
Abstract
Abstract
Background:
Despite the prevailing assumption of “smooth trachea walls” in respiratory fluid dynamics research, recent investigations have demonstrated that cartilaginous rings in the trachea and main bronchi have a significant effect on the flow behavior and in particle deposition. However, there is not enough detailed information about the underlying physics of the interaction between the cartilage rings and the flow.
Materials and Methods:
This study presents an experimental observation of a simplified Weibel-based model of the human trachea and bronchi with cartilaginous rings. A transparent model and refractive index-matching methods were used to observe the flow, particularly near the wall. The flow was seeded with tracers to perform particle image velocimetry and particle tracking velocimetry to quantify the effect the rings have on the flow near the trachea and bronchi walls. The experiments were carried out with a flow rate comparable with a resting state (trachea-based Reynolds number of Re D = 2650).
Results:
The results present a previously unknown phenomenon in the cavities between the cartilaginous rings: a small recirculation is observed in the upstream side of the cavities throughout the trachea. This recirculation is due to the adverse pressure gradient created by the expansion, which traps particles within the ring cavity, thus affecting the treatment of patients suffering from lung disease and other respiratory conditions.
Conclusions:
The detection of recirculation zones in the cartilage ring cavities sheds light on the particle deposition mechanism and helps explain results from previous studies that have observed an enhancement of particle deposition in models with cartilage rings. These results bring to light the importance of including cartilage rings in experimental, numerical, and theoretical models to better understand particle deposition in the trachea and bronchi. In addition, the results provide scientists and medical staff with new insights for improving drug delivery.
Introduction
T
The goal of this study is to present evidence of a previously unknown phenomenon that occurs in the extrathoracic portion of the respiratory tract. The flow within a tracheobronchial model with cartilaginous rings is measured using particle tracking velocimetry (PTV) and refractive index matching. The inclusion of cartilage rings changes the dynamics of the flow near the wall, generating recirculation regions in the cavities between rings. This is the first time such phenomenon has been documented in the medical literature or in respiratory fluid dynamic community.
Owing to the complexity of the respiratory tract, assumptions are usually made when studying the flow or developing mathematical models. A common simplification is to consider the trachea and bronchi walls as smooth surfaces. This simplification has been used to study both the flow characteristics(4–9) and particle deposition.(10–13) However, upper airways are lined by a series of cartilaginous rings(3) that protrude into the respiratory ducts and produce significant differences compared with a smooth wall.(14) More recently, realistic models based on CT scans have been studied.(15–19) Nevertheless, models based on CT scan are specific for each patient, and shape may vary substantially per individual, making it difficult to apply the results to the general population.
Only a few studies have incorporated cartilaginous rings in their models.(18,20–22) Russo et al.(20) and Zhang and Finlay(22) focused on the effect of the cartilaginous rings on the particle deposition. Zhang and Finlay(22) performed an experimental study and found that the presence of cartilaginous rings significantly increases particle deposition. However, their results only included rings in the first generation of their model—that is, the trachea—and flow was not measured in the study, only particle deposition. The results also indicated that the particle deposition is only affected in the zone where the rings are present, not propagating into lower generations.
In their numerical study, Russo et al.(20) also found an increase in particle deposition, both in the trachea and in the bronchi, in models where rings were included. However, they did not provide measurements of the flow inside the cavities. Furthermore, they attributed the particle deposition to impaction and sedimentation, without reporting recirculation areas in the cavities between rings. A comparison between the smooth model and the model with cartilaginous rings showed that the effect of the rings increased with increasing particle size and flow rate.
A computational fluid dynamics (CFD) study by Srivastav et al.(21) investigated the effect of cartilaginous rings on a tracheobronchial model based on a CT scan versus a simplified model. They found significant effects on the airflow pattern, showing a higher shear over the cartilaginous rings and differences in the particle deposition between models. Higher velocities were found because of the reduction of the cross section due to the rings. Owing to inertial impaction, they suggest that particles may be deposited on the cartilaginous rings.(21) However, analysis of the flow over a cartilaginous ring was only made on the top of the trachea and the comparison was difficult due to considerable geometric differences between the smooth and ringed models.
