
Abstract
Background:
Mesenchymal stem/stromal cells (MSCs) have demonstrated promise in pathogenic acute respiratory distress syndrome models and are advancing to clinical efficacy testing. Besides immunomodulatory effects, MSC derived conditioned medium (CM) has direct antibacterial effects, possibly through LL-37 and related secreted peptide activity. We investigated MSC-CM compatibility with vibrating mesh technology, allowing direct delivery to the infected lung.
Methods:
MSC-CM from bone marrow (BM) and umbilical cord (UC) MSCs were passed through the commercially available Aerogen Solo nebulizer. Known colony forming units of Escherichia coli, Staphylococcus aureus, and multidrug resistant Klebsiella pneumoniae clinical isolates were added to MSC-CM in an orbital shaker and antibacterial capacity assessed through OD600 spectrophotometry. To exclude the possible effects of medium depletion on bacteria proliferation, MSC-CM was concentrated with a 3000 Da cutoff filter, diluted with fresh media, and retested against inoculum. Enzyme-linked immunosorbent assay was used to quantify levels of antimicrobial peptides (AMPs) and IL-8 present at pre- and postnebulization.
Results:
Both BM and UC MSC-CM inhibited proliferation of all pathogens, and this ability was retained after nebulization. Concentrating and reconstituting CM did not affect antibacterial properties. Interestingly, LL-37 protein did not appear to survive nebulization, although other secreted AMPs and an unrelated protein, IL-8, were largely intact.
Conclusion:
MSC-CM is a potent antimicrobial agent and is compatible with vibrating mesh nebulization delivery. The mechanism is through a secreted factor that is over 3000 Da in size, although it does not appear to rely solely on previously identified peptides such as LL-37, hepcidin, or lipocalin-2.
Introduction
Mesenchymal stem/stromal cells (MSCs) are a self-renewing population of cells with profound immunological activity and are advancing to clinical trials for a variety of diseases.(1) They can be isolated from a wide range of tissues, with bone marrow (BM), adipose tissue, and umbilical cord (UC) being among the most commonly studied.(2) Although capable of differentiation in multiple lineages, including adipogenic, osteogenic, and chondrogenic, MSCs are not thought to typically work through replacement of damaged cells, and while cell to cell contact may be important in several of their functions, many current models assume a “paracrine paradigm,” where the majority of the MSC effects are driven by their secretome.(3) While initial human safety studies have proven encouraging, there remain concerns regarding the genetic stability of MSCs expanded under laboratory or industrial conditions. Storage of intact cells to retain high viability before transport and administration is also a significant technical challenge.(4) Hence if the MSC effects can be reproduced through utilization of their products instead of the cells themselves, a superior therapeutic is likely to result.
Acute respiratory distress syndrome
Acute respiratory distress syndrome (ARDS) is a debilitating disease of the lung that has no specific therapy and continues to have a high mortality rate.(5) Its most recognizable and lethal cause is pneumonia, where either primary or secondary infection of the lung results in uncontrolled inflammation, infiltration of leukocytes to the airspace, and ultimately drastically impaired oxygenation of the blood.(6) These infections can arise either outside the hospital (community acquired pneumonia) or in a clinical setting, often as a consequence of long-term ventilation strategies (ventilator-associated pneumonia). Causative pathogens vary somewhat between these two classes, but commonly consist of Escherichia coli, Streptococcus pneumoniae, Klebsiella pneumoniae, or Staphylococcus aureus.(7) An appreciable percentage of cases are also of polymicrobial etiology, while failure to identify the principal causative pathogen is also common. Pneumonia is also a complication of a wide range of chronic and fibrotic lung diseases, including interstitial lung disease and cystic fibrosis (CF).(8)
Antimicrobial peptides
Antimicrobial peptide (AMP) is commonly cleaved from pre-pro-peptides before release,(9) and direct killing is carried out by the following three mechanisms—inhibition of RNA, DNA, or protein synthesis, disruption of the integrity of the membrane, and interaction with cellular contents.(10) AMPs expressed by MSCs include cathelicidin (LL-37),(11,12) beta-defensin 2 (βD2),(13) hepcidin,(14) and lipocalin-2 (Lcn2).(15) LL-37 expression is upregulated in the presence of microbial structures and mediators of inflammation.(16) In addition to its broad spectrum antimicrobial activity, LL-37 can neutralize lipopolysaccharide and act as a chemotactic toward immune cells such as neutrophils and monocytes.(17,18) LL-37s antibacterial activity is credited to the binding of α-helix's two hydrophobic domains, which forms pores in the bacterial membrane.(19) Defensins have both antimicrobial and antiviral activity, with βD2 microbicidal against Gram-negative bacteria and bacteriostatic against Gram-positive bacteria.(20) Expression is also upregulated by pro-inflammatory mediators and microorganisms.(21,22) Hepcidin, a hormone regulating iron levels in the body, has broad spectrum antifungal and antibacterial activity.(23) It slows down bacterial growth through hypoferremia—decreasing iron available to bacteria.(24,25) Likewise lipocalins, proteins involved in biological protein transport, inhibit bacterial growth through sequestration of siderophores (iron chelators).(26,27) LL-37 expression can be increased through fetal bovine serum addition to media and preconditioning with cytokines IFNγ, IL-1β, and IL-12.(11,14) What is most interesting about this class of antibiotic peptides is that they do not function by a mechanism with any similarity to currently prescribed antibiotics and are therefore less likely to be subject to antibiotic resistance.(28)
Mesenchymal stem cell therapy for ARDS
MSCs have demonstrated utility in fibrotic(29–33) and infectious(3,34–37) lung disease models and are currently under investigation in clinical trials for ARDS arising from diverse etiologies.(38,39) While significant work has centered on the interaction of MSCs with lymphocytes,(40–42) neutrophils,(43,44) and both alveolar(45,46) and extrapulmonary macrophages,(47,48) it has also been demonstrated that MSCs are strong producers of AMPs such as LL-37(11) and hβD2, with expression of the latter being increased through premicrobial challenge.(13)
Nebulization technologies
Across several patient interventions including, but not limited to, invasive mechanical ventilation,(49) noninvasive high flow therapy,(50) and a facemask interface during spontaneous breathing, vibrating mesh nebulization (VMN) has been shown to deliver drug to the lungs with the potential for clinical benefit.(51) This delivery performance, in combination with technical advantages such as reduced drug wastage (residual volume), improved delivery times,(52–54) and no reported thermal inactivation of the therapeutics, provided the rationale for selection of the VMN.
