
Abstract
Abstract
Background:
Inhalation of medications is the cornerstone in the treatment of patients with lung diseases. A variety of inhalation devices exists and each device has specific requirements to achieve optimum inhalation of the drug. The goal of this study was to establish a clear overview on performance requirements of standard inhalation devices that should be met by the patient's breathing power and to develop a new method to measure the individual performance data.
Materials and Methods:
An optimum and still acceptable required breathing power (P in watts) was calculated for each device with the aid of individual device flow rates (determined by a literature search) and the flow resistances (by measuring the pressure drop over the different inhalation devices). For the in vivo part of the study, peak inspiratory flow and peak inspiratory pressure drop were measured in 21 adult patients with asthma or chronic obstructive pulmonary disease and healthy volunteers and the peak inspiratory power (PIPO in watts) was calculated.
Results:
Nearly no power is needed to achieve optimum results when using pressurized metered dose inhalers. For dry powder inhalers, the required power depends on the specific inhalation device.
Conclusions:
Inhalation devices impose differing demands on the inspiratory breathing power of patients. To ensure adequate use of the different devices, a cheap and simple assessment of patients' PIPO may be one option.
Introduction
I
However, while most of these steps are similar for all devices, there are wide variations regarding the inspiratory flow rate, inhalation time and volume, and the required flow acceleration (flow increase rate [FIR]) between DPIs and pMDIs. While MDIs (pMDIs and breath actuated inhalers [BAI]) require a preferably slow and deep inhalation, (long inhalation times), DPIs need a forceful inhalation (high flow rate) straight from the beginning. It has been shown that one of the most crucial errors for the use of DPIs is the failure to achieve a forceful and rapid inspiratory flow during the initial part of the inhalation.(1–4) It is, therefore, often recommended, that the patient's ability to generate an appropriate inhalation flow through a DPI should be checked.(1,4,5)
The inspiratory flow rate for DPIs is device specific(6) and must overcome the device's internal resistance.(1) For each DPI device, a minimum flow rate must be exceeded to guarantee an acceptable drug release and deposition in the lung.(1) These minimum required flow rates depend on the internal resistance of the inhalation device and the inhalation effort of the patient. Although the literature provides data on necessary inspiratory flow rates of individual inhalers(6) and on flow resistances of standard devices,(7,8) these individual data alone are not useful for the physician as the resistances of devices vary considerably and the requirements for inspiratory flow rates therefore vary for individual devices.(4,6)
Patients achieve lower flow rates when using a device with high resistance when compared with devices with lower resistance.(4,6,9) To achieve a device-specific minimum flow over a device resistance that is needed to generate a respirable aerosol of good quality, additional effort by the patient is needed. In a number of patients with low inspiratory flow rates, such as children,(10) COPD patients,(4) or older patients,(7) however, acceptable lung deposition cannot be achieved while using an inhaler with high resistance. Hence, the device-specific resistance must be matched to the patient's breathing capability.
To make sure that a patient can achieve the required additional breathing power needed for the adequate application of the prescribed inhaler, it is necessary for the physician to know the performance requirements of all regularly used inhalation devices and to compare them to each other. Furthermore, it would be useful to measure the patient's performance ability with a simple and fast test. Previous test methods such as the In-Check® system are simple to perform when only one device is tested.(11) However, if a device selection would be done this way, a higher time requirement is needed as the system must be adjusted to the individual devices and inspiratory peak flow measurements have to be carried out for each device.
The goal of this study was to establish a clear overview on performance requirements of standard inhalation devices that should be met by the patient's breathing power and to develop a new method to measure the individual performance data. As part of the study, in vitro and in vivo data were generated.