Another CFD study, based on a CT scan model, was performed by Luo and Liu.(18) Their simulations detected fluctuations in the flow near the wall induced by the cartilaginous rings. However, the flow disturbance was reported as “not strong enough to cause a boundary layer separation.” Nonetheless, from their figures, the rings appear to have a shallow depth. Unfortunately, the authors did not provide the actual depth value. This shallow appearance could be due to the resolution of the CT scan (0.7 mm); the typical ring depth found by Russo et al.(20) was of 0.25 mm. In addition, the numerical model used in this study has known issues with pressure differences and the capture of viscous effects at lower Reynolds numbers.(23,24)
Similar resolution issues may be present in other studies that used CT scans to fabricate the model. Thus, flow characteristics near the wall in CT scan-based studies should be taken with caution.
In a previous study, it was demonstrated that the cartilaginous rings considerably affect the flow in the upper respiratory tract, that is, trachea and main bronchi.(14) Major differences were found in the bifurcation area, where larger recirculation zones were identified on the top side of the main bronchi for the model with cartilaginous rings. This effect will mostly affect the lower bronchi branches on the respiratory system. In past studies, where rings were included in the model, detailed analysis of the flow near the wall has not been carried out. Thus, this study focuses on the observation of the flow in the cavities between the rings using a high-resolution imaging setup.
Consequently, the objective of this study is to understand the flow behavior near the wall in the respiratory tract. More specifically, we seek to shed light on the flow physics in the cavity created by the rings, and help understand the particle deposition enhancement found by Russo et al.(20) and Zhang and Finlay(22) on the models with cartilaginous rings. Theoretical considerations for the experiment and experimental setup are presented in Materials and Methods section. Results are provided in Results section and discussed in Discussion section.
Materials and Methods
Two tracheobronchial models were created to study the effects of the rings on the flow within the extrathoracic portion of the airway, one with smooth walls and the other with cartilaginous rings. The models have a circular cross section in the trachea and main bronchi. The models' geometry is based on the study by Weibel.(25) The typical diameter of the human trachea and bronchi is 18 mm and 12.2 mm, respectively.(26) The model dimensions are scaled up by 67% to have a better resolution on the measurements, making the trachea 30 mm diameter and 20.1 mm diameter for the bronchi.
In the “ringed” model, rings are 0.424 mm thick and 4.58 mm wide; the distance between rings is 5.76 mm.(14) These geometrical characteristics are also scaled up based on measurements by Russo et al.,(20) who measured the rings directly from human tracheas. A schematic of the “ringed” trachea model is presented in Figure 1. Grotberg(27) reports intrabronchial angles ranging from 64° to 100°. The model has a right bronchial angle of 25° and a left bronchial angle of 45°, resulting in an intrabronchial angle of 70°.

The Reynolds number (Re) is used as a scaling nondimensional parameter for the present experiment. The Reynolds number is the ratio of inertial forces and viscous forces. For flow in a pipe, Re is defined as
where D is the tube diameter, U the mean flow velocity, and ν the kinematic viscosity. It is important to clarify that by matching the Reynolds number, dynamic similarity is ensured between the flow in an actual human trachea and in the present model. This dynamic similarity is maintained even when using liquid as a working fluid instead of air. The working fluid used is a mixture of water, glycerin, and salt (47.9%, 37.1%, and 15% by mass, respectively). The flow rate is approximated to a resting breathing state, with a Reynolds number Re = 2650.(28) The kinematic viscosity of the working fluid is ν = 5.77 × 10−6 m2/s, a diameter of 30 mm, and a bulk velocity of U = 0.51 m/s (flow rate Q = 21.6 L/min) and a density of 1080 kg/m3.
