
Abstract
Abstract
Background:
Dr. Nelson's Improved Inhaler was first marketed with an advertisement in The Lancet in 1865. Revolutionary at the time for its ease of use and patient-friendliness, the inhaler is still in use for self-treatment by many all over the world. On the occasion of its 150th anniversary, this study reports an experimental historical medicine approach to identify evidence for the quality of vapor inhalers.
Methods:
Through accessing reviews of the device's use by the contemporary medical establishment, it was established that Dr. Nelson's Inhaler enjoyed a reputation of quality and efficacy among reputable physicians generating empirical evidence of clinical performance. There was a general absence of product performance tests during this period. Therefore, modern inhalation performance testing was applied to test the aerosol delivery performance for Friars' Balsam, and its key chemical constituent, benzoic acid (BA).
Results:
A respirable dose of 59.9 ± 9.0 μg of BA was aerosolized in a 10 minutes period from a dose of 3.3 mL Friars' Balsam (equivalent to 35.1 ± 0.2 mg of BA) in 375 mL of steaming water using the glass twin stage impinger at a flow rate of 60 L·min−1. The respirable dose from a standardized aqueous BA inhalation formulation increased from 115.9 ± 10.6 to 200.2 ± 19.9 μg by increasing the simulated inhalation period from 5 to 10 minutes. When tested with a simulated inhalation maneuver (500 mL tidal volume, 13 minutes−1 respiration rate, 1:2 inspiratory:expiratory ratio) a respirable dose of 112.8 ± 40.3 μg was produced.
Conclusions:
This work has highlighted the potential for aerosol drug delivery using steam inhalers that are popular with patients. Physicians should therefore be aware of the potential for lung dosing with irritants when patients self-medicate using the Nelson Inhaler with vaporizing formulations such as Friars' Balsam.
Introduction
I
British (Victorian) physician-inventors were introduced to inhalation anesthesia from Boston (United States) in 1846–47, which served likewise to normalize perceptions of inhaled medicines and accelerate the exploitation of new materials (e.g., rubber and basic plastics) from the empires. This also helped to industrialize the production of steam-based inhalers and pneumatic atomizers, which were at that stage being developed across France, Germany, and Britain. Increasingly steam-based inhalers were being used for treating diseases like bronchitis, croup, and catarrh that accompanied the transition to industrial and urban modes of living.
It was against this backdrop that the increasing awareness of pulmonary drug delivery in the medical press and the general demand for effective respiratory treatments congenially aligned in one of the least spectacular, but most successful pharmaceutical inventions of the period: Dr. Nelson's Ceramic Inhaler (Fig. 1). The inhaler was presented at a meeting of the Royal Medical and Chirurgical Society on May 28, 1861.(6) Its introduction to the market in 1865 by S. Maw & Son Co. from their London base in Aldersgate Street (following their introduction of various patented inhalers at the International Exhibition of 1862) heralded the acceptance in 1867 of inhalants for the first time in the British Pharmacopoiea.(7) Dr. Nelson's Inhaler was featured in The Lancet, The Medical Times and Gazette, and the British Medical Journal and became popular with self-medicators and professional physicians alike.(2,8–12) Of the contemporary reviewers, William Abbotts Smith working in the Finsbury Dispensary and the Metropolitan Free Hospital (London), recommended the device on the back of empirical experience in a clinical environment.
