
Abstract
Abstract
Background:
The delivery of antitubercular drugs through direct lung targeting can lead to reduction in the dose as well as side effects of the drug. In the present investigation, carrier (lactose)-based dry-powder inhaler of rifampicin was prepared to achieve direct targeting of the drug into the lungs.
Methods:
The dry powder inhaler formulation was prepared by simply mixing micronized rifampicin with coarse and fine lactose preblend. Preliminary blends of the drug were prepared with various lactose grades (Inhalac®, Respitose,® and Lactohale®). Rotahaler® and Revolizer® were evaluated for the performance. The 32 factorial design was used to optimize the amount of drug (X1) and amount of fine lactose (X2). In vitro lung deposition was carried out using Andersen Cascade Impactor. The % cell viability studies of the formulation were carried out using murine macrophage J774 cell lines. The in vivo toxicity was determined using histopathology. Further in vivo pulmonary pharmacokinetics of the developed dry-powder inhaler (DPI) formulation was carried out in comparison to the marketed formulation in the rat lungs.
Results:
Based on preliminary trials, Inhalac 230 and Inhalac 400 were selected as coarse and fine lactose grades, respectively. Rotahaler® exhibited better DPI performance with the evaluated drug blends. The mass median aerodynamic diameter (MMAD) was in the range of 4.3–5.8 μm with the maximum fine particle fraction of 28.9%. The formulation exhibited negligible cytotoxicity on macrophage J774 cell lines with about 75%–80% cell viability at 6- and 12-hour exposure. The histopathological examination revealed negligible toxicity of DPI in comparison to the marketed formulation. The in vivo pulmonary pharmacokinetic studies of the DPI formulation in rats showed higher drug concentration in lungs in comparison to the marketed formulation.
Conclusion:
The carrier-mediated dry-powder inhaler of rifampicin could serve as an improved and efficient system for local targeting of drugs into the lungs.
Introduction
T
DPI are chiefly composed of micronized drug admixed with the carrier particles of larger size to aid in flow and dispersion. The drug particles in the micronized form have a large surface area that readily agglomerates. In this milieu, the carrier particles reduce agglomeration and improve flow. The desired aerodynamic particle size for the drug to settle in alveoli (which is the main target site) is 1–5 μm. Many of these particles escape mucociliary clearance and deposit into the lower airways, where the air velocity is very low; thus experiencing sedimentation under the influence of gravitational forces. The particles of size greater than 5 μm undergo impaction in the oropharyngeal region from where they are further removed by swallowing. The desired aerodynamic particle size for the drug to settle in alveoli (which is the main target site) is 1–5 μm.
Many of these particles escape mucociliary clearance and deposit into the lower airways where the air velocity is very low; thus experiencing sedimentation under the influence of gravitational forces. The particles of size greater than 5 μm undergo impaction in the oropharyngeal region from where they are further removed by swallowing. The particles less than 1 μm also reach to alveoli; however, it may favor rapid absorption of drug into the systemic circulation from the periphery of the alveoli, where proximity to the blood supply and the large surface area facilitate transport.(8–10)
Several mechanisms are involved in the generation of aerosol. When the patient inhales, the airflow through the device generates turbulence; air penetrates the powder thus leading to the fluidization of the particles. The fluidized particles get separated from the carrier particles and are further carried deep into the lungs, whereas the carrier particles of larger size get trapped into the oropharyngeal region. Lactose is an excipient that is widely used in DPI as a carrier for the micronized drug particles due, in part, to desirable features, including biocompatibility, biodegradability etc.(6,11)
However, the dosing limitation of the carrier-mediated drug delivery strategy needs to be considered, as the carrier molecules constitute major portion of the formulation. Since, the dose of the drug in the DPI remains less, patient's inhalation force plays a key role in the drug administration through DPI. If the patient's inhalation force is less, most of the formulation may remain in the upper airways, owing to less amount of the drug reaching the site of action.(9)
Rifampicin is an essential component of antitubercular treatment stemming from its high affinity to the DNA-dependent RNA polymerase enzyme of the bacteria, which is mainly responsible for the mRNA transcription. Rifampicin has been chosen as the model drug because of its high lipophilicity as the lipophilic drugs show more retention in the lung tissues, which is desirable for local targeting. A variety of formulations were prepared with rifampicin, such as nanoparticles or microparticles, for its localization into the lungs. However, the aerosolized form of rifampicin with the carriers has not been much addressed until date, which may in future serve to be a promising formulation for locally targeting the drug into the lungs.(12–14)
Many researchers are developing nanoparticles, liposomes etc. to deliver the drug at the target site in the lungs. However, these formulations have limitations of poor drug entrapment, poor stability, and high cost.(15,16) Considering the developing countries, where patients cannot afford higher cost of treatment, low-cost conventional dry-powder inhaler formulations are desirable. Furthermore, the micronization may generate positive charge on rifampicin molecules,(17) which may enhance their interaction with the negatively charged sialic acid released by alveolar macrophages for significant targeting into the lungs.(18,19)
The purpose of this study was to develop carrier-mediated DPI of rifampicin with improved aerodynamic properties for better lung targeting. As the formulation is directly administered into the lungs, the in vitro cytotoxicity using macrophage J774 cell lines and in vivo cytotoxicity through histopathology were performed to understand the optimum dose administration. Further in vivo pulmonary pharmacokinetic studies in the suitable animal models were done to determine the potential of developed DPI formulation in comparison to the marketed formulation.
Materials and Methods
Materials
Rifampicin and hydroxypropyl methylcellulose capsules (rotacaps) were obtained as a gift sample from Cipla Ltd. Mumbai. Rotahaler® and Revolizer® were purchased from a local vendor. Lactose grades (Inhalac® 230 and Inhalac 400) were obtained as a gift sample from Meggle, Germany. Other grades (Respitose® SV003, Respitose SV010, Respitose ML001, Respitose ML006, and Lactohale® LH 230) were obtained as a gift sample from DMV-Fonterra Excipients GmbH & Co. The cellophane membrane was purchased from HiMedia, India. All the chemicals and reagents used were of analytical grade. The protocol for the animal study was approved by the Institutional Animal Ethics Committee held at the Institute of Pharmacy, Nirma University (Project No. IP/PCEU/PHD/19/009).