The model was created from transparent silicone, polydimethylsilaxane (PDMS), providing optical access to the flow inside the model. The refractive index of the working solution is matched with that of PDMS, thus minimizing reflections and distortions created by the irregular surface of the model and allowing unprecedented detailed measurements very close to the wall. Detailed steps for the development of the PDMS models can be found in Bocanegra Evans and Castillo.(14)
A schematic of the experimental setup is shown in Figure 1. A continuous inspiratory flow is supplied to the trachea, driven at a constant speed by gravity. Two valves are adjusted to keep a steady level on the reservoirs, whereas a pump is used to move the fluid from the bottom reservoir to the top reservoir. Level variation of the reservoir is <5% during the experiments. The flow along the trachea is not expected to be fully developed, since the length of the entrance tube and trachea is <50 trachea diameters necessary for pipe flow development.(29) However, both models are tested under equal circumstances, allowing detailed comparison between them. Furthermore, in humans, the epiglottis generates a jet in the entrance of the trachea, preventing the flow from achieving fully developed flow. The total length of the system, from top reservoir to the trachea entrance (48 cm) and trachea length (14.7 cm), is 62.7 cm.
Previous analysis by Bocanegra Evans and Castillo(14) imaged the tracheobronchial model with a resolution of 21 pixels/mm. The present analysis is carried with a resolution of 36.7 pixels/mm for particle image velocimetry (PIV) analysis (low resolution data) and 64 pixels/mm for PTV analysis (high-resolution data). The high resolution allows us to capture finer details of the flow near the walls, enough to resolve the flow within the cavities between rings. The laser setup for both data sets used a thin light sheet (∼1 mm thick), where a dual-head 532 nm Nd:YAG pulsed laser (Evergreen 145; Quantel) was used to illuminate the tracer particles suspended in the flow. Polyamide fluorescent particles with a density of 1100 kg/m3 and a mean diameter of 15 μm were used as tracers (Kanomax, NJ). Particle images were on average 3 pixels in diameter, minimizing peak-locking effects. A long-pass filter (OG 550; Edmund Optics) was employed to filter any remaining reflections.
The inertia of suspended particles, that is, how heavy they are in relation to the mean flow, is quantified using the Stokes number, defined as
where t0 is the relaxation time, U is the bulk velocity (0.51 m/s), and l0 is characteristic dimension (particle diameter). The relaxation time is defined as
where ρd is the density difference between the particle density (1100 kg/m3) and the fluid density (1080 kg/m3), dp is the particle diameter, and μf is the fluid viscosity, resulting in an St = 0.00136. This value is low enough so that particles can be considered tracers that accurately follow the flow.(30)
The imaging setup consists of a 14-bit CCD camera with a resolution of 1200 × 1600 pixels (ImagerProX; LaVision, Göttingen, Germany) and an 85 mm objective (Nikon Corp., Melville, NY). PIV determines the local flow velocities of particles in subregions of the image.(31) Because the depth of the rings is less than the side length of the interrogation window, it is not possible to accurately resolve the flow gradient in the ring cavity. In contrast, PTV analyzes each particle track individually and higher resolution velocity fields can be determined near the wall.(32) Hence, PTV can be considered a preferred method for the current application. PTV analysis allows the observation of flow features difficult to observe with other methods.(33)
For the low-resolution data, 21 different stations were measured in each of the two cases, smooth and ringed, along the trachea and bronchi. In addition, 25 extra stations with higher resolution were measured on the same setup, allowing to better capture the flow behavior near the walls. For every station, 2000 image pairs were collected. Each pair was processed with a multipass PIV algorithm for the low-resolution data and a hybrid PIV+PTV algorithm for the high-resolution data (LaVision). For PIV analysis, images are processed with an initial interrogation window of 96 × 96 pixel2 and a final interrogation window of 32 × 32 pixel2, both with a 75% overlap. On the other hand, in the PIV+PTV analysis the images are processed with an initial interrogation window of 96 × 96 pixel2 and particle tracking as a final step. The time separation between frames for both data sets is adapted to limit the tracer displacement to <30 pixels.
