
Abstract
Abstract
Background:
Ventilator-associated tracheobronchitis (VAT) is an important risk factor for ventilator-associated pneumonia (VAP). The efficacy of aerosolized vancomycin (AV) in treating VAT has not been clearly demonstrated.
Methods:
Four mechanically ventilated patients with methicillin-resistant Staphylococcus aureus (MRSA) pneumonia were treated with an additional AV. AV (250 mg twice per day) was administered through a vibrating mesh device for 5 days. All patients were receiving intravenous vancomycin and had severe tracheobronchitis, based on bronchoscopic findings before or soon after additional AV treatment.
Results:
After several days of AV treatment, follow-up bronchoscopies showed dramatic improvement of tracheobronchitis. All patients achieved microbiological eradication of MRSA. Finally, two of four patients survived through to hospital discharge.
Conclusion:
This case series study suggests a potential role of AV in the treatment of MRSA tracheobronchitis, which were accompanied by VAP. Clinical trial addressing the efficacy of AV in MRSA VAT and/or VAP should be needed.
Introduction
V
In general, systemic antibiotics are the mainstay in the treatment of VAT/VAP. However, unexpected and variable lung penetration of systemic antibiotics might result in a prolonged course of treatment, with subsequent systemic toxicities and antibiotic resistance. As such, aerosolized antibiotics (AAs) have been long proposed as an alternative option.(5–7) According to developments in nebulizing devices (e.g., ultrasonic or vibrating mesh), the effect of AA treatments has recently been highlighted.(8,9) Although AAs for VAT/VAP have been mostly used as off-label drugs, several AAs in ICU may provide effective treatment options, including adjunctive inhaled aminoglycosides or polymixins, which are recommended in patients with nosocomial pneumonia.(10)
However, aerosolized vancomycin (AV) in this field has been rarely studied and the efficacy of AV in treating VAT has not been clearly demonstrated. We aimed to demonstrate the efficacy of additional AV in mechanically ventilated patients with tracheobronchitis who were also diagnosed with methicillin-resistant Staphylococcus aureus (MRSA) pneumonia.
Materials and Methods
We selected four patients with tracheobronchitis between January 2014 and July 2017. The diagnosis of tracheobronchitis was made when severe mucosal inflammation of the trachea and/or the bronchus was seen using bronchoscopy before or soon after AV treatment. AV (250 mg) was continuously administered for approximately 30 minutes, every 12 hours, with a vibrating mesh device (Aeroneb® Pro, Aerogen, Ireland), which was placed proximal to the ventilator Y-connector and linked to an aerosol generator. Aerosol treatment lasted for 5 days. The same device was used each day for each patient. Protocols for AV treatment are detailed in Table 1.
These four patients all underwent bronchoscopies to obtain microbiologic samples or bronchial toileting. Serial bronchoscopies were also performed to follow affected lesions. Based on quantitative or semiqualitative culture results, MRSA eradication was assessed at the end of AV treatment. Follow-up cultures were done at day 3, the end of AV treatment, and the end of intravenous treatment.
As this was a study of case series, informed consent was waived for this electronic health record review and this study was approved by the Institutional Review Board (IRB) and Ethics Committee in our institution (IRB No.: B-1708-417-107) in compliance with the Declaration of Helsinki.
Results
Baseline characteristics of the four patients are summarized in Table 2. All patients showed tracheobronchitis improvement in their serial bronchoscopies and achieved MRSA eradication through hospitalization. There were no treatment-related adverse events. Patient 1 underwent bronchoscopy due to bronchial toileting on the second day of AV treatment. Severe ulcerative lesions were observed with purulent secretion at the carina and in the left main bronchus. One day after the end of AV treatment, a follow-up bronchoscopy showed improved status with remnant ulcerative mucosa. Pneumonia was resolved and he survived through to hospital discharge (Fig. 1–A, B).
