
Abstract
Abstract
Background:
Appropriate inhaler selection is of fundamental importance in obstructive lung disease management. Key factors in device selection include a patient's capacity to operate a particular device and their preference for it.
Methods:
This randomized, open-label, two-period, crossover study (NCT01739387) compared the ability of adolescent and adult patients with obstructive lung disease to correctly handle the fluticasone propionate/formoterol fumarate (FP/FORM; Flutiform®) pressurized metered-dose inhaler (pMDI) and FP/FORM K-haler®, a novel breath-triggered inhaler (BTI), following a simple, standardized training regimen. The primary endpoint was the ability to perform all steps correctly at the first attempt. Secondary endpoints included the ability to perform all critical steps correctly at the first attempt, the requisite number of attempts to successfully use the inhaler, the ability to be trained within 15 minutes, and the ability to trigger the K-haler BTI to actuate at the first attempt. Ease of device use and device preference versus patients' usual maintenance inhalers were also assessed.
Results and Conclusions:
At the first attempt, an identical proportion (77.2% [95% confidence interval [CI]: 72.1, 81.8]) of 307 patients performed all pMDI and K-haler BTI handling steps correctly, whereas the corresponding proportions performing all critical steps correctly were 82.4% (95% CIs: 77.7, 86.5) and 87.0% (95% CI: 82.7, 90.5), respectively. For both devices, >90% of patients required only two attempts to master device usage; >99% of patients could be trained to correctly use each device within 15 minutes. Virtually all patients (99.0% [95% CIs: 97.2, 99.8]) were able to successfully trigger the K-haler BTI's dose-release mechanism at first attempt. Ease of use and preference data for FP/FORM pMDI challenged the perceived wisdom that dry powder inhalers are necessarily simpler to use, whereas the corresponding data for FP/FORM K-haler strongly favored this novel BTI over the Turbuhaler®, Accuhaler®, and other pMDIs.
Introduction
I
The Flutiform® K-haler® is a novel breath-triggered pMDI (breath-triggered inhaler [BTI]) (Fig. 1). When the hinged cap of the inhaler is opened, the enclosed canister is depressed and it releases a dose of medication into a kinked “K-valve” sitting beneath the canister's metering valve. The “K-valve” holds this dose in situ until inhalation through the mouthpiece causes the kinked valve to straighten and release the medication to the patient. Drug delivery is, thus, breath triggered and avoids the requirement for the patient to coordinate manual canister depression with inhalation, a requisite step in conventional (i.e., non-breath triggered) pMDI handling that may be prone to error.(3,4)

External view of the K-haler BTI. BTI, breath-triggered inhaler.
Should the patient prime the inhaler by opening the hinged cap but fail to inhale, the drug dose in the K-valve is automatically expelled from the device when the hinged cap is closed, preventing any inadvertent “double-dosing.” During everyday use, the expulsion of an unused dose on cap closure also provides feedback to the patient that the device was not successfully triggered.
An additional feature of the K-haler BTI is its low resistance allied to a low “trigger” flow rate of ∼30 L/min. This implies that virtually all patients should be able to generate the requisite inspiratory effort through the device to cause it to actuate, including those patient subgroups that may fail to produce the requisite airflows through higher resistance DPIs to generate respirable particles.(5–7)
Flutiform is a combination of fluticasone propionate and formoterol fumarate (FP/FORM) in a (conventional) hydrofluoroalkane (HFA) pMDI that is currently approved to treat asthma in adults and adolescents. A series of studies have demonstrated improvements in lung function, symptoms, and health status with FP/FORM pMDI across a spectrum of asthma severities(8–15); whilst two long-term studies have confirmed its safety in association with a very low incidence (∼2%–3%) of severe asthma exacerbations in patients treated for a maximum of 14 months.(16)
This study was undertaken as part of a development program for the existing FP/FORM formulation in the new K-haler BTI device. Although two other BTIs, namely the Easi-Breathe® and Autohaler® devices, are commercially available, no breath-triggered devices containing inhaled corticosteroid/long-acting β2-agonist (ICS/LABA) combinations are currently approved despite the extremely widespread use of this combination class for ∼15 years.
