
Abstract
Background:
Obstructive patients may benefit from nasal high-flow (NHF) therapy, but the use of pressurized metered-dose inhalers (pMDIs) has not been evaluated in this situation.
Methods:
Using an adult circuit and medium-sized cannula, we have tested different NHF rates, pMDI positions, breathing patterns, spacers, and spacer orientation. First, we evaluated albuterol delivery at the nasal cannula outlet. The second set of experiments made use of a nasopharyngeal cast to estimate the mass of albuterol potentially reaching the lungs. Albuterol was caught on filters placed at the cannula outlet and downstream of the nasal cast, and albuterol was quantified by spectrophotometry.
Results:
The highest amounts of albuterol delivered at the cannula outlet were observed with a 30 L/min flow rate (vs. 45 and 60 L/min) and placing the device close to the nasal cannula (in comparison with a position on the dry side of the humidification chamber). The use of a spacer was associated with higher delivery. The highest albuterol delivery was observed placing the spacer close to the nasal cannula, oriented for aerosol delivery following the gas flow and a 30 L/min NHF rate. Using this optimal setting, activating the pMDI at the beginning of inspiration (compared to expiration) increased albuterol delivery downstream of the nasopharyngeal cast. Whether in a quiet- or distress-breathing pattern, our measurements showed an amount of albuterol potentially delivered to the lungs exceeding 10% of the actuated dose in optimal conditions.
Conclusions:
Albuterol delivery with pMDIs is feasible within NHF circuits. Drug delivery sufficient to induce bronchodilation can be achieved using a spacer placed just upstream of the nasal cannula, a low NHF rate, and activation of the pMDI at the beginning of inspiration. Further testing in a clinical setting is required, however.
Introduction
Oxygen therapy and inhaled bronchodilators are the cornerstone of therapy for acute exacerbation of chronic obstructive pulmonary disease (COPD)(1) and acute asthma.(2) Nasal high-flow (NHF) therapy may be considered as an alternative to low-flow devices for oxygen therapy among those patients.(3) NHF consists in delivering high flows of heated and humidified gas containing a set fraction of inspired oxygen, through nasal cannulas. This technology comes with several potential benefits and is associated with an improved comfort comparatively to other non-invasive oxygenation and ventilatory support interfaces.(4–8) It generates a low positive end-expiratory pressure(9–11) and induces a nasopharyngeal dead space washout, thus reducing carbon dioxide rebreathing and consequently work of breathing.(12–16) These effects, associated to the possibility to precisely control the fraction of inspired oxygen lead to consider NHF as an appealing modality for oxygen administration in patients suffering from COPD or asthma. Given the importance of inhaled bronchodilator therapy among those patients, the question about concomitant administration of therapeutic aerosols arises.
In vitro, in vivo, and clinical studies have examined the feasibility of connecting a nebulizer to an NHF circuit to deliver inhaled bronchodilators and provided encouraging results.(17–19) However, nebulization comes with some potential drawbacks, such as duration of drug administration, potential interference with gas humidity, temperature and fraction of inspired oxygen when using a jet nebulizer, and need of a specific equipment to connect the nebulizer to the NHF circuit.
The use of pressurized metered-dose inhalers (pMDIs) with or without a spacer represents an alternative not evaluated so far in conjunction with NHF. This alternative to nebulization is appealing as it showed efficacy to deliver bronchodilators during other invasive and noninvasive ventilatory support modalities.(20) Quick medication delivery, breath-synchronized delivery, and hygiene all represent potential advantages of using pMDIs when available to deliver medications within NHF circuits.
The aim of this study was to evaluate the optimal configuration to deliver aerosols in a NHF circuit using pMDIs, measuring the amount of drug emitted at the cannula outlet and downstream of a nasopharyngeal cast according to different pMDI positions, actuation patterns, gas flow rates, spacer use, and patients' breathing patterns.
Materials and Methods
Due to the lack of human participants in the study, IRB approval was waived.
