
Abstract
Background:
The understanding of the real flow profiles through a dry powder inhaler (DPI), generated by asthma patients, is a prerequisite for satisfactory drug delivery to the lungs. The aims of the study were to assess the relationship between spirometric measures and inhalation profiles through a low-resistance DPI, and to compare parameters of those profiles between optimal and suboptimal inhalation technique type.
Methods:
Both healthy adult volunteers and patients with asthma were included in the study. Spirometry was conducted along with modified flow-volume test to detect expiratory levels (maximum “100%” exhalation to residual volume [RV] and halfway “50%” to RV). These were the reference levels of the depth of exhalation for each patient to simulate the effect of incomplete exhalation. Individual inhalation profiles were recorded using spirometry in-house software as the volumetric airflow through the inhaler versus time. Inspiratory flow parameters were extracted: time to peak inspiratory flow through inhaler (PIFinh), time at which peak inspiratory flow occurs (tPIFinh), total inhalation time (T), and inhaled volume during maneuver (V).
Results and Conclusions:
There are significant relationships between spirometric indices and parameters of inhalation through a low-resistance, cyclohaler-type DPI (assessed by single-factor analysis of Spearman's rank correlation coefficient). Multiple regression models were constructed, predicting inspiratory flow parameters (including spirometric indices, demographic parameters, and inhaler's usage history as determinants). The exhalation halfway to RV before inhalation did not affect significantly PIFinh and tPIFinh (and, thus, initial flow dynamics) in asthma patients. T and V parameters were then significantly decreased, but seemed sufficient for successful DPI performance. Both exhalation to RV and incomplete exhalation halfway to RV preceding inhalation allow for effective usage of low-resistance DPI.
Introduction
Adequate drug delivery through dry powder inhalers (DPIs) is one of the cornerstones of the effective management of obstructive airway diseases, including asthma. Forceful flow through DPI with a certain resistance should induce fluidization and dispersion of a drug powder, which is emitted as an inhalable aerosol. Flow rate, pressure drop, shear stresses, and generated power during the inhalation maneuver are the inter-related factors known to influence the disaggregation process.(1–4) Superimposed onto the time-varying flow patterns are emission and transport “windows,” when the dose leaves a reservoir or a capsule and enters the oropharyngeal region and is inhaled to the lower airways.(5,6) Given the complexity of DPI systems, the understanding of the real flow profiles through DPI generated by asthma patients is a prerequisite for estimation of the expected deposition of inhaled therapeutic agents.
Current recommendations on asthma management focus on matching inhaler device to the patient's inspiratory capabilities and on confirming the inhalation technique adequacy to achieve an optimal drug-device performance.(7) A cardinal feature of asthma is an increased lower airway resistance due to airway narrowing caused by smooth muscle contraction, airway inflammation, mucus hypersecretion, and its intraluminal accumulation.(8,9) These conditions lead to an increase in the resistive work of breathing.(10) Considering that work of breathing (required inspiratory effort) is the rate of energy applied to the DPI platform during the whole inhalation and part of it is the energy input for the emission and dispersion processes, the increased airway resistance may negatively impact aerosol drug delivery.(11,12) Moreover, a loss of lung elasticity may result in reduced inspiratory and expiratory capabilities. Thus, severity of asthma may be an important factor determining patient's compliance with a passive DPI, hypothetically resulting in unsatisfactory flow profiles through the device in patients with severe airflow limitation. Suboptimal flow patterns do not allow for consistent and reliable dose emission and, in consequence, preclude generation of a good quality aerosol (particle size characteristics) and its appropriate deposition in the desired bronchial regions.(6)
Regarding the effective inhalation technique, a great emphasis is placed on DPI mishandling, which can be eliminated by training, retraining, or seeking alternative inhalers by health care professionals managing asthma patients. A number of studies have been aimed at the identification of patient's key errors in DPI inhalation technique, both specific to a given type of inhaler (e.g. failure to achieve forceful and rapid inspiratory flow) and nonspecific ones, that is, common to all DPI devices (e.g., not taking sufficient exhalation before inhalation).(6,13–21) The majority of inhalation errors have been shown to be repetitive and therefore, potentially possible to eradicate. However, irrespective of patients' dexterity and cognitive ability, it should be kept in mind that some individuals may demonstrate natural inhalation patterns being difficult or even impossible to be modified due to the reduced inspiratory capacity.