Materials and Methods
The study (NCT01739387), performed at two sites in the United Kingdom, was of randomized, open-label, two-period, crossover design and compared the ability of patients to correctly handle two inhaler devices: FP/FORM pMDI and FP/FORM K-haler BTI.
Male or female patients aged 12 years or older, with asthma and/or COPD for at least 6 months, currently using an ICS and LABA either via a single or separate inhalers, and able to perform spirometry were eligible for enrollment. Patients with other chronic respiratory diseases, with unstable disease that was liable to jeopardize the patient's health or to confound between-period comparisons, and with serious neuromuscular disorders or orofacial diseases preventing the application of an inhaler to the mouth were excluded from the study.
All patients and/or their legal guardians/legally authorized representatives were provided with oral and written information describing the nature and duration of the study, its purpose, the procedures to be performed, potential risks and benefits involved, and any potential discomfort. Each patient was given a copy of the patient information sheet, and an informed consent form that they were asked to sign before any study-specific procedures were performed. The study was conducted in adherence to Good Clinical Practice (GCP Directive 2005/28/EC, CPMP/ICH/135/95; EU Clinical Trials Directive 2001/20/EC) and in accordance with the Declaration of Helsinki Recommendations and all of its Amendments to date.
At screening, current inhalers and prior training on these devices, asthma and/or COPD history, smoking history, and educational level were recorded, and spirometry was performed. Eligible patients were randomized to one of two device sequences (K-haler BTI/pMDI or pMDI/K-haler BTI) by using a validated randomization system. The characteristics of those enrolled were reviewed on an ongoing basis during the study to ensure that subsequent patient screening was adjusted to achieve approximate target subgroup sizes in terms of age groups (≥12–17 years [20%]; 18–65 years [50%]; ≥65 years [30%]) and% predicted forced expiratory volume in the first second (FEV1) categories (<60%; ≥60% to <80%; ≥80% [approximately a third in each subgroup]). When the enrollment target in a particular subgroup was met, further enrollment into that subgroup could be stopped.
Patients attended two single-day study visits, separated by a 7- to 21-day washout period. The washout period, during which the patient used his/her current inhaler medication, was included to minimize the potential for confusion between devices and, hence, sequence effects.
At each study visit, trained site staff taught patients to correctly handle the applicable device (either pMDI or K-haler BTI). Placebo devices containing only the formulation excipients (including the propellant) but not the active substances were employed. Eight steps determining correct inhaler usage, and based on the available literature wherever possible, were pre-defined for each device, with four and five of the eight steps defined as being “critical” for the pMDI and K-haler BTI, respectively (Table 1).
Steps denoted as critical for each device.
BTI, breath-triggered inhaler; pMDI, pressurized metered-dose inhaler.
Patient training comprised an initial step-by-step explanation of device handling by the trainer, followed by a demonstration by the trainer of a complete handling maneuver (without narration). Patients then attempted a first “practice” use of the device, which was critiqued by the trainer but not appraised as part of any handling outcomes. Thereafter, the patient used the device a second time with this attempt formally assessed as correct/incorrect by using the criteria defined in Table 1. Successful device usage was defined as all eight steps being correctly performed. If any individual steps were incorrect, the patient received additional feedback on their technique, after which the patient was asked to again demonstrate inhaler usage with this attempt again formally assessed. A maximum of 15 minutes or eight handling attempts (not including the first “practice” use), whichever occurred first, were allowed for training and assessment.
Patients were asked to rate the handling of each study inhaler in comparison to their current inhaler as follows: much easier, a little easier, about the same/don't know, a little harder, much harder. They were also asked whether they preferred the study inhaler, their current maintenance inhaler, or had no preference/did not know.
Finally, each patient's ability to successfully trigger the K-haler BTI to fire was evaluated. This was determined when the patient closed the K-haler BTI by noting whether an audible and visible aerosol plume was emitted, as occurs if the device has not been triggered during inhalation, which serves as a feedback alert of unsuccessful use.
The primary endpoint was the ability to perform all steps correctly at the first attempt post-training. Secondary endpoints included the ability to perform all critical steps correctly at the first attempt post-training, the ability to perform each individual step correctly at the first attempt post-training, the number of attempts to successfully use the inhaler, the ability to be successfully trained within 15 minutes, and the ability to trigger the K-haler BTI to actuate at the first attempt. In addition, the ease of use of, and preference for, the study inhaler in comparison to the patient's current maintenance inhaler were assessed.