NHF system and drug delivery
In this bench study, an Optiflow™ system was used (MR 850 humidifier with RT 202 adult breathing circuit, with a medium-sized nasal cannula, OPT 544, all by Fisher & Paykel Healthcare, Auckland, New Zealand). The system was set to deliver gas with a 66% fraction of inspired oxygen with 100% relative humidity at 31°C. The NHF circuit was placed as horizontal as possible.
For all experiments, the pMDI device (Albuterol; Mylan, Canonsburg, PA) was shaken, heated inside the palm of the hand, and primed before use, as recommended per manufacturers' specifications. A 30-second time lapse was observed in between each actuation. A new pMDI device was used every 20 experiments. Preliminary experiments were performed delivering four puffs (400 μg) of albuterol. Because albuterol concentrations delivered at the cannula outlet were sometimes below the quantification threshold in some experimental configurations, we thereafter always performed 10 puffs administering a total dose of 1000 μg of albuterol, both in first and second set of experiments.
Experimental conditions
We conducted two sets of experiments, each with its own specificities and a synthetic view is proposed in Figure 1. Different flow rates (30, 45, and 60 L/min) were evaluated. Two pMDI device positions in the circuit were tested. Experiments were carried out either with a simple connector (MDI adaptor; Hudson RCI, Durham, NC) to adapt the pMDI to the circuit, or with spacers, which have their own connection method and do not require an additional connector (Fig. 2 summarizes experimental setup). The different spacers used in the study were the following: ACE® Spacer (Smiths Medical, London, United Kingdom), CombiHaler® device (Protec'Som, Valognes, France), and retractable AeroChamber® Vent device (Trudell Medical International, London, Canada). To improve experimental efficiency, all the spacers were not tested in all conditions (see Figs. 1 and 2 for details).
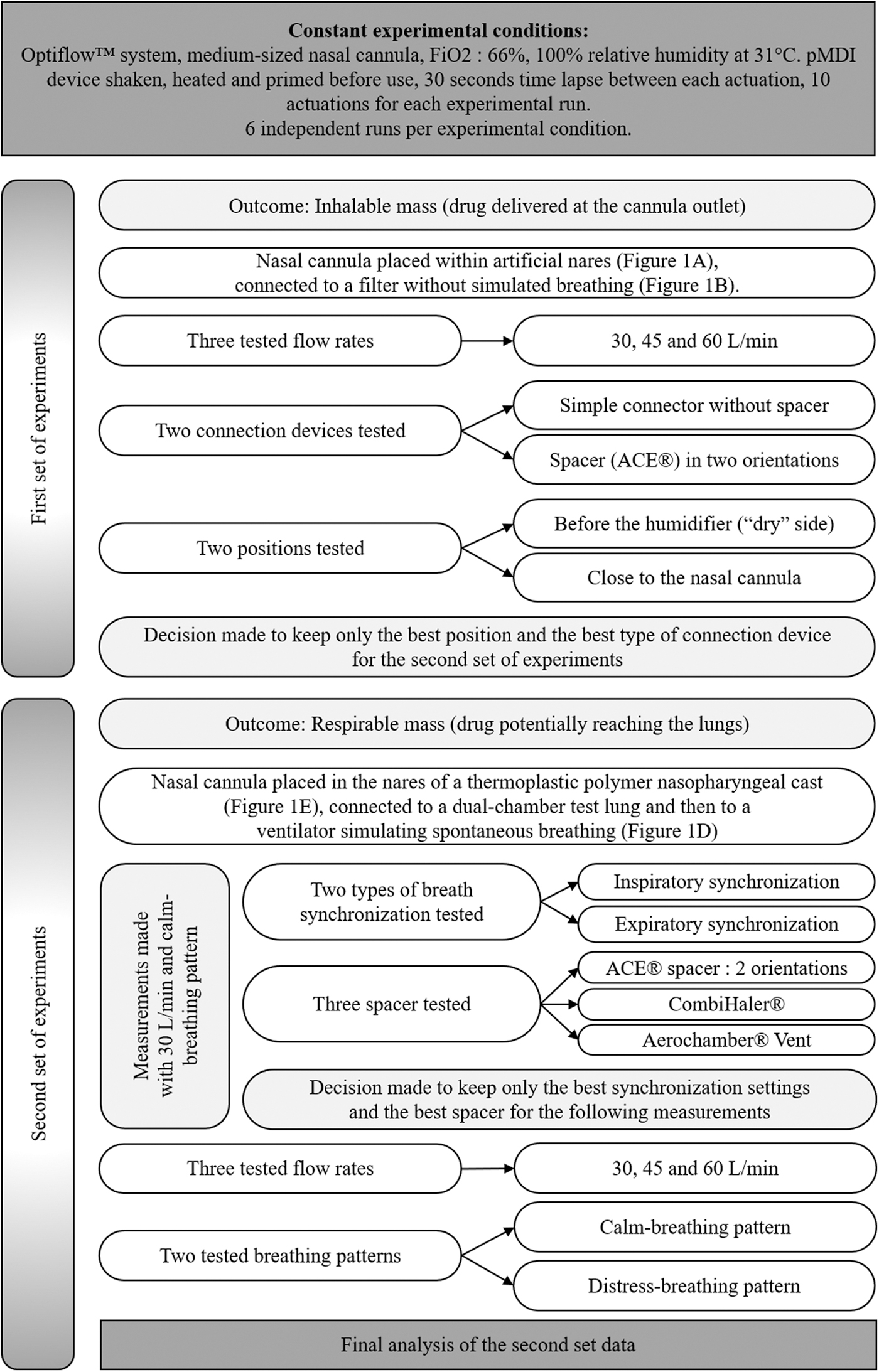
Synthetic view of the two sets of experiments and progressive analysis of data. pMDI, pressurized metered-dose inhaler.

Experimental setups. Adapted from 17 with permission.
In a first set of experiments, the nasal cannula was placed within artificial nares (Fig. 1A), as described previously,(17) to quantify delivery at the cannula outlet (inhalable mass) placing a filter immediately behind the cannula outlet (PARI GmbH, Starnberg, Germany). Cannula and artificial nares connection were air-tight and no simulated breathing was implemented downstream of the filter. Two different positions were tested: dry side of the humidification chamber and immediately