Particle size distribution, density, and aerodynamic diameter
The particle size distribution of micronized rifampicin was analyzed by Malvern Mastersizer (Hydro 2000 MU). Bulk and tapped volumes were determined by the method as per the United States Pharmacopoeia (USP).(20) The bulk and the tapped densities were further calculated. The flow properties of the powder were then determined by calculating Hausner ratio. Theoretical estimates of aerodynamic diameter were obtained from the particle size data and the tapped density values as per given equation:
where ρ1 = 1 g cm−3 and ρ is the tapped density, Dae and DV0.5 are the aerodynamic and volume mean diameters and λ is the dynamic shape factor.
Preformulation studies
Drug excipient compatibility studies by Fourier transform infrared spectroscopy
In DPI formulation, drug remains in intimate contact with the carriers, which could affect the stability of the drug. Hence, the knowledge of drug–excipient interactions becomes necessary. The drug–lactose compatibility studies were done using Fourier transform infrared spectroscopy (FTIR) (Jasco FTIR 6100, Japan). The powder blend and KBr were thoroughly mixed in 1:1 ratio and FTIR spectra were recorded in the range of 4000–400 cm−1 after 72-hour storage at room temperature.
Interference study of capsule shell and lactose
The coarse and fine lactose blend (placebo) was filled in a rotacap and was dissolved in the solvent that is, water:acetonitrile (55:45). Similarly, the blend of the drug and the lactose filled in another rotacap was also dissolved in the same solvent. Then the analysis was done using high performance liquid chromatography (HPLC) (Jasco PU-2080 Plus, Japan). The column used was Inertsil ODS 3 V (250 × 4.6 mm × 5 μ). The mobile phase comprising of isocratic solution of buffer pH 2.27:acetonitrile in the ratio of 55:45 was eluted at a flow rate of 1 mL/min at 230 nm.
Formulation development
Preliminary studies
Numerous preliminary batches were prepared with different coarse lactose grades such as Inhalac 120, Inhalac 230, Respitose SV010, Respitose SV 003, Respitose ML 001, and fine lactose grades such as Inhalac 250, Inhalac 400, Respitose ML006, and Lactohale LH 230 and were evaluated for flow properties, emitted dose (ED), fine particle dose (FPD), content uniformity, and blend uniformity. Among the devices, functionality of Rotahaler and Revolizer were evaluated and the selection was done on the basis of the minimum amount of drug left in the capsule and device.
Preparation of rifampicin DPI
Preblends of Inhalac 230 and Inhalac 400 were prepared by modifications done in the reported method.(21) The fine lactose was first added to half the quantity of the coarse lactose and mixed for 2 minutes. Furthermore, the remaining amount of coarse lactose was added and mixed for 2 minutes. Then the blend was mixed thoroughly in a vial for 10 minutes using vortex mixer (Eie Instruments Pvt. Ltd., Ahmedabad). After storage of this preblend for24 hours, micronized drug was added to the preblend and then the above mixture was mixed using vortex mixer for 15 minutes. The prepared mixture equivalent to 50 mg rifampicin was filled in the rotacaps. All the batches were analyzed for various parameters like flow properties, blend uniformity, content uniformity, ED, and FPD.
Optimization of rifampicin DPI
The 32 full factorial experimental design was applied for the optimization of various formulations and process parameters for the preparation of the DPI as per Table 1. The amount of drug (X1) and amount of fine lactose (X2) were selected as the independent variables. Each factor was set to three levels. Nine formulations were prepared according to the design. Flow properties, density, ED, FPD, blend uniformity, and content uniformity were taken as response parameters. Design expert 7.0.0 software was used for data treatment and design space generation.
Characterization
Flow properties of the micronized drug and the blend
The flow properties were determined by the method as per USP.(22) After determination of bulk and tapped volume, the bulk and tapped densities were calculated. The experiment was done in triplicate. The flow properties of the powder were further determined by calculating Hausner ratio as below:
Blend uniformity
An accurately weighed quantity of the blend was evaluated for drug content. The blend was dissolved in 100 mL of the solvent and was allowed to sonicate for 10 minutes with intermittent shaking until it dissolved completely. The drug content was determined using HPLC after filtration through a 0.45-μm syringe filter. The analysis was done in triplicate.
Content uniformity
Content from 10 capsules of each formulation were separately dissolved in about 100 mL of phosphate buffer pH 7.4 and were sonicated for 10 minutes. Then samples were analyzed after suitable dilution as per method described in blend uniformity. Homogeneity of the sample was considered if not more than one capsule content was outside the limits 85%–115% of the mean rifampicin content and none was outside 75%–125% of the mean rifampicin content. The analysis was done in triplicate.
Determination of device resistance
The device was loaded with an empty capsule and attached to dosage unit sampling apparatus, which was further connected to a high-capacity vacuum pump (Erweka DFM 2000) through a critical flow controller (Copley Scientific Limited, Model ADL/579). At each pressure drop value, the flow rate was recorded.(23,24) Device resistance was determined by the formula:
Mass balance and in vitro deposition studies
Before carrying out the in vitro deposition studies, it is necessary to determine the mass balance, which means the balance between entry and exit of a material in a system. Mass balance in terms of Andersen Cascade Impactor (ACI) refers to the total mass of active pharmaceutical ingredient recovered from an impactor.(25) After the determination of mass balance, the in vitro deposition studies were performed by an eight-stage ACI (Thermo Fisher Scientific) containing stainless steel collection plates and fine particle fraction (FPF) and mass median aerodynamic diameter (MMAD) were determined. For imitating the throat of a human, throat piece referred to as “USP throat”(26) was used. It was connected to the top of the ACI. The mouthpiece adaptor was fabricated as per Rotahaler® design. The induction port and preseparator were used to complete the impactor for DPI. The preseparator was filled with 15 mL of solvent. The rotacap filled with the powder blend equivalent to 50 mg rifampicin was further loaded into the Rotahaler®. Inspiration of single dose of formulation (n = 3) was done for 8 seconds at a flow rate of 30 L/min.