Sample size and statistical analysis
Sample size was based on a desired level of precision (±5%) around the percentage of patients able to perform all handling steps correctly at the first attempt post-training (the primary endpoint). Assuming that 75% of patients could perform all steps correctly, a sample size of 289 participants was sufficient to calculate a two-sided 95% confidence interval (CI) with a precision level of 5% either side of the proportion. The sample size was calculated by using NQuery (version 7.0) to generate a CI for a proportion using normal approximation. Assuming that 15% of randomized patients would be excluded from the per protocol population (PPP), a total of 340 randomized patients was required, 170 per treatment sequence.
Statistical analysis was restricted to descriptive statistics only, that is, inferential analyses were not performed as no formal hypothesis was evaluated. The number and percentage of patients able to perform all steps correctly at the first attempt (primary endpoint), able to perform all critical steps correctly at the first attempt, be successfully trained within 15 minutes, and able to trigger the K-haler BTI at the first attempt were calculated with associated two-tailed 95% CIs. The number of attempts that patients required to successfully use the inhalers was also summarized. For the aforementioned analyses, subgroup analyses by % predicted FEV1 and age categories were also performed.
In addition, the percentage of patients performing each individual handling step correctly at the first attempt post-training, and the ease of use and preference data were also summarized. Post hoc analyses of the ease of use and preference endpoints were performed based on subgroups of patients using specific maintenance inhalers (Symbicort® Turbuhaler®, Seretide® [Advair®] Evohaler® [i.e., pMDI], Seretide® Accuhaler® [Diskus®], and Fostair® pMDI). The post hoc analyses provided clearer insights into the data, given the distinct operational characteristics of the different maintenance inhalers, than the pre-specified analyses that grouped all “current maintenance” inhaler types together.
All handling analyses were conducted on the full analysis population (FAP: randomized patients who used either device and had at least one handling assessment) and PPP (FAP patients who completed both study periods and had no other major protocol deviations). The PPP was considered the primary analysis population for the handling analyses.
Results