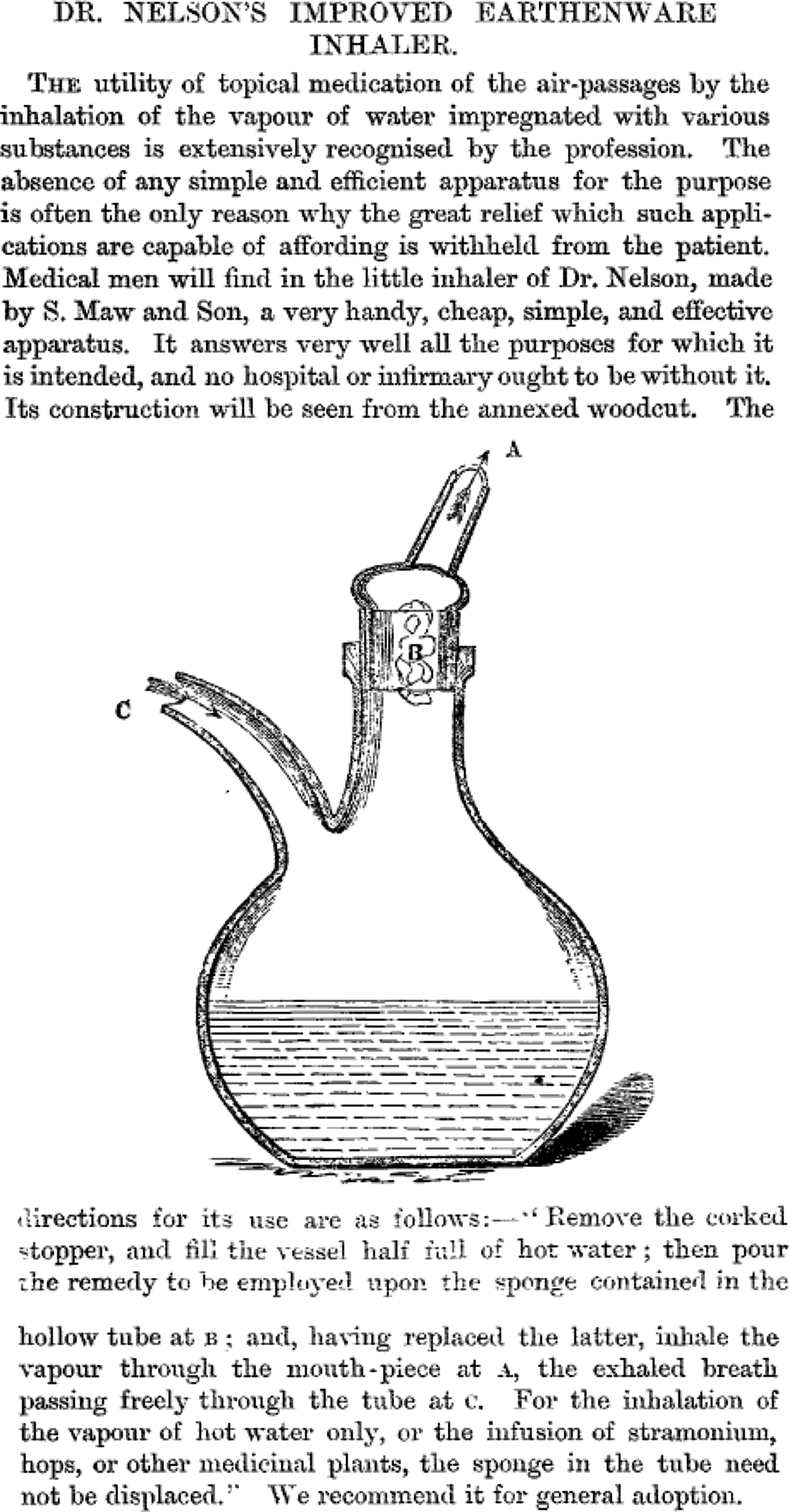
The debut of Dr. Nelson's Inhaler in The Lancet (1865).(36)
Steam inhalers were replaced in conventional respiratory medicine by modern inhaler devices from the mid-20th century.(13) However, steam inhalations remained in popular use for ameliorating chronic bronchitis throughout the 20th century,(14) and these are recommended by healthcare practitioners across the world in the 21st century.(15) Dr. Nelson's Inhaler is still produced today, although it is now more usually used by singing coaches and performers including Ella Henderson, Sam Smith, and Prof. Green.(16–18) Vapor-steam inhalations are one of the most frequently self-prescribed products for those with asthma(19) and in other pulmonary conditions such as the common cold, although there is little available evidence to support this latter use.(20) Indeed the risks of burns and scalds when using steam inhalations may outweigh any therapeutic benefit.(21,22)
Steam inhalations were not universally trumpeted and the effectiveness of the formulae of the British Pharmacopoeia was questioned in the academic press at the time.(23) Hassall challenged the use of vapor inhalants based on meticulous experiments. In his critique he anticipated that there would be improvements to inhaler devices; however without the availability of modern analytical techniques, experimentation and device development were pragmatic and empirical. It is possible that the paucity of evidence for vapor inhalants arises from the poor quality standards and inability to test for their effectiveness at the height of their use, or device inefficiencies for otherwise effective medicaments. Indeed vapor inhalation has witnessed resurgence in recent years with the advent of e-cigarettes.
