
Abstract
Background:
Inhalation therapy is a cornerstone of treating patients with chronic obstructive pulmonary disease (COPD). Inhaler types and through-device inhalation parameters influence airway drug delivery. We aimed to measure the repeatability of inhalation performance through four different commercially available inhalers.
Methods:
We recruited control subjects (n = 22) and patients with stable COPD (S-COPD, n = 16) and during an acute exacerbation (AE-COPD, n = 15). Standard spirometry was followed by through-device inhalation maneuvers using Ellipta®, Evohaler®, Respimat®, and Genuair®. Through-device inspiratory vital capacity (IVCd) and peak inspiratory flow (PIFd), as well as inhalation time (tin) and breath hold time (tbh), were recorded and all measurements were repeated in a random manner.
Results:
There was no difference in forced expiratory volume in 1 second (FEV1) between patients (S-COPD: 39 ± 5 vs. AE-COPD: 32% ± 5% predicted, p > 0.05). In controls, the IVCd was significantly reduced by all four devices in comparison with the slight reduction seen in COPD patients. In all subjects, PIF was lowered when inhaling through the devices in order of decreasing magnitude in PIFd: Evohaler, Respimat, Ellipta, and Genuair. The Bland-Altman analysis showed a highly variable coefficient of repeatability for IVCd and PIFd through the different inhalers for all COPD patients. Based on the intermeasurement differences in patients, Respimat and Genuair showed the highest repeatability for IVCd, while Genuair and Ellipta performed superior with regard to PIFd.
Conclusions:
Our study is the first to compare repeatability of inhalation performances through different inhalers in COPD patients, showing great individual differences for parameters influencing lung deposition of inhaled medication from a given device. Our data provide new insight into the characterization of inhaler use by patients with COPD, and might aid the selection of the most appropriate devices to ensure the adequate and consistent delivery of inhaled drugs.
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with the progressive decline of lung function. Acute exacerbation (AE) may be triggered by a viral/bacterial infection or environmental pollutants. COPD AE can last several days and it is associated with worsening of respiratory symptoms, necessitating the administration of additional therapy.(1,2)
Inhalation therapy is the cornerstone of COPD treatment in stable state and during an AE. Long-acting beta2-agonists (LABA) and long-acting muscarinic antagonist (LAMA) drugs can relieve symptoms and they are recommended as first-line treatment for COPD. Patients experiencing an increased number of AEs may have benefit from the addition of inhaled corticosteroids (ICS).(1,3,4)
There are three basic types of commercially available inhalation devices used for pulmonary drug delivery in patients with COPD. Pressurized metered-dose inhalers (pMDIs) contain a liquid medication, which is delivered as an aerosol spray. The adequate use of pMDIs can be challenging to patients as it requires the harmonization of the timing of device actuation and aerosol inhalation with the correct inspiratory flow.(5) Dry powder inhalers (DPIs) release a dose of dry powder, which patients have to inhale rapidly and steadily. Once the powder is loaded in the device, the flow generated by the patient during inhalation is responsible for the drug release.(5,6) Furthermore, the soft-mist inhaler (SMI) provides a premeasured amount of medicine in a slow-moving mist, reducing the need of coordination between inhalation and inhaler actuation.(7)
The main goal of inhalation therapy is to deliver the right amount of the right drug to the right place of action within the airways.(8) It has been shown with modeling studies that inspiratory vital capacity (IVC), peak inspiratory flow (PIF), breath hold (tbh), and the time for inhalation (tin) and exhalation during device use influence pulmonary drug deposition.(9–11) Furthermore, individual patient characteristics, including the anatomy of the mouth and upper and lower airways, also affect drug delivery.(12) In COPD, the actual physical condition of the patient such as the strength of inspiratory muscles and the severity of the disease can also influence the inspiratory maneuver during device use.(13)
The ease of use and patient preference are the driving factors when selecting an inhaler, but disease severity and symptom burden can also influence inhalation performance via inhalers.(14) A good repeatability of inhalation performance through a given device is a prerequisite for consistent delivery of inhaled medications to the airways and for effective inhalation therapy.(15) Previous studies examined lung deposition of drug particles inhaled through different devices,(12,16,17) but data on repeatability of inhalation performance through different inhalers in patients with COPD are lacking. Therefore, we aimed to test the repeatability of inhalation performances in control subjects and patients with stable COPD (S-COPD) and exacerbated COPD, using four commercially available inhalers.
Materials and Methods
Subjects and study design
Patients with S-COPD (n = 16) were recruited during regular outpatient visits, patients with exacerbated COPD (AE-COPD, n = 15) were included <72 hours after hospital admission due to an acute severe relapse. Patients had been previously diagnosed with COPD by a respiratory specialist according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) as post-bronchodilator forced expiratory volume in 1 second (FEV1)/FVC <0.70.(1) Therapy was decided by the treating physician, but all patients were treated with systemic steroids. Control volunteers (Control, n = 22) did not have a chronic respiratory disease and were recruited from employees of the department. Individuals in the S-COPD and Control groups with acute respiratory tract infections within 2 weeks and AE-COPD group who suffered from pneumonia or needed noninvasive ventilation were excluded. Subjects were recruited between April and December 2015 at the Department of Pulmonology, Semmelweis University, Budapest, Hungary.
