
Abstract
Background:
Positive-pressure dry powder inhalers (DPIs) have recently been developed that in combination with highly dispersible spray-dried powder formulations can achieve high efficiency aerosolization with low actuation air-volumes (AAVs). The objective of this study was to initially develop the positive-pressure air-jet DPI platform for high efficiency aerosol delivery to newborn infants by using the nose-to-lung route.
Methods:
Aerosolization performance metrics of six air-jet DPIs were first assessed at AAVs that were consistent with full-term (30 mL) and preterm (10 mL) neonates. Designs of the air-jet DPIs varied based on geometry of the inlet and outlet flow passages and shape of the aerosolization chamber. Aerosolization metrics evaluated at the device outlet were emitted dose (ED) and mass median aerodynamic diameter (MMAD). Designs with the best aerosolization performance were connected to a smoothly expanding nasal interface and full-term infant (3550 g) nose-throat (NT) model with tracheal filter.
Results:
The three best performing devices had characteristics of a cylindrical and horizontal aerosolization chamber with a flush or protruding outlet orifice. Including multiple air inlets resulted in meeting the aerosolization targets of >80% ED (based on loaded dose) and MMAD <1.8 μm. Reducing the AAV by a factor of threefold from 30 to 10 mL had little effect on aerosol formation. The three leading devices all delivered ∼50% of the loaded dose through a full-term NT in vitro model by using an AAV of 30 mL.
Conclusion:
With careful selection of design attributes, the air-jet DPI platform is capable of high-efficiency aerosolization of a 10 mg powder mass by using AAVs that are consistent with infant inhalation. The associated infant air-jet DPI system, which forms a seal at the nostril(s) and delivers both the aerosol and a complete inhalation, is capable of rapid and efficient aerosol administration to infant lungs, based on initial testing in a full-term in vitro NT model.
Introduction
Aerosol delivery to infants is known to have a number of problems, including poor lung delivery efficiency, high intersubject dose variability, and long administration times.(1–5) These issues occur for infants receiving aerosols during spontaneous respiration, noninvasive ventilation (NIV), and mechanical ventilation with an endotracheal tube.(2,4,6,7) Poor delivery efficiency of pharmaceutical aerosols to infant lungs has been documented with both in vitro experiments(8–10) and in vivo studies(11–14) employing commercial delivery systems and patient interfaces. Considering in vitro studies employing preterm or full-term newborn infant conditions and nasal or nasal–oral interfaces (i.e., nose-to-lung aerosol administration), lung delivery efficiencies are typically <1% and often 0% of the nebulized or nominal dose.(8,9) One exception is the in vitro study of Sunbul et al.,(8) which achieved a maximum 1.3% lung delivery efficiency with a preterm model through selection of the best performing mode of NIV for aerosol administration (high-flow nasal cannula) and optimization of the nebulizer position in the flow circuit. In vivo studies employing jet nebulizers or metered dose inhalers (MDIs) report similar lung delivery efficiencies with values <1% for preterm infants(12) and <1.5% for infants up to 1-year-old.(15–17)
It is often held that modern mesh nebulizers will substantially increase aerosol lung delivery efficiency to infants. However, Réminiac et al.(11) considered the delivery of a mesh nebulized radiolabeled aerosol to a macaque model of a full-term infant by using a nasal cannula interface. Lung delivery efficiency of the aerosol remained <1% of the nebulized dose, was highly dependent on ventilation gas flow rate, and was not improved with the use of a mask interface.(11) The recent in vivo human subject study of Corcoran et al.(18) implemented a vibrating mesh nebulizer with a nasal cannula interface applied to newborn infants and reported ∼1% lung delivery efficiency of loaded dose over a 2 minute period. Using a mesh nebulizer system specifically designed for infants on nasal continuous positive airway pressure (CPAP) that positions the nebulizer directly beside the nasal interface, lung delivery efficiencies in the range of 10%–20% have been reported.(19–23) However, it is not clear how much of this dose is first deposited in the interface and is then blown into the airways, resulting in much higher doses in the lower (dependent) lung of side-lying animals.(21,24)
Perhaps more significant than the poor delivery efficiency associated with administering aerosolized medications to infants is the very high intersubject variability. For example, in the in vivo study of Fok et al.,(12) one patient population included spontaneously breathing infants who received an MDI aerosol administered with a valved holding chamber and facemask. Mean lung dose was 1.35 μg with two actuations, whereas minimum and maximum lung doses were 0.215 and 4.52 μg, respectively. As a result, when using this common approach for respiratory drug delivery to an infant, a physician does not know whether the expected dose is delivered to the lungs or whether the dose delivered is approximately fivefold lower or threefold higher than expected.
Poor delivery efficiency and current aerosol delivery systems for infants (including jet and mesh nebulizers and MDIs) result in relatively slow lung delivery rates. Delivery times may be acceptable for low-dose medications such as bronchodilators and corticosteroids, whereas they are likely unacceptably long for high-dose medications. For example, medications such as inhaled surfactants, antibiotics, or antivirals with drug masses on the order of 10 mg would require delivery times in the range of hours to days. These extended delivery times may render many inhaled medications ineffective, or they may allow significant patient deterioration before the medication can act. Taken together, the issues of poor lung delivery efficiency, high intersubject variability, and long delivery times (as well as poor penetration of the aerosol to the deep lung) are expected to contribute to poor clinical results of any inhaled medication delivered to an infant beyond low-dose bronchodilators for asthma exacerbations.
One potential approach to improve the delivery efficiency of pharmaceutical aerosol to infants is to reduce the size of the particles or droplets. Multiple studies have previously suggested this approach(1,7,15,25–29); however, it has seldom been implemented for improving the delivery efficiency of pharmaceutical aerosols to infants. A recent study by Tavernini et al.(30) evaluated the deposition fraction of ambient aerosols (inhaled without jet or spray momentum commonly associated with inhalers(31)) in a series of in vitro nasal geometries that were reproduced from CT scans of infants in the age range of 0 to 3 months. As with similar studies,(32,33) Tavernini et al.(30) reported nasal deposition efficiency as a function of the particle impaction parameter (aerodynamic particle diameter squared times gas flow rate; da2Q) and as a combination of nondimensional variables that collapsed the deposition data to a single curve. Considering the impaction parameter data, the delivery of a conventional 5 μm aerosol from a mesh nebulizer(34) with an inhalation flow rate of 6 liters per minute (LPM) results in a nasal deposition range of 15%–80%.(30) In contrast, reducing the aerosol size to 1 μm reduces the nasal depositional loss range to ∼1%–12%.(30) As a result, the use of a relatively small particle aerosol, delivered without significant jet momentum forces,(31) will reduce nasal deposition losses and intersubject variability of lung delivered doses.
Using a nebulizer system, the previous study of Bass et al.(29) recently demonstrated high-efficiency lung delivery of a pharmaceutical aerosol in an infant airway model by using a mesh nebulizer, custom mixer-heater,(35) and excipient enhanced growth (EEG)(36) aerosol formulation. The mixer-heater device was used to heat the gas stream to a temperature that remained safe for direct inhalation and reduced the aerosol mass median aerodynamic diameter (MMAD) to ∼1.5 μm. A streamlined nasal cannula interface was used to further reduce device system and nasal airway depositional loss.(37) In vitro experiments and corresponding computational fluid dynamics (CFD) simulations demonstrated >90% delivery efficiency of the nebulized dose to a tracheal filter.(29) To achieve the correct temperature, relative humidity, and aerosol size combination, the output rate of the nebulizer was reduced. A study by Dhapare et al.(38) synchronized aerosol generation in the mixer-heater system with infant inhalation, thereby maintaining high delivery efficiency during cyclic respiration.