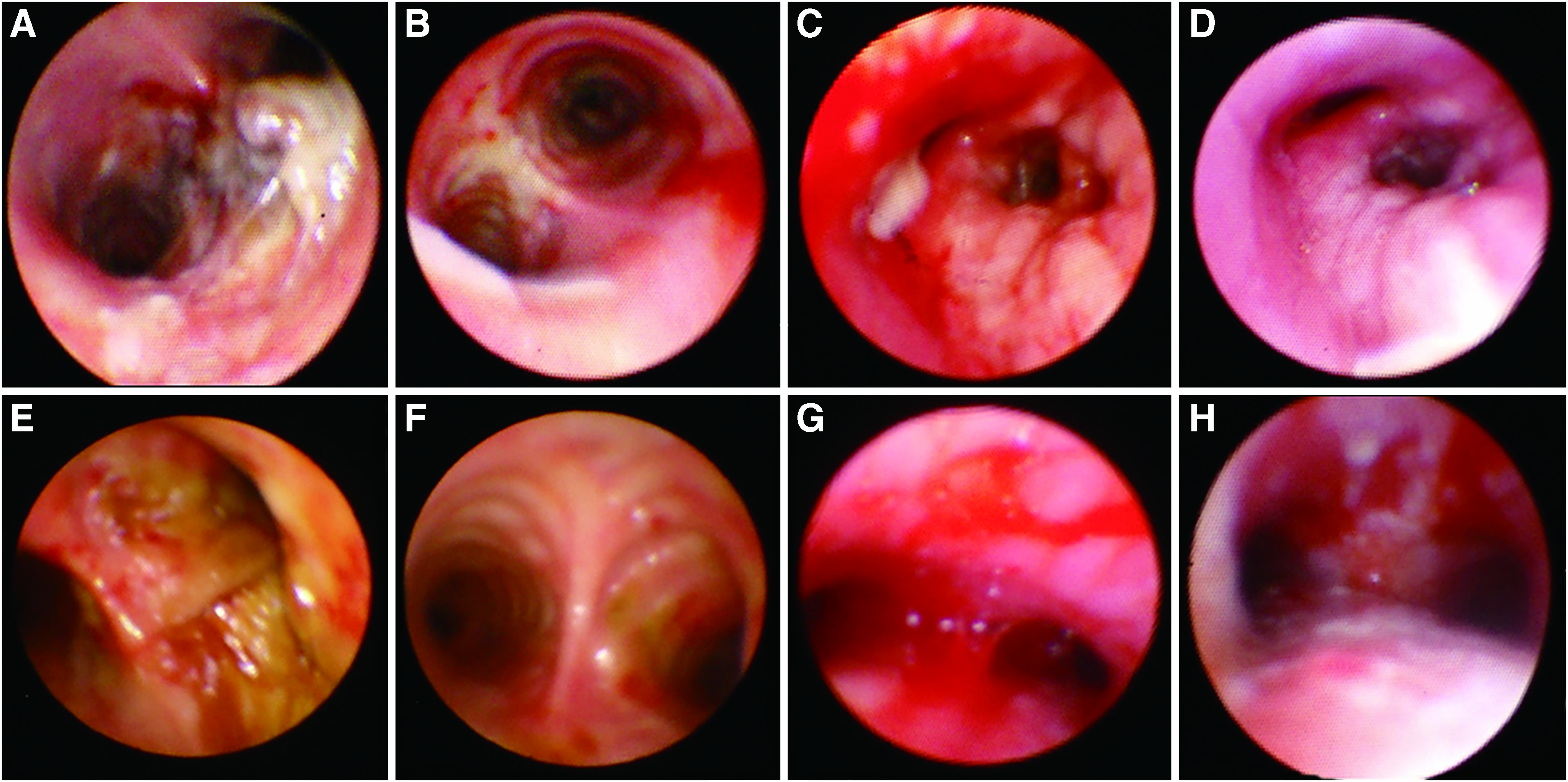
Improvement of tracheobronchitis as seen on serial bronchoscopies.
APACHE, acute physiology and chronic health evaluation; BAL, bronchoalveolar lavage; CPIS, clinical pulmonary infection score; ETA, endotracheal aspirates; HAP, hospital acquired pneumonia; MRSA, methicillin-resistant Staphylococcus aureus; MV, mechanical ventilation; VAP, ventilator-associated pneumonia.
Patient 2 showed localized consolidations in the right lung field on chest radiograph and underwent bronchoscopy to obtain a bronchoalveolar lavage (BAL) specimen 3 days before AV treatment. Diffuse erythematous hyperemic mucosal inflammation was observed in the right-sided bronchus. Five days after the end of AV treatment, a follow-up bronchoscopy showed an improved status and she was successfully weaned from MV and discharged from ICU. She showed recurrent dynamic airway obstruction on serial bronchoscopies in ICU. However, it occurred episodically even after ICU discharge. She and her family members consented to a “do-not-resuscitate”order and she died from sudden respiratory failure in the general ward (Fig. 1–C, D).