Delivery of therapeutics to the airways can be performed through instillation in animal models or in the healthy human, but is not appropriate for the ARDS patient, as it is an invasive procedure and where fluid accumulation is already a problem. Nebulization can overcome this issue through delivery of a highly respirable aerosol containing the desired therapeutic over a longer time frame and with a deeper penetration throughout the lung tissue. More recently, nebulization has been evaluated as a method of MSC administration and found to have highest MSC survival rate in the jet nebulizer (72%) and slightly better therapeutic effect than IV administration in bleomycin-induced pulmonary fibrosis.(55) However, to date, the effects of nebulization on MSC-CM (conditioned medium) direct antimicrobial activity have not been investigated.
In this study we sought to examine the efficacy of MSC-CM as an inhibitor of pathogen proliferation, both before and following nebulization. We also wished to confirm that depletion of nutrients was not a factor and to further demonstrate that the integrity of known MSC-secreted AMPs and other secreted proteins such as cytokines is preserved during nebulization.
Materials and Methods
Preparation of cells and CM
Heterogeneous BM MSCs and UC MSCs were provided by the Centre for Cell Manufacturing Ireland (CCMI) and Orbsen Therapeutics Ltd., respectively. For BM, marrow was harvested from volunteers, filtered, centrifuged, and the cell pellets cultured as previously described(56) to generate human MSCs (hMSCs). UC was finely chopped and digested with 0.2% collagenase II at 37°C for 12 hours and hMSC subpopulation isolated at the tissue aspirate step from the CD362+CD45−CD271”bright” MSC population using cell surface marker antibodies by flow cytometry. hMSCs were cultured under conditions of 37°C, 95% humidity, 5% CO2, and hypoxic conditions of 2% O2, until 80% confluent, and then trypsinized and culture expanded to passage 3–4, whereupon they were used for experiments.
For generation of CM, 175 cm2 flasks of the relevant cells were allowed to reach 80% confluence, cells were washed with phosphate-buffered saline (PBS), and refed with serum-free minimum essential medium alpha (MEMα) medium. CM was harvested 24 hours later and frozen in aliquots at −80°C.
Clinical isolates
E. coli #25932 was sourced from ATCC (Manassas, VA), and S. aureus #5624 clinical isolates were provided by Discipline of Clinical Microbiology, University Hospital Galway, Ireland. K. pneumoniae #2119 clinical isolate was provided by Tullamore General Hospital, Ireland. Using a Vitek 2 automated analyzer, this organism was determined to be resistant to gentamicin and aztreonam and therefore categorized as a multidrug resistant extended-spectrum beta-lactamase as per European Antimicrobial Resistance Surveillance Network (EARS-Net) guidelines.(57) Of note, the patient from whom the isolate was derived was switched to meropenem for treatment, which appeared to be an effective therapy.
Nebulization of MSC-CM
An Aerogen Solo vibrating mesh nebulizer (Aerogen Ltd., Galway, Ireland) was placed over a sterile 50 mL collection tube in a tissue culture biosafety cabinet and secured with parafilm. Ten milliliters of MSC-CM or MEMα was applied to the reservoir and the mist allowed to condense in the collection tube. Typically, over 9.5 mL of nebulized CM was collected.
Reconstitution of MSC-CM
To negate any possible effects on bacteria proliferation due to depletion of nutrients during medium conditioning, nebulized MSC-CM was applied to a 3000 Da cutoff concentrating filter apparatus (Amicon® Ultra; Merck, Darmstadt, Germany) and centrifuged at 2000 g, checking periodically until volume was reduced to <500 μL. Concentrated MSC-CM was aspirated and made up to the original volume with fresh MEMα.
Enzyme-linked immunosorbent assay analysis
The concentration of LL-37 (Cambridge Biosciences Ltd., Cambridge, United Kingdom), hepcidin, lipocalin-2, and IL-8 (all R&D Systems, Inc., Minneapolis, MN) was assessed in pre- and postnebulization samples using a standard sandwich enzyme-linked immunosorbent assay (ELISA) kit.