Results
Figure 2 shows the mean velocity contours and streamlines for both the smooth and the “ringed” models. Results show a separation bubble in the bifurcation, as expected,(2,19) and a bigger and stronger separation region can be observed on the smooth model, as also found by Bocanegra Evans and Castillo.(14) In Figure 3A, velocity profiles from the PIV processing are shown for both cases. The ringed model presents higher velocities on the top portion of the bronchi due to the smaller separation region. However, velocity fluctuations along the trachea do not show considerable differences, as seen in Figure 3B and C. In contrast, on the bottom of both right and left bronchi, higher velocity fluctuations can be observed on the “ringed” model (Fig. 3B).

PIV results normalized velocity (−u/U) for
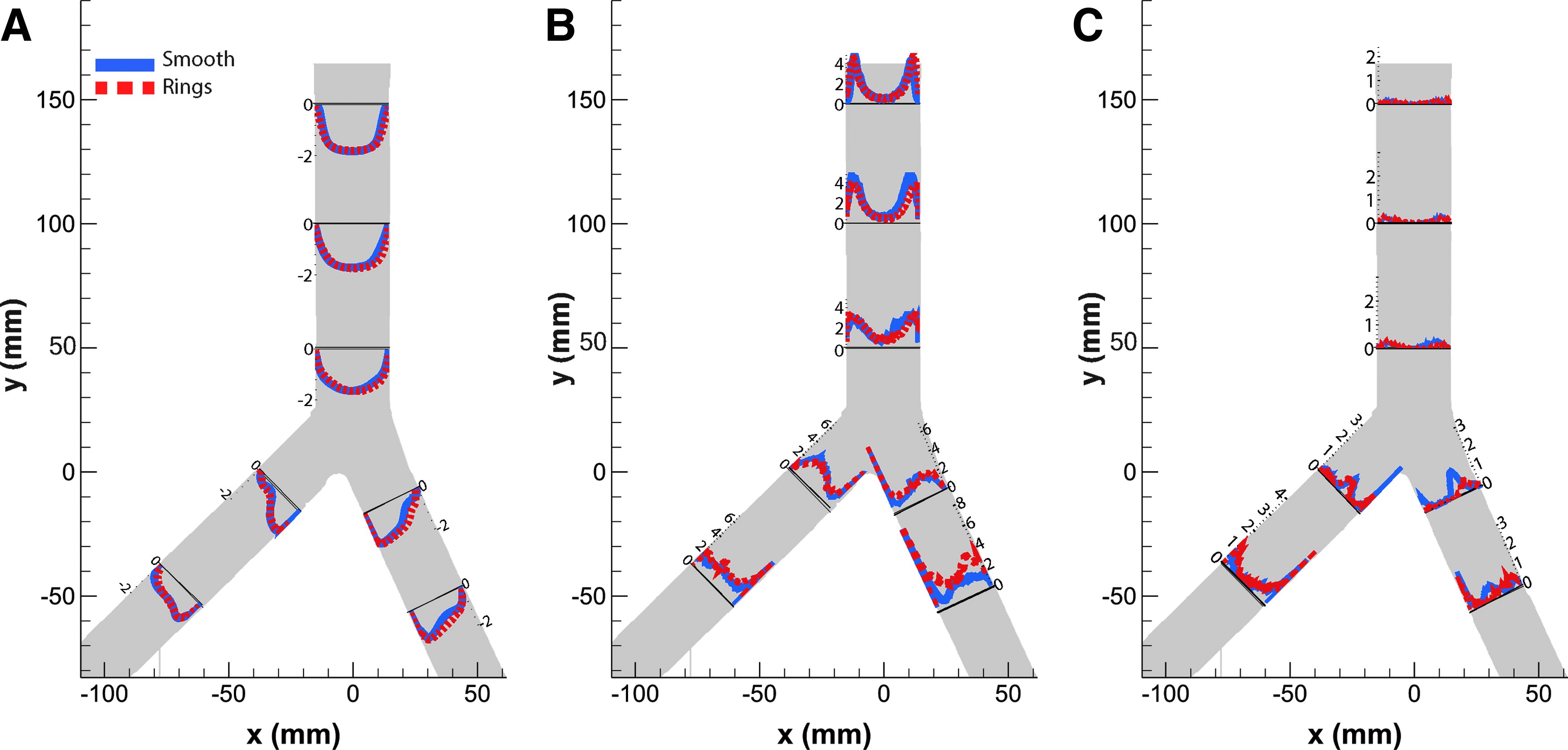
PIV results: normalized
The high resolution of the imaging setup allowed to capture a phenomenon that had not been detected in previous studies,(14,21) and which helps explain results previously reported in the literature.