The relationship between patients' characteristics, including pulmonary function and generated inspiratory flow through DPIs (of different intrinsic resistance), has been evaluated in numerous studies.(22–31) In this context, the unsteadiness of inhalation maneuver should be addressed, and in vitro/in silico analyses should include previously recognized indicators of DPI performance, which include peak inspiratory flow through inhaler (PIFinh), time to peak inspiratory flow through inhaler (tPIFinh), total inhalation time (T), and inhaled volume during maneuver (V).(32,33) The dose delivery performance was studied extensively in terms of the impact of aforementioned parameters. In vitro studies covered topics related to dose emission characteristics and aerodynamic particle size characteristics of medicinal aerosol,(34–43) while computational studies were focused on better understanding of the fluidization and mechanisms of powder dispersion, jet velocity, turbulence, fluid dynamics, and particle dynamics.(44–48) To date, studies have been focused on collecting asthmatic or chronic obstructive pulmonary disease (COPD) inhalation profiles for experimental and modeling purposes to analyze realistic flow conditions.
The aims of the study were to assess the relationship between spirometric measures and inhalation profiles through a low-resistance DPI, and to compare parameters of those profiles between optimal and suboptimal inhalation technique type with different expiratory levels before inhalation (“maximum” and “halfway” to residual volume [RV]).
Materials and Methods
General study design
This was a basic research, investigator-initiated, open-label study. The study was designed to collect the inhalation profiles of asthmatics and healthy controls inhaling through a representative DPI together with the respective clinical characteristics of the subjects. All study procedures were performed during a single visit. First, a questionnaire, which included demographic data, questions on medical history with information on the inhalers' usage, and the smoking status, was completed. Then, spirometry and modified flow-volume test to record crucial expiratory levels were performed. Afterward, individual inhalation profiles of participants as they inspired through the cyclohaler-type DPI from the RV level and halfway to RV level were recorded.
Patients and volunteers
Adult patients with physician-diagnosed, well-controlled asthma treated on an outpatient basis in the tertiary university hospital in Warsaw were included. Well-controlled asthma was defined as the absence of daytime asthma symptoms more than twice a week, nocturnal symptoms, the need for bronchodilator reliever use, and activity limitations in the previous month according to global initiative for asthma (GINA) recommendations.(7) The severity of asthma was assessed based on the level of treatment required to control symptoms and exacerbations according to GINA guidelines.(7) Healthy volunteers without respiratory symptoms and history of chronic pulmonary diseases were recruited by investigators from the general population of Warsaw, Poland.
The exclusion criteria for both study groups were as follows: the diagnosis of respiratory diseases other than asthma, asthma exacerbation, contraindications for spirometry, or inability to perform acceptable and repeatable spirometry.(49) Healthy volunteers, in whom spirometry conducted during the visit revealed airway obstruction or reduced vital capacity, were also excluded. Ethics approval was obtained from the Institutional Review Board of the Medical University of Warsaw (KB 43/2013). All participants gave written informed consent.
