
Abstract
Abstract
Background:
Remote inhaler monitoring is an emerging technology that enables the healthcare team to monitor the time and location of a patient's inhaler use. We assessed the feasibility of remote inhaler monitoring for chronic obstructive pulmonary disease (COPD) patients and the pattern of albuterol inhaler use associated with COPD exacerbations.
Methods:
Thirty-five participants with COPD used an electronic inhaler sensor for 12 weeks which recorded the date and time of each albuterol actuation. Self-reported COPD exacerbations and healthcare utilization were assessed monthly. We used generalized estimating equations with a logit link to compare the odds of an exacerbation day to a nonexacerbation day by the frequency of daily albuterol use.
Results:
Average daily albuterol use on nonexacerbation days varied greatly between patients, ranging from 1.5 to 17.5 puffs. There were 48 exacerbation events observed in 29 participants during the study period, of which 16 were moderate-to-severe exacerbations. During the moderate-to-severe exacerbation days, the median value in average daily albuterol use increased by 14.1% (interquartile range: 2.7%–56.9%) compared to average nonexacerbation days. A 100% increase in inhaler use was associated with increased odds of a moderate-to severe exacerbation (odds ratio 1.54; 95% CI: 1.21–1.97). Approximately 74% of participants reported satisfaction with the sensor.
Conclusions:
The electronic inhaler sensor was well received in older patients with COPD over a 12-week period. Increased albuterol use captured by the device was associated with self-reported episodes of moderate-to-severe exacerbations.
Introduction
R
Materials and Methods
Study design and participants
We conducted a 12-week pilot study in Veterans with COPD from December 2011 to January 2014. Inclusion criteria included: (1) veterans receiving care at VA Puget Sound Healthcare System in Seattle and Tacoma, Washington, (2) clinical diagnosis of COPD, (3) currently using an albuterol inhaler, (4) over 40 years of age, (5) former smoker with >10 pack year history, (6) residence in King or Pierce Counties in Washington State (due to availability of air pollution monitors needed for a secondary aim for the study), (7) post bronchodilator forced expiratory volume in 1 second (FEV1)% predicted ≤80%, and (8) no exacerbations in the 4 weeks before enrollment.
Exclusion criteria were: (1) diagnosis of asthma and (2) Modified Medical Research Council (MMRC) dyspnea scale score of 4 (too breathless to leave the house or breathless when dressing). Housebound patients with very severe COPD (MMRC scale of 4) were excluded due to a secondary aim of the study that evaluated the relationship of COPD exacerbation with air pollution and physical activity, which is not included in this analysis. This study was approved by the VA Puget Sound Healthcare Center IRB (ID: 00408). All participants provided informed consent.
At baseline, participants completed questionnaires regarding medical history, respiratory symptoms, physical activity, and health related quality of life. In the medical history questionnaire, participants were asked if they had a nebulizer device, whether it was used for albuterol or ipratropium, and how often they used it. Participants completed the University of California San Diego (UCSD) Shortness of Breath Questionnaire (SOBQ).(9) The 24-item questionnaire assesses dyspnea with various activities of daily living (scores range from 0 = best to 120 = worse), with a minimal clinically important difference of five points.(10) The mean SOBQ score among a previous cohort of COPD patients was 63.4 (standard deviation: 18.5).(11) COPD exacerbations and breathing symptoms were ascertained during monthly interviews as stated below. All participants were given a daily diary to record respiratory symptoms, treatment of exacerbations, and the number of daily puffs during the 3-month follow-up period.
Inhaler sensor
The study contracted with Propeller Health (Madison, WI) to provide participants the FDA-cleared portable electronic inhaler sensor to monitor participants' albuterol use. The sensor and the Propeller Health System are described elsewhere.(6) With the exception of the first three participants who used an earlier version of the sensor, all study participants used an inhaler sensor mounted to the end of the MDI canister by means of a small adapter cap (Sensor Model I, Fig. 1) and were provided a mobile smartphone to use for the study. Using a secure, low-power, wireless radio protocol, the sensor transmitted collected data to the paired mobile smartphone, which then communicated event information to the system servers. The sensor contained a real-time clock and operating system which time-stamped each separate actuation event when it occurred. Industry standard encryption was used for all exchanges of personal health information with the Propeller Health application.

Inhaler sensor.