All procedures were performed in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All subjects were informed about the methods and aims of the measurements and signed the informed consent form. The study was approved by the Ethics Committee of the Semmelweis University (TUKEB 239/2015).
Study design
The subjects attended a single visit. All patients performed standard lung function tests, which were followed by the inhalation maneuvers using at least three different inhalers after a minimum of a 30-minute break. Subjects filled out disease-specific and generic quality-of-life questionnaires.
Lung function measurements
Using an electronic spirometer and body plethysmography (PDD-301/s; Piston, Budapest, Hungary), lung function measurements were performed according to the American Thoracic Society and European Respiratory Society guidelines.(18) Pulmonary function variables were expressed as the percentage of predicted values. None of the records was post-bronchodilator measurements.
Inhalation maneuvers through different inhalers
Four commercially available inhalers were used in our study: two DPIs (Ellipta® and Genuair®), one pMDI (Evohaler®), and one SMI (Respimat®). Inhalers with active substances were not applied during the study.
For through-device lung function testing, an electronic spirometer was used (PDD-301/sh; Piston), which has built-in ambient temperature, pressure, and humidity sensors for the fully automatic BTPS (body temperature, pressure, water vapor saturated) correction. It is equipped with a PinkFlow flowmeter (PPF-18; Piston), which measures flow based on the principle of a symmetric and averaging Pitot tube. The flowmeter was attached to a plastic piece connecting the inhaler under testing (Fig. 1). Initially, eight commercially available devices were tested with a 3-L calibration pump at 30-60-90 L/min flow to investigate if our setup could accurately measure through-device flow rate. From the measured flow rate, volume was calculated. Only the four devices used in our study fulfilled the criteria for reliable flow volume measurement in our setup. The connecting piece was used to prevent an air leak and subsequent changes of measured parameters. The metal ring with a rubber overlay was attached to the different mouthpieces of the individual inhalers. All measurements were performed through a bacterial filter.
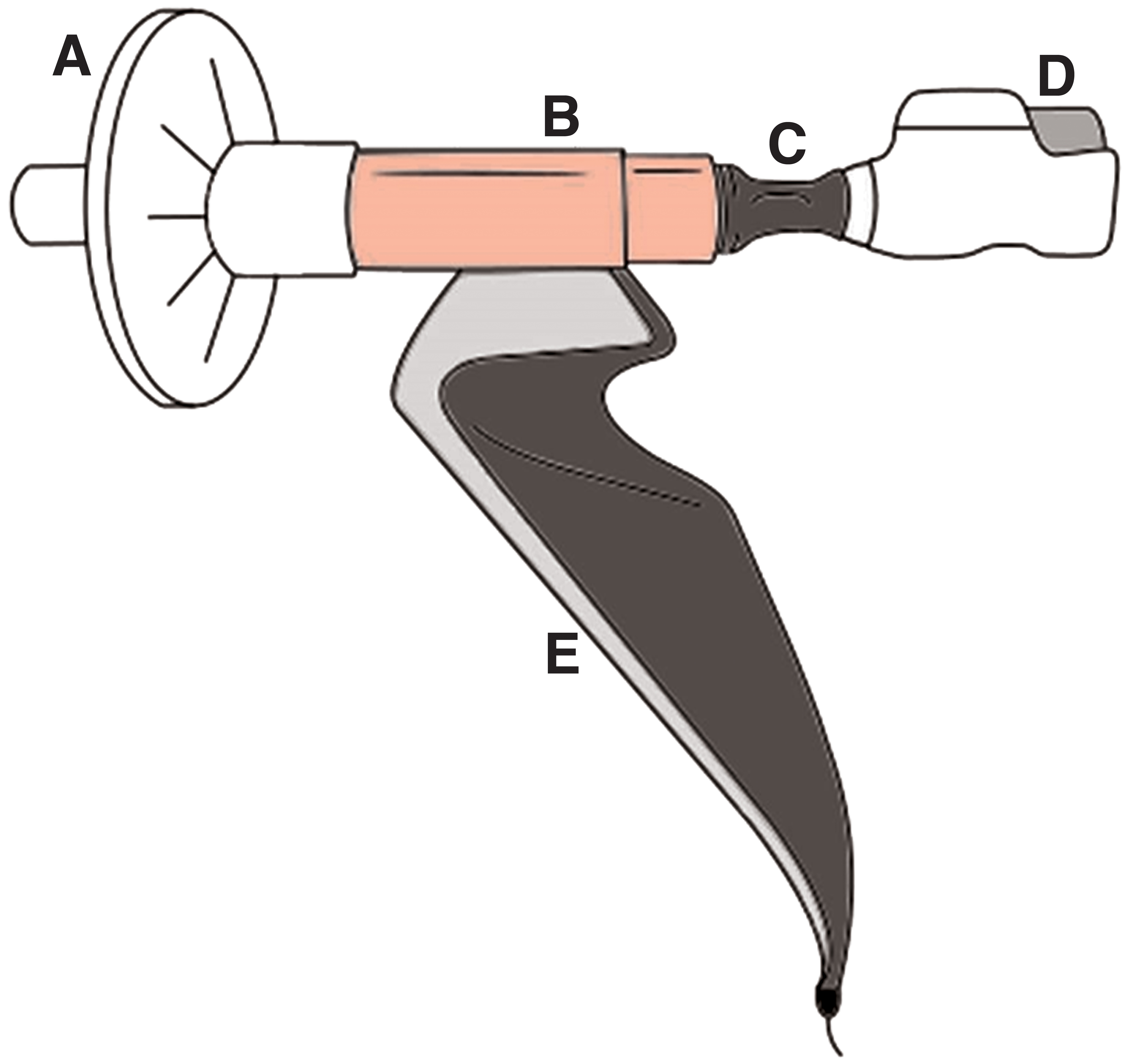
Measurement configuration attached to Genuair®.