Spirometry
Spirometry was performed with LungTest 1000 spirometer (MES, Cracow, Poland) according to the American Thoracic Society (ATS)/European Respiratory Society (ERS) recommendations.(50) Thirty-millimeter diameter reusable, sterilizable mouthpieces (MES) and reusable, sterilizable DV 40 pneumotachographs (MES) were used. Following parameters were measured: forced expiratory volume in 1st second (FEV1), forced vital capacity (FVC), maximal vital capacity (VCmax), forced inspiratory volume in 1st second (FIV1), peak expiratory flow (PEF), peak inspiratory flow (PIF), forced expiratory flow at 25%–75% (FEF25–75), mean expiratory flow at 75% (MEF75), 50% (MEF50) and 25% (MEF25) of the vital capacity. Percentages of predicted values (for FEV1 and PEF) were calculated using The Global Lung Function Initiative (GLI) ERS Task Force equations for Caucasians.(51)
Modified flow-volume test
Modified flow-volume test was performed using the same LungTest 1000 spirometer supplemented by an in-house software (SpiroMon), developed by Laboratory for Diagnostics and Therapy of Cardiovascular-Respiratory System (Nalecz Institute of Biocybernetics and Biomedical Engineering, Polish Academy of Sciences, Warsaw, Poland). Participants were asked to breathe regularly during several voluntary respiratory cycles until a stable end-expiratory tidal volume was detected. Then, participants were asked to exhale slowly to RV to measure the expiratory reserve volume (ERV). The mean value of 3–6 repeatable measurements was used for further experiments. ERV repeatability was defined as a difference between the largest and the next largest ERV of ≤10%. On the basis of above measurements three crucial expiratory levels were determined: the resting expiratory level, the level of exhalation to RV, and the level of exhalation halfway to RV. The last two expiratory levels corresponded to different levels of exhalation (further referred to as “maximum” and “halfway” level) that were tested during inhalation maneuvers in the next phase of the study. These were the reference levels of the depth of exhalation for each patient to simulate the effect of incomplete exhalation.
Collection of inhalation profiles
The final phase of the study included the recording of individual airflow profiles during inhalation maneuver through the cyclohaler-type DPI using two levels of the inhalation onset: maximum and halfway. All participants received direct verbal instructions from medical staff on how to use a low-resistance DPI. Each subject was asked to inhale 10 times through the experimental setup (Fig. 1): five times from the maximal level