With the use of vapor inhalations remaining common in self-administered pulmonary care, it is of interest to ask what modern analysis makes of the quality of vapor inhalers. Coinciding with the 150th anniversary of Dr. Nelson's Inhaler, the aim of this research was to examine whether an experimental history of science approach could offer evidence for the quality of historical therapies discounted by modern medicine.(24) The approach included applying modern pharmaceutical performance testing of vapor inhalants of relevance to both historical and contemporary respiratory therapies.
Methodology
Experimental history of science approach
The history of medical therapies increasingly focuses on the pragmatic and material dimensions of the subject,(25–27) using both literary (e.g., journal articles, patents, etc.) and nonliterary components in its understanding of medical history. Pharmacy has always been a practical, hands-on form of production, experimentation, and provision of medical therapy, and is an ideal field in which to promote the experimental history of science approach. In terms of a history of pharmaceutical therapies, this means combining traditional methods of historical analysis (including the theoretical and conceptual knowledge recorded in pharmacopoeia and formularies, advertisements, prescriptions, medical publications, and contemporary literature or popular press) with the identification of the experimental capabilities of the time (e.g., available analytical techniques), and the nature of pharmaceutical materials themselves (i.e., therapeutic use, efficacy and side-effects).(28)
In one experimental approach medicines are reconstructed according to historical sources before being analyzed according to current forms of analysis.(29) In this respect vapor inhalations represent an excellent case study, since several remedies are still widely available as over-the-counter products or as (now-regulated) herbal medicines of traditional use, which, although not allopathic, are still widely used in respiratory self-management.
A survey of historical literature and correspondences relating to Dr. Nelson's Inhaler, the history of S. Maw and Sons, and clinical, commercial, and advertising resources referring to the treatment of pulmonary diseases was conducted using online and print archival materials at the Bodleian Library, the Wellcome Library, the British Library, the Science Museum (London), and the BMJ Publishing Group Archives. These included the British Pharmacopoeia, Proceedings and Transactions of the learned societies including the Royal Medical and Chirurgical Society (now the Royal Society of Medicine), Royal College of Surgeons of Edinburgh, Royal College of Surgeons of England (RCSEng), reports on clinical studies, and medical handbooks for specialist and popular readership, historical advertisements, and medical ephemera.
Survey of these textual sources furthermore enabled identification of historical medicaments widely in use, some of which (e.g., hydrocyanic acid) were disregarded as too toxic by contemporary standards to be considered worthwhile testing, leading to the choice of Friars' Balsam for in-depth analysis. Although the actual preparation analyzed was modern, comparison with historical instructions for preparation of ingredients (e.g., Tinctura Benzoini Composita in the British Pharmacopoeia of 1867) was important in the choice of analyzed product. While some approaches to this experimental historical approach attempt to recreate actual historical experimental and testing conditions, literary sources (as Hassal's contemporary criticism shows) revealed a lack of any such stringent testing, meaning that the model of experimental history subsequently used in this study involved the deployment of modern testing methods.