Subjects were instructed for 5–10 minutes only before the measurements to explain and correct inhalation maneuvers as recommended by the manufacturers of each device. They could ask questions before measurements, but they were not allowed to practice inhalation maneuvers. Steps of the inhalation maneuver were as follows: (1) preparation of the device; (2) long exhalation; (3) attachment of the inhaler to the flexible connecting piece; (4) deep inhalation through the inhaler to total lung capacity, with optimal actuation of pMDI and SMI by the examiner and simultaneous recording of the prespecified parameters; (5) breath-holding for 10 seconds (when possible) while the inhaler device was detached from the connecting piece; and (6) long exhalation. Through-device inspiratory vital capacity (IVCd) and peak inspiratory flow (PIFd) were recorded. In addition, tin and tbh were also noted. Measurements for all four devices were performed first in a random manner followed by a different second sequence in all patients and controls, including a total of six-eight recordings/subject with at least a 5-minute break between maneuvers.
Control subjects had never used an inhaler before the study, but all patients were on inhaled medication, but the types of their actual regular inhalers were not recorded.
Assessment of symptoms and quality of life
Subjects filled out the Modified Medical Research Council (mMRC) and the Hungarian version of the COPD Assessment Test (CAT).(19,20) Furthermore, the visual analog scale (VAS) was used, which is scaled from 0 to 10, to measure the general health condition of the participants. A score of 0 reflected no health problems, while a poor condition was represented by a score of 10.(21)
Statistical analysis
Statistical analysis was performed using GraphPad Prism software 5 (GraphPad Software, La Jolla, CA) and SPSS Statistics V22 (International Business Machines Corporation, NY). The results are expressed as the mean ± standard error of the mean or median (interquartile range). One-way analysis of variance followed by Bonferroni's multiple comparison test, or Kruskal-Wallis test with Dunn's multiple comparison test was used as appropriate. Repeatability of measurements was assessed by the Bland-Altman test.(22) Results were considered to be statistically significant when the p-value was less than 0.05 (p < 0.05).
Results
Clinical characteristics of participants
Characteristics of patient groups and control volunteers are summarized in Table 1. COPD patients significantly differed from the control group with regard to age, current smoking habits, and cumulative smoking history. Patients with AE were slightly younger and had a higher proportion of current smokers but had less pack-years than S-COPD group patients. All patients in the AE-COPD group were considered GOLD D patients as all needed hospitalization due to the relapse, and no previous category from their stable state was available. COPD patients had a high number of comorbidities with a significantly higher number of vascular comorbidities in AE-COPD. Patients with exacerbation were more symptomatic with respect to mMRC, CAT, and VAS scores. The maintenance inhalation therapy was similar between patient groups, most patients being on triple therapy.
Clinical Characteristics of Controls and Patients
p < 0.05 versus Control, **p < 0.05 versus S-COPD.
Chi-square test: p < 0.01.
n = 21; 2n = 12; 3n = 20; 4n = 14.
AE-COPD, patients with exacerbated chronic obstructive pulmonary disease; BMI, body mass index; CAT, chronic obstructive pulmonary disease Assessment Test; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; NA, not applicable; S-COPD, patients with stable chronic obstructive pulmonary disease; VAS, visual analog scale.
Lung function results
Lung function parameters revealed similar severe airflow obstruction and lung hyperinflation in both COPD groups, while normal lung function parameters were noted in the Control group (Table 2).
Lung Function Values
p < 0.05 versus Control. FEF25%–75%, forced expiratory flow at 25%–75% of the pulmonary volume.
FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; IVC, inspiratory vital capacity; PEF, peak expiratory flow; PIF, peak inspiratory flow; Raw, airway resistance; RV, residual volume; TGV, thoracic gas volume; TLC, total lung capacity.
Through-device inhalation parameters using different inhalers
IVCd, PIFd, tin, and tbh were tested for all four devices (Table 3). IVCd was lower for all devices in controls, while only a slight decrease was noted in both COPD groups. In Controls and AE-COPD, PIFd was significantly lower compared with PIF during spirometry for all devices. In S-COPD, PIFd was only significantly decreased during inhalation through Genuair. IVCd and PIFd did not differ significantly for the individual devices between COPD groups. Inhalation time (tin) was in average between 2 and 3 seconds except for Genuair in Control and AE-COPD patients. Mean tbh was above 10 seconds in Controls and S-COPD, and slightly below the target in AE-COPD patients.