Previous studies have not demonstrated high lung delivery efficiency in an infant model by using a small particle dry powder aerosol. It is typically expected that small particle aerosols cannot be formed from dry powder formulations with the low air volumes and flow rates associated with infant respiration. Considering conventional dry powder inhalers (DPIs), Laube et al.(39) evaluated the penetration efficiency of a dry powder aerosol generated with the inline positive pressure Solovent (BD Technologies) device through an infant (9-month-old) nose-throat (NT) model. With this system, <4% of the loaded dose reached the tracheal filter, which required 200 mL of actuation air. Pohlmann et al.(40) developed a powder delivery system for administering high doses of spray-dried surfactant to infants. Delivery efficiency to the end of a delivery tube was ∼50% of the loaded powder dose; however, a patient interface and extrathoracic airway model were not included.
Our group has recently developed a series of low-volume air-jet DPIs by using a combination of CFD simulations, rapid prototyping, and in vitro experiments.(41–45) The air-jet DPI consists of an aerosolization chamber with a small diameter air inlet and outlet flow passages. A positive pressure gas flows through the inlet to form an inlet air jet, which initially fluidizes and then deaggregates powder in the aerosolization chamber. The exit flow passage then serves as a filter to size select the particles that are sufficiently deaggregated. These devices have been designed to efficiently aerosolize highly dispersible small and large masses of spray-dried powder formulations.(41–45) With 10 mL air bursts supplied from a hand-operated syringe, and flow rates of only 3 LPM, excellent dispersion (MMAD = 1.8 μm) and emptying (emitted dose [ED] = 85%) have been achieved.
The objective of this study is to initially develop the air-jet DPI for high efficiency aerosol delivery to newborn infants by using the nose-to-lung (N2L) route. The air-jet DPI(43) should provide a full infant inhalation simultaneously with the generation of a small particle aerosol. For initial device development, a spray-dried EEG formulation is used with albuterol sulfate (AS) as a readily quantifiable model drug. Different styles of the aerosolization chamber and inlet/outlet capillary configurations (air-jet DPI) are assessed in terms of device emptying and aerosol formation at actuation air-volumes (AAVs) of 30 and 10 mL. Initial device performance goals include an aerosol MMAD <1.8 μm and device ED >80%. For the best devices considered, delivery through a realistic NT model of a full-term newborn is evaluated with a targeted delivery efficiency value of ≥50% of the loaded dose reaching a tracheal filter.
Materials and Methods
Powder materials and formulation
AS USP was purchased from Spectrum Chemicals (Gardena, CA). Pearlitol® PF-Mannitol was donated by Roquette Pharma (Lestrem, France), and Poloxamer 188 (Leutrol F68) was donated by BASF Corporation (Florham Park, NJ).
A batch of albuterol sulfate-excipient enhanced growth (AS-EEG) powder was spray-dried by using a Büchi Nano Spray Dryer B-90 HP (Büchi Laboratory-Techniques, Flawil, Switzerland) based on the optimized method described by Son et al.(46) The AS-EEG powder formulation contained a 30%:48%:20%:2% w/w ratio of AS, mannitol,
Air-jet DPI system and experimental overview
An overview of the infant air-jet DPI system is illustrated in Figure 1. At the center of the system is the air-jet DPI, which consists of air inlet and outlet small-diameter flow pathways and an aerosolization chamber. The device is actuated with a positive pressure gas source, which in this preliminary study is a hand-actuated syringe. An important aspect of the infant air-jet DPI system is that the nasal interface is used to form an airtight seal with one or both of the infant's nostrils. Airtight communication with the infant's lungs is important such that with a single-prong interface the other nostril is held closed. The infant's mouth is also required to be held closed, either manually or with a chin strap as commonly used during infant respiratory support with nasal interfaces. The infant air-jet DPI delivers both the aerosol and a full inhalation breath to the infant in a short amount of time (typically <1 second for inhalation) and can be used to maintain a short breath hold. The use of positive pressure to deliver the aerosol and inhalation breath is expected to better expand the flexible upper airways and may enable deeper than tidal volume inhalation and improved lung penetration of the aerosol. As with manual ventilation with a bag and mask interface, this approach may also help to open closed or obstructed lung regions, further increasing the reach of the inhaled aerosol. For typical tidal volumes in the range of 7–8 mL/kg,(47–49) targeted inhalation volumes for full term (3550 g) and preterm (1600 g) infants are 30 and 10 mL, respectively, but they can be higher for a limited number of breaths to improve lung recruitment.

Schematic representation of infant air-jet DPI aerosol delivery system attached to an infant NT airway model. DPI, dry powder inhaler; NT, nose-throat.
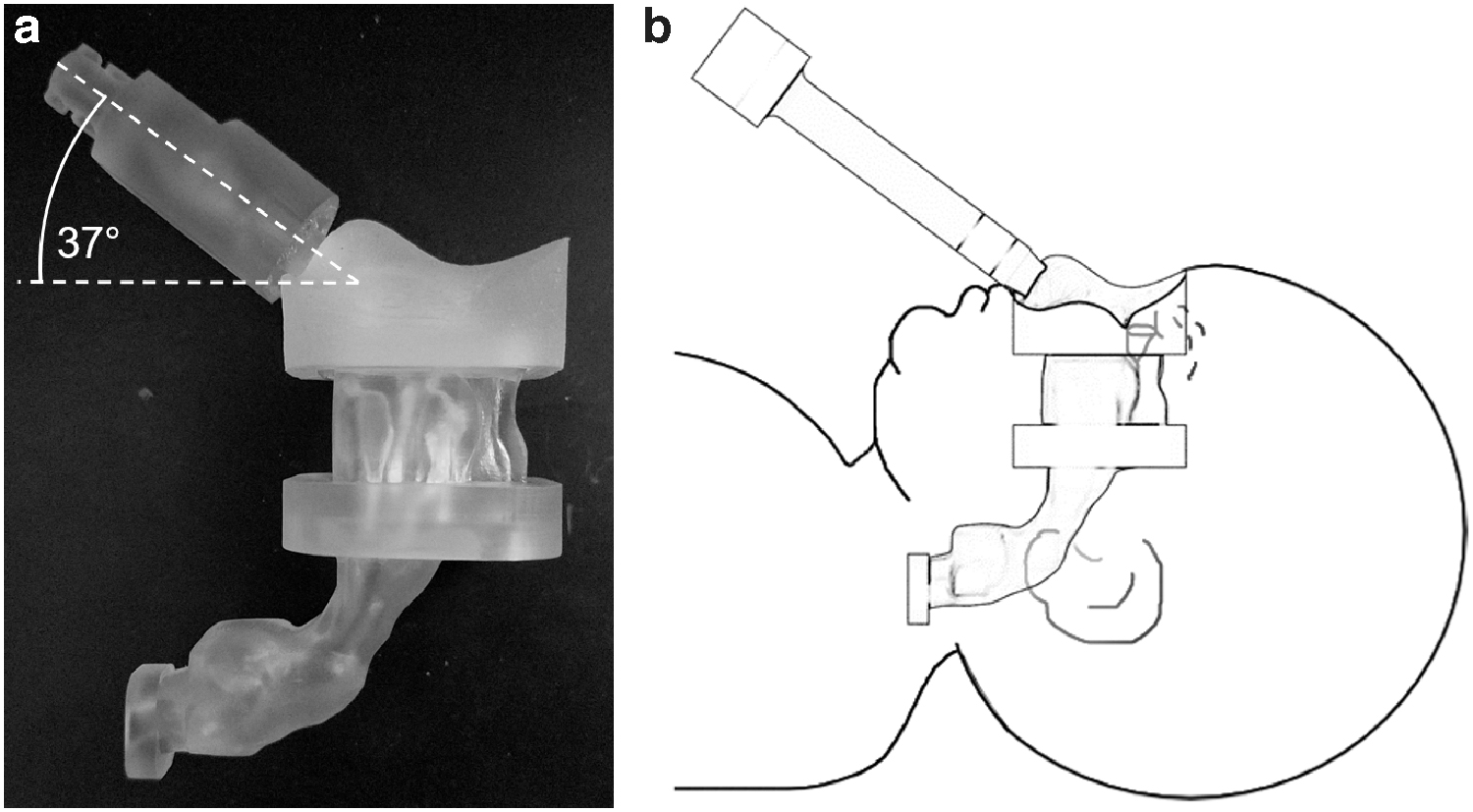
As shown in Figure 2, once the aerosol is generated in the air-jet DPI, it enters a gradually expanding nasal interface. In this study, a single-prong nasal interface was employed to minimize changes to the aerosolization characteristics of the air-jet DPI, but future studies may consider a dual-prong design as well. The exterior distal end of the nostril interface has an expanded (conical) cross-section, which forms an airtight seal with the nostril when interested ∼5 mm. The other nostril was held closed in the experiments, and the NT airway model was based on an infant with a closed oral airway.