After performing the experiment, the particles on each stage were washed with the HPLC solvent (water:acetonitrile in the ratio 55:45) and volume was made up to 20 mL using a calibrated standard volumetric flask. Rifampicin content was determined using HPLC. The cumulative percentage of dose from stages 2 to 5 depicts the FPF of the formulation which represents the cutoff diameter of the particles less than 5 μm. The FPF was determined by using Copley Inhaler Testing Data Analysis Software (CITDAS, Version 3.10). All the experiments were performed in triplicate.
Antimicrobial activity
Antimicrobial studies were conducted using agar well diffusion method to determine the retention of rifampicin activity in DPI formulation. As Bacillus subtilis shows high susceptibility to rifampicin, B. subtilis ATCC 6633 strain was taken as an indicator microorganism on the nutrient agar medium.(27) The wells were filled with different concentrations of rifampicin DPI solutions (0.25 and 0.5 mg/mL) and pure rifampicin solution (0.5 mg/mL). Plates were incubated at 37°C for 24 hours to determine the zone of inhibition.
Scanning electron microscopy
The surface morphology of micronized rifampicin, the combination of coarse and fine lactose, and the DPI formulation was observed using the LEO 1530 Scanning Electron Microscopy (SEM) (Oberkochen, Germany). The plasma deposition method was used employing a gold coating unit to make the sample surface conductive to the scanning electron beam. The gold coating of about 40–100 A° was done under the argon atmosphere. The SEM of gold-coated samples was carried out at high vacuum with specimen working distance of 17.4 mm and an accelerating voltage of 30 kV.
Cell viability assay
Cytotoxicity was evaluated using murine macrophages J774 cell lines grown in Dulbecco's modified Eagle's medium, supplemented with 10% heat-inactivated fetal bovine serum with 5% CO2. Cells were seeded in 96-well plates at a density of 1 × 105 cells/well and incubated overnight at 37°C to allow cells to adhere. The medium was then removed and cells were incubated with 180 μL of the fresh medium containing two rifampicin samples (pure rifampicin and dry-powder formulation) at 0.125, 0.25, 0.5 mg/mL concentration for 6, 12, and 24 hours. At these time points, 20 μL of Cell Titer Blue Reagent (Promega) was added to each well. Then cells were incubated for another 2 hours at 37°C, to reduce resazurin to resorufin. Fluorescence was measured at 540 nm excitation and 590 nm emission. The percentage of cell survival was determined in comparison to the control wells. The experiment was performed in triplicate.(27,28)
In vivo pulmonary pharmacokinetic studies
Lungs were homogenized in phosphate-buffered saline (PBS) and acetonitrile was added with vortex mixing for protein precipitation. The standard curve was plotted by spiking known amounts of rifampicin for the analysis of extracted lungs. Animal protocols were approved by the Institutional Animal Ethics Committee, Nirma University. The in vivo pulmonary pharmacokinetic studies of DPI formulation were compared with the marketed formulation of rifampicin to investigate the local action of dry-powder formulation. Two groups of 18 male Wistar rats (220–250 g) each were used for the study. Rats were placed in individual cages at constant temperature and were given free access to water ad libitum. Rats were kept on fasting overnight before experimentation, mouth of rats of Group I (conventional DPI) were sealed, and animals were allowed to inhale about 313.56 mg/Kg of formulation.
The second group animals were orally administered the marketed formulation in solution form (1 mg/mL) through oral cannula. Three animals from both groups were euthanized at 1, 3, 6, 9, 12, and 24 hours after administration. The extracted lungs from experimental rats were homogenized in 10 mL PBS. The lung tissues were deproteinized by the acetonitrile treatment and rifampicin released in the supernatant was analyzed by HPLC. The mean pulmonary pharmacokinetic parameters Cmax, tmax, AUC0–24, and t1/2 were calculated as reported elsewhere.(29)
In vivo toxicity studies
One animal from Group I was allowed to inhale the formulation after sealing its mouth. Twenty-four hours postinhalation, lungs were extracted and were stored in 10% formalin solution to conduct histopathological studies to determine toxic effects. The histopathology of the extracted lungs of DPI-treated animals in comparison to marketed formulation-treated group was carried out.
Stability studies
The selected formulation was subjected to stability studies as per ICH guideline at room temperature (25 ± 2°C/60% ± 5% relative humidity (RH)) and accelerated conditions (40 ± 2°C/75% ± 5% RH) up to 6 months. The blend uniformity values were determined after 3 and 6 months. The studies were done in triplicate.
Statistical analysis
Each batch of animals was prepared three times, and data values were expressed as mean ± standard deviation. A difference between means was considered significant, if p-value is equal to or less than 0.05.
Results and Discussion
DPI is widely used to deliver the drug to the lungs and is formulated using various carriers like lactose, mannitol, trehalose etc. Among all, lactose is widely used due to its well-explored toxicity profile, physical and chemical stability, compatibility profile, ease of availability, and low price.(30) The fine particles of the drug adhere onto the surface of coarse lactose and upon inhalation, coarse lactose remains in the upper respiratory tract, whereas the fine particles of the drug enters deep into the lungs. However, it is difficult for a complete dose of the drug to detach from the coarse lactose, which leads to dose inaccuracy.
It is reported that the coarse lactose should be mixed with small quantities of fine lactose so that fine lactose occupy the high adhesion sites (active sites) on the surface of coarse lactose.(31–36) This preblend was then mixed with the fine particulate drug. This results in binding of the drug on to the low adhesion sites (less active sites) on the coarse lactose which facilitates an easy detachment of the drug upon inhalation. In the present study, DPI of rifampicin was developed using various combinations of drug, coarse and fine lactose grades.
Particle size distribution and aerodynamic diameter of rifampicin
In DPI, the particle size of the drug and the carrier play a vital role in delivering the drug to the target site and hence the efficacy of formulation. The particle size distribution of the micronized drug was determined by Malvern Mastersizer. The particle size distribution of rifampicin and grades of coarse and fine lactose are presented in Table 2. In spite of the particle size distribution, aerodynamic diameter can be better correlated with the drug deposition in lungs. It is reported that the aerodynamic diameter in the range of 1–5 μm is desirable for the drug particles to get deposited deep into the lungs. The aerodynamic diameter calculated for micronized rifampicin was 3.325 μm, which is within the required range.