Spirometric and Inhalation Parameters Measured Through the Different Inhalers
p < 0.05 versus values obtained by standard spirometry; **p < 0.05 versus Control group; ***p < 0.05 versus AE-COPD.
IVCd, through-device inspiratory vital capacity; PIFd, through-device peak inspiratory flow; tbh, breath hold time; tin, inhalation time.
Repeatability of through-device inhalation parameters
The Bland-Altman analysis was used to define the variability of the inhalation maneuver parameters through a given device. Due to the limited number of patients in both groups, data from COPD patients with measurements in all devices (S-COPD and AE-COPD) were merged (All-COPD group, n = 20). Significant individual differences were present in all tested devices regarding PIFd and IVCd (Figs. 2–5). The X-axis represents the mean of the two measurements for IVCd and PIFd, while the Y-axis shows the difference of the repeated measurements (first measurement–second measurement).
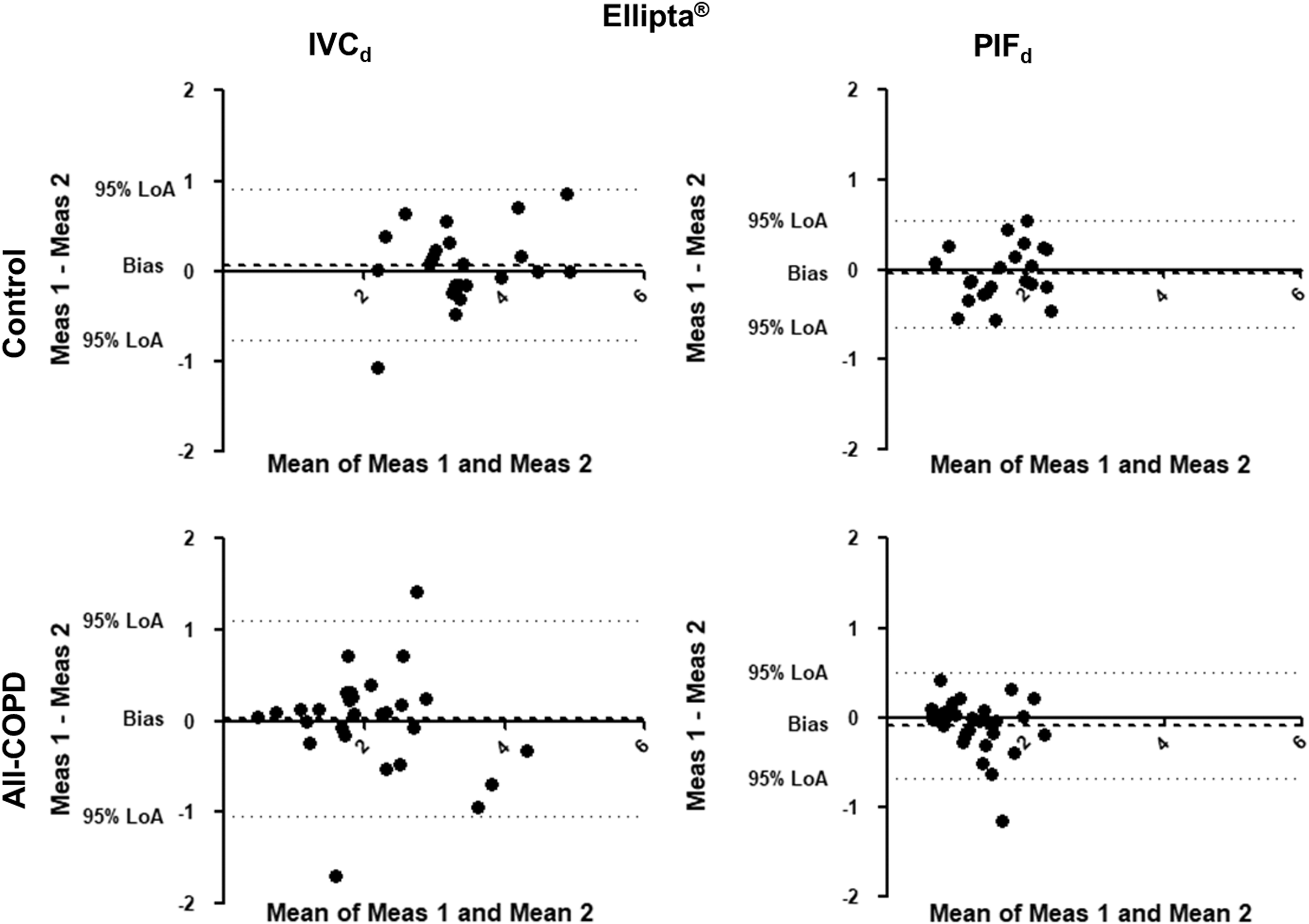
Bland-Altman analysis for Ellipta®. The X-axis represents the mean of the two measurements for IVCd and PIFd, while the Y-axis shows the difference of the repeated measurements (first measurement–second measurement). Each dot represents a person. The dashed line shows the average of the difference for all subjects. IVCd, through-device inspiratory vital capacity; LoA, Bland-Altman 95% limits of agreement; Meas, measurement; PIFd, through-device peak inspiratory flow.