Axial cross-section of the infant air-jet DPI connected to a gradually expanding nasal interface illustrating internal flow passages. The infant air-jet DPI consists of the inlet flow passage, aerosolization chamber, and outlet flow passage up to the point of nasal interface attachment.
Performance of the air-jet DPI approach was considered in two stages. In a first stage, aerosolization performance of the air-jet DPI through the end of the outlet flow passage (excluding the nasal interface) was evaluated for multiple internal flow pathway designs. To determine expected aerosolization performance for full-term and preterm infant conditions, aerosolization performance was assessed for AAVs of 30 and 10 mL, respectively. After evaluation of aerosolization performance, a second stage of assessment was conducted to determine the penetration of the aerosol through an infant NT in vitro model. Best performing devices from the first-stage experiments were connected to a gradually expanding nasal interface, which was then inserted (∼5 mm) into a single nostril of a full-term infant NT model ending with a tracheal filter. For evaluation with the full-term NT model, air-jet DPIs were actuated with 30 mL of air. Aerosol deposition on the tracheal filter was taken as an approximation of lung delivery. In this preliminary study, aerosol delivery through a preterm NT model was not assessed due to the limited amount of actuation air (10 mL) in comparison to the size of the tracheal filter housing (30 mL). Aerosol delivery with the full-term AAV of 30 mL is likely to penetrate through the filter housing and reach the filter substrate due to an airflow jet effect leaving the trachea. Future assessment of preterm aerosol delivery will require the development of a very small-volume high-efficiency filter setup.
It is noted that in vitro assessment of lung aerosol delivery frequently includes cyclic respiration of the model subject over an extended period. This aspect of the experimental setup is not realistic in evaluation of the air-jet DPI, because the subject's breath is delivered by the positive pressure actuation of the device, much as it would be when using a manual ventilation bag. The device is actuated rapidly, with actuation times <1 second, and leaving the device in place for a brief period is used to facilitate a breath hold. Further, because the device is operated with a manual syringe filled with air, exhalation into the aerosolization chamber of the device (which could degrade powder performance) is not possible.
Air-jet DPI designs
Basic elements of the air-jet DPI are illustrated in Figure 2 and include the small diameter inlet air flow passage, aerosolization chamber, and outlet flow passage. The design of the infant air-jet DPI was based on the studies of Farkas et al.,(43,44) which implemented sharpened capillaries to pierce a size zero capsule forming the inner flow pathway. In this study, the aerosolization chamber retains the size zero capsule volume of 0.68 mL; however, the capsule is not included as the device will be preloaded or implement a different loading mechanism. Approximate optimal inlet and outlet flow passage diameters from the studies of Farkas et al.(43,44) are retained with values of 0.6 and 0.9 mm, respectively, in most designs.
As illustrated in Figure 3, six air-jet configurations are evaluated based on different inlet/outlet air flow pathways and aerosolization chamber geometries. Four of the devices implement a horizontal cylindrical chamber (HC), one is vertical (VC), and one is spherical (S). Inlet and outlet conditions for each air-jet DPI included the options of rounded (R), flush (F), protruding within the aerosolization chamber (P), and multiple inlets (M). Details of the air-jet designs considered, that is, designs D1–D6, are provided in Table 1. Figure 2 illustrates the D2 design, including an outlet to form a 37° bend and attached to the infant nasal interface.

Internal airflow geometry of each device from air source inlet (left side of each image) to the device outlet (right side of each image).
Air-Jet Dry Powder Inhaler Design Parameters and Configurations
Triple diverging inlet jets.
Single protruding central jet, surrounded by triple parallel central jets.
D, design; DPI, dry powder inhaler; F, flush; HC, horizontal cylindrical; M, multi; P, protruding; R, rounded; S, spherical; VC, vertical cylindrical.
When the infant air-jet DPI is in use, the inlet flow passage is to be held in the horizontal position with respect to gravity and with the infant lying in the supine position. This orientation forms a bed of un-aerosolized powder on the floor of the aerosolization chamber before actuation. The complete internal flow passage of the air-jet DPI is required to curve through an angle of ∼37° for the nasal interface to correctly fit and seal with the infant's nostrils. Figure 3 illustrates how the different air-jet DPIs achieve this change in flow direction. Connection between the gradually expanding nasal interface and infant nasal anatomy is illustrated in Figure 4. Determination of the angle was based on the best fit after inserting the gradually expanding nasal interface into a flexible 3D-printed infant nose model and achieving an airtight seal. More details on the infant nose model can be found in the Full-Term Infant NT Model section.
Connection of the nasal interface to the infant NT model illustrating
The air-jet DPI designs were constructed by using 3D-printed parts with a division through the aerosolization chamber to allow for loading powder into the device. After powder loading, the inlet and outlet components were sealed together by using a twist-lock design and intermediate O-ring. In most cases, the inlet flow passage was created as part of the 3D-printed model, except with designs D2 and D6 where a custom-cut stainless steel (SAE 304) hollow capillary tube was used to form the protruding inlet. Inlet diameters were 0.6 mm in all cases except for D5, where three diverging inlets were used of diameters of 0.5 mm, and D6, where three inlets (d = 0.5 mm) were again used but in a bundled configuration. All outlets included custom-cut stainless steel capillaries with an internal diameter of 0.9 mm. Previous results have illustrated that very little spray-dried powder is lost on the stainless steel surface under the operating conditions of the infant air-jet DPI. The 37° angle was formed by bending the capillary against a fixed curve for all designs except for D1, which includes the angle as part of the aerosolization chamber design. All parts, including the nasal interface in the next subsection, were designed in SolidWorks (Dassault Systèmes, Paris, France), and they were exported as .STL files. The parts were then 3D printed at 32 μm resolution on a Stratasys Objet24 3D Printer (Stratasys Ltd., Eden Prairie, MN) by using VeroWhitePlus resin. The parts were cleaned in a Stratasys waterjet cleaning station and allowed to dry before assembly.
