
Abstract
Background:
Noninvasive ventilation (NIV) has an additional important effect that does not occur with medicinal therapy: a reduction in the work of breathing. Understanding the mechanical effects of these therapies is of considerable importance and can affect clinical decision making.
Objective:
Evaluate the effects of NIV compared to albuterol on lung function and respiratory mechanics in asthmatic adolescents and young adults after bronchoprovocation and determine the effects of a hypertonic saline solution on lung function respiratory mechanics.
Methods:
A randomized crossover study was conducted involving individuals with a diagnosis of asthma. Evaluations were performed with optoelectronic plethysmography (OEP) and spirometry at baseline, after the bronchial provocation test with 4.5% saline solution and after the intervention. The order of the procedures (bilevel NIV and albuterol) was randomized, with the participants crossing over to the other treatment after a 1-week washout period. Inspiratory positive airway pressure (IPAP) 12 and expiratory positive airway pressure (EPAP) 8 cmH2O were set for 10 minutes and the dose of albuterol was 400 μg.
Results:
Forty individuals were included in the study (mean age: 21.6 ± 4 years; 24 females). The recovery of FEV1% was 87.9% (80.8 ± 35 to 101.1 ± 46.1, p < 0.05) after NIV and 95.9% (84.4 ± 42.4 to 110.3 ± 44.3, p < 0.05) after albuterol. Inspiratory capacity (IC; L) reduced 12% to 15% after bronchoprovocation, with 100% recovery using NIV (2.1 ± 0.7 to 2.42.4 ± 0.6, p < 0.05) and 107.6% using albuterol (2.2 ± 0.8 to 2.8 ± 1.1, p < 0.05). Regarding OEP variables, tidal volume had greater participation in the thoracic compartment. NIV led to an increase in minute volume and a return to the baseline value, which did not occur with albuterol.
Conclusion:
NIV recovered FEV1 and improves signs of hyperinflation by improving IC. Bronchoprovocation with a hypertonic solution reduced FEV1 by 20% and reduced IC. NIV led to a faster recovery of minute volume and reduced the contraction velocity of the muscles of the rib cage compared to albuterol, although the effects on lung function were less intense.
Introduction
Asthma is a chronic inflammatory disease characterized by recurring, reversible episodes of airway obstruction. Medicinal treatment normally involves inhaled corticoids and bronchodilators.(1) These acute episodes of bronchoconstriction often progress to hyperinflation. Martin et al.(2) related hyperinflation and the consequent increase in functional residual capacity to the activation of the inspiratory muscles in the expiratory phase before the establishment of the elastic equilibrium of the lungs and rib cage, leading to impaired respiratory mechanics.
The negative impact on respiratory function caused by acute hyperinflation occurs due to the reduction in the contribution of the abdominal compartment and an increase in the contribution of the thoracic compartment, with a consequent reduction in the mechanical efficiency of the diaphragm due to the reduction in its zone of apposition. Due to this mechanical disadvantage and “reduction in the curvature” of the diaphragm, the expiratory muscles are activated in an attempt to restore the original mechanics and their primary function.(3)
Studies have demonstrated the effects of bronchoconstriction on the recruitment of respiratory muscles and respiratory mechanics in asthmatic individuals.(2,4,5) As asthma has distinct characteristics between the stable phase and an exacerbation, bronchoprovocation tests have been used to enable evaluations under different physiological conditions, similar to an episode of exacerbation without necessarily causing an asthma attack and respiratory insufficiency, which would considerably hinder the kinematic evaluation of the thoracic and abdominal compartments in each of these phases during a treatment protocol. Respiratory dynamics are complex and involve, in addition to the neural control, the kinematics of the thoracic and abdominal compartments. The movement pattern of these compartments is associated with the efficiency of breathing that must occur to meet the demands with the lowest possible energy expenditure and situations in which there is an increase in the resistive component such as in asthma.(6,7)
The interest in nonpharmacological therapies and knowledge regarding the action of the modalities often employed to alleviate the excessive load on the respiratory muscles in obstructive conditions have shown, since the 1980s,(4) that positive expiratory pressure reduces muscle work and diminishes the expiratory reserve volume, thereby contributing to pulmonary deflation. According to the most recent European consensus, noninvasive ventilation (NIV) has a B grade of evidence for the treatment of an asthma attack.(8) Thus, there is a need for more in-depth evaluations of the mechanical effects of this therapeutic modality in cases of instability of the disease.