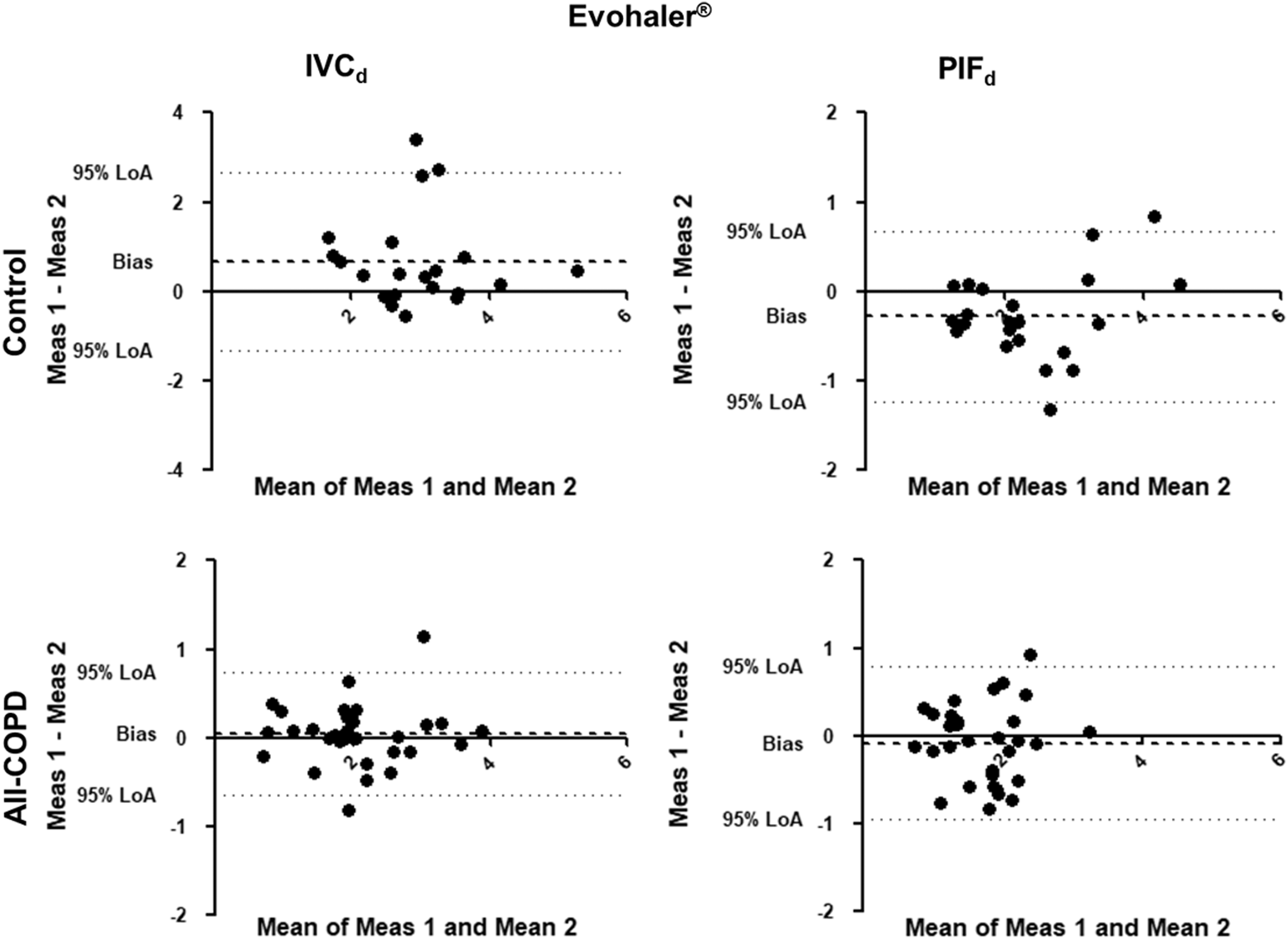
Bland-Altman analysis for Evohaler®. The X-axis represents the mean of the two measurements for IVCd and PIFd, while the Y-axis shows the difference of the repeated measurements (first measurement–second measurement). Each dot represents a person. The dashed line shows the average of the difference for all subjects.