Nasal interface design
After initial aerosolization experiments, the lead air-jet DPIs were connected to an initial nasal interface design for aerosol delivery testing through the infant NT geometry. The nasal interface consisted of a straight gradually expanding circular cross-section. The design of the nasal interface with a length of 63 mm was based on CFD predictions that indicated that a gradual expansion geometry could effectively slow the high-speed jet, leaving the DPI with minimal aerosol loss and achieving the target outlet diameter of 4 mm for aerosol delivery to the infant nose. Dimensions of the nasal interface outlet section were based on a Hudson RCI Size No. 4 nasal CPAP cannula (Teleflex Medical, Research Triangle Park, NC) for a full-term infant. Resulting nasal interface inner and outer diameters at the outlet tip were 4 and 5.5 mm, respectively. A gradual exterior taper was included at the outlet of the nasal prong to help form an airtight seal with the infant's nostril. During aerosol delivery through the NT model, the single-prong nasal interface was inserted ∼5 mm into one nostril and the other nostril was held closed.
Full-term infant NT model
To test aerosol delivery efficiency to the lungs, administration was considered through a full-term NT airway model beginning at the nostrils and passing through the pharynx, larynx, and ending with a filter (Pulmoguard II; SDI Diagnostics, Easton, MA) at the start of the trachea.
In this initial study, the full-term NT model and delivery conditions were selected for a newborn infant with weight and height of 3550 g and 49.5 cm, respectively. As described by Tavernini et al.,(50) high-quality airway CT scans of the NT region in the 0–3 month age range are rare. To address this issue, Tavernini et al.(50) presented key points on scaling nasal airways for different ages. Two methods that produced average age-appropriate depositions were achieved by scaling based on subject height or the DV/As parameter. The DV/As parameter is defined as the airway's volume divided by its surface area. However, since DV/As is not known beyond the two points reported, scaling based on infant height is a reasonable approach. Average age-appropriate height data are readily available from growth charts and can be used for a scaling parameter. A number of studies have shown that subject height can be used as a parameter for scaling airway dimensions.(51–55) Our group recently developed a high-quality NT geometry of a 6-month-old infant that provided nasal airway deposition consistent with mean values.(29) Based on infant body length (height), the appropriate geometric scaling factor to reduce this model to that of a new-born infant was 0.73.(56) The resulting full-term newborn NT model employed in this study is displayed in Figure 5, with a volume of 3.6 mL and a nasal DV/As of 0.94 mm.
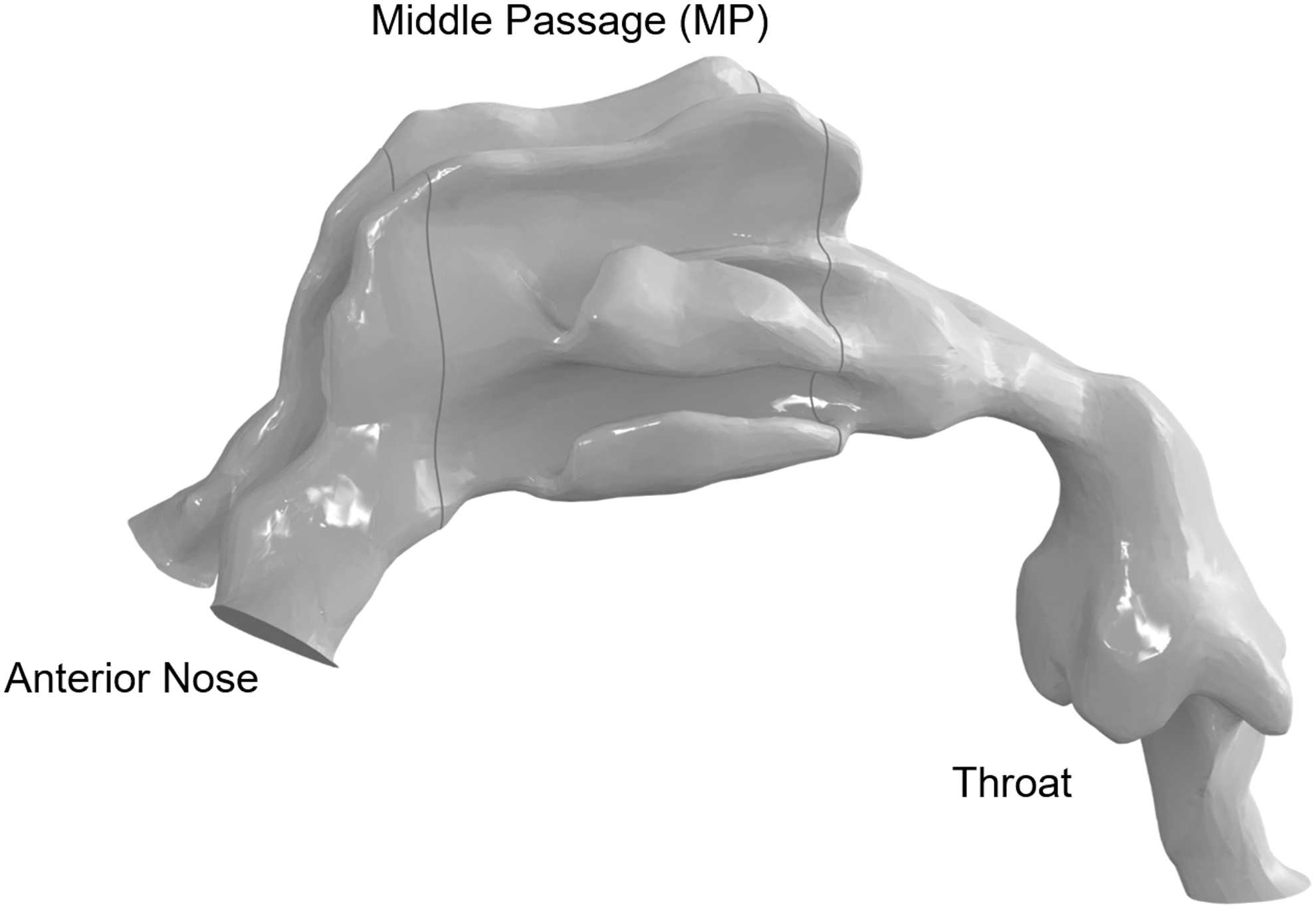
Overview of the infant NT airway model and regional sections.
The resulting DV/As value of the full-term NT model used in this study compares well with similar age-appropriate NT models in the literature. Tavernini et al.(30,50) reported nasal anatomical data for three neonates younger than 10 days old. Their DV/As values were 1.06, 0.93, and 1.0 mm with an average DV/As of 0.99 mm. Xi et al.(57) provided the nasal anatomical data for a 10-day-old female with a DV/As of 0.92 mm. Similarly, the nasal replica of a 10-day-old neonate provided by Zhou et al.(58) had a DV/As of 0.92 mm. As shown by Tavernini et al.,(30) the best characteristic length scale for collapsing impaction data to a single curve was DV/As. Since the full-term NT model employed in this study has a DV/As similar to other neonate models of the same age, we consider our scaled NT model to be a reasonable representative of full-term nasal conditions.
To provide a smooth and accurate internal airway surface, the middle passage (MP) and throat sections of the infant NT model were built by using stereo-lithography (SLA) with Accura ClearVue resin through 3D Systems On Demand Manufacturing, resulting in a rigid model. To facilitate nasal interface prong insertion and the formation of an airtight seal, the anterior nose was constructed in flexible Agilus Translucent 30-A material, also using SLA from 3D Systems. During experimental testing, the separate regions were securely connected with a paraffin film lining and a small amount of lubrication on the interface surfaces to ensure an airtight seal.