Patient 3 showed diffuse opacities in the right lung on chest radiograph and underwent bronchoscopy to obtain a BAL specimen. Severe inflammatory mucosal change with thick secretions in the right bronchus intermedius was observed. The affected lesion had resolved 4 days after the end of AV treatment. At the time of entry, he also had Acinetobacter (multidrug resistant) and Klebsiella isolates from BAL fluid, which subsequently cleared up after course of intravenous colistin. However, 15 days after the end of AV treatment, recurrent VAP due to multidrug-resistant Acinetobacter baumannii occurred during prolonged MV. Subsequently, he died from massive pulmonary hemorrhage (Fig. 1–E, F).
Patient 4 presented with a small localized infiltration on the right lung and severe mucosal inflammation with bleeding at the carina before treatment. The affected lesion was resolved on day 3 of AV treatment. She continuously improved and survived through to hospital discharge (Fig. 1–G, H).
Discussion
To our knowledge, studies that report AV treatment in MRSA tracheobronchitis are rare and we are the first to describe the dramatic improvements of tracheobronchial inflammation in four mechanically ventilated patients with MRSA pneumonia after AV treatment. Although systemic vancomycin had been administrated, the treatment period before AV treatment was relatively short. In addition, AV treatment was not accompanied with any treatment-related adverse events. Although a microbiological eradication of MRSA and clinical improvement of MRSA pneumonia were achieved in all patients, two of four patients were not finally discharged from the hospital. Some were in an advanced disease state, with MRSA bacteremia and coinfection with gram negative bacilli. However, concurrent causes of death were not directly related to MRSA infection.
The most important aspect of this case series was the visual confirmation of the efficacy of AV in MRSA tracheobronchitis. In general, nosocomial tracheobronchitis (particularly VAT) has been diagnosed clinically. Although there is no clear definition of VAT, Craven et al.(11) have proposed diagnostic criteria for tracheobronchitis, considering clinical signs and symptoms, radiologic findings, and microbiology data. However, objective assessment using clinical evaluation for the improvement of tracheobronchitis has been difficult. We consider that these bronchoscopy findings were apt examples of tracheobronchitis.
It is encouraging that MRSA was eradicated in all patients. In mechanically ventilated patients, the endotracheal tube promotes biofilm formation, and persistent colonization and infection commonly develop in airways.(12,13) In a study by Stulik et al.,(14) systemic vancomycin failed to reduce the MRSA or methicillin-sensitive Staphylococcus aureus burden in the airways among 48 mechanically ventilated patients who were confirmed as S. aureus positive through endotracheal aspirates samples. Subsequently, 38% of patients developed pneumonia despite a minimum 2-day duration of antibiotic treatment.
Systemic vancomycin may have had a limited role in MRSA eradication and improvement of tracheobronchitis because vancomycin poorly penetrates the lung parenchyma, particularly in critically ill patients.(15,16) Moreover, it is not clear whether systemic treatment led to favorable drug concentration in airway epithelial lining fluid. However, there is also no clear evidence for the role of AV against an MRSA biofilm formation and final clinical outcomes including pneumonia. Further study should be advocated to assess the appropriateness of drug delivery through aerosol route, if we can measure the drug concentration from the airway to alveoli of lung, and the mechanism and role of AV treatment in an MRSA biofilm formation should be identified.
Clinical outcomes in nosocomial pneumonia due to MRSA are still known to be poor.(17) Particularly in mechanically ventilated patients, the role of treating MRSA tracheobronchitis is still unclear in terms of the development of VAP. However, as mentioned earlier, evidence has emerged in favor of VAT treatment. We consider VAT treatment has a significant clinical effect, and the present case series suggests a potential role of AV in the treatment of MRSA tracheobronchitis and accompanied pneumonia.
In summary, this case series study suggests a potential role of AV in the treatment of MRSA tracheobronchitis, which were accompanied by VAP. Clinical trial addressing the efficacy of AV in MRSA VAT and/or VAP should be needed.
Footnotes
Acknowledgments
The authors thank all members of the medical intensive care unit in Seoul National University Bundang Hospital. This research was supported by Grant No. 11-2012-022 from the Seoul University Bundang Hospital Research Fund.
Author Disclosure Statement
The authors declare there are no conflicts of interest.
Reviewed by:
Lucy Pamer