upstream of the nasal cannula (Fig. 1B). In this experimental set, two devices were tested, in each position, for the connection of the pMDI to the circuit: the simple connector (i.e., without a spacer) and the ACE Spacer. The spacer was tested in two orientations (“with the flow” connecting the pMDI upstream of the spacer and delivering the aerosol in the same direction as the NHF gas flow and “against the flow” implementing the position recommended by the manufacturer, that is, placing the spacer the other way round, the pMDI placed downstream of the spacer, and delivering the aerosol against the NHF gas flow. Figure 1C depicts the different tested placements and spacer orientations. Three flow rates (30, 45, and 60 L/min) were evaluated. Six runs of every experiment were performed. The data were collected progressively and analyzed immediately after the end of all the measurements of this first experimental set. The best performing conditions (position, use of a spacer) were used for the second set of experiments to avoid multiplying experimental conditions excessively.
In the second set of experiments (Fig. 1D), the cannula was placed in the nares of a thermoplastic polymer nasopharyngeal cast (Fig. 1E), which enabled realistic simulation of drug deposition in the nasal cavities and upper airways, as well as the leakage between the cannula and the nares, allowing to estimate aerosol delivery to the lungs (respirable mass).(21) A filter (PARI GmbH) was tightly connected between the trachea of the nasopharyngeal cast model and a dual-chamber test lung (Michigan Instruments, Grand Rapids, MI) connected to a ventilator (Galileo, Hamilton Medical, Switzerland) simulating spontaneous breathing. To connect the pMDI to the circuit, the following different spacers were evaluated: the ACE Spacer device, which was tested in the first set of experiments, the CombiHaler device, and the retractable AeroChamber Vent device. The simple connector used in the first set was not tested in this second set. We simulated two adult sinusoidal breathing pattern: a quiet-breathing pattern, according to European norms for aerosol testing(22) (tidal volume = 500 mL, respiratory rate = 15 cycles per minute, inspiration to expiration ratio = 1:1 resulting in an average inspiratory flow of 15 L/min), and a respiratory distress-breathing pattern (tidal volume = 750 mL, respiratory rate = 30 cycles per minute, inspiration to expiration radio = 1:1 resulting in an average inspiratory flow of 45 L/min).(23,24) Inspiratory and expiratory synchronization was tested by delivering puffs, respectively, at the very beginning of inspiration and at the very beginning of expiration.