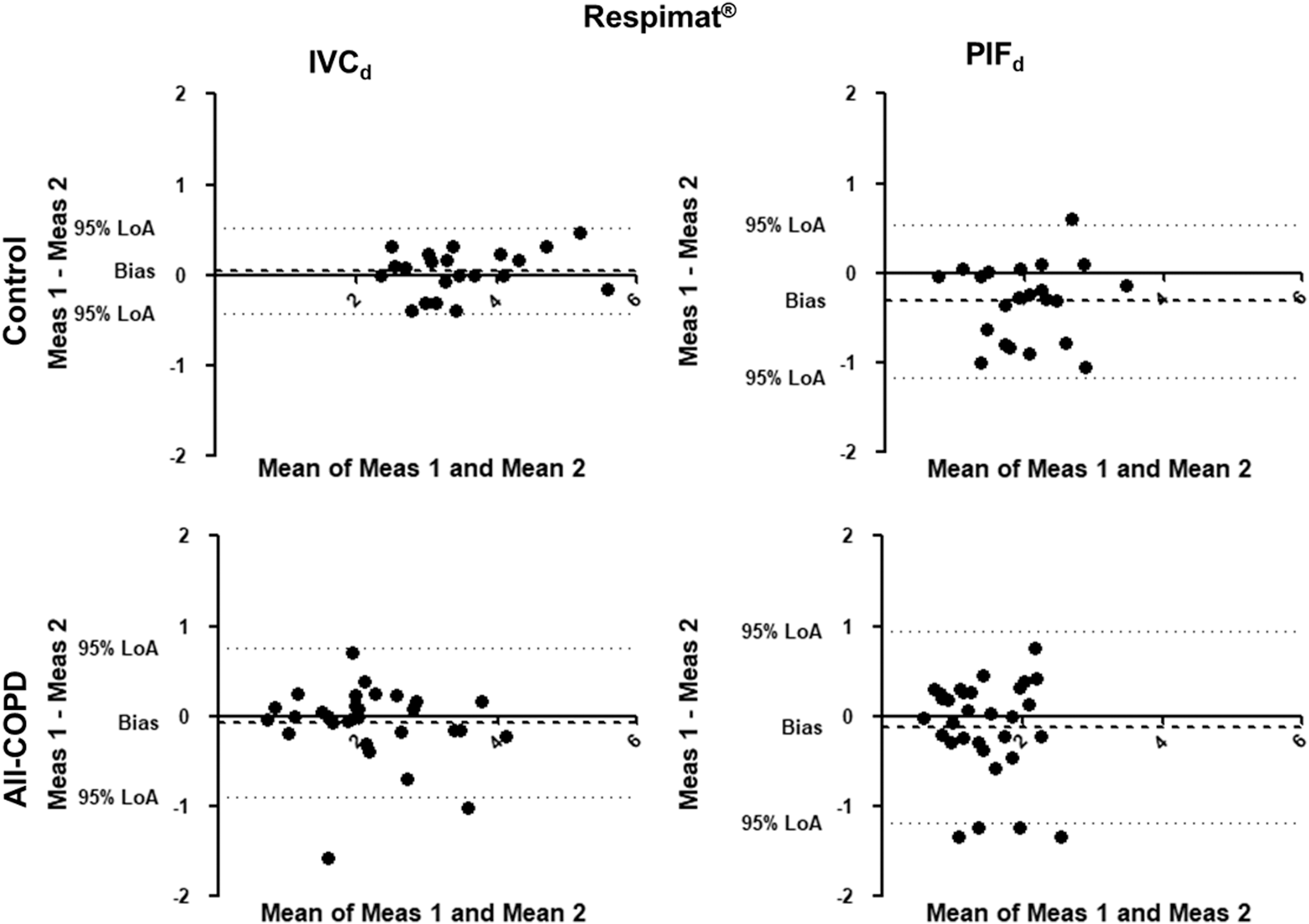
Bland-Altman analysis for Respimat®. The X-axis represents the mean of the two measurements for IVCd and PIFd, while the Y-axis shows the difference of the repeated measurements (first measurement–second measurement). Each dot represents a person. The dashed line shows the average of the difference for all subjects.
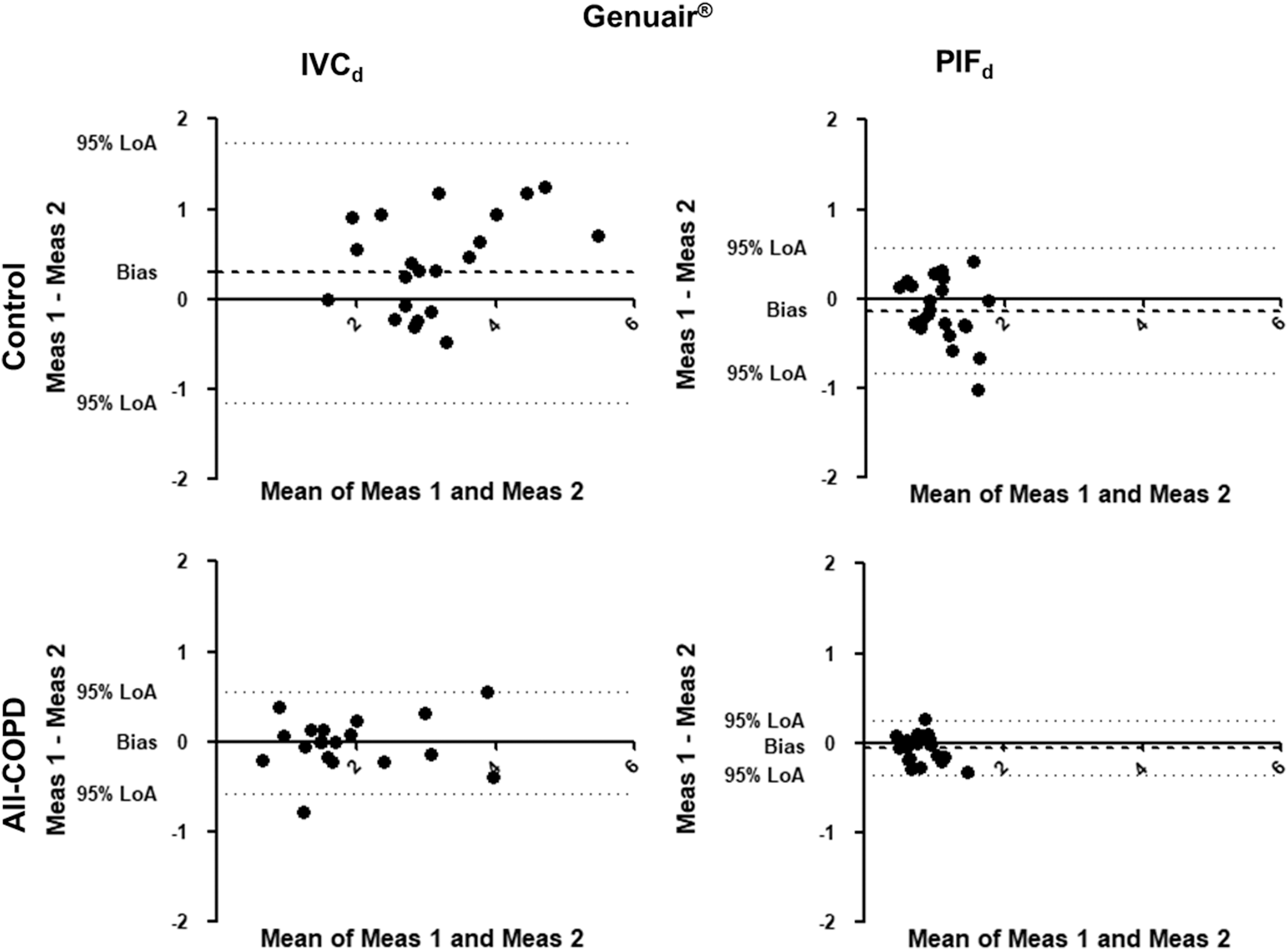
Bland-Altman analysis for Genuair. The X-axis represents the mean of the two measurements for IVCd and PIFd, while the Y-axis shows the difference of the repeated measurements (first measurement–second measurement). Each dot represents a person. The dashed line shows the average of the difference for all subjects.
We also calculated the bias (difference between the X-axis and the average mean of the two measurements for all subjects) for PIFd and IVCd in Control and All-COPD groups for each device. It shows how similar these parameters were between the two measurements, that is, deviation from zero (one-sample t-test; Table 4). We found that PIFd was significantly higher during the second measurement in controls inhaling through the Evohaler and Respimat, and there was a trend for higher values for the second maneuver with the Genuair. Furthermore, we found a trend for higher first IVCd through the Genuair in controls. Interestingly, there was only a tendency for higher PIFd for Genuair during the second measurement in patients, but no significant bias in PIFd or IVCd was noted for any inhaler in COPD.
Repeatability of Through-Device Inhalation Parameters
p-Value for one-sample t-test of the bias.
CR, coefficients of repeatability; LoA, Bland-Altman 95% limits of agreement; n, number of subjects.
Significant differences are highlighted in bold.
The 95% limits of agreement and the coefficients of repeatability (CR) of IVCd and PIFd through the different inhalers were high and variable in both controls and patients (Table 4). It is important to highlight that low CR represent better repeatability. Of note, the CR in COPD patients for IVCd were the largest using Ellipta followed by Respimat. For PIFd, CR were largest in Respimat, followed by Evohaler in the All-COPD group.
Ranking of inhalers based on the differences between inspiratory parameters