A total of 589 patients were screened, of whom 311 were randomized with 307 (98.7%) patients completing both study periods and 4 (1.3%) discontinuing prematurely (Fig. 2). There were no other major protocol deviations. The FAP and safety populations, therefore, consisted of 311 patients and the PPP consisted of 307 patients.
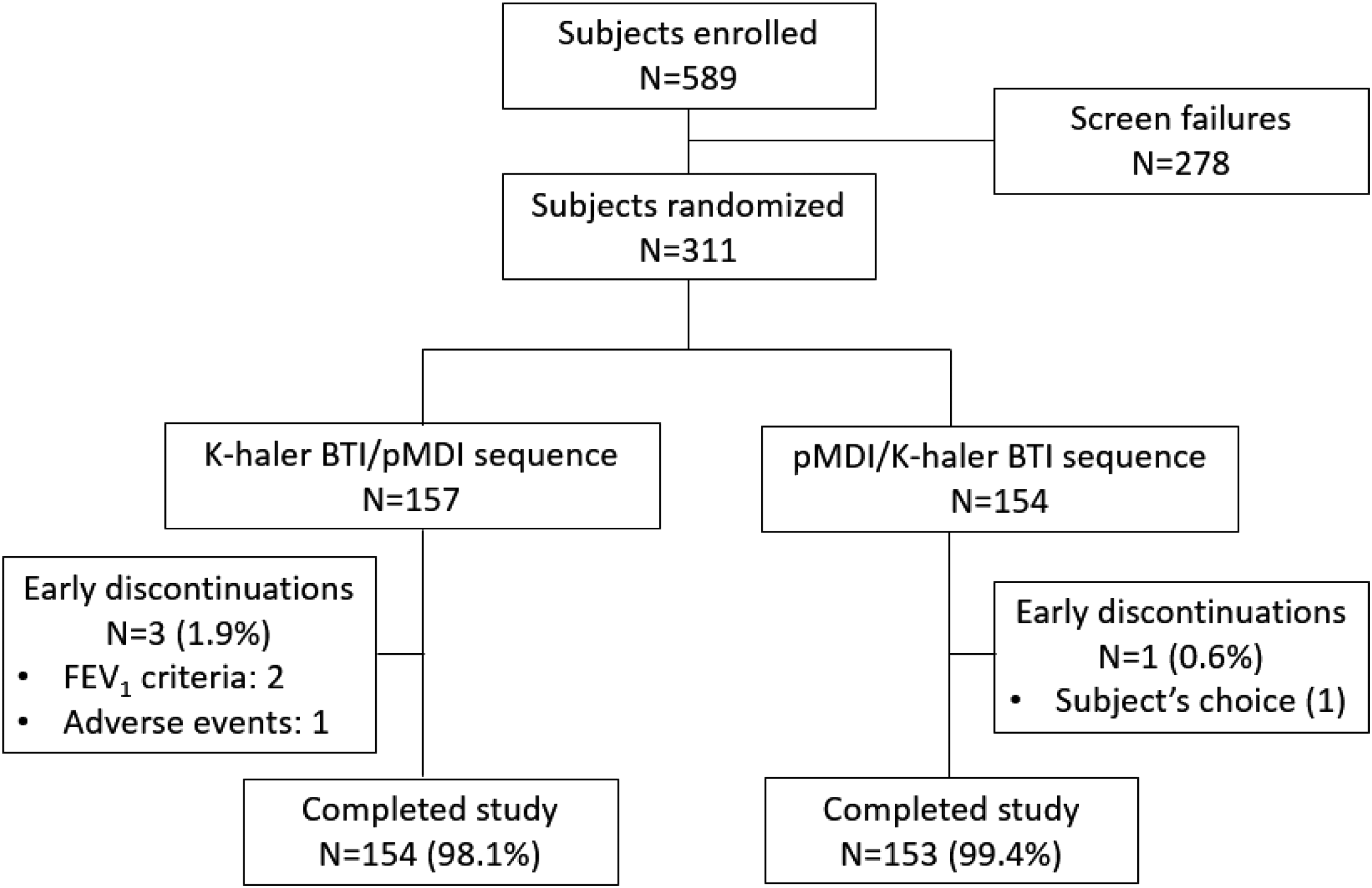
Patient disposition.
Demographic and disease characteristics at baseline are summarized in Table 2. Approximately half of the patients were currently using pMDIs (45.8%) and half DPIs (55.2%) as their maintenance inhaler at study entry, with only one patient using a BTI (Autohaler) for maintenance therapy. Seventy-four percent of patients were using a pMDI to administer reliever therapy and 40% were using a DPI, with 10% using a BTI (Autohaler or Easi-Breathe) in this context. No patients were currently using the K-haler BTI as it was not commercially available at the time that the study was undertaken.
Only includes lung function data from acceptable spirometry sessions per American Thoracic Society/European Respiratory Society (ATS/ERS) criteria. However, FEV1 subgroups in handling analyses defined based on all available spirometry data. Hence, “n” numbers here and in Table 3 FEV1 subgroup analyses differ.
n, number of patients with data available. Percentages based on n.
SD, standard deviation; FEV1, forced expiratory volume in the first second; COPD, chronic obstructive pulmonary disease.
Device handling
An identical proportion (77.2% [95% CI: 72.1, 81.8]) of patients were able to perform all handling steps correctly at the first attempt post-training (the primary endpoint) for both devices. All critical steps for the K-haler BTI and pMDI were performed correctly at the first attempt by 87.0% (95% CI: 82.7, 90.5) and 82.4% (95% CIs: 77.7, 86.5) of patients, respectively. Almost all patients (99.7% [95% CI: 98.2, 100.0] for the K-haler device; 99.3% [97.7, 99.9] for pMDI), irrespective of age or FEV1 subgroup category, were able to correctly perform all device handling steps within 15 minutes, with only 7% (K-haler) and 9% (pMDI) of patients requiring more than two attempts to master device handling.
The performance of individual handling steps at the first attempt post-training is summarized in Figure 3: For the K-haler BTI, all individual steps were correctly performed by at least 90% of patients; for the pMDI, the most frequent mistakes, although in a small minority of patients, were failure to coordinate inhalation and canister depression (step 5; in 8% of patients) and inhale for at least 3 seconds (step 6; 12%).

Percentage of patients performing each device step correctly at the first attempt.
