
Abstract
Abstract
Background:
Preclinical evaluation of new chemical entities (NCEs) designed to be administered by inhalation route requires lung administration to rodents, especially in the discovery phase. Different administration methods have been used until now, but more efforts are required to obtain controlled and reproducible lung deposition when only small amounts of neat powder material are available.
Methods:
The PreciseInhale platform used in the present study enables well-controlled powder aerosol exposures with only small amounts of micronized neat material, providing data on inhalation pharmacokinetic (PK) of NCEs at a very early stage. The DustGun aerosol technology uses compressed air to generate a respirable aerosol from milligram-amounts of powder that is delivered to one animal at a time. The new methodology was used to investigate the inhalation PK and lung retention in the rat of the novel Chiesi PDE4 inhibitor CHF6001 in three exposure models of the PreciseInhale platform: nose-only, intratracheally intubated rat, and the isolated, ventilated, and perfused rat lung. Results were compared with data from two other pulmonary delivery systems commonly used in preclinical studies: liquid instillation and powder insufflation.
Results:
Administration of micronized CHF6001 using the PreciseInhale system yielded lung exposures in the same range as the other tested devices, but the reproducibility in lung deposition was improved. The initial amount of CHF6001 in lungs at the first sampling time point was close to the predetermined target dose. Tracheal deposition with PreciseInhale (0.36 ± 0.22 μg) was significantly less than with other tested delivery systems: PennCentury (23.7 ± 3.2 μg) and Airjet (25.6 ± 7.2 μg).
Conclusions:
The PreciseInhale platform enabled the administration of CHF6001 powder with good accuracy and reproducibility, with low tracheal deposition. The new platform can be used at an early discovery stage to obtain inhalatory PK data for respirable aerosols of neat NCE powder without excipients and with minimal use of dry powder formulation work.
Introduction
I
Liquid formulation of new chemical entities (NCEs) can be obtained by using solubilizing excipients and delivered by intratracheal (IT) instillation or nebulization to anesthetized animals.(4) These methods require a low amount of substance, but are characterized by uneven distribution of the formulation in the lung and poor dose control.(5) Furthermore, liquid formulation is often different from the formulation that will be tested in the development phase, and the data obtained with these methods could be poorly predictive of the pharmacokinetic (PK) profile of the powder formulations. The excipients used for compound solubilization and suspension could affect lung absorption and their effect is often unknown.(6–8)
Improvement in lung distribution can be obtained by IT administration of dry powder (DP) formulation using the PennCentury™ device.(9–12) The disadvantage of this method is a greater powder deposition in the large airways compared to the lung,(13) yielding an increment in the swallowed fraction and consequently in gastrointestinal (GI) absorption.
Nose-only (N-O) exposure of groups of animals to powder aerosols can be performed using inhalation towers, where the animals are allowed to breath in a chamber where the aerosol is generated. This method is characterized by good reproducibility in lung deposition and the deposited dose can be calculated by measuring the aerosol concentration in the chamber during the experiment.(14) Nevertheless, the development of powder formulations for IT or N-O administration requires a large amount of substance, making these methods not suitable for the early drug discovery phase, when the NCEs are usually available only in small quantities.
The PreciseInhale® inhalation exposure platform was developed with the aim to allow well-controlled powder aerosol exposures with only small amounts of substance. It makes possible inhalation administration of a new compound as a respirable powder for PK characterization at a very early stage, making DP formulation not necessary. Moreover, the PreciseInhale system enables exposures with the same aerosol formulation of a range of preclinical models, from in vitro to in vivo. This platform is based on the DustGun technology,(15) which uses compressed air (up to 160 bar) to produce small volumes (300 mL) of concentrated respirable aerosol starting from a few milligrams of neat compound. The aerosol is immediately dispensed to one exposure subject at a time with the PreciseInhale active aerosol dosing system, which controls the inhaled dose by monitoring both aerosol concentration and ventilation rate of the exposed subject.(16)
In the present work, this new methodology was used during the early development of CHF6001, a novel selective phosphodiesterase 4 (PDE4) inhibitor identified in recent years by Chiesi Farmaceutici for inhalation administration in the treatment of respiratory diseases and currently under investigation in clinical Phase II studies.