In this observational pilot study, participants were instructed to continue their COPD medications prescribed by their caring provider as directed. The study staff did not provide any specific instruction on how often or when to use their albuterol MDI to capture the participants' actual rather than optimal usage pattern. If the participant used nebulized medications such as albuterol or ipratropium, they were also instructed to continue to use these medications as prescribed by their medical care provider.
After completion of the study, participants were provided a satisfaction questionnaire to evaluate their experience with the sensor. Because of the differences in design between the preliminary version of the inhaler sensor used by the initial three subjects, results from the satisfaction questionnaire included responses from those who used the more recent Model 1 version.
COPD exacerbations
Each month participants were asked by phone if they developed symptoms of a COPD exacerbation during the past 4 weeks, including any details related to treatment and healthcare use. COPD exacerbations were self-reported and defined as an increase in, or new onset of, one or more respiratory symptoms (cough, sputum, wheezing, dyspnea, or chest tightness) lasting for two or more days. Exacerbations were categorized as symptom only (mild), requiring the use of prednisone and/or antibiotics (moderate) or requiring care in the emergency department (ED) or hospitalization (severe). To ensure that all participants began the study at their baseline stable state, participants were required to wait at least 4 weeks after any COPD exacerbation before study enrollment. Dates of ED visits and hospitalizations were confirmed in the subject's VA electronic medical record when available.
Analysis
Using daily self-reported exacerbation status (exacerbation day vs. nonexacerbation day) as the unit of analysis, we used generalized estimating equations with a logit link to compare the odds of an exacerbation day compared to a nonexacerbation day by the frequency of albuterol use. Using log transformed puffs per day as the primary predictor we calculated the average odds of an exacerbation day associated with a 25%, 50%, and 100% increase in albuterol use. We considered the following potential confounders: FEV1% predicted, supplemental oxygen use, exacerbation within the previous year, concurrent inhaler therapy (long-acting beta-agonist, long-acting anticholinergic, or inhaled corticosteroid), gastroesophageal reflux disease,(12) and dyspnea(11) (measured at baseline by the SOBQ).(9) FEV1% predicted and inhaled corticosteroid use was associated with inhaler use in bivariate analysis and was therefore included in the final model.
To investigate whether the relationship between albuterol use and the odds of an exacerbation differed by exacerbation severity, we performed subgroup analyses to compare (1) mild exacerbation days to nonexacerbation days and (2) moderate-to-severe exacerbation days to nonexacerbation days. In a sensitivity analysis, we repeated the models comparing the odds of an exacerbation day to only the nonexacerbation days preceding the first exacerbation.
The version of the inhaler sensor used in this study did not allow us to differentiate between days when a participant did not use their inhaler and days when the sensor was not charged or was turned off. In 11 participants who returned a daily diary, sensor data were missing 23% of the time during days when participants recorded inhaler use in the diary. Therefore, days with no sensor data were excluded since imputing all missing days as 0 puffs would likely be inaccurate.
Results
Characteristics of study participants
A total of 35 participants enrolled in the study (Fig. 2). One participant died from complications of pneumonia, resulting in 34 participants who completed the study. Mean age was 66 years, with an average of 68 pack-years smoking history. Participants had moderate-to-severe airflow obstruction, with a mean FEV1 of 1.4 ± 0.1 liters among participants with ≥1 exacerbation and 1.8 ± 0.4 among participants not reporting an exacerbation (Table 1).