Another issue raised regarding pharmacological rescue treatment is that ∼34% of patients with asthma have a low bronchodilation response to β2 agonists,(9,10) which justifies the combination of therapies with a better response.
As bilevel NIV promotes a level of inspiratory pressure that increases ventilation and expiratory pressure that stimulates the stretching of pulmonary receptors, this technique may have a bronchodilating effect. Therefore, the hypothesis tested in this study seeks to answer the following questions: Does bilevel NIV promote bronchodilation and increase FEV1? What are the effects of NIV and a bronchodilator on respiratory mechanics? What are the effects of bronchoprovocation on respiratory mechanics?
There are studies(9,11) in the literature that show the bronchodilator effect of NIV and resolving or mitigating bronchospasm is the main goal during an asthma attack, but no less important is knowing how the mechanical behavior of these therapies is, and quantifying this bronchodilation is still a gap in the literature and this information will help in the best therapeutic choice that possibly can be the combination these therapies even in less severe crises.
The aim of this study was to evaluate the thoracoabdominal mechanics and lung function in asthmatic adolescents and young adults submitted to a bronchoprovocation test and in response to pharmacological (β2 agonist bronchodilator) and nonpharmacological (bilevel NIV) therapy.
Materials and Methods
Type of study
A randomized crossover clinical trial was conducted to evaluate the thoracoabdominal configuration before and after bronchoprovocation, as well as after the use of a bronchodilator (albuterol) and NIV with two pressure levels performed on two different occasions in asthmatic adolescents and young adults. The order of the treatments was randomized and allocation was concealed. Blinding was partial. Only the analysis of the data was performed by a blinded evaluator, as the therapies did not enable the blinding of either the therapist or participants.
Ethical aspects
This study was developed in accordance with the norms governing research involving human subjects stipulated in Resolution 466/2012 of the Brazilian National Board of Health, received approval from the Human Research Ethics Committee of Nove de Julho University (Certificate No. 2.130.007/2017) and was registered with clincaltrials.gov (NCT03430505).
Study setting and sample
This study was developed at the Multidisciplinary Movement Lab (Optoelectronic Plethysmography Module) and Respiratory Functional Evaluation Lab—both located on the Latin America Memorial Campus of Nove de Julho University in São Paulo, Brazil.
Inclusion criteria
Male and female individuals between 12 and 29 years of age with a diagnosis of asthma and under regular medical follow-up were included in the study. Adult participants and the legal guardians of underage participants signed a statement of informed consent. Participants younger than 18 years also signed a consent form.
Exclusion criteria
Individuals in a state of exacerbation of the disease, those who used a bronchodilator less than 12 hours before the test, those unable to understand the tests, those with an intolerance to a bronchodilator, those with no prescription for a bronchodilator, and those with heart disease or an infectious disease were excluded from the study.
Evaluation and intervention
The evaluation and intervention lasted 1 hour and 10 minutes and consisted of the following: anthropometric evaluation, lung function tests, bronchoprovocation, the administration of a clinical control questionnaire, and the determination of thoracic and abdominal kinematics. The order of treatment (NIV and bronchodilator) was randomized using opaque envelopes. The participant chose an envelope at random, which stipulated the first therapy to be executed during Visit 1 and he/she automatically underwent the other therapy during Visit 2 after a 1-week washout period.