Selective targeting of PDE4 represents a novel approach to the treatment of respiratory diseases associated with inflammatory processes such as asthma and chronic obstructive pulmonary disease (COPD). The intracellular levels of cyclic nucleotide second messengers are regulated by the phosphodiesterase (PDE) superfamily of enzymes.(17) Among the 11 PDE isoenzymes discovered to date, PDE4 is the primary cyclic adenosine monophosphate (cAMP)-hydrolyzing enzyme, expressed predominantly in inflammatory cells such as eosinophils, T lymphocytes, macrophages, neutrophils, and dendritic cells, which are all found in the lungs of patients with COPD and asthma.(18) The oral PDE4 inhibitors were proven efficacious in clinical studies, but the tolerability of these drugs was limited by mechanism-related side effects, particularly nausea, diarrhea, abdominal pain, vomiting, and dyspepsia.(19) Inhaled anti-inflammatory PDE4 inhibitors, such as CHF6001, would have minimal systemic impact and could show both improved therapeutic index and efficacy, compared to oral known PDE4 inhibitors.(20)
Lung PKs of CHF6001 [(S)-3,5-dichloro-4-(2-(3-(cyclopropylmethoxy)-4-(difluoromethoxy)phenyl)-2-((3-(cyclopropylmethoxy)-4-(methylsulfonamido)benzoyl)oxy)ethyl)pyridine 1-oxide] was widely investigated in preclinical species, performing both DP administration by the PennCentury DP-4 insufflator (Penn-Century, Inc., Wyndmoor, PA) and IT suspension instillation by the AirJet homemade device. In addition, more recently, CHF6001 lung PKs have been studied with the novel DustGun technology in well-established preclinical models.
The aims of this study were (1) to obtain early PK data with CHF6001 respirable powder aerosol in three preclinical models (the isolated, ventilated, and perfused rat lung exposed ex vivo, the rat exposed in vivo by the endotracheally intubated (INT), and the N-O inhalation methods) dosed with the PreciseInhale platform, and (2) to compare the CHF6001 PK data obtained in vivo after administration using the PreciseInhale platform with those obtained with other methods commonly used in preclinical lung administration such as IT powder administration by PennCentury and instillation of liquid suspension by the AirJet.
Materials and Methods
Generation and characterization of CHF6001 powder aerosol
The neat compound CHF6001, provided by Chiesi Farmaceutici S.p.A. (Parma, Italy) as a powder micronized to a particle size in the range of 2–3 μm, was used for aerosolization. The material was used with no further treatment.
Before exposures, the particle size distribution of the CHF6001 powder aerosol generated with the PreciseInhale (Inhalation Sciences Sweden AB, Stockholm, Sweden) was measured with a 9-stage Marple cascade impactor (MSP Corp., Shoreview, MN) at a final flow rate of 2 L/min.(21) The signal from a Casella Microdust Pro light dispersion instrument (Casella CEL, Inc., Buffalo, NY) was calibrated against the inhaled mass of the test substance using a corresponding in vitro filter test system for each preclinical model: the isolated, ventilated, and perfused rat lung (IPL) and the rat exposed in vivo by INT and N-O inhalation method, with the aim to directly perform accurate target dosing in the respective model without using animals for range-finding exposures.(16) The PreciseInhale system with the three preclinical exposure models used in the current study is shown in Figure 1.

The PreciseInhale® inhalation exposure platform with the three preclinical exposure models outlined: the IPL, and the rat exposed in vivo by either the INT or N-O inhalation methods. Before aerosol exposures, the upper part of the tracheal catheter or the restrainer tube is connected to the PreciseInhale platform, thus creating a closed system. The aerosol generation and delivery procedure are executed by the exposure control program using an active dose-control system. PN, the pneumotachograph; DG, the DustGun aerosol generator; MF, the end filter; V, the vacuum pump; Qtotal, the exposure airflow; Qvent, the ventilation airflow, generated by the breathing rodent lung; Qfilter, the constant component of the exposure airflow. The balance of the airflow streams at the three-way junction is expressed as Qtotal + Qvent + Qfilter = 0. INT, intratracheal; IPL, isolated, ventilated and perfused rat lung; N-O, nose-only.
Exposures of the IPL to CHF6001 powder aerosol
The experiments, carried out at Inhalation Sciences Sweden AB, were approved by the local ethics review board (Stockholms norra djurförsöksetiska nämnd, N256/09). Six female CD® IGS (International Genetic Standard) (Sprague Dawley) rats (Charles River, Sulzfeld, Germany), body weight (BW) 304 ± 20 g, were used.
For the IPL exposures ex vivo, the rats were euthanized with sodium pentobarbital (100 mg/kg, i.p.). Lungs were prepared as described elsewhere(22,23) and placed in the artificial thoracic chamber (Fig. 1). The lungs were perfused via the pulmonary artery in a single-pass mode, at a constant hydrostatic pressure of 12 cm of water. The perfusion medium was Krebs–Henseleit buffer (composition in mM: NaCl, 118.0; KCl, 4.7; CaCl2, 2.5; MgSO4, 1.2; NaHCO3, 13; KH2PO4, 1.2) also containing 5.5 mM glucose, 12.6 mM HEPES, and 4% bovine serum albumin, fraction V (standard grade). The buffer pH was maintained between 7.35 and 7.45. The temperature of the buffer and the artificial thoracic chamber was maintained at 37°C. The lungs were ventilated with room air at 75 breaths/min by creating an alternating negative pressure (−0.1 to −0.8 kPa)(24) inside the artificial thoracic chamber.