Patient handling by FEV1 and age subgroups is presented in Table 3. The decreasing lung function and increasing age subgroups approximately corresponded to one another. Numerically fewer elderly patients handled both devices without any errors compared with their younger counterparts at first attempt; however, following additional training for those who needed it, all age subgroups performed similarly. Broadly speaking, comparative handling of the two devices, the K-haler BTI and pMDI, was similar within each subgroup: In any given subpopulation, the percentages of patients performing all pMDI or K-haler steps correctly, or all critical steps correctly, were within 10% of one another.
% predicted FEV1 subgroups in handling analyses defined based on all available spirometry data. Hence, “n” numbers here and in Table 2 baseline characteristics summary differ.
N, number of patients in population; n, number of patients with data available. Percentages based on n.
BTI, breath-triggered inhaler; pMDI, pressurized metered-dose inhaler; FEV1, forced expiratory volume in the first second.
Finally, virtually all patients (99.0% [95% CIs: 97.2, 99.8]) were able to trigger the K-haler BTI's dose-release mechanism at their first attempt. The three patients (of 307) who failed to do so were equally distributed across the % predicted FEV1 categories. As inspiratory and expiratory flows are related,(5,17) this implies a failure of technique in these three individuals, rather than an inherent inability to generate the requisite inspiratory flow rate in association with severe airway obstruction.
Ease of use and preference
A total of 288 patients (94% of the total population) used Symbicort Turbuhaler (n = 126), Seretide Evohaler pMDI (n = 118), Seretide Accuhaler (n = 35), or Fostair pMDI (n = 9) as their existing maintenance ICS/LABA inhaler. Results for the ease of use and preference analyses (comparing the study inhaler versus the current maintenance inhaler) in each of these subgroups are summarized in Figures 4 and 5.
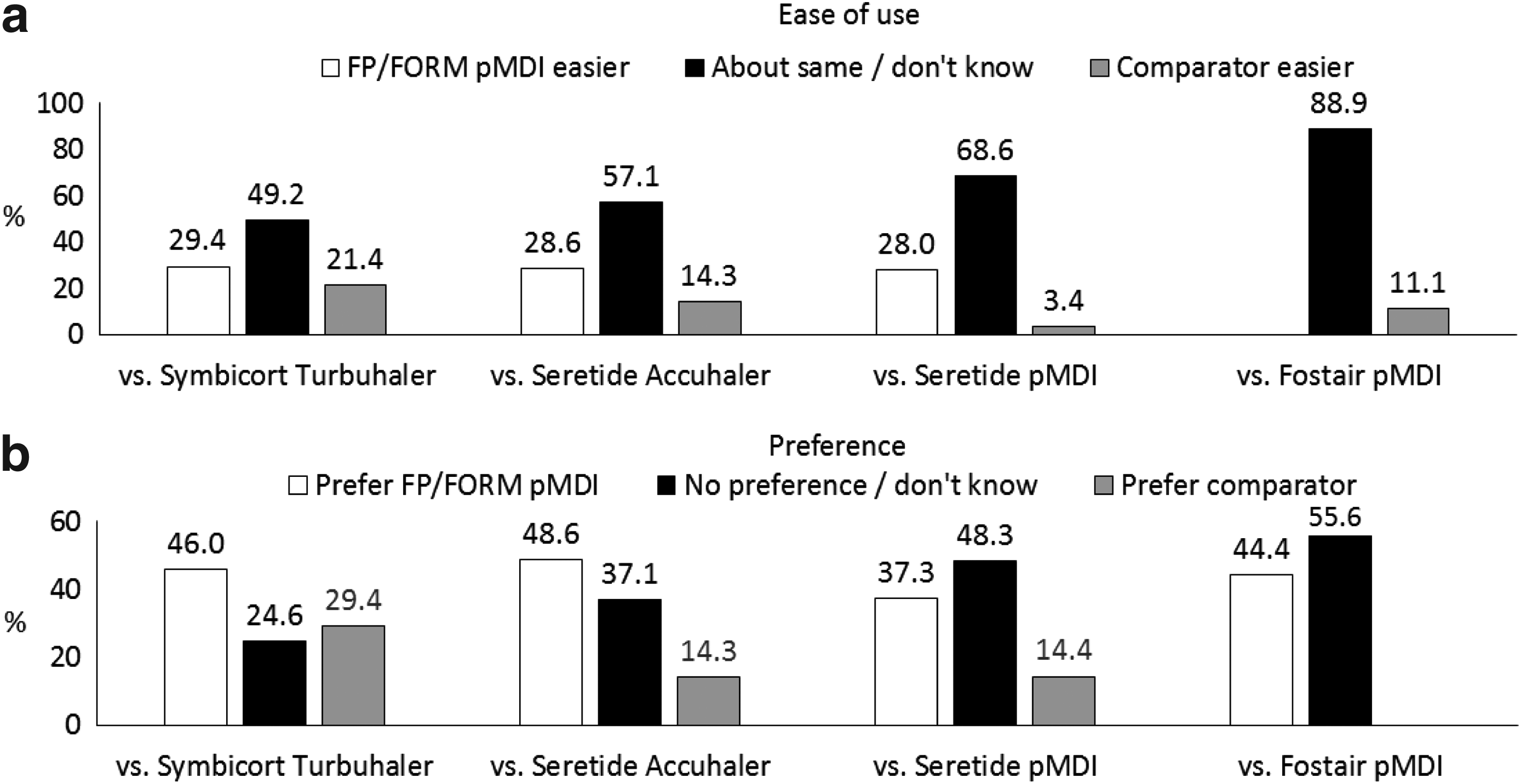

Many patients did not note differences in the ease of use of FP/FORM pMDI versus their existing inhalers (Fig. 4). Interestingly, however, among those who did note a difference, a numerically greater proportion found the pMDI easier to use than either the Turbuhaler or Accuhaler DPIs. Somewhat surprisingly, of the patients who reported differences between FP/FORM pMDI and Seretide Evohaler pMDI, the great majority found the FP/FORM device easier to use. Preference data for FP/FORM pMDI were also unexpected (Fig. 4): ∼40%–50% of patients preferred the FP/FORM pMDI versus their usual maintenance inhaler and in all cases, these patients considerably outnumbered those favoring their existing inhaler device.