NIV was performed with the BIPAP Respironics device, with inspiratory positive airway pressure (IPAP) of 12 cmH2O and expiratory positive airway pressure (EPAP) of 8 cmH2O for 10 minutes using a face mask. The bronchodilation treatment consisted of four puffs of albuterol, totaling a dose of 400 μm administered using a spacer (Agachamber™/GSK). The evaluation was performed 10 minutes after the administration of albuterol to ensure the same length of time in both treatments (Figs. 1 and 2).
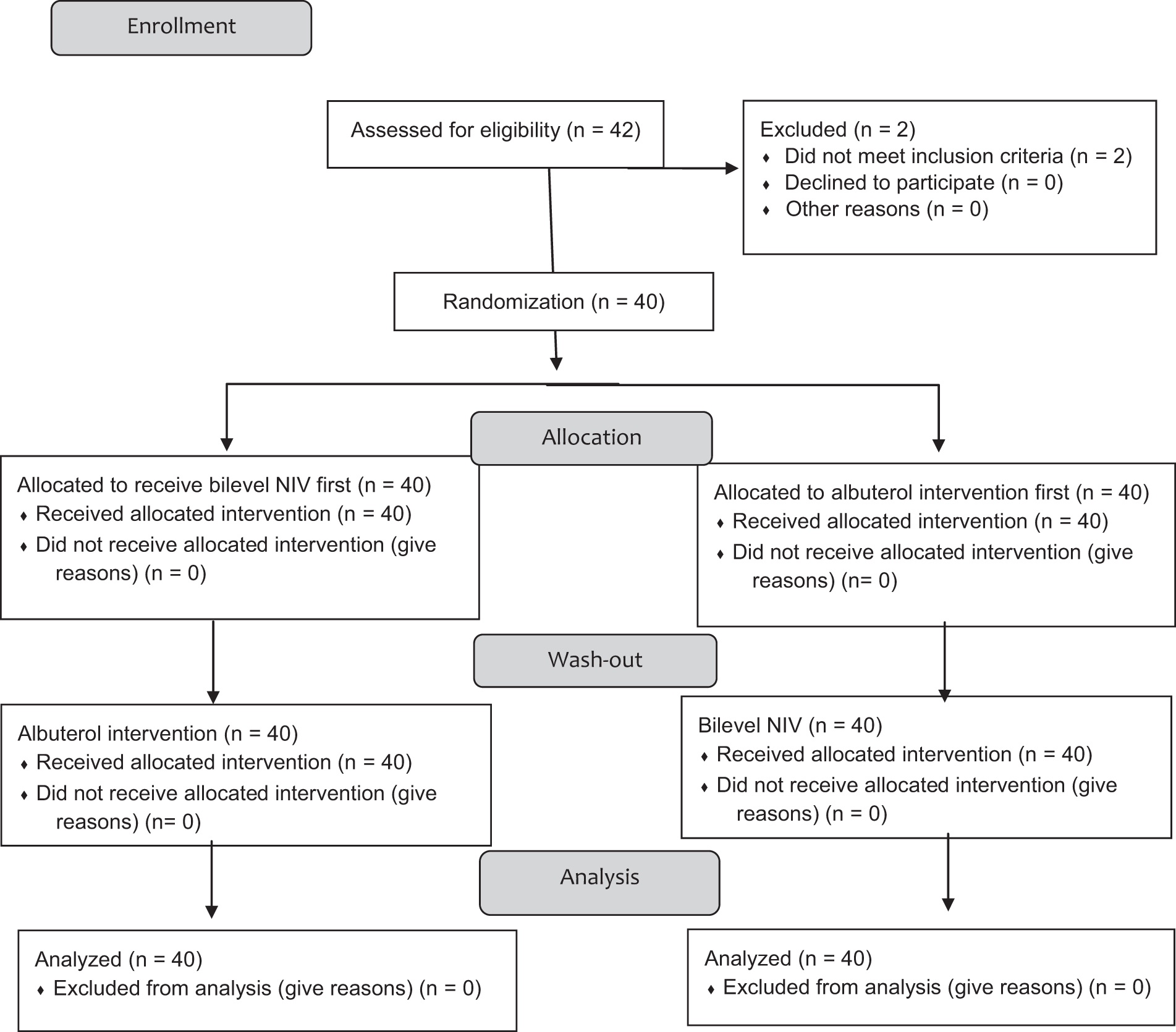
Consort flowchart.