Except during the exposure episodes, tracheal air flow velocity and pressure inside the thoracic chamber were measured with a heated pneumotachograph (8430 Series, 0–3 L/min; Hans Rudolph, Kansas City, MO) and a differential pressure transducer (EMKA Technologies, Paris, France), respectively. The physiological lung function variables, tidal volume (Vt), dynamic lung compliance (Cdyn), and lung conductance (Gaw), were calculated online by a data acquisition system with the software IOX v. 6.1a (EMKA Technologies). The perfusate flow rate after passage through the lung (Qperf) was measured gravimetrically. Normal stability was achieved concerning all the physiological parameters measured. The lungs were allowed to stabilize for 30 minutes before aerosol exposures.
The baseline values were Vt, 1.9 ± 0.3 mL; Gaw, 122.7 ± 24.9 mL/s/kPa; Cdyn, 7.9 ± 2.1 mL/kPa; and Qperf, 27.1 ± 2.7 mL/min (average ± standard deviation, n = 6).
Two groups of three rat lungs were exposed ex vivo to target doses of, respectively, 10 and 100 μg CHF6001 deposited per lung (Table 1). After exposure, the lungs were maintained for a 120-minute perfusate collection period, during which perfusate samples were collected with a custom-made sample collector at the following time points: 1.5, 3, 4.5, 6, 7.5, 9, 10.5, 15, 30, 45, 60, 80, 100, and 120 minutes from the start of the aerosol exposure (t = 0). Immediately after the end of the perfusion period, the lungs were harvested for measuring the total amount of CHF6001 remaining in the lung and trachea. The trachea was dissected separately from the lung tissue and tissues were then weighed and frozen on dry ice. The lung perfusate and tissue samples were stored at −80°C until analysis.
Total powder amount loaded in the DustGun system to reach the target deposited dose.
INT, intratracheal; IPL, isolated, ventilated, and perfused rat lung; N-O, nose-only.
The quantification of CHF6001 in lung perfusate and tissue samples was performed by LC-MS/MS (liquid chromatography/tandem mass spectrometry; Pharm-analyt Labor GmbH, Baden, Austria). The lowest limit of quantitation (LLOQ) of the method was 0.03 ng/mL. The PK evaluation was performed as previously described.(16)
INT and N-O exposures of the rat to CHF6001 powder aerosol
The experiments, carried out at Inhalation Sciences Sweden AB, were approved by the local ethics review board (Stockholms södra djurförsöksetiska nämnd, S30-13).
For INT exposures in vivo, 33 male CD IGS (Sprague Dawley) rats (Charles River, Sulzfeld, Germany) with a BW of 258 ± 13 g at the day of the treatment were used. The animals were anesthetized with i.p. hypnorm+midazolam (solution containing 1 part H + 1 part M + 2 parts aq. pro inj., i.p. 0.27 mL/100 g BW), placed in supine position on an adjustable table, and endotracheally intubated under a good visual control using a PennCentury spatula device. The stainless steel catheter (outside diameter 2.02 mm, inside diameter 1.67 mm, length 6 cm) was used as an intubation catheter. For N-O exposures in vivo, 18 male CD IGS (Sprague Dawley) rats (Charles River, Sulzfeld, Germany), with a BW of 259 ± 8 g, were used. The animals were placed awake into the customized N-O exposure restrainer (CHT 249; CH Technologies, NJ).
The tracheal catheter or the restrainer tube was connected to the PreciseInhale platform (Fig. 1) and each animal was monitored for 5 minutes before aerosol exposure to ensure stable spontaneous breathing.
Two groups of rats were intratracheally exposed to target doses of, respectively, 10 and 50 μg CHF6001 deposited per lung (Table 1). In the first group (n = 18), a terminal blood sample, lungs, and trachea tissues were collected at the following fixed 6 time points from the end of the aerosol exposures (t = 0): 5, 30, 60, 180, 360, and 1440 minutes, in three rats per time point. In the second group (n = 15), a terminal blood sample and the lung and trachea tissues were collected at the following 5 time points: 5, 60, 180, 360, and 1440 minutes after dosing, in three rats per time point.
One group of rats (n = 18) was exposed N-O to a target dose of 10 μg CHF6001 deposited per lung (Table 1), and then a terminal blood sample, lungs, and trachea tissues were collected at the following 6 time points: 5, 30, 60, 180, 360, and 1440 minutes after dosing, in three rats per time point.
Terminal blood sampling was performed by cardiac puncture after sacrifice with sodium pentobarbital (100 mg/kg, i.p.). Blood was centrifuged to obtain plasma samples, which were immediately frozen on dry ice and stored at −80°C until analysis. Directly after terminal blood sampling, the whole lung and trachea were excised and washed with cold saline. Thereafter, the trachea and lung tissues were dissected separately, weighed, and frozen on dry ice. The plasma and tissue samples were stored at −80°C until analysis.
Exposures of the rat to CHF6001 DP by PennCentury
The experimental procedures and conditions carried out at Chiesi Farmaceutici S.p.A. (i.e., the exposure of the rats by PennCentury and AirJet) were reviewed and approved by the local ethics committees and were performed in full compliance with the international European ethics standards (86/609-EEC), the Italian legislative decree 116/1992, the French National Committee (décret 87/848) for the care and use of laboratory animals, and the Animals (Scientific Procedures) Act of 1986.