(20,22) In the flow near the walls, small recirculation regions between the cavities created by the rings were observed. These recirculation areas were specifically located in the upstream side of the cavities, where the expansion of the airway creates an adverse pressure gradient, triggering separation. Even though visual inspection of the data shows the recirculation, PIV analysis did not capture the phenomenon because of limited resolution. However, the high resolution data generated by PTV analysis did capture the flow within the cavities. The recirculation occurs regularly in all the cavities along the trachea.
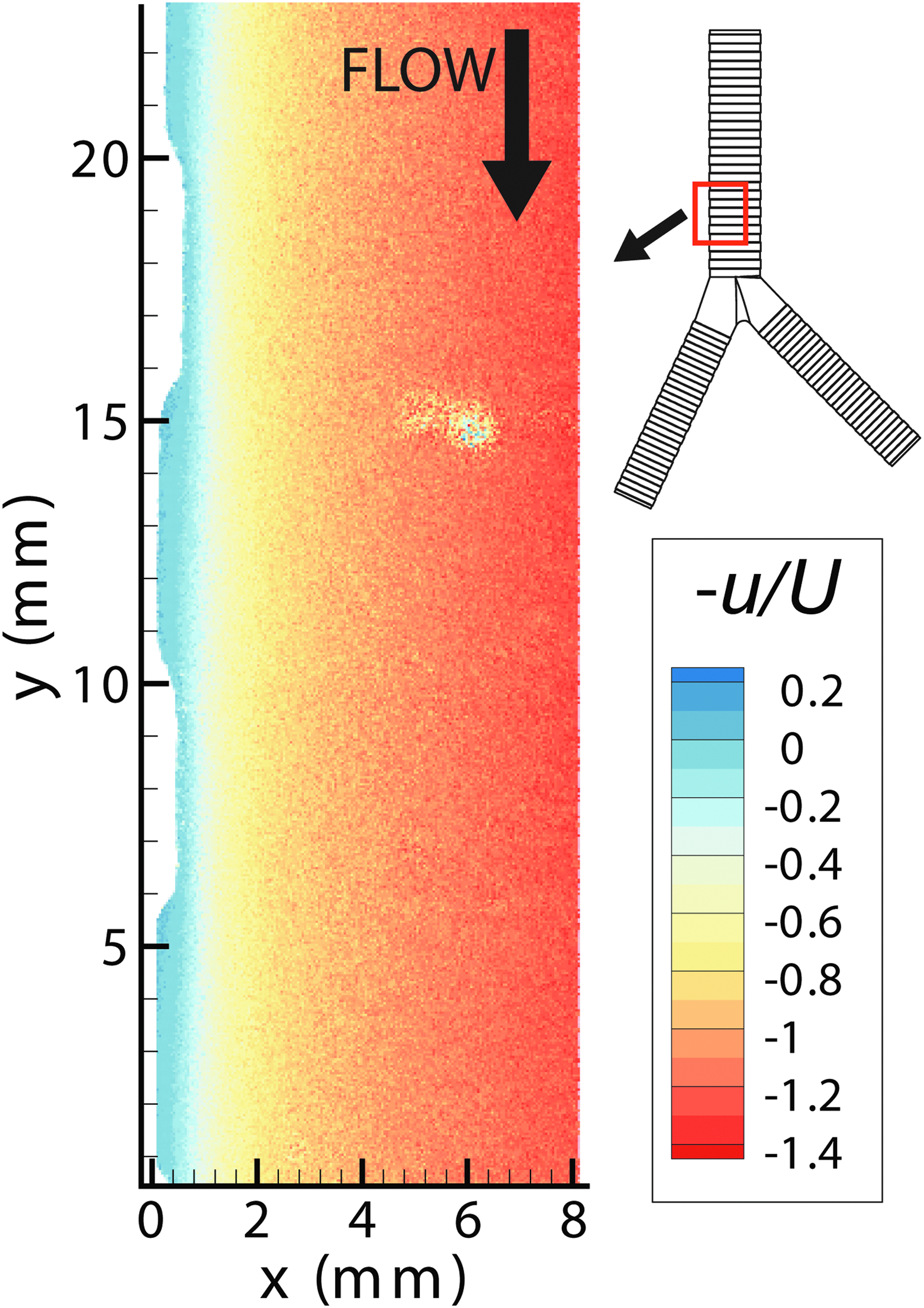
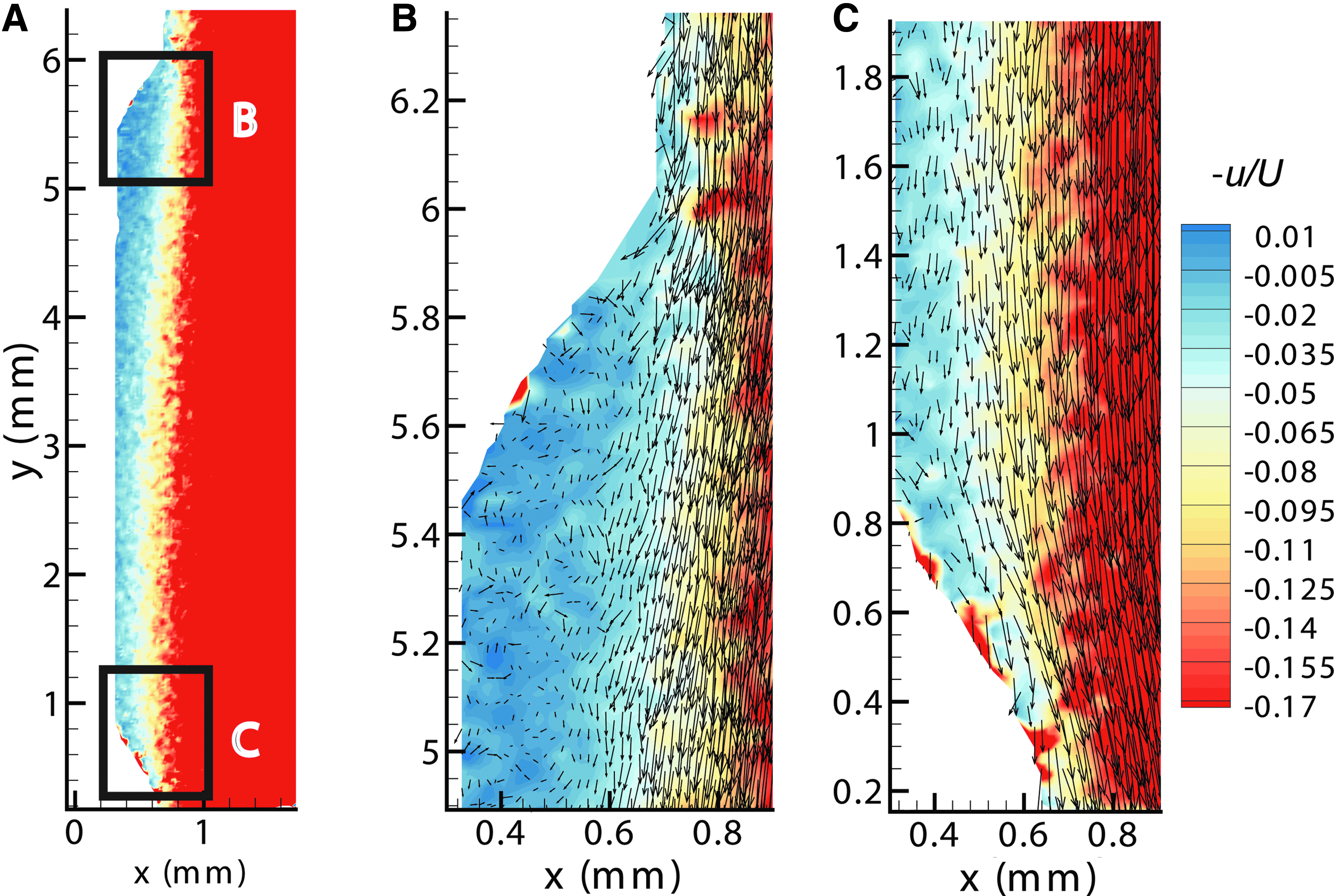
An example of a data image can be seen in Figure 4A (left); flow moves from top to bottom and the rings smoothly protrude over the trachea wall. Even though the data obtained are not time resolved, it was possible to recover particle trajectories near the wall due to the low velocity found in this area. In Figure 4B and C, the observation of the recirculation can be seen on a series of 10 superimposed images for two different ring cavities. The particles move