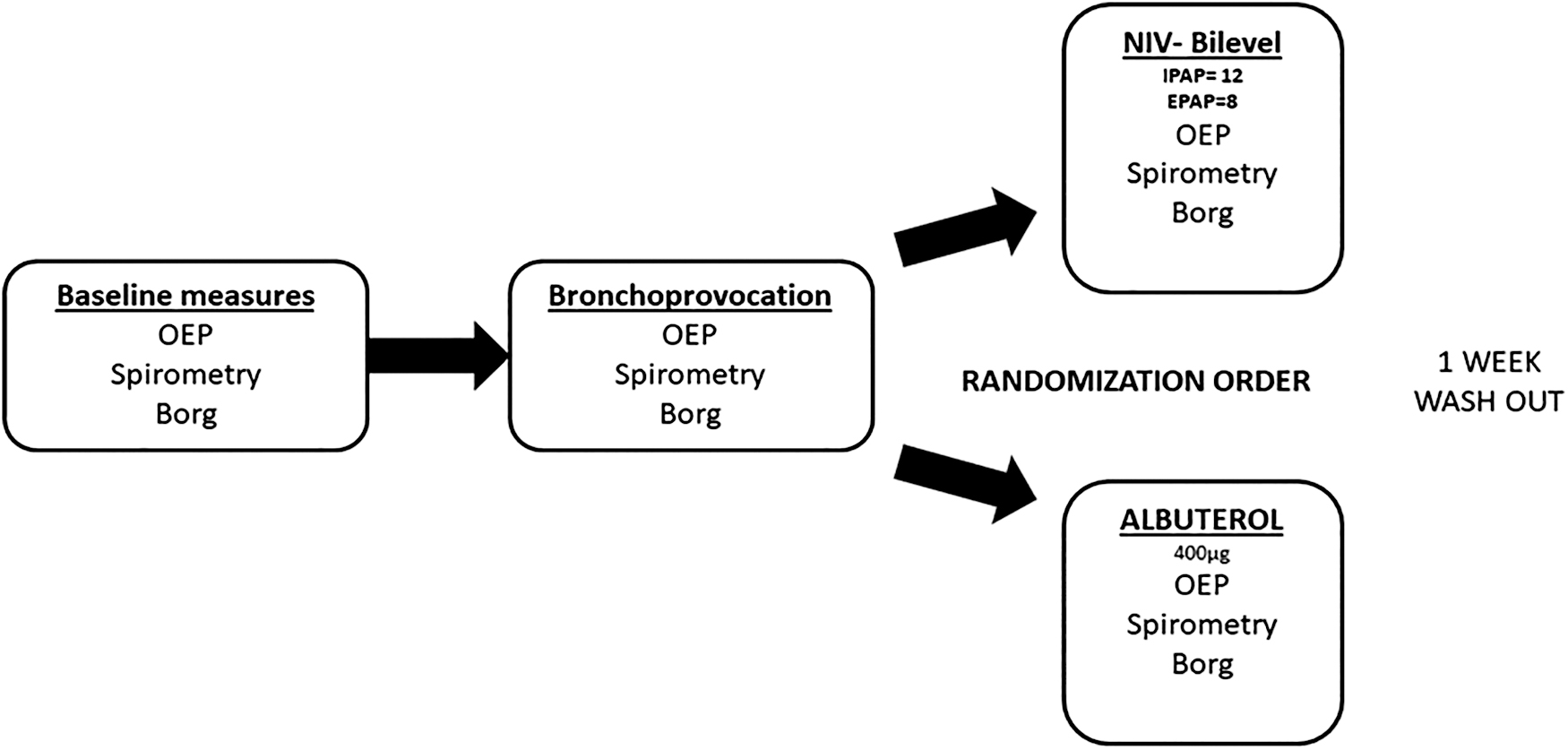
Timeline of experimental procedures.