DP formulation of CHF6001 was prepared by tubular blending of mainly coarse lactose and fine crystalline compound.
Eighteen male CD IGS (Sprague Dawley) rats (Charles River, Calco, Italy), with a BW of 298 ± 16 g at the day of treatment, were used for powder IT administration. Before dosing, PennCentury DP-4 insufflator was loaded with a weighed amount of DP formulation (10 mg/kg BW) and connected through a valve to a plastic syringe whose plunger was equipped with a spring that is necessary for the propulsion for powder delivery. Then, rats were anesthetized with sevoflurane (Sevorane; Abbott S.p.A., Latina, Italy), placed in supine position on an adjustable table, and intratracheally exposed to the DP formulation by opening the valve between the PennCentury and the plastic syringe: the spring, previously compressed, provided a suitable and reproducible airflow for powder administration. The dose was 1 μmol/kg CHF6001 (corresponding to 0.6875 mg/kg).
After administration, rats were removed from the table and placed into a cage. At fixed time points (0.25, 1, 2, 4, 8, 24 hours after administration), dosed animals were anesthetized with sevoflurane and sacrificed by total bleeding from abdominal aorta; blood aliquots were centrifuged to obtain plasma samples. After animal sacrifice, lung and trachea tissues were excised immediately, washed with cold saline, weighed, and stored at −80°C until analysis. Three rats were used for each time point.
Exposures of the rat to CHF6001 liquid suspension by AirJet
CHF6001 suspension was prepared by suspending a weighed amount of powder in Tween 80, 0.2% (v/v) in saline. CHF6001 concentration in the suspension was assessed by high-performance liquid chromatography/tandem mass spectrometry (HPLC-MS/MS) analysis.
Twenty-four male CD IGS (Sprague Dawley) rats (Charles River, Calco, Italy), with a BW of 297 ± 12 g at the day of treatment, were used for IT administration. Rats were anesthetized with sevoflurane and placed in supine position on an adjustable table. IT administration was performed using a homemade AirJet device, consisting of two syringes, whose plungers were equipped with springs necessary for the propulsion of the formulation, and connected by a valve to a polyethylene tube where the formulation (0.5 mL/kg BW) was loaded. Using a laryngoscope, the polyethylene tube was inserted into the rat trachea until the trachea bifurcation; formulation was then delivered by switching the valves: the springs, previously compressed, provided a suitable and reproducible airflow for the formulation administration.
After administration, rats were removed from the table and placed into the cage. At fixed time points (0.25, 1, 2, 4, 8, 24 hours after administration), dosed rats were anesthetized with sevoflurane and sacrificed by total bleeding from abdominal aorta; blood aliquots were centrifuged to obtain plasma samples. After animal sacrifice, lung and trachea tissues were excised immediately, washed with cold saline, weighed, and stored at −80°C until analysis. Three rats were used for each time point.
Quantification of CHF6001 in plasma samples and lung and trachea tissues
Plasma and tissue samples were analyzed by HPLC-MS/MS system, consisting of a 4000 QTrap mass spectrometer (AB Sciex LLC, Framingham, MA) with an electrospray ionization (ESI) source, coupled to an Agilent 1100 HPLC (Agilent Technologies, Santa Clara, CA). Analyte separation was obtained using a Gemini C18 column (Phenomenex, Inc., Torrance, CA) and water with 0.1% v/v AcOH in gradient with acetonitrile with 0.1% v/v AcOH as eluants.
Before analysis, lung and trachea samples were transferred into suitable homogenization vials, added with acetonitrile/saline 50/50 mixture, with a ratio of 3 and 4 mL/g tissue, respectively, and homogenized using Precellys 24 homogenizer (Bertin Technologies, Montigny-le-Bretonneux, France).
Sample preparation was performed by protein precipitation using preassembled filtration devices (Mini-UniPrep Syringeless Filters, 0.45 μm PTFE, Whatman; GE Healthcare, Buckinghamshire, United Kingdom). Aliquots of 50 μL of sample (plasma or homogenate) were transferred into the bottom part of the device, spiked with 10 μL of the appropriate internal standard solution, and added with 150 μL of acetonitrile. The calibration and quality control samples were prepared by adding 10 μL CHF6001 working standard solution in acetonitrile to 50 μL blank matrix (plasma or homogenate). After vortex mixing, the obtained mixture was filtered by manual compression of the device and the filtered solution was diluted with 100 μL of water. The Mini-UniPrep devices were directly placed in the autosampler rack of the HPLC system.
PK analysis
Data obtained from the ex vivo exposures in the IPL model were evaluated according to the method previously reported.(16) The PK evaluation of the in vivo experiments was done using the software Phoenix 6.2.1 (Certara, NJ). The PK parameters here reported were obtained using noncompartmental analysis.
Cmax represents the maximum concentration obtained in tissues or plasma after administration, and Tmax is the time of its occurrence.