In a previously published study by Haidl et al., a literature search was carried out to establish the required flow rates for different inhalation devices.(6) Flow resistances of each inhaler were then measured and the minimum and optimum required breathing power were calculated for all devices. In the second part of the study, in vivo measurements were carried out in healthy subjects and in patients with COPD or asthma to determine their peak inspiratory power (PIPO). This parameter describes the effort that can be applied by a patient to an inhalation device to generate a pressure drop and an inspiratory flow depending on the resistance of the device. The in vivo data were analyzed to find a parameter that can be used in practice by physicians to identify an inhaler with a suitable power requirement for individual patients.
Materials and Methods
Flow rates
In a preparatory study that was recently published, a literature search was conducted for publications released between 1980 and 2015 with the aim of determining inhaler performance and associated inhalation flow rate. The results were used for this study as well. For more details, see publication by Haidl et al.(6)
Flow resistances
To determine the resistances of the inhalers, the pressure drop over the different inhalation devices was measured using the design depicted in Figure 1.

Measurement setup for flow and pressure measurements.
The measurement setup consisted of a glass mouth, pressure sensor (Kalinsky DS 2-010), filter (standard glass fiber filter Sartorius 13400), flow sensor (Sensirion SFM300), and computer. The inhaler was attached to the glass mouth and a volume flow was drawn through the filter. The pressure behind the inhaler was recorded directly at the exit of the glass mouth and a flow sensor at the end of the filter was used to measure the flow rate. Pressure and flow rate were constantly monitored by the computer.
At first, pressure was determined over various flow rates without the attachment of an inhaler. No measurable pressure drop was observed, and all subsequent pressure measurements with attached inhalers were equivalent to pressure drops over individual inhalation devices. The specific flow resistance (R) for each inhaler was calculated using the square root of pressure drop (Δp) and the volumetric flow rate (
Required breathing power
The optimum and still acceptable required breathing power (P in watts) can be derived from the measured resistance and the flow rates described in the literature for each inhalation device. Power is defined according to Equation (2):
Inserting Equations (1) into (2) results in the following equation:
With this equation, the required breathing power for each individual inhaler can be calculated if the internal resistance and the minimum/optimum flow rate are known.
In vivo measurements
If one places a flow resistor in the inhalation flow path, as is the case when using inhalers, the excess work of breathing can be defined as follows:
The product
To determine E and hence PIPO, an add-on device to a pneumotachograph (MasterScope Spiro; CareFusion) was developed, which measures the pressure drop using three exchangeable orifice adapters with increasing diameters from 4 to 7 mm (high to low resistance; R1 = 0.14, R2 = 0.089, R3 = 0.049 mbar1/2/(L·min), having resistances corresponding to commercial inhalers (Figs. 2 and 3 and Table 1).

Schemata of set up used to measure the inspiratory energy E and PIPO. PIPO, peak inspiratory power.

Orifice adaptors used during measurements.
Data on the Device Specific Flow Resistances (measured) and Power Requirements (calculated) of Different Inhalation Devices at Optimum and Still Acceptable Flow Rates (if not identical with optimum flow rate)
The flow rates were obtained from a literature review.6 Different units for resistance are given for convenience to compare with other literature.
AB, aclidinium bromide; BDP, beclomethasone dipropionate; BUD, budesonide; FF, fluticasone furoate; FORM, formoterol; FP, fluticasone propionate; IND, indacaterol; pMDI, pressurized metered dose inhalers; SALB, salbutamol sulfate; SALM, salmeterol; TB, tiotropium bromide.
The study comprised 21 adult patients and volunteers. Subjects were randomly recruited from the database of the Fraunhofer Institute according to diagnosis (asthma, COPD, and healthy) and disease severity (according to GINA and GOLD guidelines for asthma and COPD). At the time of the study, all patients were receiving medication for their respective disease. In vivo measurements were approved by the Ethics Committee of Hannover Medical School. All subjects provided written informed consent after being informed about the study procedures.
Pressure drops were recorded with the three exchangeable orifice adapters connected to a pneumotachograph as an add-on device. During the measurement, patients inhaled at maximum effort from residual volume up to total lung capacity while the pressure drop across the orifice adapter was measured. The peak inspiratory power (PIPO in watts) was calculated using the following equation, where
From a series of three measurements through one orifice adapter the mean values were taken; for two patients with COPD only two repeat measurements could be carried out.