With respect to FP/FORM K-haler BTI, ∼45%–60% of patients found this device easier to handle than their existing maintenance devices (Fig. 5). By comparison, 21% of patients currently using the Turbuhaler device reported their existing device being easier to handle, whereas the corresponding proportions for Evohaler pMDI-, Fostair pMDI-, and Accuhaler-using patients were 17%, 11%, and 11%, respectively. The preference data were even more strongly in favor of the K-haler BTI, with around 60%–70% of patients preferring the K-haler BTI to their usual inhaler (Fig. 5).
Discussion
In this first published study reporting patient handling of the K-haler BTI, enrollment criteria were deliberately unrestrictive. Only patients whose inclusion would have been unethical or medically inappropriate were excluded, to allow extrapolation of the data to the intended patient population. To further ensure that the study results were generalizable, patient enrollment was monitored and adjusted during the study to facilitate the inclusion of a reasonably large number of patients in all lung function and age subgroups. Evaluation of elderly subjects is particularly important since multiple studies have demonstrated poorer device handling in this age group,(18–20) which may be related to cognitive and psychiatric deficits.(18) Furthermore, evaluation of patients with severe airway obstruction is pertinent to all BTIs and DPIs as such individuals may be unable to generate an optimal inspiratory flow against the inherent resistance of some inhaler devices.(17,21)
Training was designed to be feasible within a general practice setting, the most relevant context for the large majority of patients with obstructive lung disease. Thus, a maximum of 15 minutes was allowed for training while assessment was performed via direct observation only without the use of subsequent video review or the use of an inhalation profile monitor. To aid the recall of three steps that are subject to frequent errors [including for DPIs(22,23)], patients were instructed to exhale for at least two seconds (step 3; approximating to [at least] functional residual capacity), inhale for at least three seconds (step 6; corresponding to ∼90 L/min or less),(24) and breath-hold for at least four seconds (step 8; to facilitate optimal deposition and, hence, pharmacodynamic effect).(25,26)
Note that the instruction regarding inhalation duration (and, thus, target flow rate) was based on an earlier study of a breath-triggered chlorofluorocarbon (CFC) pMDI, whereby a 3-second inhalation (corresponding to a target inspiratory flow rate of 90 L/min) led to optimal lung deposition.(24) Interestingly, however, the flow rate dependence for drug deposition that is well described for CFC pMDIs(27–29) may be less applicable to FP/FORM HFA: Thus far, in vitro data have revealed that FP/FORM HFA has a consistent fine particle fraction of ∼40% at flow rates of 30–60 L/min,(30) whereas functional respiratory imaging data have demonstrated consistent total lung deposition of 36%–44% with either a sharp or gradual inspiratory profile and an inspiratory flow rate of 30 or 60 L/min.(31) These data imply that FP/FORM HFA may be more forgiving of variance in inspiratory flow rate than the earlier generation of CFC pMDIs.