AUClast is the area under the curve for the plasma or tissue concentration as a function of time up to the last measured sampling point calculated by trapezoidal integration. Similarly, the AUC0–24 hours (calculated only for lung) is the area under the concentration curve calculated up to 24 hours.
t1/2 represents the apparent terminal elimination half-life calculated according to the equation: t1/2 = ln2/λz (where λz is the apparent terminal elimination rate constant).
MRTlast indicates the mean residence time calculated from the time of dosing to the last measurable concentration.
Results
Highly dispersed aerosols with a mass median aerodynamic diameter (MMAD) and geometric standard deviation (GSD) of 2.6 μm and 2.1, respectively, were obtained from the micronized CHF6001 powder when aerosolized with the DustGun aerosol generator. Based on the theoretical deposition of each size fraction of the CHF6001 aerosol as calculated by the MPPD (multiple-path particle dosimetry model) v.2.1 software (Applied Research Associates, Inc., Albuquerque, NM), a weighted theoretical total deposition of aerosol was calculated to be ∼33% when inhaled either by the IPL or rats exposed in vivo by the INT inhalation method, and 3% in the rat exposed in vivo by the N-O inhalation method. The theoretical normalized deposition of the inhaled aerosol can then be divided into a tracheobronchial and alveolar fraction of around 60% and 40%, respectively, in all the three models.
The key parameters in the inhalation exposures of the IPL and in the in vivo exposures of the rat by the INT and N-O methods are shown in Table 1. For the INT inhalation methods (IPL and INT models), the duration of the exposures was around 0.5–1 and 5–6 minutes for lower and higher lung doses, respectively. For the N-O inhalation method (N-O model), the duration of the exposure was around 3 minutes for the dose of 10 μg deposited in lung. The longer time required by the N-O model to reach the target dose is due to the lower fraction (about 3%) of inhaled aerosol that reaches the lung.
The concentration of CHF6001 in lung perfusate after aerosol delivery to the IPL is shown in Figure 2 and the corresponding PK parameters are presented in Table 2.

The concentration of CHF6001 (average ± SD, n = 3) as a function of time in the single-pass perfusate of the IPL, exposed ex vivo to CHF6001 powder aerosol with the PreciseInhale to reach two different levels of deposited lung dose. The LLOQ level in the perfusate was 0.03 ng/mL. LLOQ, lowest limit of quantitation; SD, standard deviation.
The data are presented as average ± SD; coefficient of variation (cv%) is given in the brackets.
The maximum concentration of drug in the perfusate.
The time when the maximum concentration is reached.
The cumulative amount of drug passed into the perfusate (calculated with trapezoid integration as previously described2).
The amount of drug retained in tissues after the perfusion period (120 minutes postexposure).
The initially deposited drug dose, calculated from the amount of drug retained in tissues (lung and trachea) after the perfusion period (120 minutes postexposure), plus the total amount of drug cleared to the perfusate during the perfusion period (0–120 minutes).2
The ratio between the achieved deposited dose and the target dose.
The retention of drug in the lungs at the end of the perfusion period (i.e., at 120 minutes postexposure), normalized to the calculated achieved deposited dose.2
The data of fractional retention in the lung were fitted to first-order decay functions for calculating the half-time of retention in the lung.2
SD, standard deviation.
After administration, CHF6001 appeared rapidly in lung perfusate, with a Tmax ranging from 3 to 7 minutes depending on the administered dose. The Cmax value was proportional to the administered dose (Table 2). The achieved deposited dose of the compound in the IPL model, as calculated from the total amount retained in the lung tissues (lung and trachea) at the end of the experiment plus the total amount of drug passed to the perfusate,(2) was 40%–90% higher than the target dose, and some variability was observed for the low dose (Table 2). In the IPL model, around 90% of the initially deposited dose of CHF6001 was retained in the lung 120 minutes postexposure (Table 2). The half-life of compound disappearance from the lung in the IPL model resulted to be about 14 hours for both of the tested doses (14.2 ± 5.7 hours for the low dose and 13.5 ± 1.0 hours for the high dose).
The concentration of CHF6001 in lung and plasma after administration of the respirable aerosol to rats in vivo using the PreciseInhale system is shown in Figure 3. Aiming for the same target dose of 10 μg/lung in both in vivo exposure models of the PreciseInhale system produced similar lung levels, as measured immediately (i.e., 5 minutes) after administration (8.11 ± 1.28 and 11.9 ± 6.3 μg/lung for INT and N-O exposure, respectively), and similar lung exposure, with AUC0–24 hours, lung values of 76.4 ± 5.9 hr*μg/g for INT rat and 95.9 ± 7.7 hr*μg/g for N-O administration (Table 3). The amount of deposited compound at the first sampling time point was close to target, with an accuracy within ±25%, for both the INT and N-O models (Table 3).

The lung amount
IT inhalation of respirable powder aerosol with the PreciseInhale system.
N-O inhalation of respirable powder aerosol with the PreciseInhale system.
Target dose of drug deposited in lung (parameters selected in the instrument setting).