Besides peak inspiratory flow (PIF), which can be calculated from Δp using Equation (1), and inhaled volume, the flow increase rate (FIR; which is the acceleration in airflow) may be a relevant inspiratory flow parameter for the performance of DPIs.(12) Therefore, FIR was calculated from the measured data for comparison with the newly identified parameter PIPO. FIR was calculated as the average FIR from 20% to 80% of PIFRx (FIR20%–80% [L · s−2]). FIR20%–80% (L · s−2) was calculated as the ratio of flow 20% of PIF and 80% of PIF to time 20% of PIF and 80% of PIF.
Results
Flow rates
The review of the literature revealed obstacles in making clear distinctions between optimum (sufficient) inhalation flow rates and still acceptable (minimum) flow rates for each device. Minimum required inspiratory flow rates to deposit the medication dose in the airways are described for most inhalers in the literature. An overview of the required inspiratory flow rates for the use of different inhalation devices is shown in Table 1. While the optimum flow rate for pMDIs is generally low (20 L/min), there are vast differences between the various DPIs, with the Turbohaler® device needing the highest flow rate (60 L/min) to achieve optimum results.
Flow resistances
The flow resistances of the different inhalers are shown in Table 1. The lowest resistance was measured for pMDIs, while the resistances between DPIs were markedly different. The highest resistance of the investigated devices was observed for the HandiHaler® device.
Required breathing power
The optimum and still acceptable required breathing power were calculated using Equation (3) for each of the inhalation devices (Table 1). Nearly no power is needed to achieve optimum results when using pMDIs. For DPIs, on the other hand, the required power depends on the specific inhalation device. While some inhalers, such as the Diskus® device, only require little power, the use of other inhalers, for example, the Turbohaler device, necessitates more effort from the patient.
In vivo measurements
In total, three healthy controls (two women and one man) nine patients with asthma (five women and four men) and nine patients with COPD (five women and four men), were included in the study. COPD patients were not only older (range from 61 to 72 years) than patients with asthma (range from 19 to 54 years) but also than healthy controls (range from 34 to 50 years). Patients with COPD also exhibited worse lung function (defined by forced expiratory volume in one second [FEV1]/forced vital capacity [FVC]) than patients with asthma or healthy controls. An overview of individual characteristics is given in Table 2.
Characteristics of Individual Study Participants Regarding Health Status, Disease Severity, Sex, Age, and Lung Function
COPD, chronic obstructive pulmonary disease; F, female; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; M, male.
Peak inspiratory power
Figure 4 illustrates the results of all individual subjects included in the study. From the mean PIPO values for each participant of the study over the three different resistances, mean values classified by underlying disease were calculated and shown in Table 3 and Figure 5.