and five times from the halfway level. Individual inhalation profiles through a cyclohaler-type inhaler in airtight housing connected to a pneumotachograph of spirometer were recorded as the volumetric airflow through the inhaler versus time, using the software protocol of 25 Hz sampling rate. RS01® inhaler (Plastiape Spa, Osnago LC, Italy) was selected for this study, as a representative of breath-actuated low-resistance DPIs (intrinsic resistance = 0.017 kPa 0.5 L/min). Inhalation maneuvers were performed with DPI containing empty hard gelatin DPI Coni-Snap capsule (Capsugel, USA). No study drugs were administered in this protocol. No follow-up visits were required.
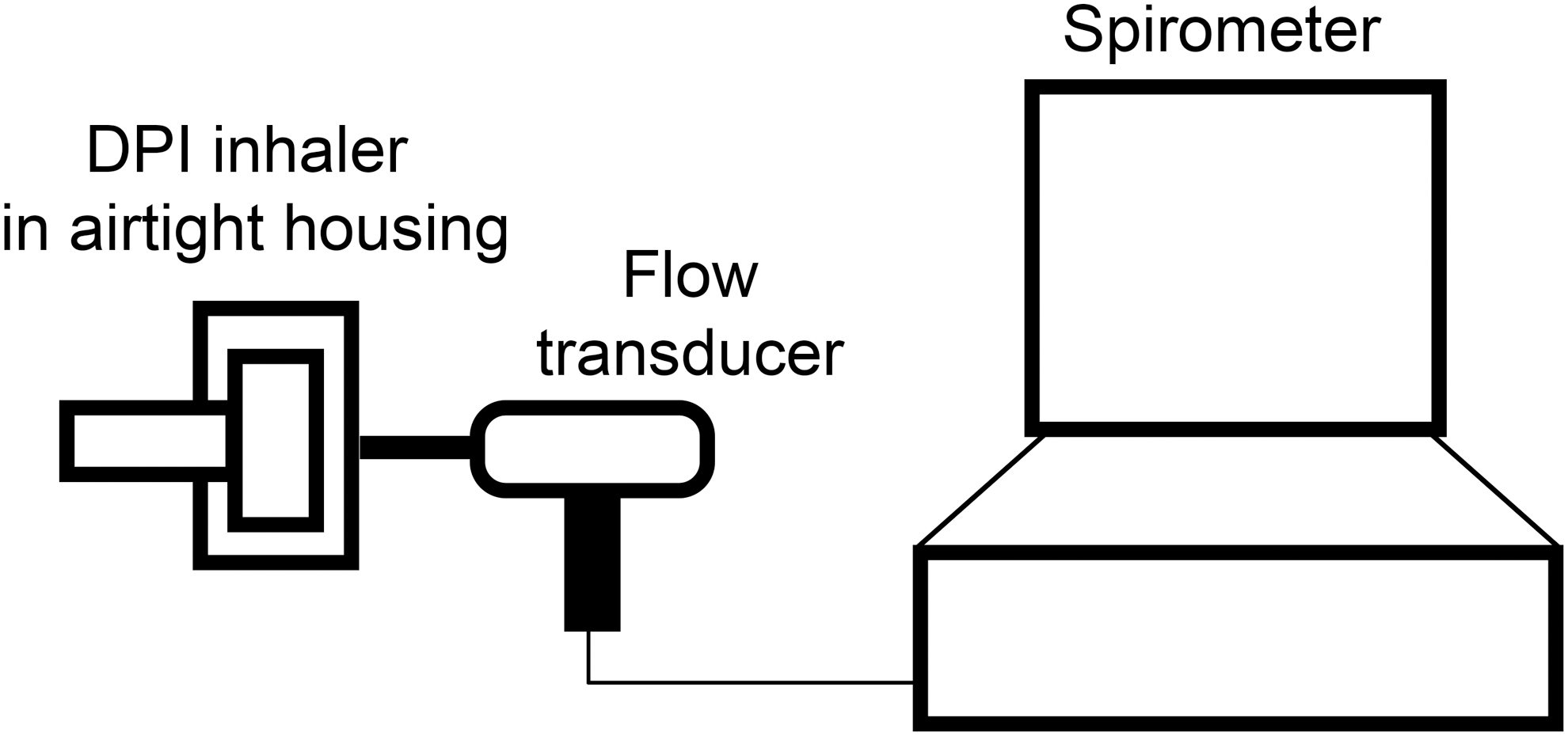
Experimental setup for modified flow-volume test. Individual inhalation profiles through a cyclohaler-type inhaler in airtight housing connected to a pneumotachograph of spirometer were recorded as the volumetric flow rate of air exiting the mouthpiece of the inhaler versus time, using the software protocol of 25 Hz sampling rate. DPI, dry powder inhaler.
Data analysis and statistics
Demographic and spirometry data are presented as mean ± standard deviation. Asthma patients' characteristics, including current and previous inhaler's usage, are presented as number and percentage. Inhalation profiles recorded during the modified pulmonary function test were analyzed to determine their association with two factors: level of exhalation before inhalation (“maximum” and “halfway”) and asthma diagnosis. For this purpose, typical inspiratory flow parameters were extracted from each inhalation profile: PIFinh, tPIFinh, T and V described previously elsewhere.(52) Sets of values for PIFinh, tPIFinh, T and V were assessed. The maneuver with preceding exhalation to RV resulted in the data set denoted PIFinh100%, tPIFinh100%, T100%, V100%. The maneuver with preceding exhalation halfway to RV resulted in the data set denoted PIFinh50%, tPIFinh50%, T50%, and V50%.
We used the independent t-Student test and the U Mann–Whitney test to assess differences between healthy and asthma group in normally and not-normally distributed variables, respectively (when the assumption of homogeneity of variance has been met). In case of normally distributed variables exhibiting heterogeneity of variances, the t-Student test with Cochran–Cox adjustment was used. The t-Student test for dependent variables and the Wilcoxon matched pairs test were used to assess the differences between maximum and halfway types of exhalation, depending on the fulfilled assumptions of normally distributed variables and homogeneity of variance.