The data from this “real-world” study revealed very similar handling results for both devices: Almost all patients were able to correctly use both the K-haler BTI and pMDI within 15 minutes, and more than 90% of patients required only one or two attempts to master device usage. Nonetheless, it is plausible that this study may have underestimated differences between the pMDI and K-haler BTI through not using an inhalation profile recorder. Instead, visual observation was used to determine the temporal relationship between inhalation and canister actuation for the pMDI.
An earlier study by Chapman et al. that compared another BTI and pMDI in elderly subjects supports this view: Differences in successful device handling between these devices were magnified when using objective recordings of inhalation and canister actuation compared with visual observation alone.(20) Chapman et al.'s20 study is consistent with the intuitive notion that a breath-triggered device should improve handling performance compared with a pMDI in patients with poorer coordination.(32)
The positive handling results for the K-haler BTI from this study are perhaps unsurprising, as prototypes of this novel device have been through rounds of iterative design modifications based on user feedback. Further, after shaking the K-haler BTI, in simplistic terms, patients “open, inhale and close.” Thus, the device is conceptually similar to recently launched DPIs that have been well received by patients.(33,34)
Results for the pMDI may, however, be more unexpected since perceived wisdom is that pMDIs are difficult to use.(35) Despite such views, there is no evidence to indicate that improved clinical outcomes are obtained with DPIs compared with pMDIs.(36,37) By contrast, Price et al. reported significantly greater odds of achieving asthma control and treatment success, and a trend toward a lower exacerbation rate, with Seretide pMDI than Seretide Accuhaler.(38) In a further real-world study, Müller et al. noted better asthma control and symptoms and lesser rescue use with a beclomethasone/formoterol pMDI formulation compared with two fixed combination DPIs.(39)
Further, in two recent long-term studies, a very low incidence of severe exacerbations was observed in patients treated with FP/FORM pMDI,(16) lower than in the large majority of previous ICS/LABA studies, including those evaluating Seretide Accuhaler and Symbicort Turbuhaler.(40) Thus, although a number of studies have reported more device errors with pMDIs than certain DPIs,(41,42) the various data indicated earlier suggest that the prevalence of truly meaningful errors that reduce pulmonary drug delivery below a critical threshold is no greater with pMDIs than with DPIs.
Furthermore, the success of a simple, structured instruction in this study and longer-term success rates in centers that are highly focused on the inhaler technique(41) suggest that the poor technique reported with pMDIs in some, particularly observational, studies(43,44) may reflect a lack of knowledge of pMDI technique among healthcare professionals themselves. As these practitioners are, in turn, responsible for training patients, the reported extent of such deficiencies has, in some cases, been alarming.(45–47) In this suboptimal albeit real-world context, the availability of an ICS/LABA combination BTI to obviate the need for actuation-inhalation coordination may be beneficial.
The observation that virtually all patients in this study could be rapidly trained to use both devices has important implications: Multiple studies have demonstrated that poor device technique is associated with reduced pulmonary drug delivery,(48–50) inadequate asthma control,(51–53) and the increased requirement for oral corticosteroid bursts,(4,52) emergency room attendance,(52) and hospitalization.(52) Thus, the ability of a broad spectrum of “real-world” patients to correctly handle the FP/FORM K-haler BTI and pMDI is clinically meaningful. Second, even in the absence of a formal health economic evaluation, the substantial excess healthcare costs associated with uncontrolled asthma(54–56) clearly suggest the cost-effectiveness of the low-cost, low-tech training intervention employed that is well suited to community practice.