Experimental performance testing of Dr. Nelson's Inhaler
A Dr. Nelson's Improved Inhaler (medium size) was purchased from John Bell & Croydon (London, United Kingdom) to assess the drug delivery performance of Care™ Friars' Balsam (Thornton and Ross, Huddersfield, United Kingdom) in a glass twin stage impinger (TSI) (Copley Scientific Ltd., Nottingham, United Kingdom). This instrument enables the determination of the nonrespirable (on Stage 1), and the respirable dose (i.e., the amount of drug emitted from an inhaler with an aerosol size below 6.4 μm, on Stage 2) of an inhalation product.
Briefly, a standardized inhalation formulation was prepared containing 3.3 mL of Friars' Balsam in 375 mL of steaming hot water (heated to 90°C). The latter concentration is in accordance with instructions to add 5 mL of tincture to 1 pint of water. The inhaler was connected to the prepared TSI using a rubber adaptor, and the impinger was operated using an airflow rate of 60 L·min−1 for 10 minutes. The TSI was cooled for 30 minutes over ice, and maintained over ice to prevent postdeposition evaporation of the volatile components. Following completion of the standard “inhalation,” the dose of Friars' Balsam emitted into the TSI was determined using a validated reversed phase high performance liquid chromatography ultraviolet (HPLC-UV) method calibrated for the principal chemical component of Friars' Balsam, benzoic acid (BA). Analytical standards of BA were purchased from Sigma Aldrich (Poole, United Kingdom), and HPLC-grade reagents (methanol, ethanol, and ammonium acetate) were purchased from Fisher Scientific (Loughborough, United Kingdom). The Friars' Balsam was itself standardized for BA content using the HPLC-UV quantification.
To assess the influence of patient use on the drug delivery performance, a standardized inhalation formulation of BA in hot water was prepared. A simulated tincture in accordance with the composition of the British Pharmacopoeia (2014) Benzoin Inhalation was prepared by dissolving BA in ethanol (1.875 g in 50 mL). Five milliliters of this solution was added to 375 mL steaming hot water as above. The drug delivery performance of the inhalant was assessed as above, but with operation of the TSI for 5 or 10 minutes duration, respectively.
Finally, the most onerous test of the Dr. Nelson's Inhaler for delivery performance of the standardized BA formulation was performed using the Copley BRS 3000 inhalation simulator with a fast screening twin stage impactor (FSI) and mixing inlet (both from Copley Scientific, Nottingham, United Kingdom). The FSI was cooled with ice packs for 30 minutes and maintained wrapped in ice packs to prevent postdeposition evaporation of the volatile components. Rather than a continuous airflow, the “inhalation” of a patient through the device was simulated using the Canadian Standard adult sinus breathing profile (500 mL tidal volume, 13 minutes−1 respiration rate, 1:2 inspiratory:expiratory ratio) for a 10 minutes test period.(30) The nonrespirable and respirable doses of BA were determined by HPLC-UV, as above. In the case of the FSI, the respirable dose is retained on a glass fiber filter trap, and corresponds to an aerosol size below 5 μm.
Results
Historical evidence of quality for Dr. Nelson's Inhaler
At the conclusion of a meeting of the Royal Medical and Chirurgical Society (RMCS) on May 28, 1861, a certain Dr. Nelson presented an inhaler (Fig. 1), “its claims to notice being, great ease and simplicity of action; perfect cleanliness; and an arrangement of the mouthpiece by which is secured economy in the use of any medicated ingredient that may be required for inhalation.”(6,7) It is of interest that the presentation noted issues that remain of concern in modern inhalation therapy, namely the requirement for simplicity and ease of use by the patient to minimize errors of use. The inhaler was manufactured by Maw & Sons, a company at the forefront of manufacturing and supplying medical equipment to British hospitals and medical practitioners in Victorian Britain. Its reputation was such that it was featured in the 1862 Exhibition,(7) where coincidentally a range of its ceramic inhalers were displayed.