Evaluation of thoracoabdominal movement
Data collection was performed using an optoelectronic plethysmography (OEP; BTS, Italy) equipped with eight cameras (four positioned in front and four positioned behind the participant). Thoracoabdominal movements were captured with the aid of 89 reflective markers attached to the thorax of the participant. The movements were transmitted in real time at 60 frames a minute synchronized with axial diodes that emitted infrared light, which was reflected by the markers to the OEP system. The signals were instantly recorded by the OEP Capture software and analyzed using the Smart Analyzer, which transformed the data into three-dimensional (3D) geometric information and calculated data regarding pulmonary mechanics and thoracoabdominal kinematics.(12)
The cameras were adjusted and calibrated to ensure the accuracy of the 3D reconstruction. The reflective markers were attached with double-sided adhesive tape to the thorax of the participants who remained seated on a bench with no back support in a position previously determined by the model found in the software of the equipment. The placement of the markers on lines was orientated by anatomic structures (suprasternal notch and clavicles to the level of the anteroposterior crest), with 42 anterior markers, 37 posterior markers, and 10 lateral markers (total: 89 markers) (Fig. 3).

Anterior and posterior views of marker placement.
During the readings, the participant was instructed to remain seated, with hips and knees flexed at 90°, feet supported on floor, and arms supported on waist in such a way as to not affect the capture of any of the markers by the cameras. The participant was instructed to breath normally to capture the thoracic and abdominal movements for 50 seconds (mean of 20 respiratory cycles per reading). After the reading, the three most homogeneous and technically adequate (size and height) cycles were selected for analysis. This procedure was performed with the volunteer in spontaneous breathing prebronchoprovocation, postbronchoprovocation, during NIV, after NIV (during the NIV portion of study), and after the use of the bronchodilator (during the albuterol portion of the study).
The following were the OEP variables: minute volume, tidal volume (TV), inspiratory time (Ti), expiratory time (Te), total cycle time (Ttot), thoracic TV, % TV thoracic TV, intermediate compartment TV and %TV intermediate compartment, and TV abdomen and %TV abdomen; variations in abdomen volume (VAb) and pulmonary rib cage (RCp) divided by Ti were used as contraction velocity indices of the diaphragm (VAb/Ti) and rib cage (VRCp/Ti), respectively; variations in abdomen volume divided by the expiratory time (VAb/Te) were used as the contraction velocity index of the abdominal expiratory muscles, as described elsewhere.(8) We also evaluated the end-expiratory and end-inspiratory lung volumes (EELV and EILV) and respective variations per thoracoabdominal compartments.(12)
The markers enabled capturing the rib cage movements by the cameras and determining the movements in the different compartments with the aid of the Smart Capture software. For this study, three compartments were considered: pulmonary rib cage, thoracoabdominal cage, and abdomen. As the respiratory movements were performed, the markers enabled the generation of reports per compartment through derivations and 3D geometric compositions.
Bronchoprovocation test and Borg scale
The bronchoprovocation test was performed following the protocol established by Anderson,(13,14) based on the hyperosmolarity of the airway, which leads to a reduction in its diameter. The protocol consisted of inhaling a 4.5% hypertonic solution through an ultrasonic nebulizer (Pulmosonic™/Soniclear-2,4Mhz) for 30 seconds. Forced expiratory volume in the first second (FEV1) was measured before and after first exposure. If the reduction was 10% to 15%, the same time was repeated. If no reduction occurred, the participant inhaled the solution for 1 minute and the procedure was repeated (30 seconds and 1, 2, 4, and 8 minutes). Maximum exposure was 8 minutes.(13–15) Perceived shortness of breath was measured using the Borg scale before and after bronchoprovocation, as well as after treatment.