The data were collected and compared incrementally as shown in Figure 1. For reducing the multiplicity of measures, the device having shown the best results with a flow rate of 30 L/min and a calm-breathing pattern was the only one used to test different NHF rates and breathing patterns. In the same way, only the best breath synchronization time (i.e., inspiratory) was used after initial evaluation.
Albuterol quantification
After each experiment, the filter placed to recover the aerosol was rinsed with sodium hydroxide, and specific albuterol absorbance was measured in triplicate with a spectrophotometer (WPA Lightware II; Biochrom Ltd., Cambridge, United Kingdom) at 296 nm wavelength within 2 hours, as previously described.(17) The previously determined calibration equation of the spectrophotometer enabled to calculate the corresponding albuterol mass deposited on the filter, which was expressed as a percentage of the mass administered by the pMDI (1000 μg).
Results
Mass of drug delivered at the cannula outlet (inhalable mass)
Flow rate had an important influence on the amount of albuterol delivered at the cannula outlet. All other settings being equal, the highest values of albuterol delivery were observed with a flow rate set at 30 L/min, compared to 45 and 60 L/min (Table 1).
Amount of Drug Delivered at the Cannula Outlet (Inhalable Mass)
Data are indicated in micrograms (mean ± SD and inhalable mass %) of albuterol recovered on the filter. For all experiments, 1000 μg (10 puffs) of albuterol were delivered and each experiment was repeated six times independently. The ACE® Spacer was used when indicated, with two spacer orientations tested: “with the flow” connecting the pMDI upstream of the spacer and delivering the aerosol in the same direction as the NHF gas flow and “against the flow” implementing the position recommended by the manufacturer (Fig. 2).
NHF, nasal high flow; pMDI, pressurized metered-dose inhalers; SD, standard deviation.
Regardless of the chosen circuit condition (simple connector vs. spacer), the amount of albuterol deposited on the filter was always higher when the device was placed close to the nasal cannula compared to the dry side of the humidification chamber, in all tested conditions (Table 1). For example, when using a simple connector (without spacer) and a flow rate set at 30 L/min, the albuterol mass measured on filters was 3.4% and 2.0% of the emitted dose, respectively. Albuterol delivery was always higher when the spacer was used, regardless of its orientation. Albuterol delivery was highest when delivering the aerosol with the flow with NHF rates of 30 L/min (9.4% vs. 5.9% against the flow) and 60 L/min (4.8% vs. 4.0%); no difference was observed at 45 L/min (5.7% vs. 6.0%).
The highest delivery of albuterol observed with the simple connector was 3.4% (with a flow rate of 30 L/min); conversely the lowest delivery of all measures observed with the spacer was 4.0% (60 L/min, aerosol delivered against the flow). The highest albuterol delivery (9.4%) was observed with the spacer placed close to the nasal cannula with the pMDI delivering the aerosol “with the flow” and an NHF rate set at 30 L/min. All subsequent measurements were made with this optimal setting as defined a priori, that is, using a spacer placed just upstream of the nasal cannula.
Mass of aerosol potentially reaching the lungs (respirable mass)
Delivering the aerosol during expiration at 30 L/min simulating a quiet-breathing pattern with the different spacers resulted in very low respirable masses of albuterol (less than 0.5% of actuated dose whatever the condition). Implementing inspiratory synchronization, respirable masses observed were higher, but varied according to the type of spacer. The highest results were observed with the CombiHaler spacer (11.8%) and was significantly higher compared to the AeroChamber Vent (5.5%) and the ACE spacer in “with the flow” orientation (11.1%). According to those results, subsequent measurements were all performed with the CombiHaler placed close to the nasal cannula implementing inspiratory synchronization.