Bacteria culture preparation
Bacteria beads were taken from cryostorage and added to 3 mL Bijou of Nutrient Broth (Fannin LIP, Galway, Ireland) and incubated in an orbital shaker at 200 RPM, 37°C, for 9 hours. To establish initial concentrations and confirm strain, cultures were serially diluted and plated to Brilliance Clarity urinary tract infection (UTI) agar (Fannin LIP). E. coli and K. pneumoniae were c. 5 × 109 per vial, while S. aureus was c. 10 × 109. Observed colony colors were also appropriate to pathogen strain.
Bacteria proliferation assay
Two hundred microliters of MEMα control and pre- and postnebulization MSC-CM were added to wells of a V-bottomed 96 well tissue culture dish (Sarstedt, Nümbrecht, Germany). Pathogen cultures were prepared as above and pelleted by centrifugation at 2000 g for 30 minutes. Pellets were resuspended in PBS and serially diluted such that adding 10 μL/well of culture would result in 0–10,000 colony forming units (CFUs) per microliter of the 210 μL final volume. After adding appropriate concentrations of culture to wells, the plate was incubated in an orbital shaker at 200 RPM, 37°C, for 4 hours. Plates were centrifuged at 4°C in a plate-compatible benchtop centrifuge (Model 5804R; Eppendorf, Hamburg, Germany) at 2000 g for 30 minutes and medium aspirated. The bacteria pellet was then resuspended in 200 μL of PBS and transferred to a round bottom 96-well plate and optical density at 600 nm assessed by spectrophotometer (Victor 2; PerkinElmer, MA). Control groups were serial diluted and plated to UTI agar overnight to construct OD600 versus CFU standard curves.
Aerosol droplet size characterization
Nebulized BM MSC-CM, PBS, and MEMα aerosol droplet size were assessed using laser diffraction as previously described.(58) Briefly, nebulizers were attached directly to the test apparatus (Spraytec; Malvern Panalytical, United Kingdom), and a vacuum of 5 L/min applied to ensure that all droplets passed through the laser only once. A test volume of 1 mL was used, and data were acquired until the entire dose was aerosolized. In separate experiments, aerosol flow rate was calculated by recording the time taken to aerosolize completely 10 mL of sample.
Meropenem inhibition of pathogen isolate proliferation
To approximately compare MSC-CM antimicrobial activity with an existing clinically relevant antibiotic, meropenem was serially diluted in MEMα with an upper concentration of 0.03 mg/mL corresponding to the recommended human dose.(59) Known CFUs of clinical isolates were added, incubated, and OD600 assessed as above.
Statistical analysis
Data were analyzed using GraphPad PRISM (GraphPad Software, San Diego, CA). The distribution of all data was tested for normality using Kolmogorov–Smirnov tests. Data were analyzed by one-way ANOVA, with post hoc testing using Dunnett's test with the vehicle group as the single comparison group or with Student-Newman-Keuls between group comparisons as appropriate. A two-tailed p-value of <0.05 was considered significant.
Results
Bacteria OD600 versus CFU standard curves
Plots of absorbance at 600 nm versus UTI agar CFU counts showed a linear relationship for E. coli (R2 = 0.9434) (Fig. 1A), K. pneumoniae (R2 = 0.9274) (Fig. 1B), and S. aureus (R2 = 0.8501) (Fig. 1C) when bacteria were cultured in MEMα medium. This indicates that the absorbance measurements in subsequent experiments are reflective of viable bacteria numbers.

Pathogen isolates have a linear relationship between OD600 and viable colony counts. Clinical isolate cultures were seeded to MEMα and incubated for 4 hours. Bacteria were resuspended in PBS, OD600 measured, and diluted cultures plated to UTI agar for CFU counts. OD600 and CFU were graphed and R2 values calculated.
BM derived MSC-CM is antiproliferative in ARDS relevant pathogens
Culturing pathogen isolates in BM MSC-CM significantly reduced OD600 compared to MEMα vehicle for E. coli inoculated at 10,000 CFU/μL and slightly though not significantly at 1000 CFU/μL (Fig. 2A). BM MSC-CM that passed through VMN had similar antiproliferative properties at these inoculation densities (Fig. 2A). With both K. pneumoniae (Fig. 2B) and S. aureus (Fig. 2C) pathogen isolates, BM MSC-CM significantly inhibited proliferation at inoculations of 100, 1000, and 10,000 CFU/μL. Again, BM MSC-CM continued to slow pathogen growth after passing through a vibrating mesh nebulizer at the same starting bacteria densities (Fig. 2B, C).