Preformulation studies
Drug excipient compatibility studies
Drug and excipient compatibility studies were conducted by FTIR. The FTIR spectra of rifampicin and mixture of rifampicin and lactose have been shown in Figure 1, which indicated the presence of identical peaks (3333, 2935, 1726, and 1649 cm−1) in both rifampicin as well as its mixture with the excipients thus showing the compatibility of the drug and the excipients.
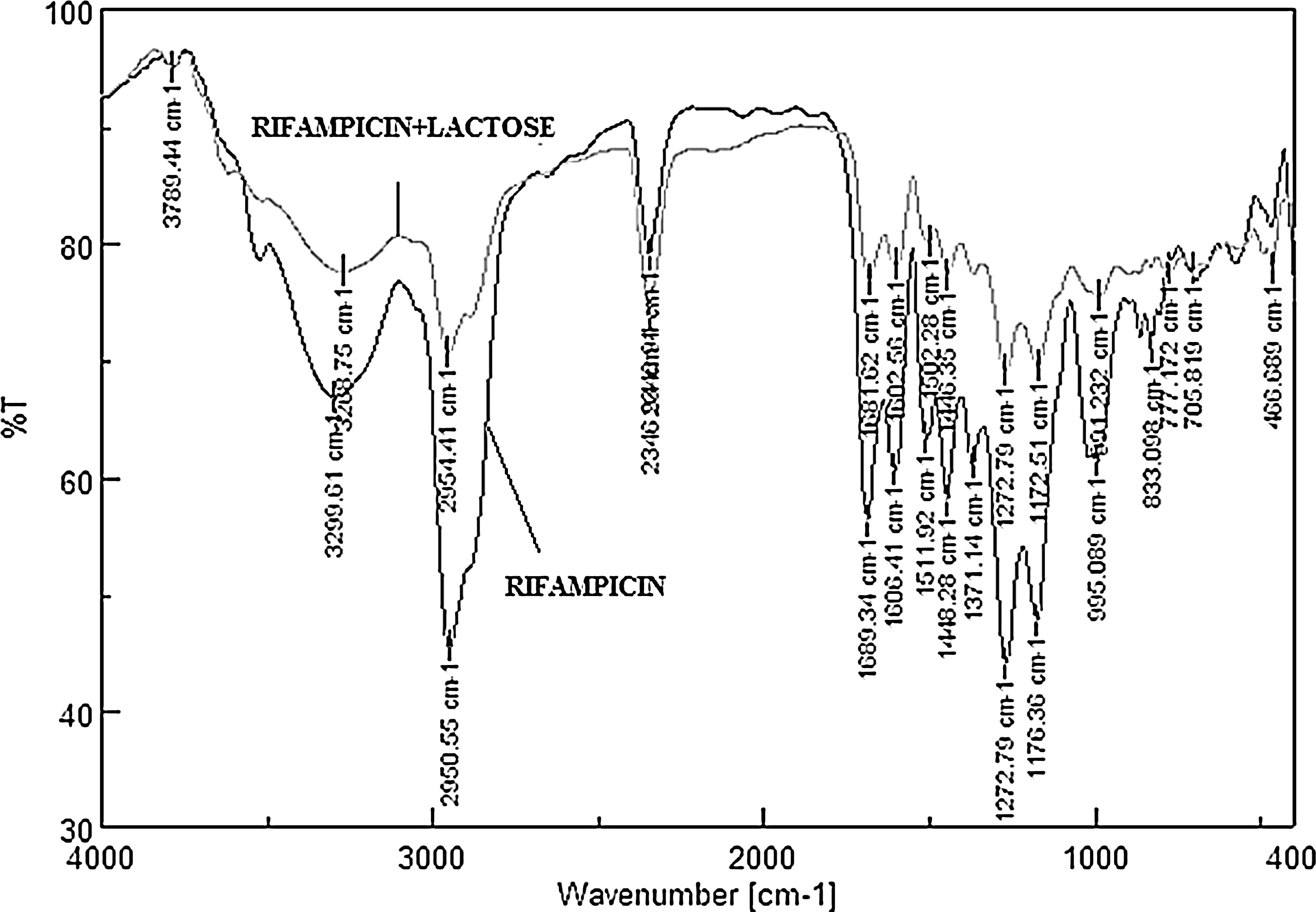
FTIR spectra of
Interference study of capsule shell and lactose
The reported HPLC method was used with some modifications.(37) Chromatogram of the capsule containing lactose was a straight line, whereas the characteristic peak of the drug was observed in the case of the capsule containing the blend of drug and lactose. It revealed that interference was not exhibited by the capsule shell and lactose.
Preliminary trials
Several preliminary batches were prepared using various ratios of coarse lactose grades like Inhalac 120, Inhalac 230, Respitose SV010, Respitose SV 003, Respitose ML 001, and fine lactose grades such as Inhalac 250, Inhalac 400, Respitose ML006, and Lactohale LH 230. Out of these, Inhalac 230 was selected as coarse lactose in combination with Inhalac 400, a fine lactose grade based on their good flow properties. So this combination was chosen as the carrier for further optimization.
Optimization
Quality by design (QbD) is a well-known concept being used in many industries to build quality in the product. The USFDA made it mandatory to use these concepts in pharmaceutical formulation development and design of experiments (DOE) is one of the tools of QbD. However, QbD is a newer concept, but researchers have been using DOE since long specially for formulation development. Various optimization designs can be used based on the outcome of the preliminary trials. There are a few excipients required in the DPI, and in the present investigation, we have observed that the amount of drug, fine lactose, and coarse lactose were important factors affecting the performance of the DPI. Hence 32 full factorial design was used taking the amount of drug as X1 and amount of fine lactose as X2. Nine batches were prepared and evaluated extensively for following parameters.
Flow properties of the micronized drug and the blend
The micronized rifampicin showed higher value of the Hausner ratio (1.58), whereas the design batches showed the Hausner ratio between 1.21–1.25, except batch C3. As per the Chapter 1174, powder flow of USP [16], the micronized rifampicin, can be characterized in the category of “exceedingly poor flow” and the design batches in the “fair flow” properties, except batch C3, which showed the Hausner ratio of 1.33 depicting the “poor flow.” This might be due to the presence of more amounts of the drug and the fine lactose. Large amounts of fine lactose might have bound to both high as well as low adhesion sites of the coarse lactose, thereby not allowing the rifampicin to bind to the coarse lactose. This might have led to the poor flow of the blend. However, the developed formulation fulfilled the requirement of minimum flow properties for filling the blend into the capsule shell.