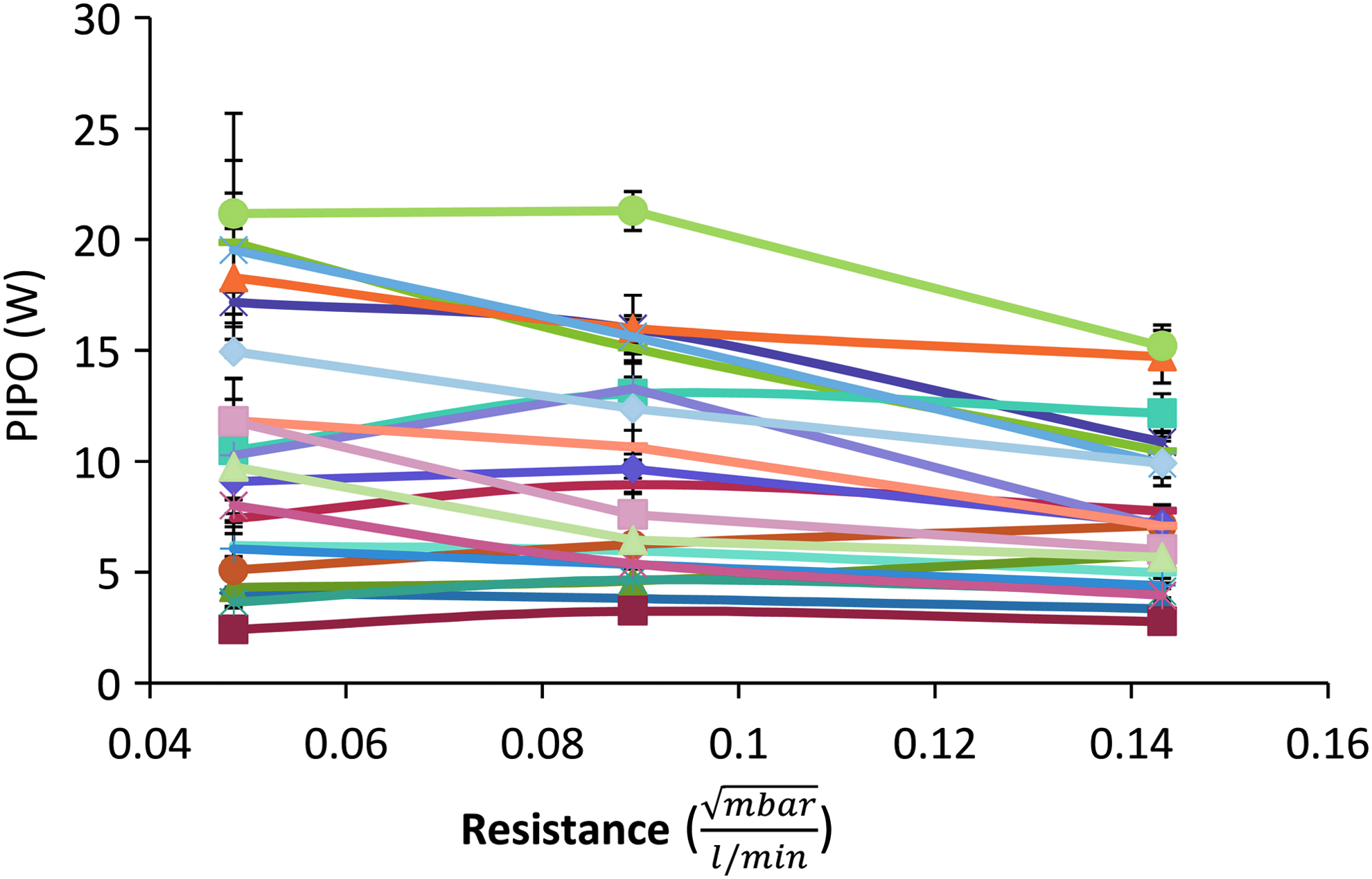
Results of the PIPO measurements from individual subjects (each line represents one subject). Each point represents 3 (in one case 2) measurements. The bars represent the standard deviations.