The mid-19th century is usually reconstructed with the narrative of Victorian Britons developing quality, safety, and evidence concepts in medical therapy. For example, the Medicine Act of 1802 and the Apothecaries Act of 1815 exerted control over the practice of medicine. Likewise, the formation of the Pharmaceutical Society in 1841 and the Pharmacy Act of 1868 limited the activity of apothecaries and druggists to registered individuals.(31) However, despite this narrative, evidence of testing and regulating the efficacy of volatile medicaments (including those of the Pharmacopoeia) and related apparatuses is rare. In many cases, evidence can be derived from empirical findings gained through limited published medical case histories.
Successful experiments by James Young Simpson in Edinburgh (1830s and 1840s) confirmed the ability to generate pharmacological affects by inhalation and Scudamore performed clinical trials of inhalation in respiratory patients “to show that they are capable of exerting a very important and beneficial influence in certain states of pulmonary and bronchial disease.”(32) Albert Hill Hassall's study in the BMJ (although notably, not including Dr. Nelson's Inhaler) criticized the efficacy of three of the five Pharmacopoeia inhalations as being “infinitesimal, and may be said to be homeopathic.”(23) It is notable that the designs of Dr. Nelson's Inhaler (Figs. 1 and 2) lack many of the features that Hill Hassall criticized for the devices he tested, and device performance was also affected by the poor formulation design at the time.
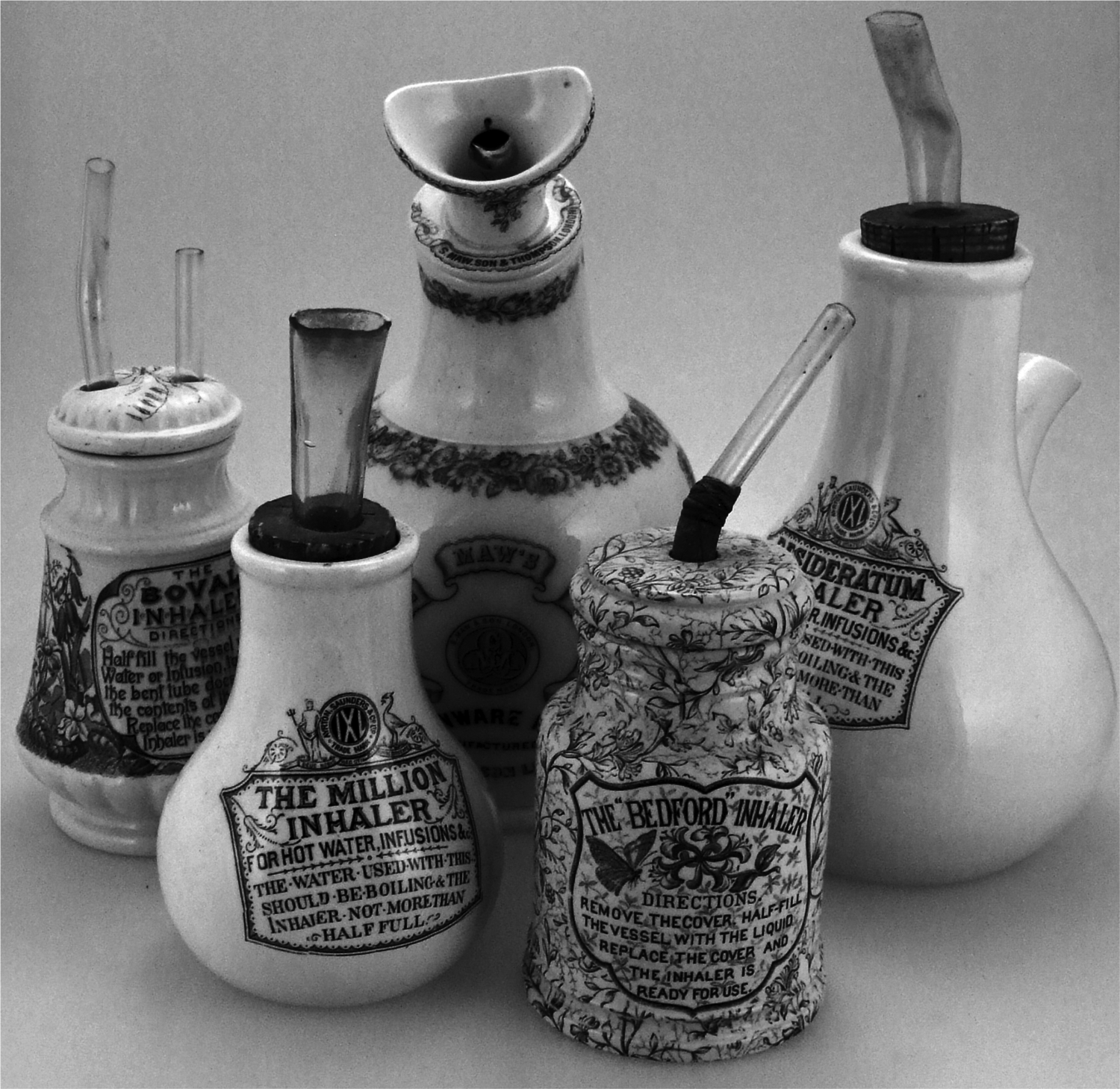
A collection of the many design copies and modifications of the Original Dr. Nelson's Inhaler from throughout the Victorian era, demonstrating the continued simplicity of device construction, as praised by contemporary reviews.
Experimental examination of the functional performance of Dr. Nelson's Inhaler