Blend uniformity
As per Chapter 601, aerosols, nasal sprays, metered-dose inhalers, and DPIs of USP,(20) the drug content for a DPI must be within 85%–115% of the label claim. The results have been shown in Table 3. All the batches were found to be within the assay limits. However, the batches A3, B3, and C3 containing higher proportion of fine lactose showed poor blend uniformity. This might be due to the fact that as the fine lactose was increased, it does not allow the drug to properly bind to the coarse lactose. Additionally, these batches showed poor flow properties, which might also contribute to the poor blend uniformity.
All values are expressed as mean ± SD; n = 10.
SD, standard deviation.
The complete polynomial regression model for the blend uniformity of the design batches was described by the following equation:
The above equation shows that the amount of drug (X1) had a positive impact and the amount of fine lactose (X2) had a negative impact on the blend uniformity. As percent of the drug in the total content increased, the lower amount of it adhere to the capsule shell as well as the device thus resulting in the increase in blend uniformity. The increase in the fine lactose leads to poor flow properties, which might be responsible for its negative effect on the blend uniformity.
Content uniformity
As per the USP, the amount of active pharmaceutical ingredient should not be outside 80%–120% of the label claim for more than one of the 10 capsules, none of the capsules should be outside 75%–125% of the label claim, and the average should not be outside 85%–115% of the label claim. The average of the ten capsules of each batch was found to be within 85%–115% of the label claim (Table 3). But again, in the case of batches A3, B3, and C3, the average value of the content uniformity was low. This indicates that increase in the proportion of the fine lactose negatively affected the content uniformity.
Device resistance calculation
The device resistance is a parameter which is inversely proportional to the flow rate. If the device resistance is less, the flow rate required will be more. Since in tuberculosis, the inspiratory flow rate of a patient reduces, so in this perspective a device with medium to high resistance is required. The criterion for the device resistance has been shown in Table 4. The device used in the present work was Rotahaler®. Rotahaler® was operated at different pressure values so as to set different flow rates as shown in Table 5. The device resistance at different flow rates varied from 0.033 to 0.034, which indicated that Rotahaler® fall in the upper border of medium-level resistance. The operating flow rate used for the developed rifampicin DPI for further ACI analysis was 30 L/min, which was achieved at 1 KPa pressure.
In vitro deposition studies by Andersen cascade impactor
Before carrying out the in vitro deposition, the mass balance was determined.(38) The mass balance within the limits of 85%–115% is acceptable. All the batches showed a mass balance of around 100%–115%, thereby revealing no drug loss in the system (Table 6). Furthermore, for a drug to act deep into the lungs, proper deposition is required. ACI serves as one of the best tool to perform in vitro deposition studies due to its several merits. First, it serves as a very effective device for the determination of mass median aerodynamic diameter (MMAD) of the inhalation formulation, which is a key factor influencing deposition of the drug in various regions of the lungs and the respiratory tract.
All values are expressed as mean ± SD; n = 3.
FPF, fine particle fraction
Second, ACI chiefly determines the fraction of the drug which gets deposited deep in the lungs (also known as FPF), thus providing the best resolution for the particles in the desired size range for DPI, that is, 1–5 μm. ACI fundamentally functions on the principle of inertial impaction (separation based on the inertial differences, which is a function of particle size and velocity). It basically consists of eight stages with a cutoff diameter between 0.7 and 10 μm.(39) The particles of the desired size range of 1–5 μm reside in the stages 2–5 of the ACI, as the cutoff diameter of these stages lie between 1.1 and 4.7 μm. The results of FPF and MMAD values for all the batches have been shown in Table 6. The in vitro deposition of all the DPI formulation from stages 2 to 5 has been shown in Figure 2 and the overlay plot showing design space has been shown in Figure 3. The polynomial equation obtained for the FPF was:

Comparative in vitro deposition studies of the design and the optimized batches.
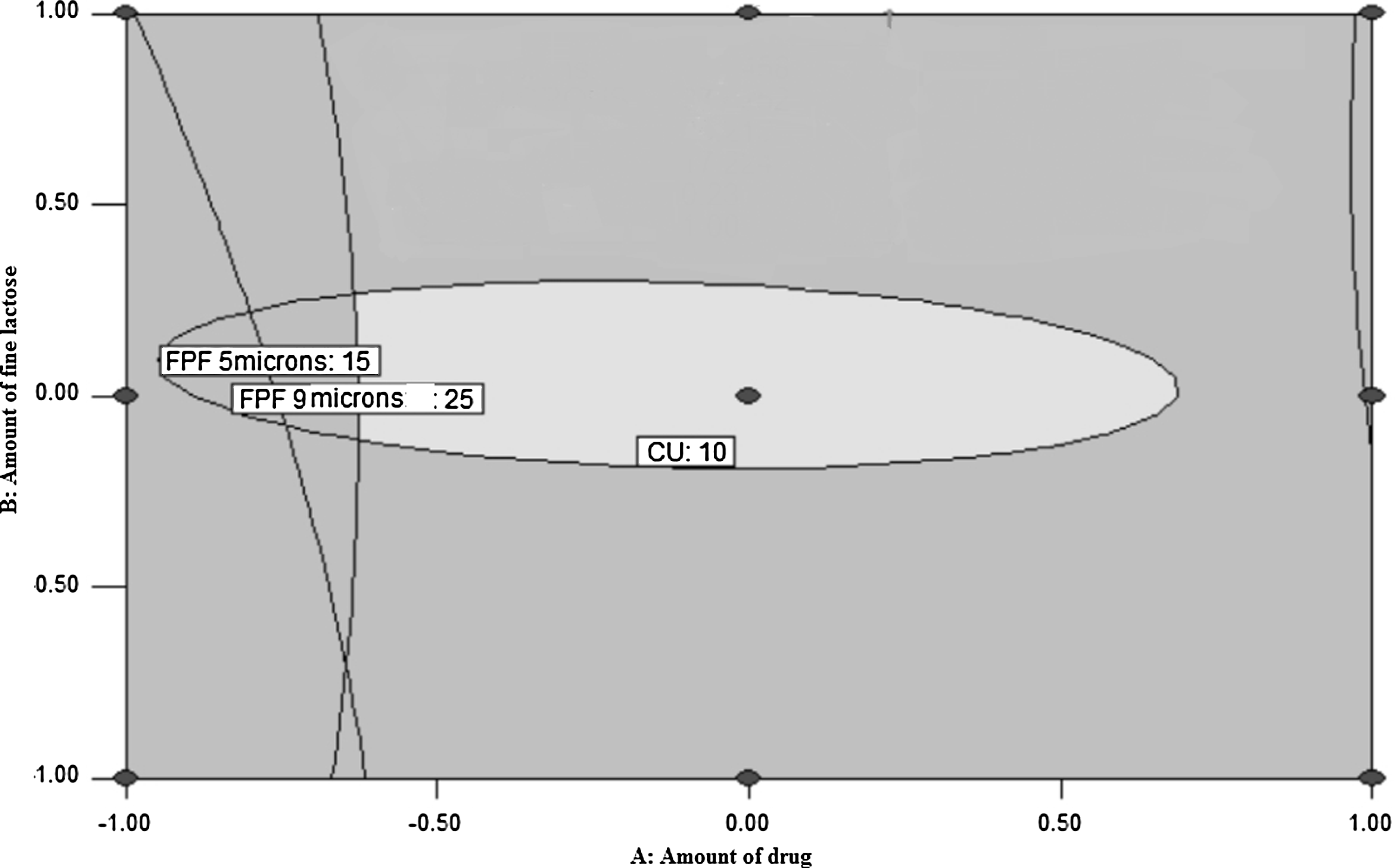
Overlay plot showing design space.