Lung function test
The lung function test was performed using spirometry. The following volumes, capacities, and flows were determined: forced vital capacity (FVC), FEV1, FEV1/FVC ratio, slow vital capacity, inspiratory reserve volume, expiratory reserve volume, and inspiratory capacity (IC).
Asthma Control Questionnaire
The Asthma Control Questionnaire (ACQ6) is used to evaluate the clinical control of asthma and is composed of six questions: five addressing the symptoms of asthma and one on the use of a short-lasting β2 agonist as a rescue medication. The score is the mean of the six items and ranges from 0 (completely controlled) to 6 (uncontrolled) using a 7-day period as reference. The cutoff point for controlled/uncontrolled asthma is 1.5 points. In this study, the participants were classified as having controlled asthma (<0.75), partially controlled (0.75–1.5), or uncontrolled (>1.5).(16,17)
Sample calculation and statistical treatment
The sample size was calculated based on the results of a pilot study involving 10 individuals who underwent both treatments. For the outcome FEV1 (% of recovery), considering 90% recovery with albuterol and 70% recovery with NIV with a standard deviation of 15%, a total of 18 patients would be needed. For the outcome of IC, considering 100% for albuterol and 80% for NIV with a standard deviation of 15%, a total of 35 patients would be needed. Considering an 80% power and a significance level of 0.05, 40 patients were included.
The Shapiro–Wilk test was used to determine the normality of the data. Comparisons between groups were performed using either the unpaired t-test or the Mann–Whitney test. Analysis of variance (ANOVA) was used with Tukey's post hoc test for the intragroup analyses of the OEP data. The statistical analysis was performed using the Minitab 14, with the level of significance set to 5% (p < 0.05).
Results
Forty patients were treated with each therapy. The sample was composed of adolescents and young adults in the ideal range for body mass index. The female sex accounted for 65% of the sample. The characteristics of the participants are displayed in Table 1.
Characteristics of Sample
p < 0.05 intergroup; †‡p < 0.05 intragroup.
ACQ6, Asthma Control Questionnaire; ERV, expiratory reserve volume; F, female; FEV1, forced expiratory volume in first second; FVC, forced vital capacity; HSI, hypertonic saline inhalation; IC, inspiratory capacity; IRV, inspiratory reserve volume; M, male; NIV, noninvasive ventilation; SVC, slow vital capacity.
Regarding the results of the ACQ6, asthma in the sample was partially controlled,, The severity of the patients was mild to moderate persistent.(18) Mean exposure time to the inhaled hypertonic saline solution was 2.6 ± 1.6 minutes in the NIV group and 2.3 ± 1.3 minutes in the albuterol group.
Lung function variables
The mean reduction in FEV1 following bronchoprovocation with the saline solution was 20% in both groups. The recovery rates following treatment were 87.9% in the bilevel NIV group and 95.9% in the albuterol group. IC was reduced due to pulmonary hyperinflation, with a reduction of 15% to 20% in both groups and both treatments restored IC to baseline levels.
Shortness of breath (Borg scale)
An increase in shortness of breath occurred after bronchoprovocation. Both treatments improved this variable, with no statistically significant difference between NIV and albuterol (Table 1).
Optoelectronic plethysmography
Tables 2 and 3 displays the OEP data. Bronchoprovocation led to an increase in minute volume in both groups. This variable increased even more during bilevel NIV, followed by a return to the baseline level. Minute volume did not return to baseline values in the bronchodilator group in the same time period (10 minutes after administering albuterol) (p < 0.05).
Optoelectronic Plethysmography (OEP) Data
p < 0.05 baseline × intragroup; †p < 0.05 after HSI × intragroup; ††p < 0.05 in treatment × intragroup; ‡p < 0.05 post-treatment × intragroup; **p < 0.05 intergroup comparison.
Min Vol, minute volume; RR, respiratory rate; Ti/Ttot, inspiratory time and total cycle time index; TV, tidal volume total; TVabd, tidal volume made by the abdominal compartment ; TVin, tidal volume made by the intermediate compartment; TVth, tidal volume made by the thoracic compartment; VAb/Te, variations in abdomen volume divided by the expiratory time; VRcp, variation in pulmonary rib cage volume.