HPLC analysis of the Friars' Balsam revealed the content of BA in the proprietary product to be 10.64 ± 0.07 mg/mL of tincture (i.e., 1.06% w/v). Therefore, the total dose formulated as the steam inhalation was 35.11 ± 0.23 mg of BA. The TSI contains a solvent trap to capture the total aerosol that enters the apparatus. However, the performance testing revealed that only 130.8 ± 14.7 μg of BA was emitted from the Nelson's Inhaler into the TSI as an aerosol (i.e., ∼0.37% of the total available BA dose). The dose of BA with an aerosol size suitable for deposition in the lungs (i.e., <6.4 μm) was 59.95 ± 9.00 μg following 10 minutes of simulated inhalation at 60 L·min−1. It is of note that this corresponded to 45.7% ± 2.9% of the total emitted aerosol.
BA was selected as an appropriate marker compound for further mechanistic study, since it was the only compound appearing in the Friars' Balsam HPLC-UV chromatograms that was also observed in the samples of aerosol depositing in the TSI. The deposition profile and performance metrics for steam aerosolization of the BA tincture are presented in Figure 3. The respirable dose (fine particle dose in Fig. 3) was higher following 10 minutes compared to 5 minutes of operation (p < 0.05), however, the respirable fraction was unaffected by the aerosolization airflow (p > 0.05 for 5 minutes vs. 10 minutes of operation). This indicted that the aerosolization process would be consistent between patients, consistently delivering a high fraction suitable for deposition in the lungs of the user (∼45%).
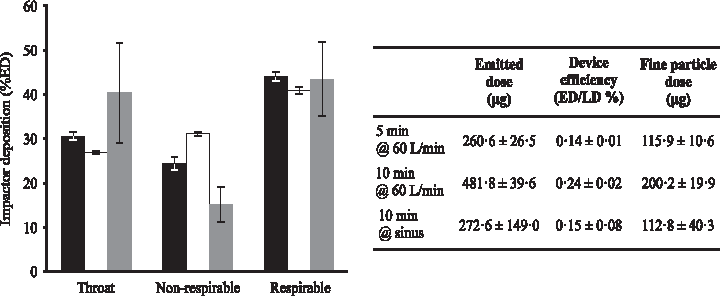
Deposition profile and performance data for benzoic acid inhalation aerosolized using Dr. Nelson's Inhaler in the twin stage impinger with an airflow of 60 L·min−1 for 5 minutes (black), 10 minutes (white), and in the fast-screening impactor with a human sinus breathing profile for 5 minutes (gray). Deposition profiles are presented as a percentage of the total ED, LD is the loaded dose in the inhaler, and the data represent mean ± SD, n > 3 for each condition. ED, emitted dose.