Nominal dose deposited in lung, calculated for a rat with a body weight of 300 g (1 μmol/kg = 206.3 μg/rat), and assuming 100% lung deposition.
Fraction of the nominal dose deposited in lung, calculated as a ratio between the amount deposited in lung at the first sampling time point and the nominal dose.
AUC, area under the curve.
In the INT model exposed to CHF6001 powder aerosol at two dose levels (10 and 50 μg/lung deposited dose), a good correlation between the target dose and the lung AUC0–24 hours was observed (Table 3): the lung exposure yielded by the administration of the high dose (AUC0–24 hours 393.3 ± 51.9 hr*μg/g) resulted to be fivefold greater than the value obtained with the lower dose.
Regarding the systemic exposure, the plasma Cmax value obtained in the N-O model (6.6 ± 2.2 ng/mL) was significantly higher than the one obtained in the INT model (1.8 ± 0.6 ng/mL) at the same target dose of 10 μg/lung deposited dose (Figure 3 and Table 3).
The administration of CHF6001 using the PennCentury insufflator and the AirJet suspension instillation method produced lung deposition, determined at the first sampling time point after administration, around 8.4% and 55.3% of the nominal dose (1 μmol/kg = 0.6875 mg/kg), respectively (Table 3).
A comparison of lung and plasma profiles obtained after administration of CHF6001 with the PreciseInhale, PennCentury, and AirJet devices is shown in Figure 4. The curves are normalized to the same lung deposited dose (10 μg/lung).
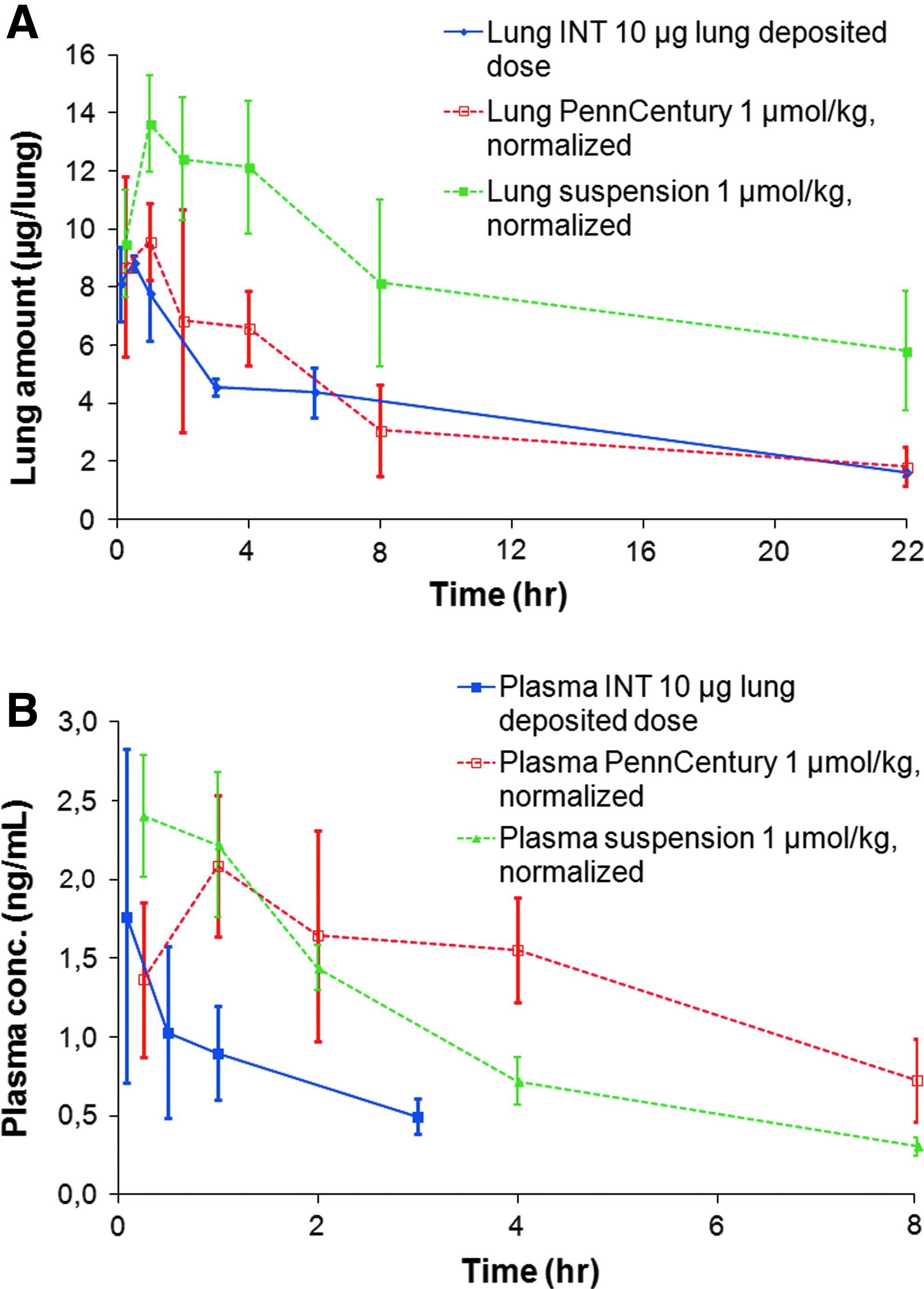
The lung amount
Lung exposure proved to be consistent between IT administration using the PreciseInhale or the PennCentury (Fig. 4), as confirmed by lung AUC0–24 hours, lung values (Table 3) that are not significantly different between INT rat model of the PreciseInhale (76.4 ± 5.9 hr*μg/g) and the PennCentury (77.6 ± 8.8 hr*μg/g) when the lung levels are normalized by the deposited dose. Nevertheless, administration by the PennCentury generated higher variability in lung data. Administration of CHF6001 suspension produced higher lung levels (twofold higher than INT model and PennCentury administration, normalizing the levels by the deposited dose) and data variability comparable to the PennCentury device.