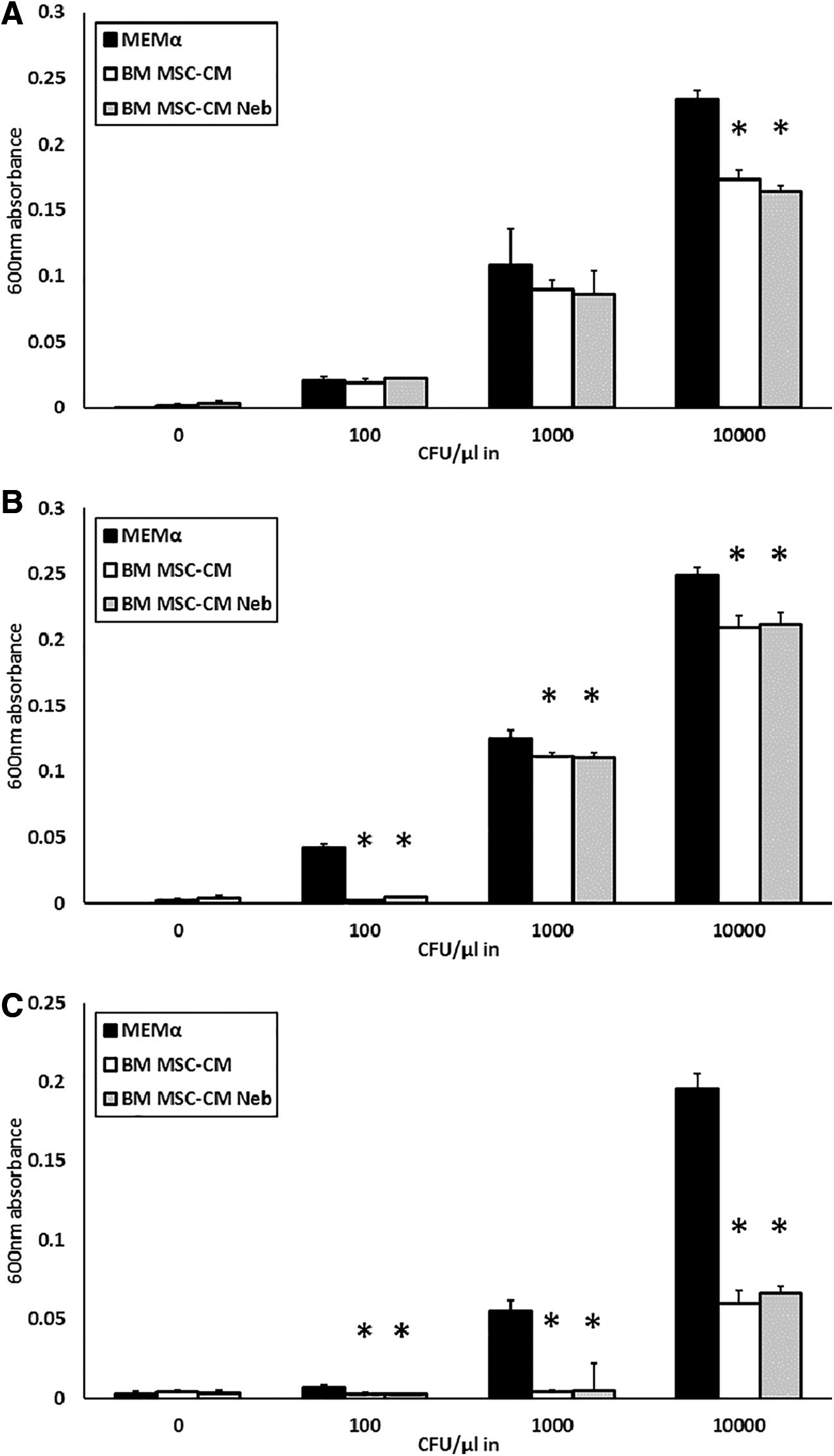
Pre- and postnebulization BM MSC-CM inhibits pathogen proliferation. Estimated CFU of clinical isolates was added to control and nebulized BM MSC-CM, incubated for 4 hours, and OD600 of resuspended bacteria measured.
UC derived MSC-CM is antiproliferative in ARDS relevant pathogens
UC MSC-CM significantly reduced OD600 of E. coli cultures compared to MEMα vehicle when inoculated at 100, 1000, and 10,000 CFU/μL, and this inhibition continues to function after nebulization of the UC MSC-CM (Fig. 3A). UC MSC-CM, both unprocessed and nebulized, had antiproliferative properties against K. pneumoniae (Fig. 3B) and S. aureus (Fig. 3C) pathogen isolates with initial densities of 1000 and 10,000 CFU/μL.

Pre- and postnebulization UC MSC-CM inhibits pathogen proliferation. Estimated CFU of clinical isolates was added to control and nebulized UC MSC-CM, incubated for 4 hours, and OD600 of resuspended bacteria measured.
Inhibition of bacteria growth and nutrient depletion
Concentrated and reconstituted BM MSC-CM was not inhibitory to E. coli growth, whereas the medium flow through after filtration concentration was (Fig. 4A), suggesting that the reduced proliferation of this pathogen may be at least partially due to depletion of glucose or other factors in the MSC-CM. However, concentrated and reconstituted MSC-CM continued to reduce proliferation of K. pneumoniae (Fig. 4B) and S. aureus (Fig. 4C), indicating that specific factors of size >3000 Da are involved in this mechanism. Of note, the flow through from the concentration process was also effective at slowing these latter two pathogens (Fig. 4B, C), indicating medium depletion or possibly extremely small secreted factors that may also be contributing to the antibacterial activity observed.