Optoelectronic Plethysmography (OEP) End-Inspiratory Volume and End-Expiratory Volume Data
p < 0.05 intragroup baseline × after HSI; †p < 0.05 intragroup after HSI × treatment; ‡p < 0.05 between groups treatment; ΔI − E, difference between inspiration and expiration of each compartment evaluated.
abd, abdominal; arc, abdominal rib cage; cw, chest wall; EEV, end-expiratory volume; EIV, end-inspiratory volume; RCp, pulmonary rib cage.
There was a predominance of the thoracic compartment over the other compartments, with no significant difference or change after the two therapies. An increase in the contraction velocity of the muscles of the rib cage occurred with bronchoprovocation and bilevel NIV. After bilevel NIV, the contraction velocity returned nearly to the baseline level. The same did not occur with albuterol (Fig. 4).

Contraction velocity index of muscles of rib cage: bilevel NIV × albuterol (**p < 0.05 intragroup; *intergroup). NIV, noninvasive ventilation.
A significant difference between groups was found regarding the contraction velocity of the muscles of the rib cage (VRCp/Ti) (p < 0.05). Bilevel NIV restored this variable to baseline levels. An increase was also found regarding the contraction velocity of the diaphragm, with no significant difference between therapies and a return to baseline values after both treatments (Table 2).
Regarding EILV and EELV, there was a predominance in the thoracic compartment. EILV tended to increase and EELV tended to decrease with bronchoprovocation, but no statistically significant differences were found in either the intragroup or intergroup comparisons (Table 3).
Discussion
Bilevel NIV was able to restore nearly 90% of FEV1 and 100% of IC following bronchoprovocation. To the best of our knowledge, this is the first study to evaluate the isolated effect of NIV on these variables. NIV proved to be better than medicinal therapy (albuterol as rescue drug) regarding the restoration of minute volume and the reduction in the contraction velocity of the muscles of the rib cage. No change in the respiratory pattern occurred with either therapy.
OEP has the great advantage that it can measure breathing patterns in any condition (e.g., rest, exercise, phonation, and sleep) where the chest wall can be visualized totally noninvasively. It is highly accurate in the measurement of total chest wall volume variations, allowing partitioning of the complex shape of the chest wall into different compartments. In addition to being noninvasive, it requires no connection to the patient. Furthermore, it can be used without a subject-specific calibration, because it provides a direct measurement of the volumes in a 3D reference frame and the calibration is not based on particular respiratory maneuvers requiring subject cooperation. All these features make the OEP not only a reliable system for basic physiological and pathophysiological studies but also an attractive tool for evaluating breathing under a wide variety of circumstances both in health and disease.(19)
In normal breathing at rest, for greater efficiency and less energy expenditure, there is a synergistic action between the primary motor muscles that act in a phasic way and breathing accessories that act in a tonic way to stabilize the costal fence. This synergistic action is observed by the movement of the thoracoabdominal compartments that must move in phase (together) upwards and outwards in the inspiratory phase and inwards and downwards in the expiratory phase. In conditions of increased demand, it is normal greater participation of the thoracic compartment generating greater expansion in the thoracic rib cage and an increase in minute volume and TV, due to a better muscle length and capacity to generate movements of the accessory breathing muscles.(6,7)
Inhaling a β2 agonist is the main form of therapy for an asthma attack/exacerbation.(20) However, ∼30% of patients do not have a satisfactory response to this treatment, which can lead to a worsening of the clinical condition. Another issue is sensitivity to the common side effects of the medication, such as tachycardia and tremors.(10) The response to a bronchodilator is determined by criteria of the American Thoracic Society/European Respiratory Society as indicative of a positive response,(20) such as a higher absolute FEV1 after using the bronchodilator compared to baseline. However, this is not the only criterion for determining whether an individual responds well to a bronchodilator, as the FEV1 varies on a daily basis and the increase in FEV1 may be smaller if the baseline value was already high. In such cases, the return to the baseline value after the use of a bronchodilator may also be considered a positive response.