Further inferential statistics were estimated as follows: the quantitative relationship between mean inspiratory flow parameters (PIFinh, tPIFinh, V, and T) and set of explanatory factors (independent determinants) was examined using multiple regression method. Regression coefficients of factors were investigated, concerning selected demographic factors, spirometric parameters, and inhaler's usage history. Potential independent factors were gender, age, height, body mass index (BMI), FEV1% predicted (FEV1%pred), PEF % predicted (PEF%pred) or PEF, PIF, “DPI then/now,” “pressurized metered dose inhaler (pMDI) then/now” concerning past and/or present DPI and pMDI usage, respectively. Additional independent variable was coded as occurrence of “expiratory limitation.” Expiratory limitation was defined by FEV1/FVCex percentile (pseudo-Tiffeneau index percentile), where the index value below the fifth percentile of the reference population was applied to diagnose expiratory limitation.
General linear models were used to assess the chosen sets of independent determinants in terms of multicollinearity among the variables in a regression model.
Single-factor, nonparametric analysis of Spearman's rank correlation coefficient was done to test the relationship between mean inspiratory flow parameters (PIFinh, tPIFinh, V, T) and chosen spirometric parameters: FEV1, FEV1%pred, FIV1, FVCex, FVCin, VCmax, PEF, PIF, FEF25–75, FEF25–75% predicted (FEF25–75%pred), MEF75, MEF50, MEF25, MEF75% predicted (MEF75%pred), MEF50% predicted (MEF50%pred), MEF25% predicted (MEF25%pred). “In” and “ex” denote inspiratory and expiratory parameters, respectively.
For every statistical analysis conducted throughout the study, a p-value <0.05 was regarded as statistically significant. Normality of the residuals was judged by normal quantile plots, visual inspection of the distribution of residuals, and the result of Shapiro–Wilk test. Statistica 13.0 (StatSoft Inc., Tulsa, OK) was used for all statistical analyses.
Results
Subjects
Forty-three subjects were initially enrolled. However, 3 (7%) of them had to be excluded from analysis due to the following reasons: inability to perform repeatable maximal exhalations (one asthma patient), diagnosis of asthma–COPD overlap (one asthma patient), and inability to perform repeatable spirometric maneuvers (one healthy volunteer). Thus, data from 40 eligible subjects (19 M, 21 F) were included in the final analysis. These included 16 healthy volunteers and 24 asthma patients. The comparative demographic, clinical, and baseline spirometry characteristics of the study groups are shown in Table 1. In our cohort asthma patients were significantly older compared with healthy subjects (45.7 ± 17.0 years, p < 0.008 vs. 31.6 ± 9.4 years). Furthermore, we found that FEF25/75%pred and MEF50%pred were significantly lower in asthma patients compared with healthy subjects: (61.9 ± 26.9% vs. 83.4 ± 19.7%, p = 0.009 and 60.3 ± 26.8% vs. 86.7 ± 21.5%, p = 0.002, respectively). As expected, we recorded that significantly higher percentage of asthmatic patients currently or previously used pMDI compared with healthy subjects (91.7% vs. 18.8%, p < 0.0001). However, there was no significant difference between asthmatic patients and healthy subjects in terms of current or previous usage of DPI (41.7% vs. 18.8%, p = 0.13). In healthy subjects, pMDIs and DPIs were used incidentally in the past for the treatment of respiratory symptoms due to acute respiratory infections.
Summary of Subject Demographics, Spirometric Parameters, and Inhaler's Usage History by Occurrence of Asthma
(T) denotes t-test for independent groups, (C–C) denotes the Cochran–Cox test and (M–W) denotes the Mann–Whitney U test.
BMI, body mass index; DPI, dry powder inhaler; FEF25/75%pred, percentage predicted of forced expiratory flow between 25% and 75% of forced vital capacity; FEV1%pred, percentage predicted of forced expiratory volume in 1 second; MEF75%pred, MEF50%pred, MEF25%pred, percentage predicted of maximal expiratory flow at 50%, 75%, and 25% of the forced vital capacity, respectively; PEF, peak expiratory flow; PEF%pred, percentage predicted of peak expiratory flow; PIF, peak inspiratory flow; pMDI, pressurized metered dose inhaler.