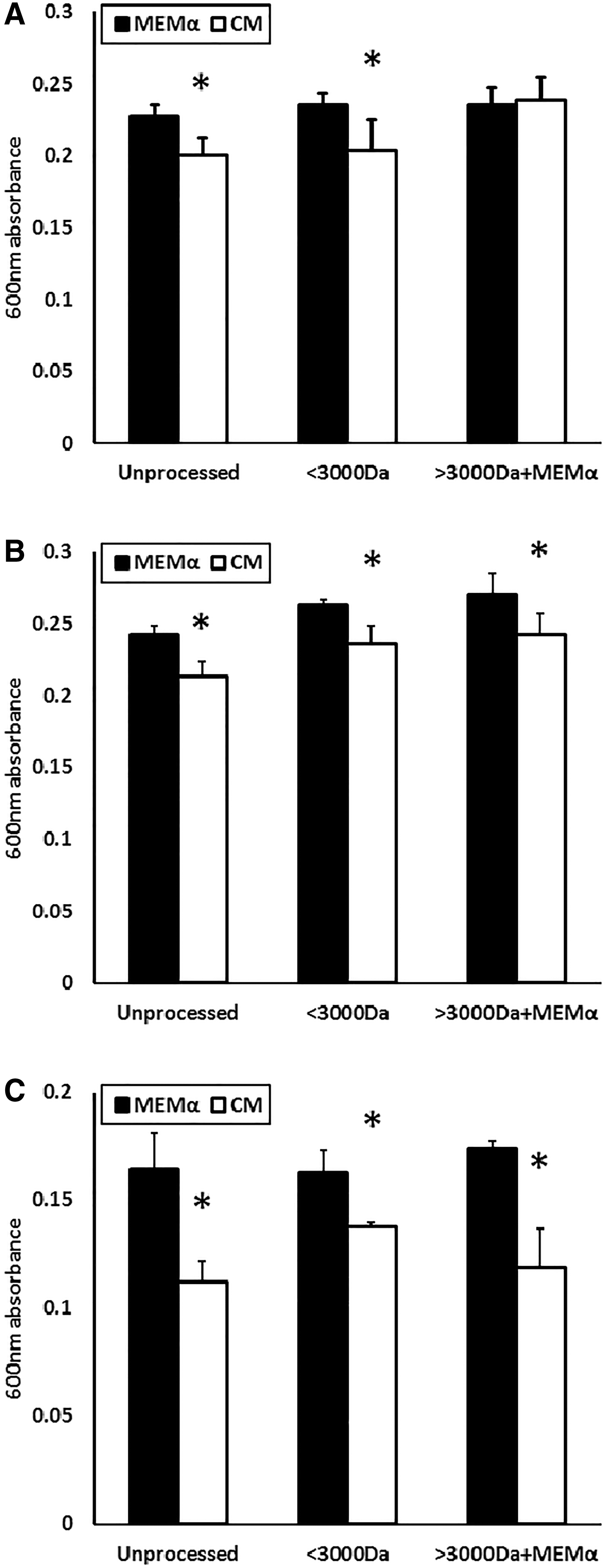
MSC-CM inhibition of pathogen proliferation is not dependent on depletion of nutrients. An estimated 10,000 CFUs of cultured clinical isolates were added to unprocessed media, flow-through from the concentrator or reconstituted media, incubated for 4 hours, and OD600 of resuspended bacteria measured.
Nebulization largely preserved hepcidin, lipocalin-2, and IL-8 but not LL-37 levels
The antimicrobial protein LL-37 was readily detected in both BM MSC-CM and UC MSC-CM (Fig. 5A). Surprisingly, however, this was almost undetectable in both MSC-CM types postnebulization, despite their continuing antibacterial properties. Levels of intact hepcidin (Fig. 5B) and lipocalin-2 (Fig. 5C) were not significantly affected by nebulization, although the importance of the low picogram concentrations detected is unknown. As an example of a non-AMP, IL-8 cytokine was readily detectable pre- and postnebulization in UC MSC-CM, although slightly and significantly lower in the latter (Fig. 5D), indicating that the lability of proteins in the MSC secretome or their adherence to the nebulizer mesh may be quite divergent. Interestingly, BM MSC-CM contained negligible levels of IL-8 compared to UC MSC-CM (Fig. 5D).
