statement
The authors have stated explicitly that there are no conflicts of interest in connection with this article. The Health and Family Planning Commission of Liaoning Province has acted as a paid consultant to R.Z. and has received funding for research carried out in this work (No. LNCCC-D14-2015). All authors read and approved the final article.