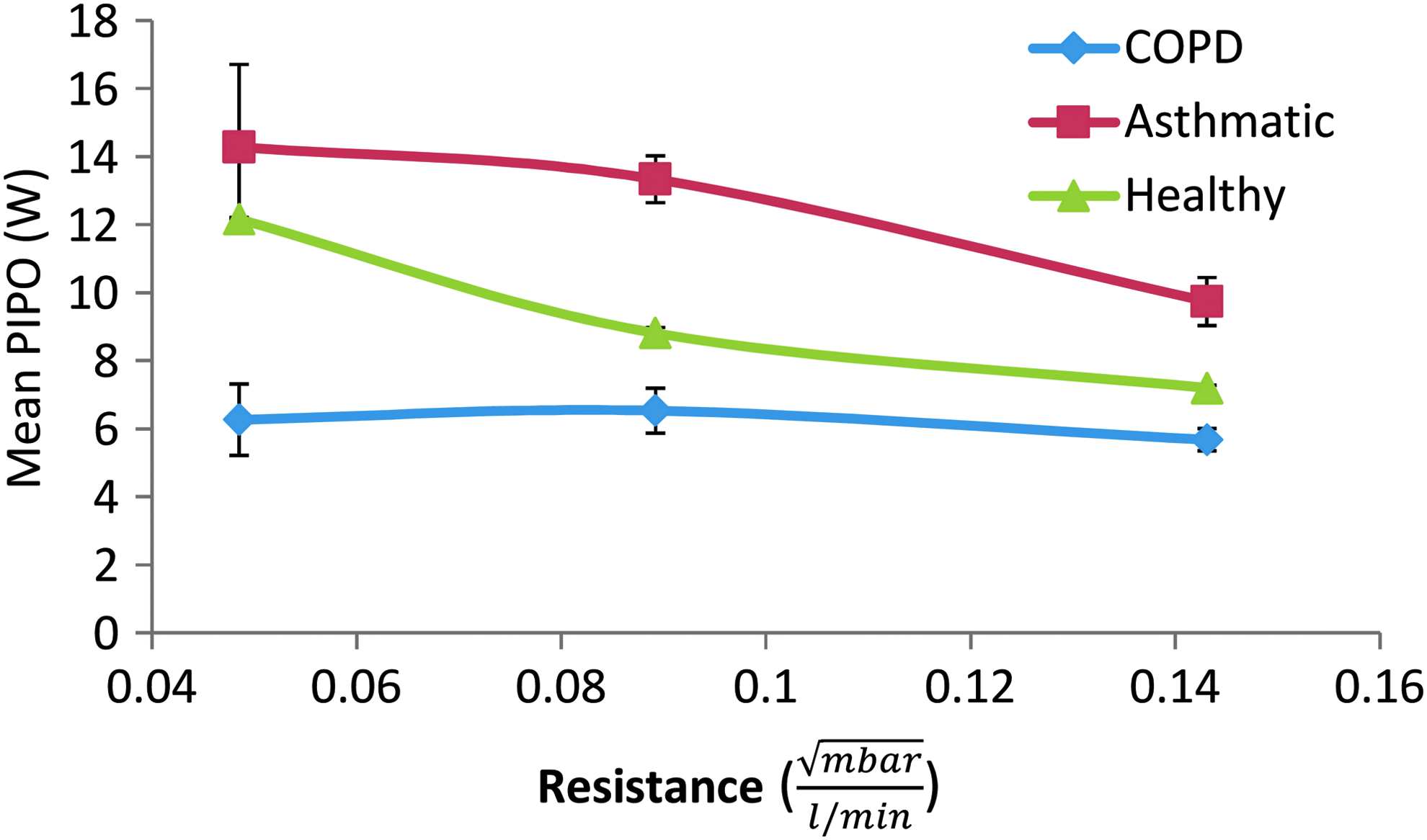
Results of the PIPO measurements. The curves show the mean PIPO values aggregated according to underlying disease. COPD, chronic obstructive pulmonary disease.
Data on Peak Inspiratory Power and Flow Increase Values for Healthy Adults, Patients with Asthma, and Patients with Chronic Obstructive Pulmonary Disease
FIR, flow increase rate; PIPO, peak inspiratory power; R, resistance.
Boldface values help for better readability.
Flow increase rate
The mean FIR values for each participant of the study over the three different resistances were calculated and the mean values classified by health status are shown in Table 3. The FIR decreases with increased resistance to airflow (Table 3).
Correlation between PIPO and FIR
Figure 6a–c show an increasing correlation (R2: 0.41; 0.57; 0.73) between PIPO and FIR values for individual patients measured for the three resistances with a tendency for better correlation with lower resistances. This tendency might be due to increasing scatter especially for FIR values with increasing resistance.