The ease of use and preference data in the present study were also of interest. Somewhat unexpectedly, ∼50%–60% of patients using marketed DPIs found their existing devices no easier to use than FP/FORM pMDI, whereas approximately a quarter of patients actually found the FP/FORM pMDI easier to handle. Further, approximately half the patients preferred the FP/FORM pMDI to the Accuhaler and Turbuhaler devices. Although it is possible that these data were influenced by training on the FP/FORM pMDI but not on patients' current inhalers during the study, they, nonetheless, intimate that the generalized view that DPIs are easier to use may be unfounded.
The results comparing FP/FORM pMDI with Seretide Evohaler pMDI were also surprising: Among those expressing a preference, a clear inclination in favor of FP/FORM was observed. Again, it is possible that this is an artefact of study design, although the gentler, warmer, slower, and longer lasting aerosol plume from FP/FORM pMDI versus Seretide Evohaler pMDI(57) may be implicated, suggesting that subtle differences between pMDIs may have important impacts on patient perception.
For the K-haler BTI, ease of use and preference data strongly favored this novel device over usual maintenance inhalers, with ∼60%–70% of patients finding it preferable to each of the Turbuhaler, Accuhaler, and Seretide and Fostair pMDIs. These are encouraging data since the importance of patient engagement with inhaler selection is widely accepted,(58) with ease of use and preference being associated with improved adherence to treatment.(59–61) Although greater inhaler adherence has unsurprisingly been associated with improved clinical outcomes,(4,51–53) a direct link between patient device satisfaction and clinical outcomes has been more difficult to establish: Small et al. reported improved health status, fewer exacerbations, and fewer primary and secondary care visits with improved device satisfaction in the large majority of patients,(59) but most other studies have not produced similar results.(61,62)
The difficulty in establishing a relationship between device satisfaction and clinical outcomes may stem from the multiple factors that influence patient satisfaction. These include patient expectations (which may be altered by the treating physician), disease and treatment history, and the specific drug-device combination.(62) In addition, negative outcomes unrelated to the device per se, such as side effects, may temper a patient's enthusiasm for a product even where the device itself has very favorable characteristics and where an effective drug has beneficial effects on important outcomes such as exacerbation risk and healthcare utilization.
A final observation of note from this study is that virtually all patients (304 of 307) were able to inhale through the K-haler BTI and trigger it to fire. By design, the study population included a substantial proportion of elderly patients (with 75 patients aged older than 65 years) and with severe airway obstruction (87 patients had <60% predicted FEV1). These results, therefore, indicate the suitability of the K-haler BTI for use in a broad spectrum of patients with obstructive lung disease, including those most likely to generate low inspiratory flow rates.
In conclusion, this study demonstrated that almost all patients from a representative population with obstructive lung disease could be rapidly trained to use the FP/FORM pMDI and K-haler BTI. Similar handling outcomes were obtained for both devices by using a simple instruction method applicable to general practice. Preference and ease-of-use data for FP/FORM pMDI challenged the notion that DPIs are necessarily easier to use, whilst the corresponding data for the K-haler BTI indicated a very favorable perception of this device among patients. Almost all patients were able to trigger the K-haler BTI to actuate.
Footnotes
Acknowledgments
This study was sponsored by Mundipharma Research Limited. Writing assistance to prepare this article was provided by MD Medical Communications. Mundipharma Research Limited provided financial support for the preparation of this article, including all article processing charges. All named authors meet the ICMJE criteria for authorship, have been involved in the analysis and interpretation of the data, the writing and review of this article, and the decision to submit this article for publication, and have given final approval of the version to be published.
Trade Mark Statements
® Flutiform is a registered trade mark of Jagotec AG. K-haler is a registered trade mark of Clinical Designs Limited. Seretide, Advair, Evohaler, Accuhaler, and Diskus are registered trade marks of Glaxo Group Limited. Symbicort and Turbuhaler are registered trade marks of AstraZeneca AB. Autohaler is a registered trade mark of 3 M Company. Easi-Breathe is a registered trade mark of Norton Healthcare Limited. Fostair is a registered trade mark of Chiesi Farmaceutici S.p.A.
Author Disclosure Statement
Dr. D.B. was principal investigator at BioKinetic Europe Limited, one of the two sites at which the study was conducted. Dr. L.M. and Mr. M.L. are employees of Mundipharma Research Limited. There are no other conflicts of interests related to this publication.