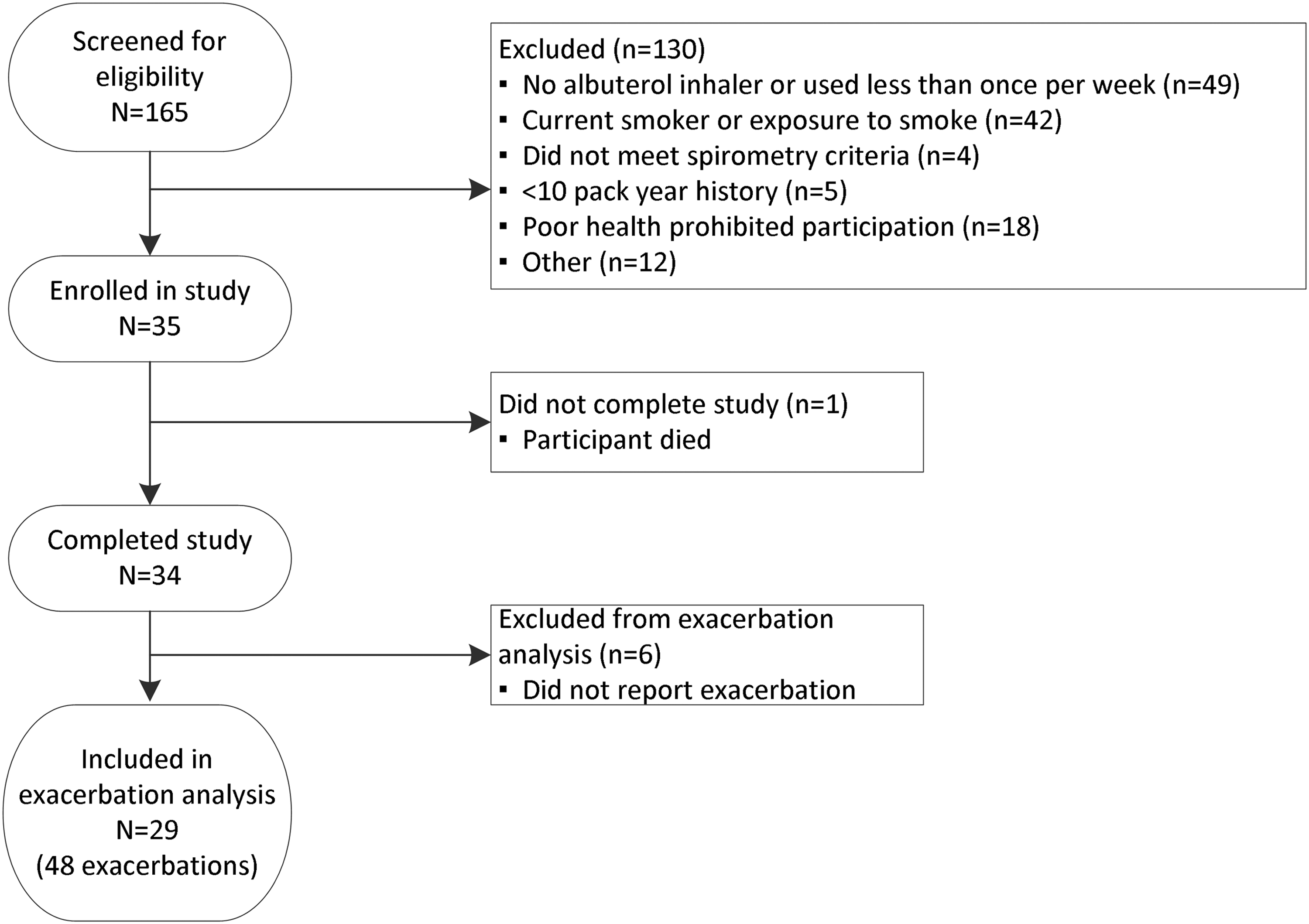
Participant flow diagram.
Participants with MMRC = 4 were excluded from the study.
Participants with FEV1 > 80% were excluded from the study.
The mean albuterol use (puffs) was calculated for each participant, then the median (IQR) of the means of participant albuterol was calculated.
ED, emergency department; IQR, interquartile range; SD, standard deviation; MMRC, Modified Medical Research Council; COPD GOLD, Global Initiative for Chronic Obstructive Lung Disease; FEV1, forced expiratory volume in 1 second; SOBQ, Shortness of Breath Questionnaire.
Characteristics of COPD exacerbations
The median number of days from the baseline period to the first exacerbation was 18 days (interquartile range [IQR]: 7–31). There were 48 exacerbation events observed in 29 participants. The average number of exacerbations reported was 1.4 ± 0.9 events. The median length of an exacerbation was 9.5 days (Table 2). Twelve participants reported a total of 16 moderate-to-severe exacerbations (median duration 14 days [IQR: 8.5–22.5]). The median days of prednisone and/or antibiotic use was 9.5 (IQR: 7–17.5), and the median hospitalization length was 3 days (IQR: 2.5–3.5).
Daily albuterol use measured with the inhaler sensor
The 35 participants had 3199 days of follow-up, and the inhaler sensor recorded at least one puff per day for 69.1% of days. An example of daily albuterol use recorded by the inhaler sensor in one participant is shown in Figure 3 (a participant hospitalized for an exacerbation). The average daily albuterol use for each participant during nonexacerbation days ranged from 1.5 to 17.3 puffs per day. The median of average daily albuterol use during nonexacerbation days was 3.9 (IQR 2.7–6.3), but in 23% of the nonexacerbation days, more than eight puffs a day of albuterol were used.