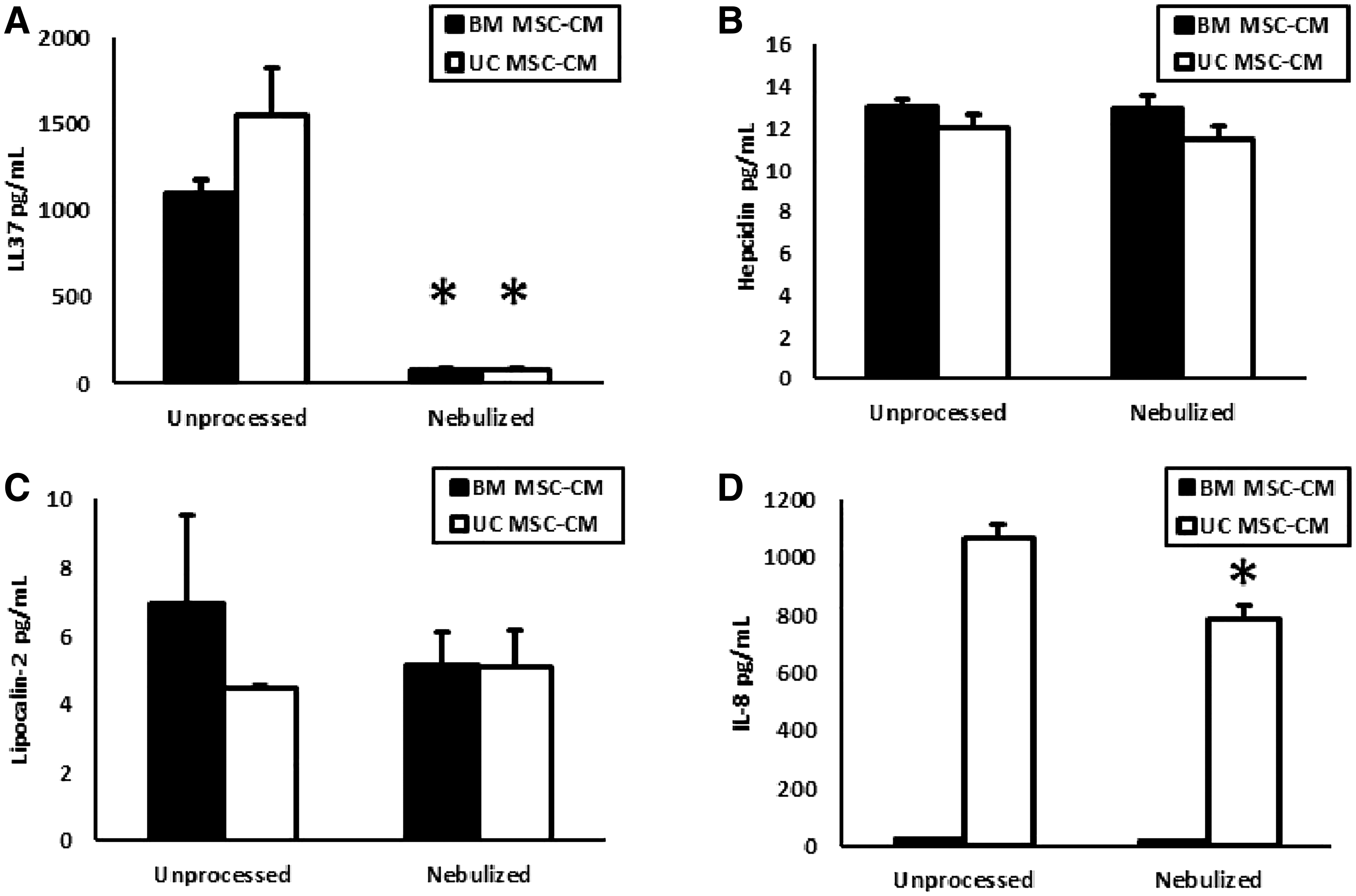
Nebulization effects on the integrity of MSC-CM proteins. Nebulized BM and UC MSC-CM were examined in ELISAs for the secreted proteins
Nebulized MSC-CM physical characteristics
BM MSC-CM had similar droplet size and flow rate as PBS or MEMα when applied to a vibrating mesh nebulizer (Fig. 6A), indicating likely compatibility with delivery to patients. Nebulized BM MSC-CM droplet size distribution is illustrated (Fig. 6B).
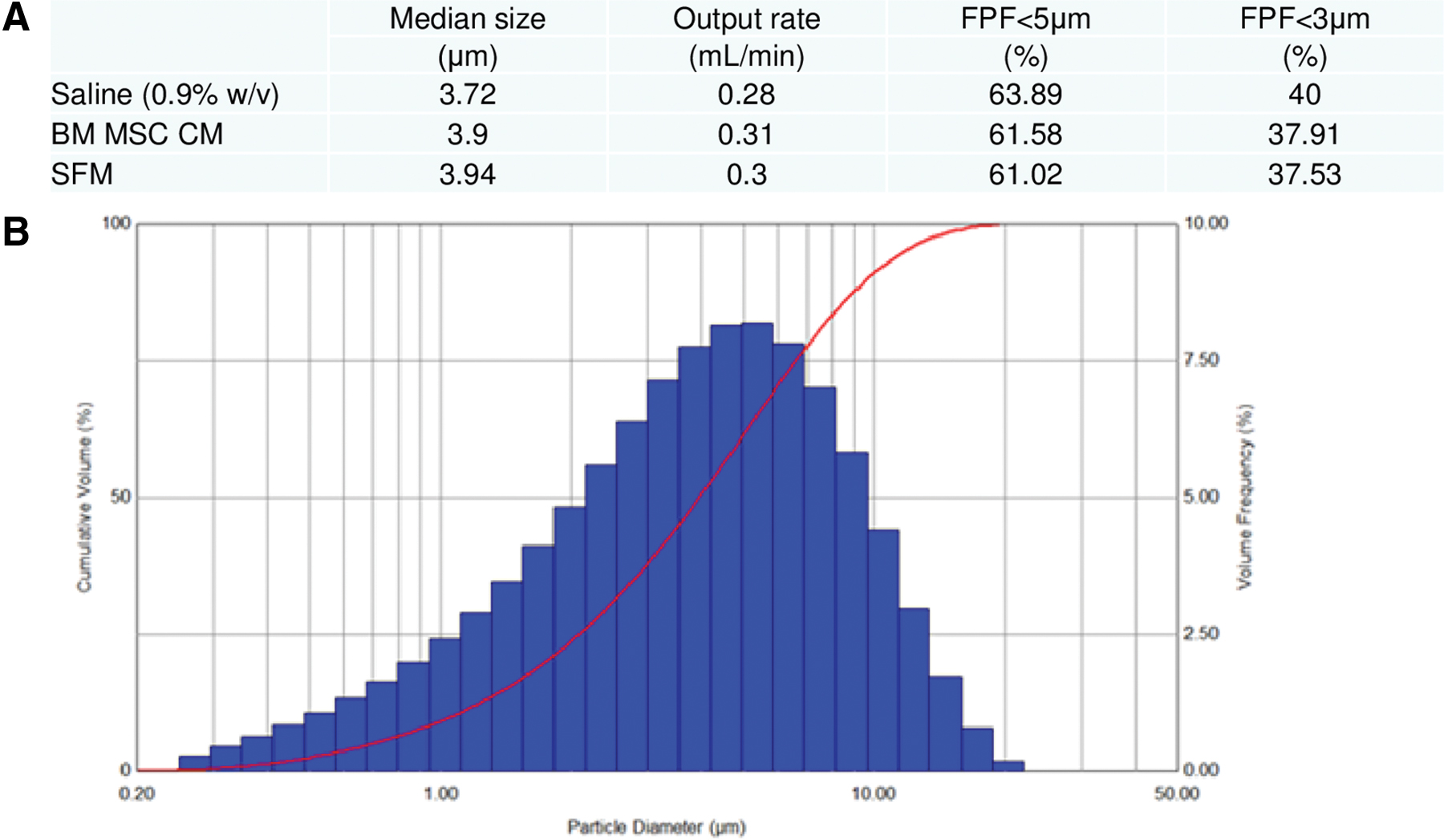
BM MSC-CM aerosol droplet size characterization. Nebulized BM MSC-CM, PBS, and MEMα were applied to a vibrating mesh nebulizer, aerosol droplet size assessed by laser diffraction, and flow-through rate calculated
Effects of traditional antibiotic therapy on clinical isolates
Meropenem antibiotic was effective on all clinical isolates at the recommended dose of 0.03 mg/mL and at least one further twofold dilution (Fig 7A–C).