An increase of NHF rate resulted in a decrease of the respirable mass of albuterol, from 11.8% to 10.7% and 6.2%, at flow rates of 30, 45, and 60 L/min, respectively, simulating a quiet-breathing pattern (Table 2). The same was observed simulating a distress-breathing pattern. Of note, the respirable mass of albuterol at 30 L/min NHF was higher when simulating a distress-breathing pattern (mean patient inspiratory flow of 45 L/min) versus a quiet-breathing pattern (mean inspiratory flow of 15 L/min), which was not the case at 45 and 60 L/min NHF (Table 2).
Amount of Drug Potentially Reaching the Lungs, Deposited Downstream of the Nasopharyngeal Cast (Respirable Mass)
Data are indicated in micrograms (mean ± SD and inhalable mass %) of albuterol recovered on the filter. For all experiments, 1000 μg (10 puffs) of albuterol were delivered and each experiment was repeated six times independently. Quiet breathing pattern and respiratory distress pattern resulted in a patient simulated mean inspiratory flow of 15 and 45 L/min, respectively. Measurements were made with the CombiHaler® spacer directly connected to the circuit, without additional connector, placed just upstream of the nasal cannula, and the pMDI was activated at the beginning of inspiration.
The highest respirable mass was observed placing the CombiHaler immediately upstream of the nasal cannula, activating the pMDI at the beginning of inspiration and setting the NHF rate at 30 L/min. With those optimal settings, the respirable mass of albuterol was 11.8% and 16.8% of the actuated dose, for quiet-breathing and distress-breathing patterns, respectively (see Table 2 for the results of all conditions).
Discussion
The use of pMDIs is a novel approach for delivering bronchodilator medications to patients undergoing NHF, without interrupting oxygen flow. To optimize delivery, we tested different situations and observed that using a spacer placed just upstream from the nasal cannulas and using a low NHF rate is the best way to maximize the amount of drug potentially reaching the lungs. Overall, using pMDIs to deliver aerosols within an adult NHF circuit is technically feasible and gives clinically relevant results: when implementing optimal practice, 11% to 16% of the mass of aerosol emitted by the pMDI is likely to reach the lung (respirable mass). Thus, when using a standard pMDI administration consisting in 4 actuations of 100 μg, about 40 to 60 μg will deposit in the airways and are likely to induce significant bronchodilation.(25,26) For example, Zainudin et al.(27) observed significant increases in forced expiratory volume, peak expiratory flow, and vital capacity in asthmatic patients receiving 400 μg of aerosolized albuterol, of which about 10% (i.e., 40 μg) were estimated to deposit in the lungs based on radiolabeled aerosol imaging. Based on these quantitative considerations, delivering five puffs could be a condition to be tested in the clinical setting: based on the present bench results, delivering five 100 μg puffs within the NHF circuit would ensure the administration of a minimum of 50 μg of drug, outreaching the 40 μg proposed by Zanuidin et al.
Differences between spacers
Connector or spacer type has an influence on the drug delivery with pMDIs,(28,29) and we also observed such differences in this bench study. These differences may be explained by the specificities of used devices. Higher volume spacers such as ACE and CombiHaler spacers may be more effective by decreasing aerosol impaction due to initial high velocity after pMDI activation. Various shapes of the devices (ACE is rounded on one side and conical on the other; CombiHaler is a double cone device; AeroChamber Vent is a retractable cylindric device) may also influence the air flow transporting aerosol inside the spacer.
Influence of the pMDI position in the circuit and NHF rate
Contrary to the results of studies evaluating nebulization during NHF,(17) we observed that the best position for drug delivery seemed to be placing the pMDI just upstream of the cannulas. This result is related to the fact that pMDI aerosol delivery is synchronized with inspiration. Of note, when actuating the pMDI during expiration, very low amounts of drug were delivered. The correct actuation of the pMDI at the beginning of inspiration may require proper staff training to be optimally implemented in the clinical setting. High NHF rates were associated with a lower albuterol delivery. A previous study observed the same results using nebulizers.(17)
Influence of breathing patterns
We tested two different breathing patterns: one simulating quiet breathing (mean inspiratory flow rate of 15 L/min) and one simulating respiratory distress (45 L/min mean inspiratory flow rate). Respirable mass was higher simulating respiratory distress when the NHF rate was set at 30 L/min. This result is in line with two bench studies(17,30) evaluating nebulization within NHF circuits that similarly observed higher delivery with a respiratory distress breathing pattern. We did not observe this result using the pMDI at 45 and 60 L/min in the present study as delivery was reduced with the respiratory distress breathing pattern. While in nebulization studies aerosol is delivered continuously (i.e., during inspiration and expiration), pMDI actuation was synchronized with the very beginning of inspiration in the present study. The complex interplay between inspiratory, expiratory flow, and aerosol leakage during inspiration and expiration as described by Réminiac et al. may not apply in the present pMDI work.