Operating the inhaler for 10 minutes at 60 L·min−1 provided a statistically significant doubling of device efficiency and fine particle dose compared to 5 minutes operation, indicating that duration of inhalation and total inhaled volume are the key patient-use factors affecting the dose inhaler performance. Statistical analysis of the performance data (ANOVA and post hoc Tukey's testing) demonstrated no difference between the emitted dose, device efficiency, or fine particle dose for the 5 minutes (60 L·min−1) and 10 minutes (sinus breathing) conditions, generally derived from the high variability in the simulated inhalation testing.
Discussion
This study sought to identify remedies employed during the age of the steam inhaler, on which basis, tincture of benzoin(33) was chosen due to its widespread use as an expectorant at this period. The most commonly available form of this particular therapy to emerge from our literature review was Friars' Balsam.(1,34) It is interesting that Friars' Balsam as a volatile inhalant provides an unbroken link to the period when Dr. Nelson's Inhaler was invented. Although a prescribed therapy in the 19th century, it retains a place as proprietary products in self-care and has an undiminished popular reputation.
Despite the fact that there was a low overall efficiency of drug aerosolization from the inhaler, the fine particle fraction of the emitted dose (45.7% ± 2.9%) compares favorably with many modern dry powder and pressurized metered dose inhalers. The key issue appeared to be the inefficiency of aerosol emission from the steam inhaler—an issue that could be addressed, for example, through improved entrainment and air-liquid mixing within a vapor device. The difference in throat and nonrespirable deposition fractions for the TSI and FSI-breath simulator derive from the different construction of the test equipment. Nevertheless, using modern pharmaceutical performance testing approaches, it has proved possible to generate a dose of BA suitable for lung deposition from Friars' Balsam using Dr. Nelson's Inhaler.
When inhalations entered the British Pharmacopoeia of 1867, there was some scepticism as to their medical efficacy and safety. It is questionable whether the lack of clinical success for steam inhalations derived from the questionable pharmacology of the agents (e.g., hemlock), the poor delivery performance of the devices, or both.(23,35) Dr. Nelson's Inhaler, on the other hand, is conspicuous by the clinical success it was said to have had. It was successful among professionals (one only needs to examine the variety of copies that emerged under various commercial brands over the years) and essentially “peer reviewed”: the clinical benefits of the device were praised by various physicians, from Spencer Thomson's Dictionary of Domestic Medicine to William Abbotts Smith's On Affections of the Throat and Lungs.(11,12) In this work, it has been demonstrated that Dr. Nelson's Inhaler can produce an inhalable dose of volatile organic agents typically employed (mainly) in self-care of respiratory infections, and hence a contribution has been made toward understanding its popularity among lay and medical communities in the second half of the 19th century.
Conclusion
Some 150 years after the Dr. Nelson's Inhaler was introduced onto the market, this work has constructed historical evidence for the clinical efficacy and usability of the inhalation device in pulmonary medicine. Furthermore, it has demonstrated for the first time, using testing approaches unavailable when steam inhalers were being rejected by clinical medicine (1880–1900), proof of the delivery of a dose with properties suitable for deposition in the lungs. The findings of this article should not be construed as an attempt to ignite resurgence in the clinical use of volatile inhalants using Nelson's Inhaler. Nevertheless, clinicians should be aware of the potential for lung deposition in patients who self-medicate with steam inhalations that contain irritants such as BA, including the Dr. Nelson's Inhaler.
Footnotes
Author Disclosure Statement
No competing financial interests exist.