The above equation shows that both factors, that is, the amount of drug and amount of fine lactose had a positive impact on the FPF. This might be due to the fact that as the amount of fine lactose increased, it bound effectively with the active sites of the coarse lactose, and thus preventing the binding of the drug to such sites. This might lead to ease of detachment of the drug from the coarse lactose leading to high FPF.
Antimicrobial activity
Next, we decided to determine antimicrobial activity of rifampicin–DPI formulation by an agar well diffusion method. Our results show nearly the same antimicrobial activity as that of pure rifampicin. The zone of inhibition estimated by pure rifampicin solution, 0.5 and 0.25 mg/mL of rifampicin DPI were calculated to be 20.4 ± 0.67, 18.4 ± 0.41, and 17.2 ± 0.20 mm, respectively. In brief, our results indicate that rifampicin antimicrobial activity remained intact when delivered through DPI formulation (Fig. 4).

In vitro antimicrobial studies of pure rifampicin and developed DPI formulation on Bacillus subtilis ATCC 6633. The representative experiment is a mean of three independent experiments. DPI, dry-powder inhaler.
Scanning electron microscopy
The SEM images (Fig. 5) show that the fine lactose has occupied most of the active sites of the coarse lactose (
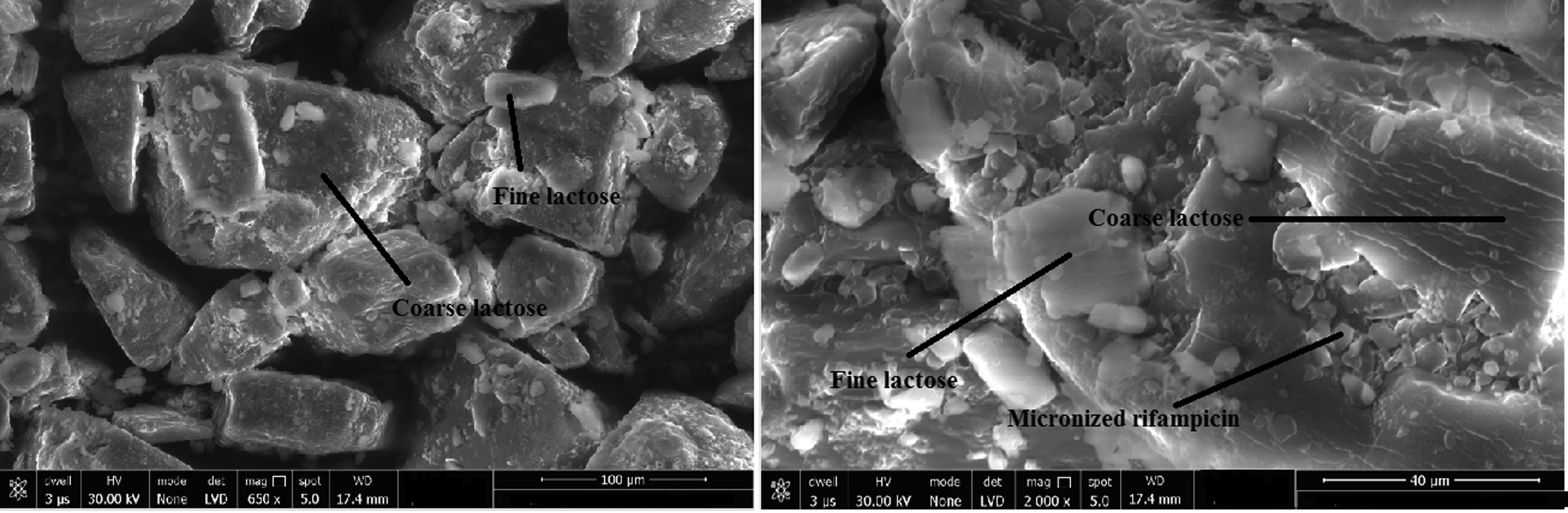
Analysis of optimized formulation through SEM,
Cell viability assay
The drug delivery to the lungs for tuberculosis is to have a local targeting of the drug for the improved clinical outcome. In that context, the dose for the lung delivery can be directly taken up considering the dose per kilogram body weight to the organ weight, which is 10 mg/kg in the case of rifampicin. Since the weight of the human lungs is ∼1 kg, considering 20% of the drug will reach the target site, 50 mg of the drug can be taken to formulate DPI. This would help to attain local minimum inhibitory concentration over24 hours. However, lung clearance needs to be studied. To check the safety of the formulation, % cell viability studies were performed using macrophage J774 cell lines. The cytotoxicity test results, expressed as % cell viability (survival) v/s incubation time, have been shown in Figure 6. The observed effect of dry-powder formulation on cell viability was similar as that of the pure rifampicin. Negligible cytotoxicity with about 75%–80% of cell viability was observed after 6 and 12 hours exposure of 0.125 mg/mL dose.