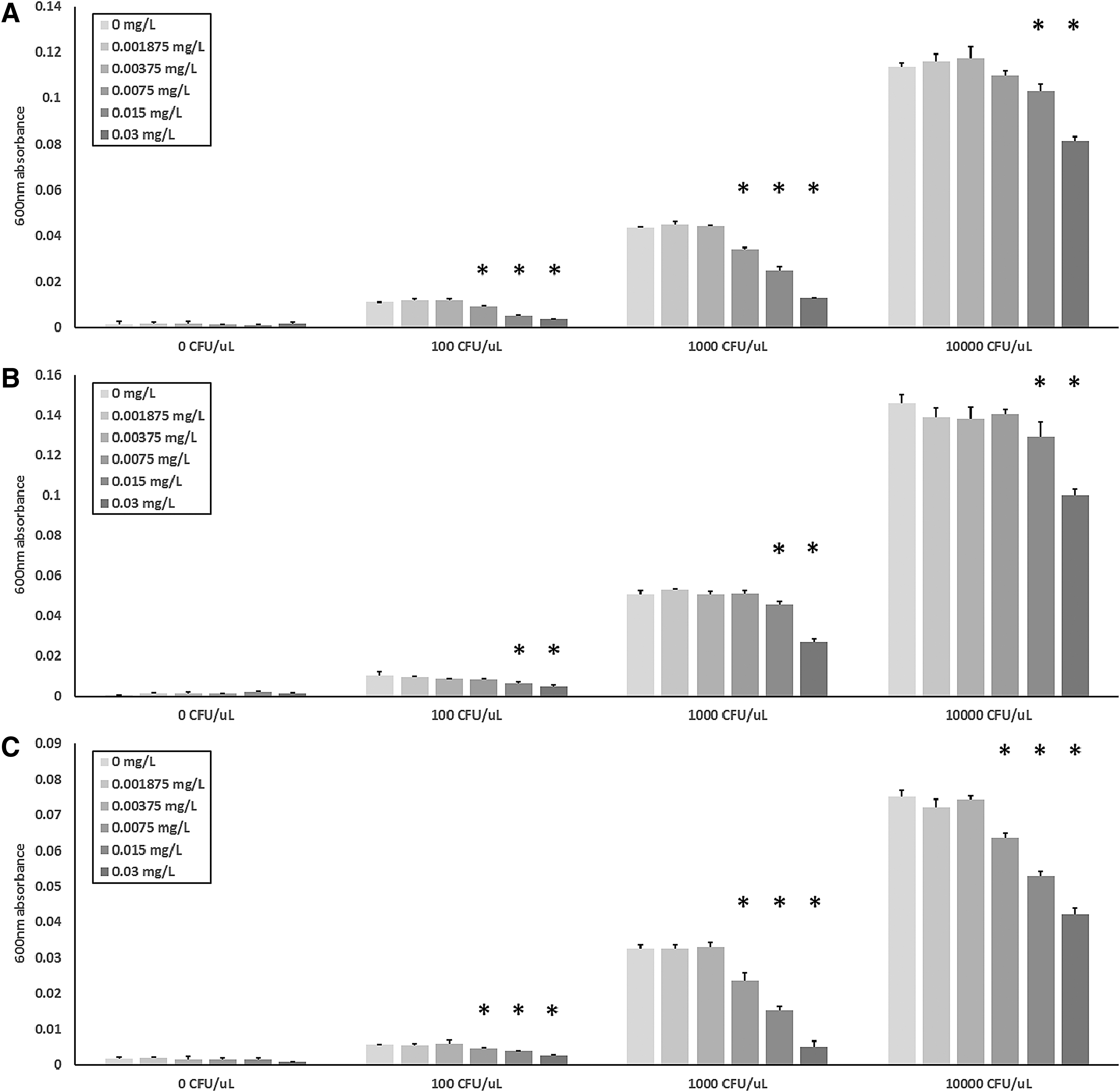
Meropenem inhibition of pathogen isolate proliferation. Various estimated CFUs of clinical isolates were added to MEMα containing various concentrations of meropenem with an upper concentration of 0.03 mg/mL, incubated for 4 hours, and OD600 of resuspended bacteria measured.