Evaluation of flow rate and actuation
For each device, differences in air-jet design geometry led to different resistances that, in turn, alter the flow rate during actuation. Actuation was performed by hand after filling the 60 mL syringe to the desired AAV (either 10 or 30 mL) with room air and connecting to the device with a luer lock adapter. Quantification of the average flow rate for each device was performed by using a pressure sensor (SSCDLNN040MBGSA5; Honeywell, Sensing and Control, Golden Valley, MN) affixed perpendicular to the outlet flow channel before the nasal interface. Pressure recordings (Sensor Evaluation Kit, Honeywell, Honeywell Sensing and Internet of Things, Fort Mill, SC) were taken at 500 samples per second. The pressure profile of the actuation was used to calculate average flow rate based on the fixed AAV and elapsed time. Elapsed time was determined by the number of samples with a pressure reading over a set threshold recorded during actuation, where the threshold was set to double the baseline pressure value.
Evaluation of air-jet DPI aerosolization performance
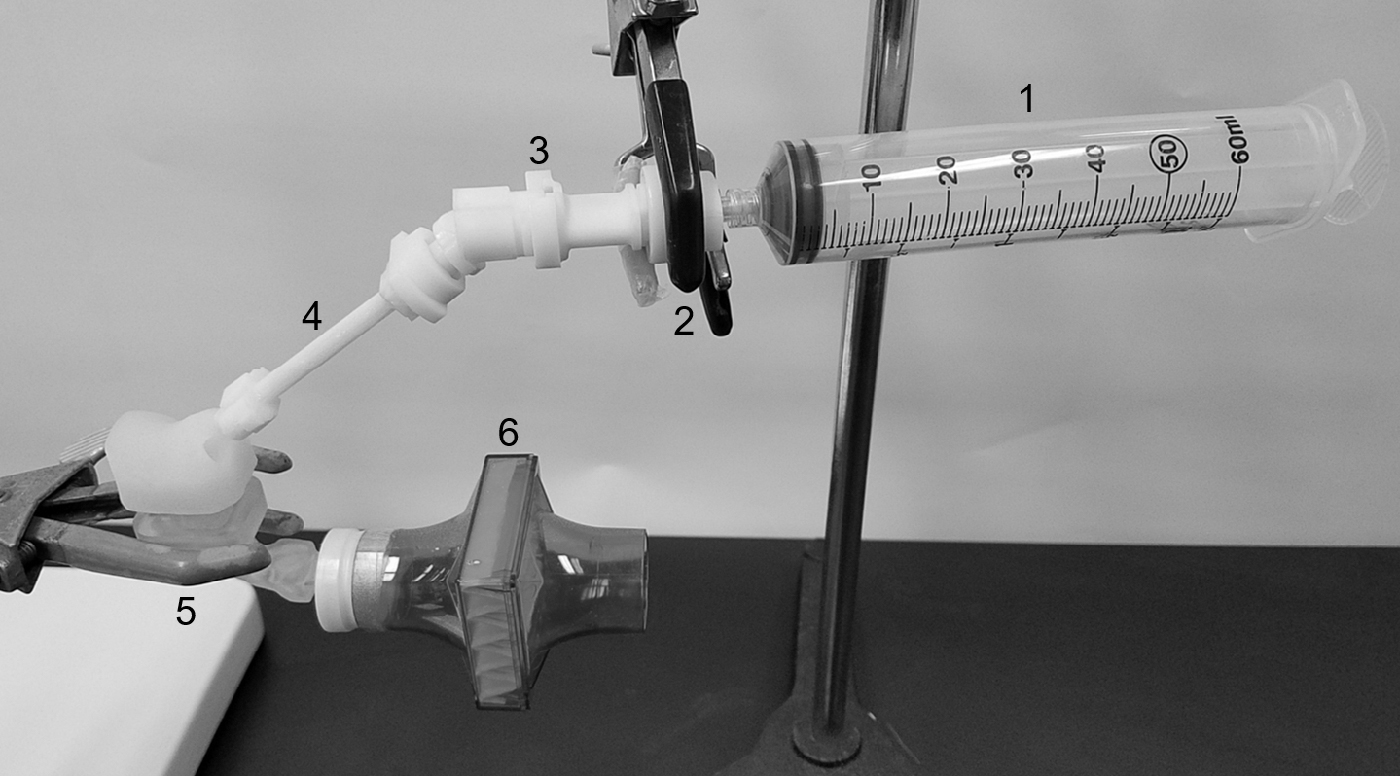
Consistent with previous studies by our group, experiments used 10 mg of AS-EEG powder formulation (manually weighed) and a Next Generation Impactor (NGI, MSP; TSI Incorporated, Shoreview, MN) for aerosol particle size analysis. After weighing, the powder mass was poured into the inlet half of the air-jet DPI, which was then assembled and sealed with a twisting motion. To assess the aerosol size distribution, the air-jet DPI (without the nasal interface) was attached to the preseparator inlet of the NGI by using a custom adapter, as seen in Figure 6. This adapter positioned the outlet of the air-jet DPI 1 cm away, perpendicular from the center of the preseparator inlet with open space allowing for co-flow room air to enter the NGI, which was operated at a flow rate of 45 LPM by using a downstream vacuum pump. Room temperature and relative humidity were recorded for every run and found to be between 21°C–24°C and 20%–40%, respectively. The NGI was positioned 53° off horizontal to allow the device to remain level during use and maintain an inline flow path from the device outlet to the NGI inlet (shown in Fig. 6), as it would be during administration to a supine infant. Each stage of the NGI was coated with MOLYKOTE® 316 silicone spray (Dow Corning, Midland, MI) to minimize particle bounce and re-entrainment. The NGI flow rate of 45 LPM was chosen to ensure collection of the aerosol, minimize any effects of settling, and provide appropriate stage cutoff diameters for evaluating small aerosol sizes. Before each set of experimental runs, the flow rate was confirmed by using a flow sensor (Sensirion SFM3000; Sensirion AG, Stafa, Switzerland) connected to the NGI inlet.

Experimental setup for device aerosolization performance as determined by NGI. Parts labeled include: 1. Air source (60 mL syringe), 2. Luer adapter, 3. Air-jet DPI (D2 pictured), 4. NGI adapter, 5. Vacuum for NGI (operated at 45 LPM), and 6. Guide to angle the NGI at 53° off horizontal. Insert shows expanded view of custom NGI adapter schematic allowing for co-flow room air. LPM, liters per minute; NGI, Next Generation Impactor.
Each device was actuated into the NGI via the 60 mL hand syringe at 30 or 10 mL AAV to compare aerosolization at full-term or preterm infant conditions. Three replicate runs for each device at each condition were performed in a randomized order. Analysis metrics included ED and MMAD. The ED was calculated as the mass of AS in the loaded dose minus the mass of AS remaining in the device divided by the initial loaded mass of AS. Aerosolization calculations were based on the mass of AS recovered in the NGI. The MMAD/ED was also used as a general parameter to indicate overall performance (lower values being preferable). Drug masses were determined by using high-performance liquid chromatography (HPLC) analysis, as described next.