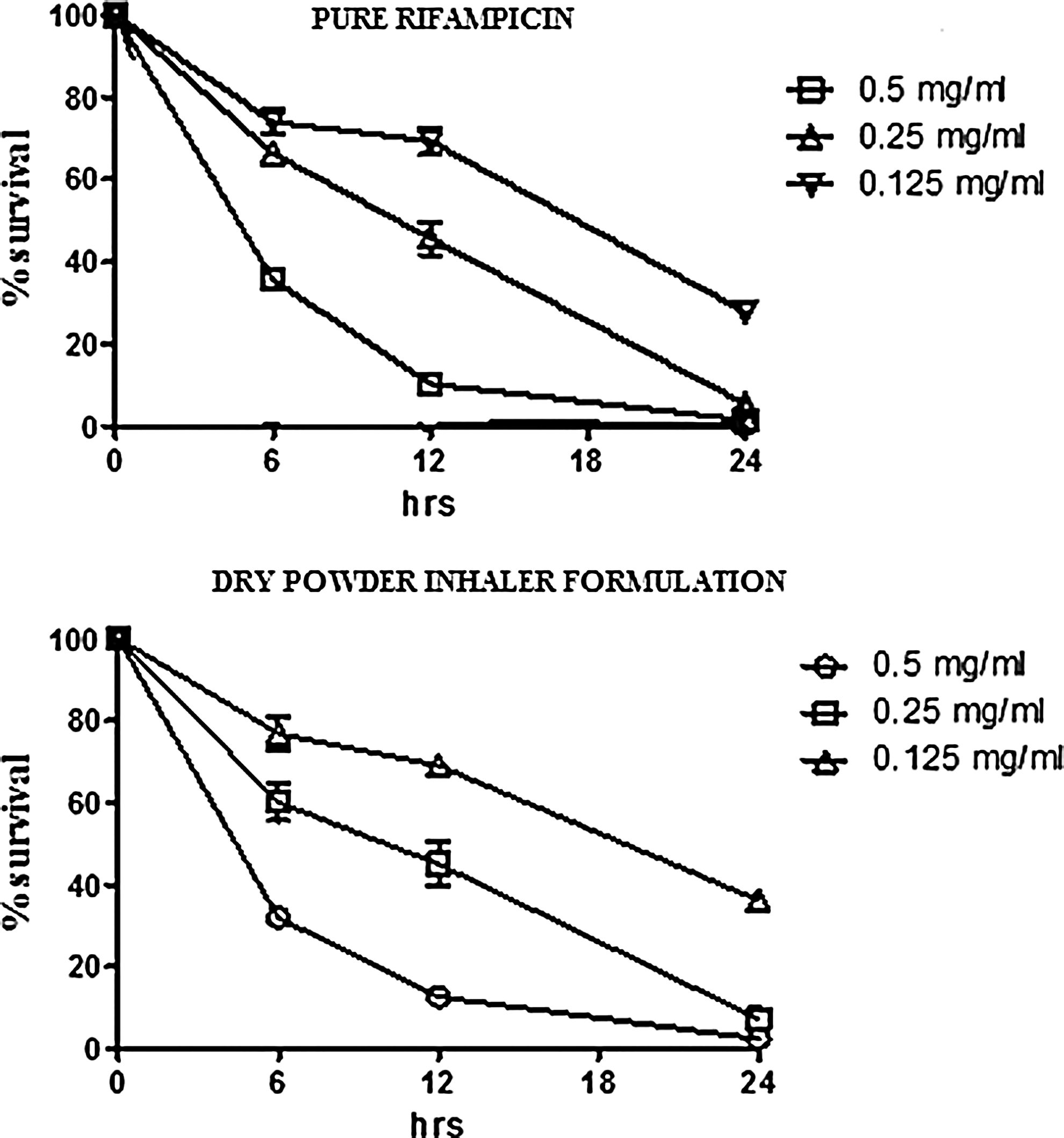
Cell viability studies of pure rifampicin and developed DPI formulation on macrophage J774 cell lines. The representative experiment is a mean of three independent experiments.
However, higher concentrations, that is, 0.25 and 0.5 mg/mL, showed some toxicity. Considering the slow drug release profile and volume of the fluid available in the lungs, we can assume that the maximum concentration of rifampicin attained in lungs would be safe. Furthermore, considering the higher number of human alveolar macrophages dispersed on the total surface area of alveoli compared with that of the cell culture,(40) the formulation can be considered as noncytotoxic. However, in vivo pulmonary pharmacokinetic studies were carried out to measure rifampicin concentration in the lungs.
In vivo pulmonary pharmacokinetic studies
The primary objective of the in vivo studies was to demonstrate drug concentrations in the lungs after administration of developed DPI in comparison with oral marketed product. Administration of dose equivalent to 50 mg human dose in the form of DPI gave higher drug concentration in lungs in comparison to 600 mg human dose of marketed product. Thus, we can assume a lower concentration of drug in blood after the use of DPI.(25,41)
However, an additional blood analysis could have been done to understand the safety of the formulations. The comparative drug concentration in the lungs and time profiling of all the formulations tested are shown (Fig. 7). A marked increase of 1.5-fold was seen in Cmax of Group I treated with the developed DPI formulation (970.76 ± 60.83 μg/mL) in comparison to Group II treated with marketed formulation (677.03 ± 47.61 μg/mL). Furthermore, marked increment of t1/2 and AUC0–24 was seen in Group I (10.26 ± 1.15 and 8783.33 ± 100.66) when compared with Group II (3.33 ± 0.58 and 4140.51 ± 84.77). The increased t1/2 in Group I may be due to improved local retention of rifampicin in the form of conventional DPI, which indicates the potential use of this lung-targeted DPI formulation to deliver rifampicin for an effective pulmonary administration.