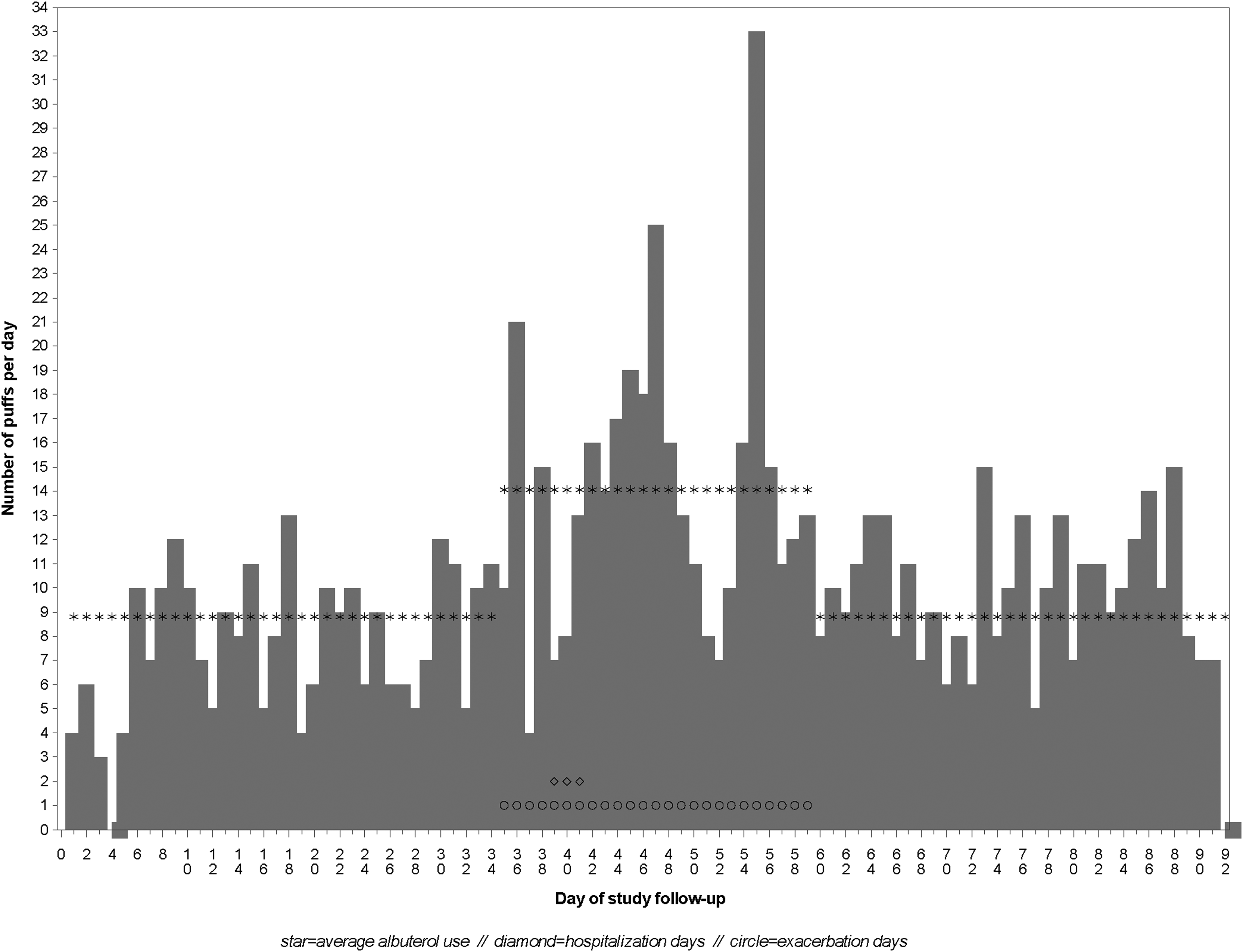
Example of a study participant's daily albuterol use during nonexacerbation days and days of a reported severe chronic obstructive pulmonary disease exacerbation.