Discussion
This study investigated the power requirements for optimal use of current inhalation devices and looked at in vitro and in vivo data. For the in vitro data, it was shown that there are vast differences regarding flow resistances of different devices. As expected, the lowest flow resistances were measured for pMDIs. While resistances of pMDIs also vary from device to device, they are still considerably lower than those for DPIs. The variability of those low resistances for pMDIs may be relevant for the use of different spacer systems with so-called alert whistles,(13) but they are not of relevance for the required breathing power of patients. Varying from these manually triggered pMDIs, flow resistances for BAIs are generally higher due to their trigger mechanism.
For DPIs, the flow resistances are considerably larger than for inhalers powered by propellants and there are large differences regarding flow resistances between the different inhalation devices of DPIs, with the HandiHaler device being the inhaler with the highest flow resistance. As previously mentioned, patients achieve lower flow rates when using a device with high resistance when compared with devices with lower resistance.(4,6,9) However, resistance on its own does not determine whether a patient can use an inhalation device.
Another factor that plays a role is the minimum required flow rate for each device. As with the resistances, these vary markedly between the different devices. The optimum flow rate for pMDIs is generally very low since the propellant actively releases the aerosol. Patients should therefore not inhale too fast.
As for DPIs, there are not only vast differences between the inhalers regarding the flow resistance but also regarding the flow rate. Below the minimum threshold, poor aerosol quality or even no dose is emitted and will therefore affect the therapeutic benefit.(1) While the HandiHaler device requires only a minimum flow rate of 20 L/min to achieve acceptable deagglomeration of the powder that leads to a high proportion of inhalable particles, the Breezhaler® device requires 50 L/min. To achieve optimum results while using the Turbohaler device, a flow rate of 60 L/min must be achieved.
On their own, neither resistance nor inspiratory flow rate is conclusive of whether a patient can handle the inhalation device appropriately. The important aspect is how high the inspiratory flow must be to overcome the flow resistance and meet the device-specific requirements. This can be expressed by the required breathing power, which is derived from both flow resistance and inspiratory flow rate, and is, in our opinion, therefore more useful than the single parameters.
The breathing power required for the use of an inhalation device can easily be determined with a fast method. In our study, we have shown that there are considerable differences in PIPO values for different patients (Fig. 4) and also for mean PIPO values when aggregated for different indications. Comparing this data with the optimum power for the inhalers tested (Table 1), only few PIPO values are smaller than the inhaler with the highest power requirements (4.36 W).
By the course of the curves in Figure 4, one could hypothesize that three measurements could be sufficient to gain an overview of the breathing capability of patients for a wide range of inhaler resistances regarding PIPO. Therefore, to ensure adequate use of different devices, a cheap and simple assessment of patients' PIPO could be one option.
PIPO measurements could be carried out with a spirometer or via body plethysmography after technical adjustments and the addition of flow resistances. Principally, technically simple “low price” flow measuring systems could also be used to examine whether a patient can achieve the required power for a particular inhalation device.
Such “cheap” measuring devices could be produced quite inexpensively for single use and contain simple means to check three different resistances. Such devices make use of the relations in Equations (1) and (2) by measuring the pressure drop resulting from sucking air through an orifice. An exemplary device is shown in Figure 7. Here, for example, PIPO can be read from a scale that corresponds to the position of the movable swivel that is used to select one of the three built in orifices. Thereby, a measurement could easily and quickly be carried out and is not tied to specific premises such as rooms with a spirometer.