upstream (bottom to top) near the bottom wall of the cavities between the rings, specifically in the backside of the rings. When approaching the ring (ramp shown in ring 1 and ring 2 of Fig. 4A), the particle moves away from the wall and then is recaptured by the incoming bulk flow.

Results from the PIV+PTV analysis (Fig. 5) allowed for a more detailed view of the velocity field near the wall, providing a better understanding of the flow physics inside the cavities. A reduction in the velocity can be observed near the walls. A more detailed view of the cavity is shown in Figure 6, where the contour levels are limited to highlight the flow behavior near the wall. Figure 6B shows the upstream portion of the cavity, where the recirculation can be observed. As expected from mass conservation, the velocity is affected by the difference in thickness of the walls and slower velocities are found on the cavities. Figure 6C shows the downstream portion of the cavity, where an acceleration of the flow can be observed at the end of the cavity.
PTV results near the wall between 25 and 50 mm above the beginning of the bifurcation of the trachea into the bronchi. It can be observed that the flow slows down considerably within the cavities, which is a result of the adverse pressure gradient generated by the expansion. PTV, particle tracking velocimetry.
Discussion
High-resolution experiments were carried out to capture the two-dimensional (2D) velocity field inside a trachea model with cartilage rings. A high-resolution imaging system allowed to capture the flow in detail near the wall and to further understand the flow dynamics in the presence of wall rings. PIV results present differences in velocity fluctuations, similar to the discovery from Bocanegra Evans and Castillo,(14) a slightly higher velocity fluctuation 〈uv〉 was observed on the top wall of the right bronchi, as seen in Figure 3C (x = 25, y = −10). This occurs due to the larger (macroscale) recirculation region seen in the bifurcation area in the smooth model. However, at the lower levels of both bronchi, higher fluctuations in the vertical component of the velocity 〈u2〉 were found for the model with cartilaginous rings, as shown in Figure 3B (at y < −30 mm).