Evaluation of lung delivery in the full-term NT model
Based on device assessment, the second stage of this study used the three best performing designs for full-term NT in vitro model testing at an AAV of 30 mL. The experimental setup was the same as for device assessment in terms of device actuation, powder loading, and randomization. However, instead of the device connecting to the NGI adapter, it was connected to the gradually expanding nasal interface, as seen in Figure 7, which was inserted ∼5 mm into the left nostril of the infant NT model (the right nostril was manually held closed during actuation). A small amount of lubrication was applied to the exterior of the prong to ensure an airtight seal. All NT model segments were internally coated with silicon spray to minimize particle bounce similar to airway surface liquid. At the end of the NT model, a respiratory filter (Pulmoguard II; SDI Diagnostics, Easton, MA) collected powder passing through the extrathoracic regions and represented the amount of drug delivered to the lung. After aerosol delivery, the nose was held closed and the syringe was not disconnected for 10 seconds to help aid in the capture of all particles. In practice, a breath-hold such as this would help prevent drug loss during expiration, as the EEG particles significantly increase in size through hygroscopic growth.(59) Calculations for ED and regional deposition, including the nasal interface and in the NT model and tracheal filter (amount delivered to lungs), were expressed as a percentage of the loaded dose of AS.
Experimental setup for aerosol delivery efficiency testing through the infant NT model. Parts labeled include: 1. Air source (60 mL syringe), 2. Luer adapter, 3. Air-jet DPI (D2 pictured), 4. Nasal interface, 5. Infant NT model, 6. Respiratory filter.
Drug mass characterization methods
After actuation and aerosolization, drug masses retained or collected in the air-jet DPI and NGI or nasal interface, NT model, and filter were recovered by dissolving in an appropriate volume of deionized water followed by HPLC analysis. The loaded drug mass was determined through content uniformity analysis of the AS-EEG formulation; where known masses of AS-EEG were dissolved in water and the AS content (μg/mg of formulation) was determined. AS quantification was performed for each deposition site and for the drug mass used to calculate the drug recovery. Drug recovery percentage was expressed as the amount of AS recovered on all deposition sites divided by the loaded AS dose for each experiment.
Based on an airflow rate of 45 LPM, the NGI stage cut-off diameters were determined by using the formula specified in USP 35 (Chapter 601, Apparatus 5). The MMAD was calculated through linear interpolation between appropriate stages by using a plot of cumulative percentage drug mass versus cut-off diameter.
Powder formulation characterization method
In preliminary experiments before device testing with the NGI and infant NT model, primary particle size of the AS-EEG powder formulation was determined by laser diffraction using the Sympatec HELOS (submicron R1 lens with 20 mm focal length) with RODOS/M disperser at 4 bar, and ASPIROS sample feeder set to 60 mm/s (Sympatec GmbH, Clausthal-Zellerfeld, Germany). Three consecutive samples were tested on the same day. Testing at a high pressure of 4 bar is intended to show maximum particle dispersion. This primary particle size then serves as a benchmark to evaluate the aerosolization efficiency of the air-jet DPI, which is operated with 1000 × to 10,000 × less pressure.
Statistical analysis
Statistical analyses for comparing aerosolization performance across all devices and comparison of device performance at different AAVs were performed by using JMP Pro 15 (SAS Institute, Inc., Cary, NC). Comparison of device performance utilized one-way ANOVA followed by post hoc Tukey. Comparisons of preterm versus full-term AAVs for each device were performed with the Student's t-test. All statistical tests used a significance limit of p = 0.05.
Results
Formulation characterization and air flow rate
The AS-EEG formulation was characterized as having a mean (SD) geometric diameter of 0.99 (0.0) μm. To compare laser diffraction primary particle size with the air-jet DPI performance, the geometric size (measured with laser diffraction) was converted to an aerodynamic diameter by using a theoretical solid particle density of 1.393 g/cm3 (based on weighted particle densities of the formulation components).(60) Figure 8a shows the mean cumulative aerodynamic diameter size distribution of the AS-EEG powder formulation, resulting in a mean MMAD of 1.17 μm. This size is expected to be near full dispersion based on the high pressure used with the laboratory scale dispersion unit.

Time-averaged air flow rates were determined for each device actuated by hand six times, with the mean (SD) results reported in Table 2 for an AAV of 30 mL. Figure 8b shows the pressure profile during actuation for D2, D5, and D6, which characterize pressure profiles for all devices tested. A fixed volume of 30 mL and the average total time for each device were used to calculate the time-averaged flow rate. D2 was found to have the lowest time-averaged flow rate of 1.9 LPM, whereas D5 and D6 had the highest of 2.7 LPM. In the same manner, the time-averaged flow rates for each device were calculated with an AAV of 10 mL, with the results provided in Table 3. There was no statistically significant change in average flow rate between the two AAVs, with the exception of D6, which was slightly, but significantly lower at 10 mL (t-test, p = 0.007). All devices have acceptable time-averaged flow rates within the target 1–5 LPM for infant aerosol delivery.
Aerosolization Performance and Measured Flow Rate with an Actuation Air-Volume of 30 mL
Mean values with SD shown in parentheses.
p < 0.05 significant effect of device design on each of the individual reported parameters (one-way ANOVA).
n = 6.
n = 3.
ED, emitted dose; LPM, liters per minute; MMAD, mass median aerodynamic diameter; SD, standard deviations.
Aerosolization Performance and Measured Flow Rate with an Actuation Air-Volume of 10 mL
Mean values with SD shown in parentheses.
p < 0.05 significant effect of device design on each of the individual reported parameters (one-way ANOVA).
n = 6.
n = 3.
Performance of air-jet DPIs
Aerosolization metrics in terms of ED and MMAD for full-term and preterm AAVs of 30 and 10 mL are presented in Tables 2 and 3, respectively. Surprisingly, all devices tested produced an aerosol MMAD below 2 μm at both AAVs. The ED values were also relatively high, with multiple devices emptying more than 85% of the loaded dose. The highest ED values were from designs D5 (94.1%) and D1 (88.1%) actuated with 30 mL of air. Choosing best device performance based only on aerosolization metrics is difficult, as increasing ED is often associated with increasing MMAD, which may have a net negative effect on aerosol delivery to the trachea and lungs. A potentially useful metric is MMAD/ED, where lower values are desirable and expected to improve aerosol delivery to the lungs. For both AAVs, the lowest three values of MMAD/ED were provided by designs D5, D6, and D2 (using full-term AAV conditions, the MMAD/ED values were 0.0198, 0.0200, and 0.0210, respectively). Examining Table 2 for the 30 mL AAV, it was observed that there were statistically significant differences among the different device designs for each of the aerosolization performance parameters. For the MMAD/ED metric, D4 design with the highest value MMAD/ED was observed to be significantly different to both designs D5 and D6, with the two lowest MMAD/ED values (post hoc Tukey: p = 0.003 and 0.006, respectively).
To assess overall DPI performance, it is useful to graph MMAD versus ED, as shown in Figure 9a and b for the two AAVs considered (30 and 10 mL, respectively). In these figures, at each AAV, two distinct sets of DPI performance are observed, which fall along linear best-fit lines of MMAD versus ED. If the linear performance curve formed by D1, D3, and D4 is considered as a reference, then improved performance is achieved by devices that fall in the space below and to the right of this line. As a result, devices D2, D5, and D6 are shown to have overall improved performance compared with D1, D3, and D4. Viewed another way, if an ED of 85% is set as a performance target, both D1 and D6 are acceptable, but D6 reduces the MMAD at the same ED by ∼0.1–0.3 μm. Fortunately, the group of D2, D5, and D6 performs better than the other designs at both AAVs. Comparing performance between AAVs of 30 and 10 mL, D5 shows an increase in MMAD variability, which is not present with D2 or D6.