The terminal half-life of CHF6001 in the lung ranged between 12 and 16 hours in all the in vivo powder exposure models and for all tested doses (Table 3), and these results are in good agreement with the disappearance half-life calculated with the IPL model (14.2 ± 5.7 hours, Table 2). The lung terminal half-life of CHF6001 resulted to be slightly longer (19 hours) after administration of the suspension formulation (Table 3).
To evaluate compound deposition in the trachea with the different techniques, excised trachea tissues were collected at the first time point after administration. The PreciseInhale enabled good penetration of DP aerosol into the lung in both in vivo models (INT and N-O), with only a small deposition in the trachea (4%–5%) that is in good agreement with theoretical airway deposition models (MPPD). In contrast, the PennCentury and AirJet devices yielded much higher tracheal deposition, due to the airflow used for the propulsion of the formulation into the lung, with the likely consequence of the swallowed fraction being increased.
The systemic exposure to CHF6001 was higher when the compound was administered by the PennCentury. Normalizing the plasma levels to the CHF6001 lung deposited dose (to make comparable the experiments performed using different doses and devices, i.e., PennCentury and PreciseInhale), the plasma AUClast obtained with the PennCentury (20.1 ± 3.2 hr*ng/mL) was eightfold higher than that of the INT model (2.5 ± 0.3 hr*ng/mL) and twofold higher than that of the N-O model (8.9 ± 1.2 hr*ng/mL). Administration of the liquid formulation yielded a systemic exposure (AUClast 11.5 ± 0.7 hr*ng/mL, normalized for the lung deposited dose) significantly higher than the INT model of PreciseInhale system and lower than PennCentury, with a rapid absorption of the compound to plasma, as reflected by plasma Tmax that corresponds to the first sampling time point.
Regarding the substance consumption to perform the experiment with the PreciseInhale system, it required a total amount of 301 mg substance to deposit a total amount of 1.46 mg CHF6001 in the lungs of 57 rats, including aerosol optimization and characterization, filter exposures, and animal dosing.
Discussion
Inhalation administration of candidate drugs to animal models in the lead optimization phase of drug discovery is a crucial step for the investigation of the PK and pharmacodynamic (PD) profiles of the compounds. Selection of a suitable formulation and control over the administered dose are challenging aspects of the PK and PD experiments.
A short bolus dose can be achieved by IT instillation of liquid formulation or DP insufflation; these methods are normally used during drug discovery when powder formulation is not completely developed and availability of compound material is too scarce to perform in vivo studies with inhalation towers. The great disadvantage of the bolus methods is an uneven distribution of deposited materials in the lungs and often too large particles administered during powder insufflation.(2,5,25,26)
With inhalation exposures in N-O towers, the desired respirable size aerosol can be achieved, but the dose rate can be lowered by a need for mixing the active pharmaceutical ingredient with excipients such as lactose. Moreover, this equipment requires a larger amount of compound to generate aerosol with the correct concentration for a sufficient duration of exposure.
With continuous aerosol generators such as the Wright dust feeder, the need for mixing with excipients may lower the achieved aerosol concentration of the respirable size fraction of active compound below the maximum aerosol concentration of 2 mg/L recommended by the Organization for Economic Co-operation and Development (OECD),(27) thereby reducing the dosing rate. In one example, with N-O inhalation exposure of roflumilast (an oral PDE4 inhibitor) to rats, a dose of 10 μg/kg deposited lung dose was achieved in 30 minutes, giving an approximate dose rate in 300 g BW rat of 0.1 μg lung deposition/min.(28) In another study with a brush generator, the dose rates of respirable rapamycin in the rat were achieved up to 0.2 μg lung deposition/min.(29)
With the high-power aerosol generator of the PreciseInhale system,(15) aerosol concentration of respirable neat compound can be achieved in the range of the maximum level recommended by OECD. In the case of CHF6001, the novel PDE4 inhibitor investigated in this study, the dose rate achieved was 3.7 μg lung deposition/min for the N-O model, due to a higher aerosol concentration in the breathing zone. Considering this high aerosol concentration during the exposure, the possibility to monitor the breath rate of the single animal enabled by the PreciseInhale is very useful to calculate the inhaled dose for each rat in the presence of different entities of breathing suppression in the animals reacting to the high-concentration exposures.(30)
After inhalation administration, CHF6001 showed long lung retention and low systemic exposures, such features are attractive for inhaled compounds.(31) During the Lead Optimization Phase, the different techniques used to obtain CHF6001 PK lung data were compared in terms of reproducibility and accuracy in lung deposition. Furthermore, data obtained in the ex vivo model (IPL) were evaluated to assess the ability of this model to predict lung persistency in vivo.