In addition, velocities near the wall were obtained for the flow within the cavities generated by the rings. A small recirculation region was found in the cavities of the trachea, near the expansion ramp (upstream side), which generates an adverse pressure gradient, enabling the flow to recirculate. This is in contrast to Luo and Liu's(18) study, wherein the disturbance caused by the cartilaginous rings was not considered strong enough to cause such phenomenon. These results provide a better understanding of the effects the rings have on the flow within the respiratory system.
Apart from the direct visual observations in the captured images, a 2D PTV study confirmed the existence of the recirculation zones. This phenomenon was observed along all of the trachea cavities under the tested conditions. Few upstream velocities were captured by the PTV analysis in the bronchi cavities, but due to the lack of resolution (given the smaller size cavities in the bronchi), no conclusive evidence was obtained to determine a recirculation region on the bronchi cavities.
Furthermore, these small recirculation regions can also be observed in studies with flow over periodic hills, such as the study of Breuer et al.,(34) where the size of the recirculation is decreased as the Reynolds number increases, until it reaches a minimum and then slightly increases again. However, it is argued that recirculation regions “seem to be geometry related and not much affected by Reynolds number effects.” Therefore, it is expected that recirculation regions will decrease in size at higher Reynolds numbers, but they will still be present. Furthermore, flow reattachment is observed after the recirculation regions, which increases the probability of inertial deposition. In addition, Li et al.(35) demonstrated that the recirculation regions affect the deposition of particles. Particles are to be deposited into the trachea and the ring walls by the turbulent dispersion created by the recirculation regions.
In this study, the Stokes number for the tracer particles used is close to 0 (O [10−3]), since the density of the particles and the density of the fluid are practically the same. Owing to the large difference in density between droplets and air (three orders of magnitude), actual aerosols transported through the trachea have St = 0.02–0.23,(11) or even larger in a few cases. Thus, the denser particles cannot follow the curved streamlines and instead get deposited by inertial impaction or by separation from the recirculating flow. Hence, this effect will increase the particle deposition, which is also consistent with observations in the studies by Russo et al.(20) and Zhang and Finlay,(22) by trapping particles in these small recirculation areas and increasing the probability of collision with the walls. Consequently, this will reduce the amount of aerosol particles that reach the lower generations of the bronchial tree.
In the downstream side of the cavity, an acceleration of the flow can be observed as it approaches the contraction generated by the following ring. As suggested by Srivastav et al.,(21) particles may also be deposited by hitting the ramp due to the inertia of the particles. The results of this study uncover a mechanism that contributes to the enhancement of particle deposition observed by Russo et al.(20) and Zhang and Finlay(22) when cartilaginous rings are present. This occurs by trapping particles in the cavities due to the flow recirculation and inertial impaction. In addition, this phenomenon helps understand the effect cartilaginous rings have on tracheobronchial flow, especially flow characteristics near the wall.
This study also strengthens the argument of incorporating rings (and other anatomical features) in future tracheobronchial models for particle deposition and flow characterization to improve the data and generate effective drug delivery treatments. Furthermore, this discovery is highly valuable to the inhaled medication delivery and pollutant transport community. Finding the optimum particle size is, indeed, an area to explore further, which can lead to improvement in respiratory treatments for asthma and cystic fibrosis, among other respiratory illnesses. Future studies, including oscillating flow (inhalation and exhalation) and inertial (heavy) particle behavior in the recirculation zones, would help in selecting optimum characteristics of the particles for medication delivery systems and other treatment protocols.
Footnotes
Acknowledgments
Luna M. Castillo and many other premature children with chronic lung diseases have inspired this research. This work was possible thanks to the student fellowship from the Whitacre College of Engineering at Texas Tech University and Endowment from the Cash Family.
Author Disclosure Statement
No competing financial interests exist.
Reviewed by:
Edgar Matida
Thomas Janke