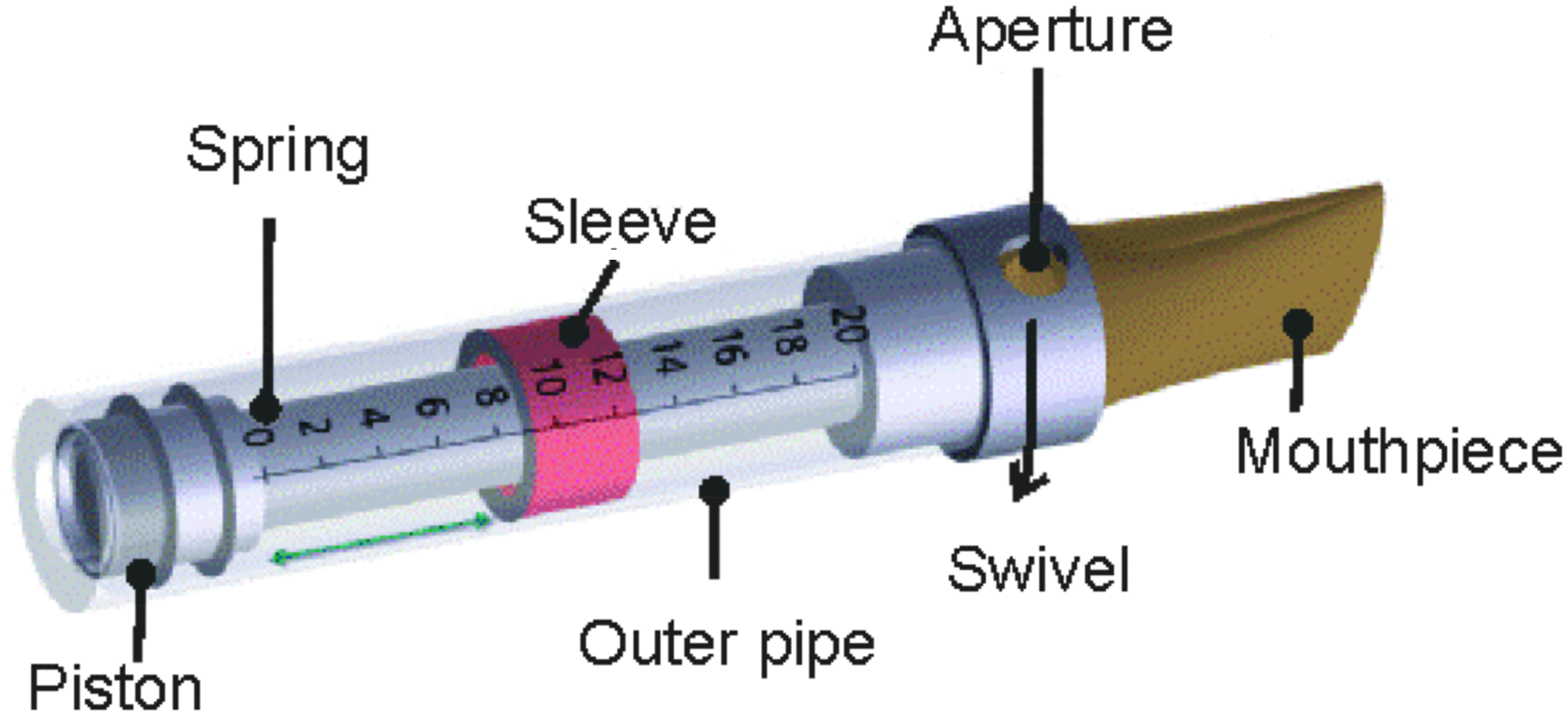
Design study of a simple, single use/single patient PIPO measurement device.
The results of our study indicate that patients with COPD are the worst performers when comparing data for PIPO between healthy volunteers and patients with asthma or COPD (Fig. 5). This is in agreement with data from de Koning.(12) Even though the resistances used by de Koning do not match the resistances used in this study, the calculated data for PIPO are at the same order of magnitude and comparable trends can be observed. Healthy volunteers and asthmatics generally show better performance than people with COPD. The lower the resistance, the more the performance increases.(12) In our study, this trend is less pronounced for patients with COPD, indicating that these patients may struggle while using inhalation devices with high resistance.