Administration of CHF6001 as a suspension using a homemade Airjet device yielded high lung deposition (about 55% of the administered dose was deposited in lung), and also a considerable tracheal deposition of the compound that could be subsequently swallowed and absorbed in the GI tract. Compared to PennCentury administration of DP formulation, lung exposure was much higher (15-fold) with suspension administration, and lung persistency was found to be longer, as suggested by the different lung t1/2 values. Consequently, suspension administration is not expected to be representative of the DP formulation for CHF6001. On the contrary, DP administration by PennCentury produced a rather low lung deposition (8.4% ± 3.0% of the nominal administered dose) and a much higher tracheal deposited fraction, calculated as a fraction of the total amount deposited in the lung and trachea at the first time point.
Considering the difficulties in delivering a controlled dose of compound aerosol during inhalation studies, one of the greatest advantages of the PreciseInhale technology was that the CHF6001 lung concentration immediately after dosing was very close to the target dose selected in the instrument parameters, for both endotracheally intubated rat (INT) and N-O exposure models. Accuracy of dosing, expressed as deviation from the target lung doses, was within ±25% for both PreciseInhale exposure models (INT and N-O), which is acceptable in inhalation in vivo experiments where the ability to get the expected amounts in the lung with reasonable accuracy is one of the most challenging aspects. Moreover, the tracheal deposition was low, reducing the amount of compound swallowed.
The linearity of the dose delivered by the PreciseInhale system was assessed by administration of two different doses in the INT model, resulting in good correlation between the lung AUC values and the target dose level (Table 3).
Analyzing the plasma concentration curves, systemic absorption of the compound from the lung was found to be enhanced by using liquid formulation with related excipients (e.g., Tween 80); this profile may be explained by a substantial fraction of the compound being solubilized in the liquid formulation, which may be rapidly absorbed from the lung after administration. Moreover, the solubilizing excipients added in the liquid formulation (e.g., Tween 80) may also affect the rate of compound dissolution/absorption and possibly the lung PK.(7,8)
Comparing the CHF6001 plasma profile after powder administration, the INT model produced significantly lower plasma levels (AUClast plasma 2.5 ± 0.3 hr*ng/mL) compared to both the N-O model (AUClast plasma 8.9 ± 1.2 hr*ng/mL) and PennCentury (AUClast plasma 20.1 ± 3.2 hr*ng/mL, normalized for the lung deposited dose) administration. A possible explanation for these differences is that CHF6001 is almost exclusively deposited in the lung (bronchial and alveolar region) with the INT model, while, during N-O inhalation, a substantial deposition of aerosol occurs in the nasal airways, which may contribute to absorption into systemic circulation and also yield an increment in swallowed fraction. Similarly, PennCentury administration yields high tracheal deposition and consequently increases the amount of compound swallowed.
Such a considerable amount of compound reaching the GI tract could give a rise in the CHF6001 systemic levels due to intestinal absorption, although the oral bioavailability of the compound is low (about 10%, unpublished data). The delayed plasma Tmax (about 1 hour) observed after DP administration with PennCentury is in line with observations after oral administration of CHF6001 (unpublished data).
The obtained lung half-life was comparable between all the powder administration procedures (PennCentury and PreciseInhale).
Comparing the three exposure models linked to the PreciseInhale system, the two in vivo models (INT and N-O) had better accuracy and precision than the IPL model. Considering the lung PKs, the t1/2 values obtained for CHF6001 with the IPL model were in line with the t1/2 values obtained with both of the in vivo models (INT and N-O) and with the value obtained after administration by PennCentury device (Tables 2 and 3), suggesting that this ex vivo model is suitable to predict in vivo lung PKs of CHF6001. Previously, the IPL model has been used to demonstrate lung half-lives, following aerosol exposures, of 40 minutes for budesonide(23) and ∼4.5 hours for fluticasone furoate.(16)
In conclusion, the presented study demonstrated that PreciseInhale system enabled the investigation of the pulmonary PK of new compounds as neat powder with reproducibility and accuracy higher than the usual techniques routinely adopted for inhalation administration to rodents, avoiding the use of a huge amount of substances and allowing to get PK data without DP formulation, often available only during the Lead Optimization phase of the drug discovery processes.
Footnotes
Author Disclosure Statement
Drs. F.A., P.G., and E.S. are minority shareholders in Inhalation Sciences Sweden AB.