Change in albuterol use during exacerbation
There was a median increase in albuterol use of 5.9% (IQR: −12.4% to 27.3%) comparing average mild exacerbation days to average nonexacerbation days (Fig. 4A) and a median increase of 14.1% (IQR: 2.7%–56.9%) comparing average moderate-to-severe exacerbation days to average nonexacerbation days (Fig. 4B).
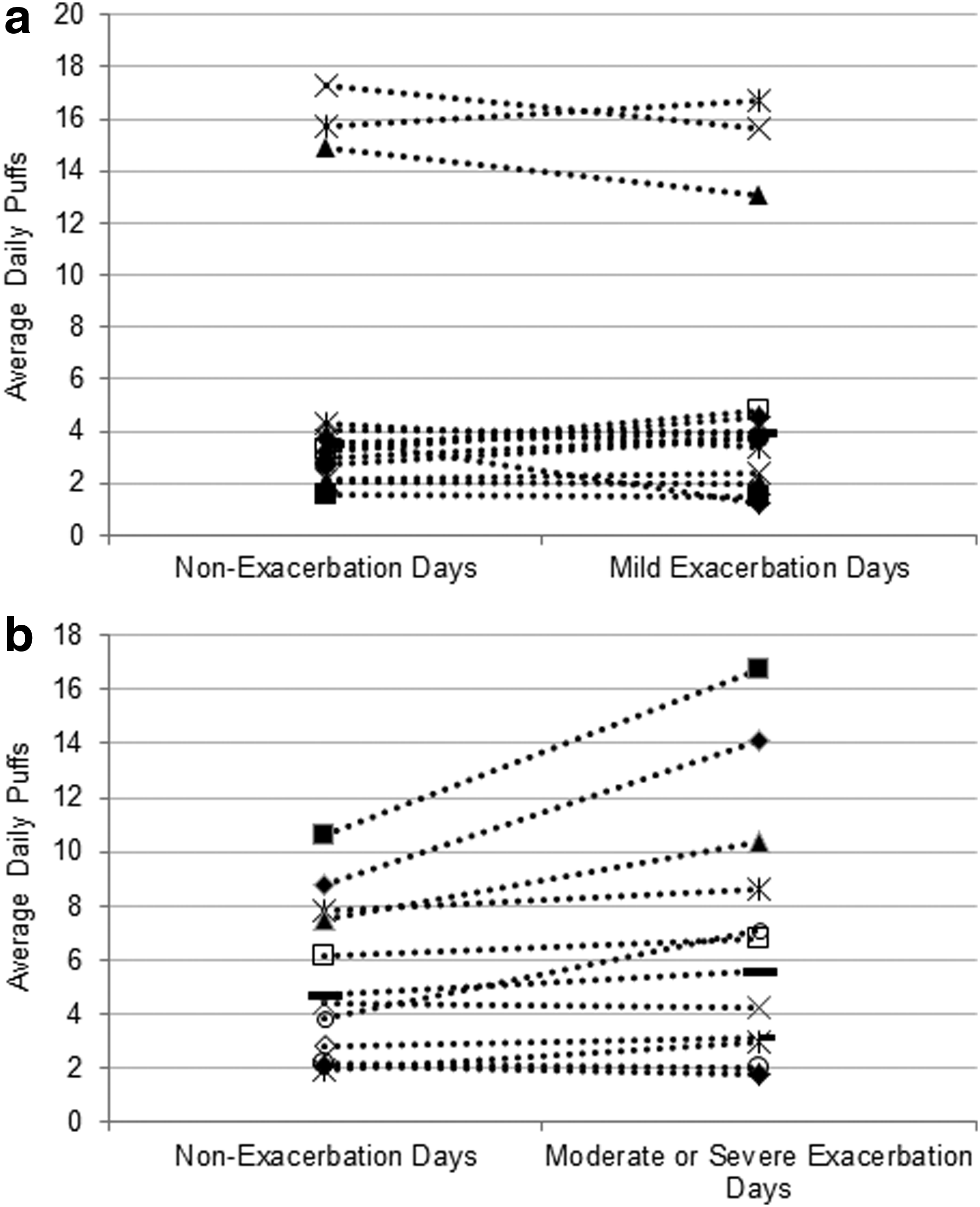
Average puffs during exacerbation and nonexacerbation days among subjects with one or more exacerbation (N = 29).