Discussion
In this study we have attempted a proof of concept approach to utilizing the MSC's secretome as a direct antibacterial agent when delivered by a high performance, commercially available vibrating mesh nebulizer. Both BM and UC MSC-CM proved to be effective at inhibiting proliferation of pneumonia relevant pathogens. This was particularly evident against the Gram-positive S. aureus used in this study. Against Gram-negative bacteria, the MSC-CM was more effective against K. pneumoniae than E. coli, which is of interest as the K. pneumoniae isolate was resistant to multiple antibiotics and proved difficult to treat in the patient from which it was isolated.
The possibility that the reduction in bacteria number was solely due to depletion of glucose, amino acids, or other nutrients in the MSC media was also negated through concentration and reconstitution of the MSC-CM, thereby restoring it to approximately the original nutrient concentrations while also keeping all proteins >3000 Da present. This also negated any possible effects of MSC waste metabolites such as lactate on bacteria growth. The preparation continued to have antibacterial effects, although not against E. coli. This may lead us to conclude that MSCs produce a range of factors with activity against different pathogens. The continuing beneficial effect of MSC-CM that has passed through the nebulizer, that is, containing only molecules <3000 Da, also suggests that some of these AMPs, or indeed nonprotein antibacterial factors, are extremely small in size, although medium nutrient depletion itself cannot be ruled out.
VMN and jet nebulizers are less prone to thermal effects than ultrasonic nebulizers and have been shown to be compatible with wide variety of therapeutics. However, in the process of converting bulk liquid into aerosol droplets, every nebulizer generates air–liquid interfaces, which can be detrimental to protein stability. The amphiphilic nature of proteins leads to protein-interface interactions, causing protein adsorption, aggregation, and partial denaturation. This is dependent on the probability and intensity of an interface reaction, as well as the aggregation propensity governed by each protein's individual characteristics.(60) The reduction in detectable LL-37 in the nebulized MSC-CM may be attributable to these effects. An unrelated protein, IL-8, while significantly reduced in quantity as assessed by ELISA, was still present in appreciable quantities. Both MSC types secreted low picogram levels of hepcidin and lipocalin-2 which were not affected by nebulization, but the significance of such concentrations of these AMPs is unknown. A larger study may be required to determine which elements of the MSCs secretome are most susceptible to nebulizer related effects and to compare various nebulizer technologies in this regard.
This LL-37 reduction could potentially cause problems in the treatment of infectious lung diseases such as chronic obstructive pulmonary disease (COPD) and CF, where mucociliary obstruction is a key feature. One study estimated that antibiotic levels need to be 25 times higher than the minimum inhibitory concentration (MIC) for bactericidal activity, when taking into account increased sputum levels in CF.(61) Likewise, droplet deposition may be affected due to remodeling caused by chronic inflammation, another characteristic of infectious lung diseases.(62,63) The beneficial effect of aerosol-mediated delivery may be decreased if turbulent breathing results in increasing conducting airway impaction. Optimization of aerosolization is important in targeting the correct portion of the lung. First, aeration may differ substantially within the lung, with apical regions being aerated twice as much as basal regions.(64) Second, droplet deposition in the lung occurs through gravitational sedimentation, diffusion, and inertial impaction. In the upper airways, inertial impaction is most prevalent,(65) which would be the regional target in COPD therapy. Whereas, in targeting alveoli, diffusion and sedimentation must be considered, meaning droplet size must be between 1 and 3 μm for optimal delivery.(65,66) This has been proven possible, however, with alveolar deposition demonstrated in models of pediatric lungs, for example,(67) and the utility of systemically targeted drugs through inhalation.(66) Further research is needed to identify possible occurrence of local toxicity and pulmonary injury, possible worsening of hypoxemia, and nebulization times that may lead to tolerance.
Despite the establishment of a linear relationship between viable pathogen and optical density at spectrophotometry, it remains to be conclusively demonstrated whether the MSC-CM activity is antiproliferative or indeed can directly kill bacteria. In addition, since the patient presenting with ARDS is likely to be immediately administered broad spectrum antibiotics, particularly where pathogens have been isolated in the bronchoalveolar lavage (BAL) or serum, it remains to be determined what added value, if any, MSC-CM therapy will have over and above that of antibiotic alone. In mitigation, this study does provide a possible additional mechanism for the effects of MSCs beyond their expected anti-inflammatory and immunomodulatory aspects. Finally, there remains much work to be done to properly identify the AMPs, or other factors, which confer the MSCs' antibacterial effects, a study of which would require a broader and dedicated proteomic approach.
In conclusion, this study has demonstrated that VMN is compatible with BM and UC MSC-CM delivery as it allows retention of the direct antibacterial effects. It also demonstrates efficacy against multiple pathogen isolates, including Gram-positive, Gram-negative, and antibiotic resistant strains. However, the active AMP mechanism remains to be elucidated and must be a topic of future investigation.
Footnotes
Author Disclosure Statement
Dr. Ronan MacLoughlin is Chief Scientific Officer at Aerogen Ltd. All other authors have no conflict of interest to declare.
Funding Information
This research was funded by Health Research Board, Dublin, Ireland (HRA-POR-2015-1099, ILP-POR-2017-024) and Science Foundation Ireland (16-TIDA-4001).
Reviewed by:
Philip Kwok
Nani Kadrichu