We also ranked the four inhalers based on the differences between the two measurements of PIFd and IVCd (Fig. 6). This figure highlights the inhalers with the smallest difference (given Rank 1) in parameters between the two inspiratory maneuvers. Similarly to the findings based on the CR values in patients with COPD, Respimat and Genuair produced the smallest intermeasurement differences for IVC, while Ellipta and Genuair showed the lowest variability for PIF measurements.

Repeatability sequence summary for the four inhalers.
Discussion
Our work is the first to compare the profiles of maneuver repeatability through four different commercially available inhalers in COPD patients during stable states and exacerbations. As the action of inhaled medication is highly dependent on proper lung deposition of the drugs, intraindividual variability in inhalation maneuvers can lead to inconsistent pulmonary drug delivery and consequently to varying degrees of bronchodilation.(12,17)
Adherence to inhaled medications in patients with obstructive airway diseases is poor, and inhalation technique errors have remained frequent over the past 40 years.(23,24) International recommendations also emphasize the importance of regular inhaler training in asthma and COPD.(1,25) Patients require detailed training from well-educated respiratory specialists.(1,26,27) Low adherence to COPD medications is a known important fact and one potential reason of the daily symptom variability of the disease.(23,28) In addition, patients' preferences for individual devices might vary.(29)
Individual differences of inhalation breath profiles are generally used to model inhaler performance.(12,30) The most important breath profile parameters influencing pulmonary drug deposition include IVCd, PIFd, and tin.(17,31) Inhalation parameters have an impact on fine-particle fraction, mass median aerodynamic diameter (MMAD), as well as on emitted dose, especially in DPIs.(17,31) MMAD can be determined by measurements with a cascade impactor at different flow rates and is highly influenced by PIF. Differences between interinhalation PIFd in a given patient result in altered MMAD using DPIs, as well as differences in deposition pattern and subsequent alteration of therapeutic response.(31) Tbh is crucial for small-particle deposition in the lungs. However, in this highly controlled setting directed by the examiner, no clinically meaningful difference was noted.