Mean (SD) values of MMAD versus ED based on device actuation into the NGI and AAVs of
Figure 10 provides a comparison of the three best performing (based on ranking of MMAD/ED and linear best-fit lines seen in Fig. 9) DPI designs D2, D5, and D6 actuated at 30 and 10 mL. It is observed that reducing the AAV by a factor of threefold has little influence on device performance, based on similarity in the data points for each device along the best-fit curve. Table 4 reorganizes the data from Tables 2 and 3 to show a side-by-side comparison of the best performing devices operated at each AAV. Statistical analysis (t-test) was performed for each device comparing performance at the two AAVs. Although it can be seen that the lower AAV (10 mL) corresponds with a slightly but statistically significant lower ED, there was no statistical difference for MMAD or the MMAD/ED parameter. Based on results from Table 4 and similarity in the data plot locations (Fig. 10), it is observed that device D5 was least influenced by the three-fold reduction in AAV.

Mean (SD) values of MMAD versus ED based on device actuation into the NGI for the three best performing devices actuated with 30 mL (open circles) or 10 mL (filled circles) of room-condition air.
Comparison of Best Design Aerosolization Performance at 10 and 30 mL Actuation Air-Volumes
Mean values with SD shown in parentheses, n = 3.
p < 0.05 significant difference between 10 and 30 mL AAV (Student's t-test).
AAV, actuation air-volume.
N2L aerosol delivery
Best performing devices D2, D5, and D6 were connected to the gradually expanding nasal interface and tested for aerosol delivery through the full-term NT model at an AAV of 30 mL. Deposition fractions in each region of the delivery system and NT model are displayed in Figure 11. Considering drug mass retained in the device, connecting to the nasal interface and NT model moderately increased retention in device D2 to about 29%, whereas the drug retention for devices D5 and D6 slightly decreased to about 5% and 15%, respectively. All delivery systems lost ∼7%–10% in the gradually expanding nasal interface, which is significantly better than 30%–40% loss in preliminary rapidly expanding nasal interfaces. In the nose, highest deposition was seen in the MP and throat regions. Surprisingly, results showed that depositional losses in different regions tend to provide similar total values, leading to a narrow range of 48%–53% lung delivery efficiency. Reasons for similar lung delivery efficiencies across the three devices tested can be further explored in Figure 11b and Table 5. These results present aerosol deposition (or retention) fractions grouped for each device and subdivided for the nasal interface, complete NT regions, and tracheal filter (lung delivery). Despite statistically significant differences between designs in all deposition regions leading up to the tracheal filter, there was no significant difference in filter deposition (lung delivery). Interestingly, it is observed that the D2 device generating the smallest aerosol (1.55 μm) produced only 8.0% NT depositional loss, whereas increasing aerosol size to 1.85 μm with D5 dramatically increased nasal depositional loss to 36.1%. With D2, the low nasal depositional loss is offset by ∼29% device retention, resulting in a tracheal filter deposition fraction of 52.2%. Device D5 reduced DPI retention to about only 5%, but it then dramatically increased NT deposition leading to a similar 48.5% lung delivery efficiency. Average total AS recovery percentages for the best performing designs were between 95% and 98%, ensuring mass balance and validity of the experiments.
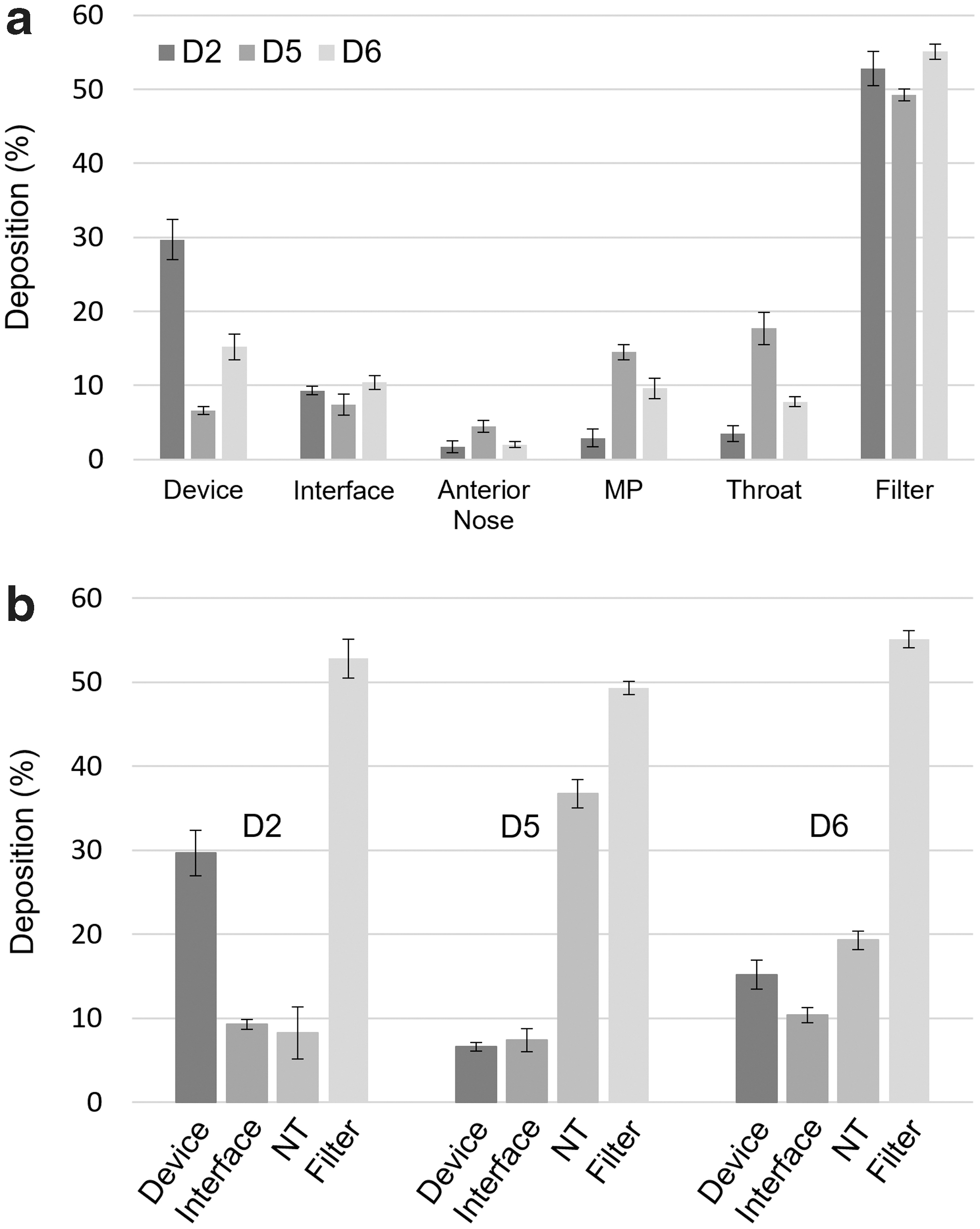
Experimentally determined mean (SD) drug deposition fraction (based on loaded dose) grouped by
Regional Deposition Fractions (Based on Loaded Dose) for Air-Jet Dry Powder Inhaler Designs in Full-Term Nose-Throat Model and 30 mL Actuation Air-Volume
Mean values with SD shown in parentheses, n = 3.
Total extrathoracic is the sum of anterior nose, middle passage, and throat deposition.
p < 0.05 significant effect of device design on deposition (one-way ANOVA).