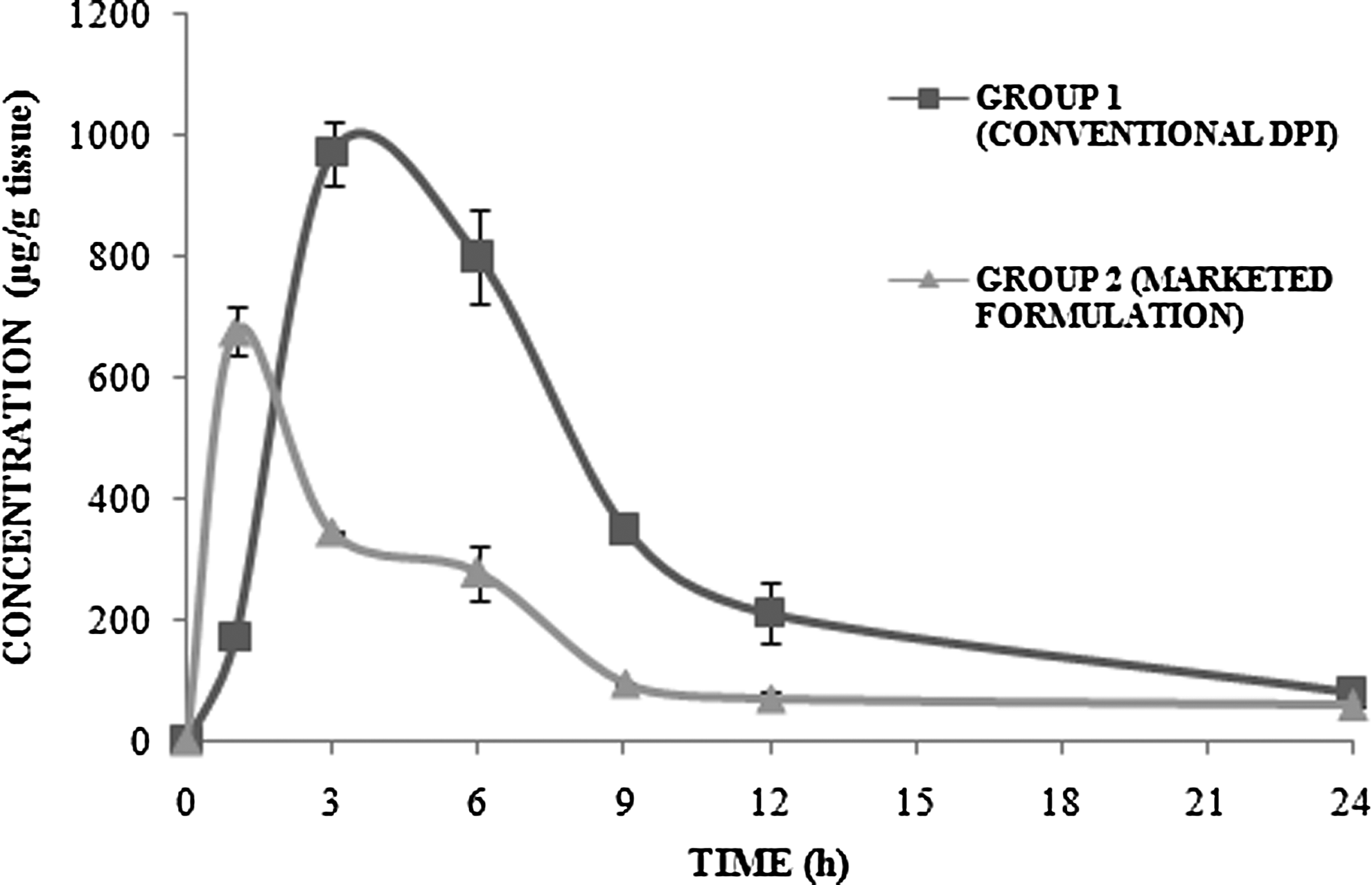
Comparative in vivo pulmonary pharmacokinetic studies of developed DPI formulation and marketed formulation.
In vivo toxicity studies
The administration of conventional DPI (Group-I) produced mild changes in the pathology of treated lungs (Fig. 8B) in comparison to normal lung (Fig. 8A) showing hardly any toxicity. Whereas Group-II administered with the marketed formulation showed severe toxicity in peribronchial infiltration of inflammatory cells, hyperplasia of lymphoid tissue, and interalveolar septal thickening (Fig. 8C). Thus, it is inferred from our results that local targeting of rifampicin through conventional DPI is nontoxic and safe to use. However, repeated dose toxicity studies are indeed required to assess the long-term safety of the formulation.

Photomicrographs of rat lungs showing histopathological changes,
Stability studies
The results for the stability studies of the formulation are shown in Table 7. It can be concluded from the studies that the developed DPI was stable even after 6 months as the blend uniformity was within the limit (85%–115%) at room temperature as well as accelerated conditions.
All values are expressed as mean ± SD; n = 3.
RH, relative humidity.
Conclusion
The rifampicin DPI formulation was developed systematically and evaluated extensively. The optimized formulation of DPI when evaluated using Rotahaler®, showed desired MMAD (1–5 μm) and higher FPF (28.9%). The in vivo pulmonary pharmacokinetic studies showed the improved localized retention of rifampicin in the DPI-treated group in comparison to the marketed formulation. No signs of severe toxicity were seen in the histopathological studies. Thus, from the above studies it can be concluded that rifampicin DPI can serve as a safe formulation to provide better local drug concentration in the lungs in comparison to the marketed formulations.
Footnotes
Acknowledgments
The authors would like to thank the Institute of Pharmacy, Nirma University, Ahmedabad, for providing them all the facilities to carry out their research work. The authors acknowledge the Department of Science and Technology, Government of India for financial support vide reference no. SR/WOS-A/LS-1119/2015 (G) under Women Scientist Scheme. The authors kindly thank Zydus Cadila Healthcare Ltd., Ahmedabad, for granting them permission to work on Andersen Cascade Impactor and Lupin Ltd. Aurangabad for providing them rifampicin as gift sample. They would also thank Dr. Rajeev Tyagi and Mr. Rajesh Parmar for helping them in carrying out pulmonary pharmacokinetic studies. They would also like to thank Meggle Germany and DFE Pharma for providing them various inhalable lactose grades.
Author Disclosure Statement
No competing financial interests exist. The authors are responsible for the overall content and writing of the article.