A former study by Feldman et al. confirmed in a crossover setting differences in lung function improvement using the LABA-LAMA combination from Ellipta compared with Respimat in COPD patients, emphasizing individual response to different inhaled therapies in a particular patient.(32) To assess variability between the repeated measurements, we also analyzed data using the Bland-Altman plot. Significant individual differences were present in all tested devices in Controls and All-COPD patients. We found a significant difference for PIFd through Evohaler and Respimat in the Control group, which can be related to the limited experience of inhaler use and the good inspiratory muscle function of these volunteers. Notably, despite the high through-device variability of PIFd and IVCd in COPD as shown by the high CR values, the biases between the two measurements were not statistically significant in COPD. This might be explained by the previous experience of patients with inhaled therapy.
According to our and previous data,(34) intrasubject repeatability in the breath profile is an important factor for therapeutic success. However, lung deposition might differ using different inhalers, drug formulations, and the quality of the produced aerosol as well as its sensitivity to breath profile.(5,8,33–36) In addition, variabilities between batches, inhaler types, and doses are also important quality attributes to inhaler performance. Our study focused on one possible influencing factor: the repeatability of inhalation maneuvers. We are aware of the limitations of this study; however, this is the first investigation recording at least two consecutive maneuvers using four different inhalers in a COPD patient or healthy volunteer.
In COPD patients, meaningful individual differences for all inhalers were noted without any specific change attributable to disease severity. Examining the through-device measurements in COPD patients, it can be observed that the repeatability of IVCd and PIFd results in a different sequence of devices in each patient (Fig. 6). IVCd difference was the smallest in COPD patients using Respimat and Genuair. However, in some patients, these only ranked at the third and fourth place, showing the individual, not predictable, sequence of inhalers. For PIFd, Genuair and Ellipta reached the best rankings, again the individual ranking of inhalers presented marked differences. These data support the clinical observation and the recommendation of the GOLD document for switching the inhaler device or molecules within the same class when therapy is considered ineffective.(1) However, no suggestion is given regarding which other device or molecules should be prescribed.
AE of COPD can last several days, and the acute worsening of symptoms necessitates additional therapy. Importantly, AEs are more common in patients with more critical inhaler handling errors.(27) It is difficult to assess though, if previous maintenance medication was properly used in our patients. The majority of patients in our AE study population used triple therapy (ICS, LABA, and LAMA) and theophylline. However, despite high treatment intensity, most patients were symptomatic. Symptom relief is the most important treatment result from a patient's perspective and a decrease in symptoms can decrease health care utilization.(37) In the exacerbating symptomatic patient group on triple therapy, there is no real possibility to further increase the intensity of inhaled therapy, but an optimal choice from the available inhalation devices can be offered. As changes of devices may decrease adherence, it would be useful to measure upfront which inhaler is best suited for a given patient.(32,38,39) This is further emphasized by the measurements performed in healthy volunteers, where the correlation of inhalation parameters was less optimal, especially using inhalers where actuation of device and inhalation needs coordination.
Our study has limitations as well. It is important to mention that only two sets of measurements were performed limiting the power of the study. A small number of patients were included in the study because of the strict inclusion criteria. In addition, only four inhalers were used, as other devices showed distortion in through-device volume and flow measurements in our setup (e.g., Turbuhaler®, Breezhaler®, Easyhaler®, and HandiHaler®). However, future studies should aim a higher sample size and the inclusion of more inhalers available on the market. Furthermore, our measurement method should be also tested to aid in the context of predicting the pulmonary deposition of inhaled drugs.
Conclusions
This study provides new evidence that inhalation parameters through different inhalers show considerable intrasubject and interdevice variability in healthy subjects and COPD patients. We found that some individuals may use specific devices more easily and more reliably. Therefore, to ensure effective inhalation therapy and symptom relief, it is of great importance to optimize inhaler technique individually, especially in patients with COPD independent of disease stability or exacerbation. Our data indicate that in COPD patients, Respimat and Genuair are ranked first and second in most patients with regard to interinhalation variability in IVCd, while Genuair and Ellipta ranked highest in most patients for PIFd. These observations could potentially provide relevant information to guide the switch of inhaler devices when therapy fails in patients with COPD.
Footnotes
Acknowledgment
The authors are thankful to Sándor Nyágúj for performing the plethysmography measurements.
Author Disclosure Statement
M.V. and T.L. received consultation fees from Chiesi Hungary, Berlin Chemie Menarini, Boehringer Ingelheim, and Glaxo Smith Kline. All other authors have no conflict of interest to declare.
Funding Information
This work was supported by KTIA_AIK_12_1_2012_0019 and the Bolyai Research Grant of the Hungarian Academy of Sciences (BO/00559/16 to Dr. Zsófia Lázár).
Reviewed by:
Bo Olsson