We next modeled the odds for an exacerbation associated with the increase in number of puffs during any exacerbation day compared to nonexacerbation days in all 48 exacerbation events (mild, moderate, or severe) among 29 participants. For an average participant, a 100% increase in daily albuterol puffs was associated with an odds ratio (OR) of 1.24 (95% CI: 1.11–1.39) for a COPD exacerbation. In other words, for a participant whose albuterol use increased from four to eight puffs per day, the odds of experiencing an exacerbation increased by 24% (95% CI: 11%–39%). Adjusting for FEV1% predicted and inhaled corticosteroid use did not appreciably change the estimate.
We then performed a subgroup analysis by severity of exacerbation comparing: (1) mild exacerbation days (405 days) to nonexacerbation days (1246 days) in 29 participants with mild exacerbations and (2) moderate and severe exacerbation days (222 days) to nonexacerbation days (1246 days) in 28 participants who had moderate-to-severe exacerbations. A 100% increase in inhaler use was associated with an OR of 1.54 (95% CI: 1.21–1.97) in a moderate-to-severe exacerbation adjusted for FEV1% predicted and corticosteroid use (Table 3). We next compared only those baseline days that preceded an exacerbation to all moderate and severe exacerbation days in a sensitivity analysis and observed an increase in odds of an exacerbation with a 100% increase in daily use of albuterol of 1.23 (95% CI: 1.07–1.44).
Model adjusted for FEV1% predicted and concurrent inhaler corticosteroid use.
OR, odds ratio.
Satisfaction with the inhaler sensor
Overall, 74.1% of participants were very satisfied with the inhaler sensor (Table 4). While most participants commented that using the inhaler sensor did not affect their daily routine, some participants noted that using the sensor on the albuterol inhaler may have changed the way they used it. One participant mentioned that he was more likely to question whether he really needed the medication before using it. The sensor gave feedback by blinking lights after actuation and when the battery was low, but several participants expressed a need for more feedback from the inhaler sensor to ensure that it was working correctly.
Results presented only for participants using the new version of the sensor.
Discussion
In this pilot study, we demonstrated that (1) a remote inhaler sensor can monitor albuterol inhaler use in older patients with COPD and is associated with high satisfaction, (2) increased albuterol use captured by the sensor was associated with self-reported episodes of moderate-to-severe exacerbations, yet (3) large variation was seen in the daily use of albuterol in this population even in nonexacerbation days. Prior studies have used this inhaler sensor to monitor inhaler use for asthma patients(3); however, to our knowledge, this is the first study reporting the use of inhaler sensors in COPD patients during exacerbations.
Previous studies have evaluated the use of remote inhaler sensors to assess adherence to controller medications. The SmartTouch™ inhaler sensor improved the adherence to inhaled steroids in adults and adolescents with asthma,(4,13) and more recently, the use of the reminder function of the inhaler sensor was shown to improve adherence and reduce asthma morbidity in children who visited the ED for asthma exacerbations.(5)
Another potential use of remote inhaler sensors is to assess disease control. In asthma, monitoring SABA use is recommended as a measure of asthma control.(14) One small study in which 30 patients with asthma used an inhaler sensor to monitor short-acting bronchodilator use found that weekly feedback to patients of inhaler use was associated with improvement in asthma control.(6) In a pragmatic randomized controlled trial of 495 patients with asthma, use of the Propeller Health sensor to monitor albuterol use was associated with decreased albuterol use overall and improvement in asthma control in the subgroup of adult patients who had uncontrolled asthma at baseline.(7) However, the concept of disease control in COPD is less developed,(15) and SABA use as a measure of disease control in COPD is also not clear.
Since COPD exacerbations are often accompanied by increased SABA use,(8) another potential use of real-time monitoring of SABA inhaler use is early detection of COPD exacerbations by the healthcare team to promptly initiate appropriate therapy. Current telemonitoring approaches for COPD include monitoring of symptoms or pulse oximetry; however, results of telemonitoring in COPD have been equivocal in terms of detection of exacerbations and reducing healthcare utilization.(16)
Inhaler sensors may have advantages over existing telemonitoring methods as they can monitor inhaler use with minimal effort by the patient without interrupting their usual daily activity and, therefore, have potential for higher adherence to the use of the monitoring device. A recent systematic analysis in the effectiveness of telemonitoring in COPD patients in nine studies from 2011 to 2013 demonstrated that telemonitoring may decrease overall healthcare utilization,(17) and although patients were generally satisfied with the devices they used, low adherence to these devices was seen.(18)
In our study, we report the feasibility of using an inhaler sensor to monitor SABA use in COPD patients. Most studies using inhaler sensors focused on patients with asthma, who tend to be younger and may be more comfortable with newer technology. Participants in our study were older with a mean age of 66 years, and many had comorbidities such as coronary artery disease. In this group, we demonstrated that the inhaler sensor was easy to use and that it captured increases in SABA use associated with a moderate-to-severe exacerbation.