Study limitations
We simulated calm and respiratory distress breathing patterns in a very simplified way in this bench study compared to real-life breathing patterns. Thus, the results observed in the present study need confirmation in a clinical study. We used humidification settings of 100% relative humidity at 31°C, as higher humidification could have further jeopardized aerosol delivery.(31,32) Results cannot be extrapolated to other humidity and temperature settings such as 37°C, also frequently used in clinical practice. Due to measurement constrains of lower limits of quantification, we tested a pMDI emitted dose of 1000 μg of albuterol (10 actuations) for all experiments. This limit is unlikely to affect interpretation of our results as the relative inhalable and respirable mass should not be influenced by the dose emitted by the pMDI. Several experimental conditions were not evaluated in the present study such as placing the pMDI at the wet side immediately downstream of the humidification chamber or testing NHF rates lower than 30 L/min. Moreover, in the first experimental set, evaluating the amount of drug delivered at the cannula outlet, no breathing simulation was performed; in particular, no patient inspiratory flow was simulated. This represents a limit of the model and may explain that in certain experimental conditions the drug amounts recovered on the filter in this first set of experiments was lower than in the second set. At last, another potential option for pMDI administration is to interrupt NHF for a few seconds and deliver actuations through as spacer with a facemask; this study only tested the experimental condition where NHF is not interrupted and no comparison was performed with other modes of delivery.
Clinical implications
This bench study may pave the way for clinical evaluation of administrating aerosols with pMDIs in patients undergoing NHF. Using a pMDI with a spacer placed in the NHF circuit may be a method to consider at the bedside. However, Alalwan et al.(33) in a recent pediatric bench study showed that pursuing NHF while administering an aerosol with a pMDI and a spacer connected to a facemask was associated with a low aerosol delivery, thus calling for interrupting NHF at least briefly during aerosol delivery. The present bench study shows that connecting a spacer to the circuit is feasible and albuterol may be effectively delivered to the lungs. In highly oxygen-dependent patients and those who cannot tolerate an interruption of NHF, this technique may be beneficial compared to interrupting NHF, removing the cannulas and administering the aerosol with a spacer and a facemask. The practical aspects such as the spacer weight, health care worker intervention to actuate the pMDI require specific clinical evaluation; a major point seems to be the need to synchronize the pMDI actuations with the beginning of inspiration.
In conclusion, the present bench study shows that pMDI aerosol delivery is feasible during NHF and probably associated with a respirable mass likely to induce a clinical bronchodilation effect when optimal settings are implemented. Efficacy study to seek an effective dose and clinical evaluation are needed to validate these experimental findings.
Footnotes
Author Disclosure Statement
P.S., S.G., T.B., C.L., M.P., D.L.P., L.M., and F.R. do not have any conflicts of interest to declare. L.V. is part time employee of Nemera. N.H.V. is cofounder and scientific expert for Cynbiose Respiratory, she receives consultancy fees from Argenx, and research support from Sanofi, Aerogen Ltd. and Signia Therapeutics. S.E. declares receiving consulting fees, unrestricted research grants and equipment research support from Aerogen Ltd., unrestricted research grant from Fisher & Paykel, unrestricted research grant form Hamilton medical, and consulting fees from La Diffusion Technique Française.
Funding Information
This study was funded by Association pour la promotion a Tours de la reanimation medicale.
Reviewed by:
Jie Li
Ann Cuccia