NIV is widely used in different clinical situations, but its use for an asthma attack remains unclear. The 2017 consensus of the ERS/ATS(8) expresses uncertainty regarding the recommendation of NIV for acute asthma. Although studies have offered physiological support for its indication,(2) few clinical trials have been conducted with this group of patients. These results confirm the physiological benefits of NIV for asthmatic patients. The recommendation in the consensus was based on observational and retrospective studies. It should be stressed that we are not speaking about a severe asthma attack, but rather a mild to moderate attack, with the aim of complementing the therapy previously established by the consensus, not only for this type of patient but also in different situations of respiratory illnesses.
Among the clinical trials conducted to evaluate the effect of NIV on an asthma attack, Soma et al.(9) investigated the isolated effect of this therapy compared to standard treatment (three groups; two with bilevel NIV—high pressure and low pressure). The authors found a greater improvement in FEV1 in the high-pressure group, especially after 40 minutes. In 2013,(11) our research group evaluated the effect of CPAP in children undergoing an asthma attack and found an increase in peak flow after 20 minutes. In both studies, the attacks were mild to moderate. In 2010, Gupta et al.(21) investigated the effect of bilevel NIV combined with conventional therapy compared to conventional therapy alone for patients undergoing a severe asthma attack; improvements were found in both groups regarding FEV1 and the PaO2/FiO2 ratio, but the NIV group spent less time in intensive care, had a shorter hospital stay, and had less need for the use of a bronchodilator.
In this study, NIV led to the normalization of contraction velocity of the muscles of the rib cage and minute volume, proving to be better than the bronchodilator with regard to these variables. In the presence of bronchial obstruction, the inspiratory muscles need to work against increased load generating a new biomechanical arrangement and an asynchrony between the primary breathing muscles and the accessories. The accessory muscles come into play at rest or at a low level of effort and the forces of this muscle group, which in normal situations work in an additive way, start to work in a dispersive way. The result is an early elevation of the chest compartment, shorter muscle length, and limited relaxation. Reducing the speed of contraction, while not changing this biomechanical arrangement, becomes an advantage that can increase the fatigue threshold and prevent intubation and the need for invasive mechanical ventilation.(6,7)
In this study, hypertonic saline bronchoprovocation was able to generate a satisfactory response with approximately a 20% reduction in baseline FEV1, similar to previous studies.(22–28) The reduction in IC suggesting hyperinflation was also observed, as well as in the study by Taube et al.(28) that evaluated this response in chronic obstructive pulmonary disease (COPD) patients. The concentration used in the aforementioned studies was around 3%, and in our protocol, we used 4.5% as in the Anderson(13) study. With this, we obtained a satisfactory response to bronchial provocation with increased sensation of dyspnea and changes in respiratory mechanics, as well as the reversal of changes by the therapies employed.
We should address issues regarding the NIV application time and the pressures employed. A different response may have been obtained with a longer application time, such as that used in the study by Soma et al.,(9) in which the best response occurred after 40 minutes, and different pressure levels. Moreover, an important limitation of this study is the impossibility of extrapolating these effects to situations involving a severe asthma attack, as this type of evaluation was unviable. Thus, further studies are needed, especially with patients undergoing a severe asthma attack. In addition, it would be important to assess other pressure levels and application times.
Conclusion
These findings demonstrate that NIV has a bronchodilating effect and significantly reduces pulmonary hyperinflation by reducing the contraction velocity of the muscles of the rib cage and normalizing the minute volume. Bronchoprovocation with a hypertonic solution was able to reduce both FEV1 and IC. Moreover, there is a predominance of the thoracic compartment in the breathing of asthmatic patients, which is not altered and only amplified by the therapies employed.
Footnotes
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
No funding was received for this article.
Reviewed by:
Arzu Ari
James Fink