However, we also identified a potential challenge unique to COPD patients. Unlike patients with asthma in whom albuterol use is minimal during well-controlled days, in our population albuterol use varied largely even during nonexacerbation days indicating the difficulty in determining the baseline use. In addition, some patients overused their albuterol even in the nonexacerbation days.(19) Therefore, our study suggests that future statistical models are likely needed to account for individual baseline short-acting bronchodilator use to more accurately detect the early development of a COPD exacerbation.
Several limitations are important to note. Our study was a 3-month pilot study to assess the feasibility of inhaler sensor usage in COPD, so the analysis of the association of COPD exacerbation with changes in the number of albuterol puffs was likely underpowered. In addition, we relied on self-report to identify exacerbations, so inaccuracies may exist in recalling the exact start and end dates of the exacerbations, as well as in recalling mild worsening of symptoms. Although we observed COPD exacerbations in 83% of the participants during the 3-month study period, most of these were mild and only 12 (34%) had moderate-to-severe exacerbations.
In addition, the 3-month observation time may not have been sufficient to establish a true baseline value especially given the large fluctuations in rescue inhaler use even during participants' stable state. In addition, inhaler sensor data were available for only 70% of follow-up days for each participant. This is not unusual for an intervention in which patient data are collected every day and consistent with a study of pedometer use in COPD during which patients wore their pedometer 77% of the time.(20) It is possible we underestimated albuterol use if participants increased albuterol nebulizer use at home or received albuterol nebulizers or MDIs in the ED or hospital which may have attenuated the relationship between albuterol use and exacerbations.
For the 30% of time that sensor data were not available, we were not able to determine whether this was due to no inhaler use on a given day or whether the sensor battery was not charged or was turned off. We observed that among the 11 participants in this study who also completed a daily diary, sensor use data were missing an average of 23% of the time during days with corresponding self-reported diary use suggesting that most missing sensor days were due to the sensor either not being charged or not being used with the inhaler. The newest generation of this sensor automatically records whether the sensor is operational, even during days in which it is not used, so it can differentiate whether there is a technical issue with the sensor or the sensor is not used.
We provided smartphones to participants because we assumed that many would not own their own. To ensure that more COPD patients are able to use this type of inhaler monitoring program, alternative ways to transmit data that do not require a smartphone such as transmitting data automatically through Bluetooth connection to a data hub at the patient's home should be considered. These issues indicate that regular follow-up and reminders on how to use the device, as well as availability of technical support, are likely important to successful electronic monitoring of inhaler use.
Conclusion
We found that a remote inhaler sensor was convenient for most of these older participants with COPD over a 3-month period in our pilot study. Increased albuterol use captured by the sensor was associated with self-reported episodes of moderate-to-severe exacerbations, but not in mild untreated exacerbations. Further studies of longer duration are necessary to establish a stable state of inhaler use patterns and to capture multiple episodes of exacerbation to fully evaluate the device's utility in early real-time identification of exacerbations and prompt treatment.
Footnotes
Acknowledgments
Hong T.K. Nguyen and Carol Simons participated in recruitment, data collection, and data management for the study. This research was supported by Pilot Project No. PPO 10-299 from the United States Department of Veterans Affairs Health Services Research and Development (HSR&D) Program. ![]() identifier: NCT0266132.
identifier: NCT0266132.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government. This material is the result of work supported by resources from the VA Puget Sound Health Care System, Seattle, Washington. Propeller Health did not play a role in the financing, design, or conduct of the study.
Author Disclosure Statement
O.H. is a shareholder and former employee in Propeller Health, formerly Reciprocal Labs, which was contracted with by the study to provide the electronic inhaler sensors. Propeller Health did not play a role in the funding, design, or conduct of the study. K.S., E.R.L., S.M., I.G., H.Q.N., R.M.T., V.S.F.: In the past 3 years have no conflict to report.