Discussion
A primary outcome of this study was the development of new infant air-jet DPI prototypes that achieved the performance metrics of >80% ED, MMAD <1.8 μm, and a lung delivery efficiency of ∼50% of device-loaded dose. In assessing the air-jet DPI designs, two distinct sets of devices were identified based on aerosolization performance. Designs D2, D5, and D6 were found to produce a superior combination of MMAD and ED (based on MMAD/ED and linear best-fit lines) than the remaining three devices. Common design features of the three best performing air-jet designs were a cylindrical and horizontal aerosolization chamber together with a flush or protruding outlet. Designs that also included multiple inlets (D5 and D6) achieved the best aerosolization metrics of approximately >80% ED and MMAD <1.8 μm, whereas D2 with a single air inlet did not. Nevertheless, when tested in conjunction with a gradually expanding nasal interface design and infant NT model, all three lead designs achieved ∼50% drug delivery to the lungs, which compared with a previous positive pressure infant DPI(39) evaluated in a 9-month-old infant model represents more than a 12-fold improvement.
Several previous studies have considered air-jet DPIs operated with an AAV of 10 mL.(41–45) These studies have typically focused on single inlet aerosolization chamber designs with inlets and outlets protruding at least 2 mm as well as loading drug with a capsule. Best case performance with those previous devices has typically been an ED of about 85% and MMAD in the range of 1.7–1.8 μm for a 10 mg powder fill mass. One exception is the previous study of Boc et al.,(61) in which multiple air inlets were employed with a much smaller aerosolization chamber volume. In the current study, D6 performance was the most consistent with previous devices. In comparison, the D5 design appears to perform better than previous devices with an ED of 94% and small aerosol size increase to 1.85 μm. As a result, this study indicates that air-jet performance was enhanced through the development of an aerosolization chamber with multiple inlets and a flush or protruding outlet.
Despite significant variation in the best performing devices (D2, D5, and D6 with an ED range of 75.6%–94.1%), in vitro lung delivery efficiency was consistently around 50% when using the full-term NT geometry. As described, the D2 design provided excellent NT penetration with only 8.0% depositional loss, but relatively poor emptying with ED of 75.6% (71.6% when connected to the infant NT model). Increasing the device emptying also increased the MMAD, which led to a significant depositional loss in the NT model. An ideal device for infant N2L aerosol delivery, therefore, appears to be one that can achieve an MMAD of 1.6 μm and ED near 95%. However, as illustrated by persistent occurrence of aerosolization performance data points on a straight line of MMAD versus ED, it is expected that new device design ideas will be required to achieve this level of performance.
Intended uses of the infant air-jet DPI include the rapid administration of high-dose inhaled medications such as aerosolized antibiotics and surfactants. For either of these applications, total doses higher than the 10 mg loaded dose employed in this study will likely be needed. The aerosolization chamber in this study has a total volume of 0.68 mL, which if approximately half full can accommodate 40–50 mg of powder based on typical EEG powder density. However, Longest et al.(41,62) have previously found that forming the aerosol too quickly within the air-jet device increases measured MMAD. Further testing is, therefore, needed to determine which devices can best accommodate higher dose loading without affecting performance. An alternative to accommodate higher total dose loading may be an auto-loading system for the air-jet DPI such that each actuation delivers a 10 mg dose of powder formulation.
As demonstrated in this initial study, the infant air-jet DPI is expected to provide a number of advantages for aerosol delivery to infants of all ages. First, device actuations of 10 and 30 mL require time periods between 0.2 and 1.0 seconds. The devices tested performed very similar at both AAVs in terms of aerosolization performance. Therefore, the only reason to implement the higher AAV for the older full-term infant is to provide a full inhalation breath. This air volume can be reduced to accommodate stiff or noncompliant lungs as needed. Further device testing will be required to reduce the AAV below 10 mL, as with 3 mL used in the previous study of Boc et al.(61) By operating the delivery system with positive pressure, it is expected that the highly flexible infant upper airways will be expanded, enabling better deep lung penetration of the aerosol. In this study, an enforced breath hold of 10 seconds was implemented; however, this length of time is not needed for aerosol retention, as EEG aerosols approach their fully hydrated droplet size within ∼0.5 to 1 seconds under infant airway conditions.(26) Nevertheless, under resuscitation conditions, te Pas and Walther(63) demonstrated that infant lung inflation followed by a 10 second breath hold improved lung mechanics and patient outcomes compared with standard rapid ventilation with a bag and mask. With a single-prong design, infant exhalation can be accomplished by releasing the nostril without the nasal interface. For a dual-prong design, an exhalation port will be included in the nasal interface close to the patient. Ideally, opening of the exhalation port can be automated with a single button on the device that also controls actuation of the air source.
The in vitro NT model employed in this study has several differences from in vivo conditions that should be considered. As previously described, the air-jet DPI delivers both the aerosol and a full inhalation breath such that cyclic breathing of the model is not required. However, more realistic airway delivery conditions need to include the downstream resistance and compliance of the lungs. The effect of this resistance and compliance on aerosol generation is expected to be small considering the relatively low ventilation volumes (7–8 mL/kg) that are employed. Further, the airway walls were not warmed and humidified to physiologic conditions. It is know that some size increase of hygroscopic aerosols occurs in the nose.(64,65) However, this aerosol size increase in the extrathoracic region was previously reported to be small with an associated negligible increase in NT deposition (<5% relative difference) for adult airway conditions.(66) As previously described, the air-jet DPI forms a closed system with the airways such that subject exhalation into the aerosolization chamber containing the powder is not possible.
Additional study limitations include the use of a hand-operated air syringe as an air source, consideration of a limited number of designs, use of one nasal interface design, and delivery testing through a single NT airway model. Variations in airflow delivery associated with hand-operation of the gas source are observed in Figure 8b. However, despite these variations, performance of the air-jet DPI was relatively consistent with acceptable standard deviation (SD) values. However, it is expected that operation of the hand syringe will vary significantly across different operators. Therefore, a consistent push-button operated air source is needed for future device actuation. Considering all possible design choices provided by the air-jet DPI, the six designs explored in this study form a relatively small set of options. Still, a set of improved designs with unique features were identified. The nasal interface is an important source of potential aerosol loss and also influences loss in the NT model. The single gradual expansion nasal interface used in this study was the result of preliminary design work that improved on nasal interface losses as high as 40% of the loaded dose. Although 10% nasal interface depositional loss is acceptable, it is expected that this deposition can be further reduced. Finally, this preliminary study considered only one NT model under full-term neonate conditions. Aerosol deposition in the NT region is known to be highly variable and where the tested model falls within this spectrum is currently not known. Future studies with additional aerosol delivery system optimizations will consider NT models based on even younger subjects with smaller AAVs (e.g., 6–9 mL).
In conclusion, this study has developed an air-jet aerosol delivery system to administer high doses of spray-dried powder formulations to infants. The patient interface is a simple gradually expanding flow passage that produced low depositional loss, and device actuation times are in a range between 0.2 and 1.0 seconds. Delivery efficiency of drug to the lungs was ∼50% of the loaded dose across the three best performing devices. Advantageous design options in the air-jet DPI were identified as a horizontal and cylindrical aerosolization chamber, flush or protruding outlet, and multiple inlets. With continuing advances in device improvement, delivery will be tested and optimized in even younger airway models across multiple subjects with smaller administered volumes of air.
Footnotes
Acknowledgments
The authors would like to thank Dale Farkas (VCU Engineering) for assistance and training with positive pressure DPI development and testing. Karl Bass and Sarah Strickler (VCU Engineering) are gratefully acknowledged for help with development of the infant nasal model.
Author Disclosure Statement
Virginia Commonwealth University is currently pursuing patent protection of devices and methods described in this study, which, if licensed and commercialized, may provide a future financial interest to the authors.
Funding Information
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under award number R01HD087339 and by the National Heart, Lung and Blood Institute of the National Institutes of Health under award number R01HL139673. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Reviewed by:
Ariel Berlinski
Israel Amirav
James Fink