In our study no patient inhalation was below the minimum required flow rate of a DPI device. This result does not correspond to the experience of everyday practice and contrasts with the outcome of various studies on the use of DPIs, which have shown that a significant proportion of patients (children and adults) with asthma or COPD and with significant broncho-obstruction do not exhibit satisfactory inspiratory flow rates for the use of DPIs.(7,11,14–18)
This can be explained by the facts that we collected the data with a small group of patients. All patients in our study received their respective medication for either asthma or COPD and their diseases were controlled. This could also explain why the asthmatics on average showed higher PIPO values than the healthy volunteers. However, all findings in our study are based on a very small number of volunteers who were also not age matched. A larger study is therefore needed to confirm our results.
Following de Koning, a minimal acceleration in FIR is necessary for an optimal drug deposition into the airways.(12) In our study, PIPO measurements correlated with FIR with a tendency for better correlation with lower resistances, which may be because PIPO measurements generally show lower scatter. Furthermore, in comparison to the easy measurement of PIPO, measurement of FIR is more elaborate. Therefore, PIPO is assumed to be more predictive than FIR and easier to measure.
In conclusion, our study shows that inhalation devices impose differing demands on the inspiratory breathing power of patients. To ensure adequate use of the different devices, an assessment of the breathing power of patients (one way could be PIPO) is therefore an option as soon as a cheap and simple assessment is available. But further studies are needed to investigate what kind of measuring systems are needed and for which diseases these measurements should preferably be used to determine breathing capabilities also for resistances down to 0.01 mbar1/2/(L·min) and to compare these data with vital capacity (inhaled volume) of patients, as this may be important for some inhalers. Further work on using a consistent approach to determine minimum flow rates for a variety of inhaler types would also be useful.
Footnotes
Acknowledgments
The authors would like to thank Dr. Maren Klug (kw medipoint, Germany) for medical writing assistance. Medical writing support was funded by Mundipharma GmbH, Germany. The device resistance measurements and the calculation of the required breathing power for each individual inhaler were sponsored by Mundipharma GmbH, Germany. The in vivo measurements were carried out by and at the expense of Fraunhofer ITEM. Writing assistance in the preparation of this article was provided by Dr. Maren Klug, kw medipoint. Mundipharma GmbH Germany provided financial support for the preparation of the article, including all article processing charges.
Registered Trade Mark Statements
® AUTOHALER is a registered trademark of 3M Company; EASI-BREATHE is a registered trademark of Norton Healthcare Limited; NOVOLIZER, GENUAIR, and TURBOHALER are registered trademarks of AstraZeneca AB; EASYHALER is a registered trademark of Orion Corporation; DISKUS and ELLIPTA are registered trademarks of Glaxo Group Limited; AEROLIZER, BREEZHALER, and FORSPIRO are registered trademarks of Novartis AG; HandiHaler is a registered trademark of Boehringer Ingelheim Pharma GmbH & Co. KG; NEXTHALER is a registered trademark of Chiesi Farmaceutici S.p.A.; SPIROMAX is a registered trademark of IVAX International B.V.; IN-CHECK is a registered trademark of Clement Clarke International Limited.
Author Disclosure Statement
During the last 3 years G.P. has received honoraria for attending advisory boards of Mundipharma GmbH, Germany. J.M.H. has received lecture fees or consultancy honoraria from Boehringer Ingelheim, Mundipharma, and Novartis. P.H. has received honoraria for attending advisory boards or giving lectures for the following companies: AstraZeneca, Astellas, Berlin-Chemie, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Forest companies, Mundipharma, Novartis, Nycomed, and Teva.
No conflicts of interest exist for J.P. R.M.C. was an employee of Mundipharma GmbH, Germany, during the study period. All named authors meet the ICMJE criteria for authorship for this article, have been involved in the analysis and interpretation of the data, writing and review of the article, in the decision to submit the article for publication, and have given final approval of the version to be published.
Reviewed by:
Davd Prime
Michael Hindle