Inspiratory flow parameters
Data on inspiratory flow parameters measured after full exhalation and exhalation halfway to RV in asthma patients and healthy volunteers are presented in Table 2. We did not find significant differences between asthmatic patients and healthy volunteers in inspiratory flow parameters recorded after full exhalation and exhalation halfway to RV. We observed that time of inhalation and inhalation volume were significantly greater when measured after full exhalation compared with exhalation halfway to RV both in asthma patients and in healthy subjects. Furthermore, we recorded that tPIFinh was significantly greater when measured after full exhalation compared with exhalation halfway to RV in healthy subjects. In asthmatic patients the above difference was not significant.
Descriptive Result Summary of Inspiratory Flow Parameters, by Occurrence of Asthma
(T) denotes t-test for independent groups or dependent samples, respectively. (C–C) denotes the Cochran–Cox test and (W–M) denotes the Wilcoxon matched pairs test. Parameters measured during the maneuver with preceding exhalation to residual volume are denoted as PIFinh100%, tPIFinh100%, T100%, and V100%. Parameters measured during the maneuver with preceding exhalation halfway to residual volume are denoted as PIFinh50%, tPIFinh50%, T50%, and V50%.
PIFinh, peak inspiratory flow through inhaler; T, inhalation time; tPIFinh, time to peak inspiratory flow through inhaler; V, inhalation volume.
The relationship between inspiratory flow parameters and spirometry results: single-factor analysis of Spearman's rank correlation coefficient
Correlations between the respective inspiratory flow parameters measured after full exhalation and exhalation halfway to RV (PIFinh100%, PIFinh50%, tPIFinh100%, tPIFinh50%, V100%, V50% and T100%, T50%) with individual spirometric parameters are shown in Tables 3 and 4. We found that both PIFinh100% and PIFinh50% correlated significantly with FEV1, FVCin, VCmax, PEF, and PIF in healthy subjects as well as in asthma patients. We also observed significant correlations of PIFinh100% and PIFinh50% with FEV1%pred and of PIFinh100% with FEF25/75%pred, MEF50%pred, and MEF25%pred in healthy subjects. Furthermore, we demonstrated significant correlations of PIFinh100% with FEV1 and MEF25%pred in asthma patients. We did not find significant correlations between tPIFinh and spirometric measures, except for significant correlation between tPIFinh100% and PIF in asthma patients. Inhalation time correlated significantly with several spirometric measures in healthy subjects (significant correlations of T100% with FEV1, FIV1, FVCex, and VCmax as well as of T50% with FEV1, FEV1%pred, FIV1, and FEF25/75%pred) and in asthma patients (significant correlations of T100% with FEV1%pred, FEF25/75, MEF75, and MEF25 as well as of T50% with FIV1, FVCex, and VCmax). Moreover, both V100% and V50% correlated significantly with FEV1, FVCex, FVCin, VCmax, PEF, PIF in healthy subjects as well as in asthmatic patients. Finally, significant correlations of V100% and V50% with FEF25/75, MEF75, MEF50, MEF25 as well as of V100% with FEV1%pred were demonstrated in asthma patients.
The Relationship between Peak Inspiratory Flow Parameters (PIFinh and tPIFinh) and Respective Spirometric Parameters, by Occurrence of Asthma
FEF25/75, forced expiratory flow between 25% and 75% of forced vital capacity; FEV1, forced expiratory volume in 1 second; FIV1, forced inspiratory volume in 1 second; FVCex, forced expiratory vital capacity; FVCin, forced inspiratory vital capacity; MEF75, MEF50, MEF25, maximal expiratory flow at 50%, 75%, and 25% of the forced vital capacity, respectively; VCmax, maximal vital capacity.
The Relationship between Peak Inspiratory Flow Parameters (V and T) and Respective Spirometric Parameters, by Occurrence of Asthma
Multiple regression models predicting inspiratory flow parameters
The multiple regression models predicting inspiratory flow parameters for inhalation preceded by maximal exhalation in asthma patients are presented in Tables 5–8. We recorded the following independent significant predictors of inspiratory flow parameters: (1) for PIFinh100%: BMI, the previous usage of DPI, PIF; (2) for tPIFinh100%: the previous usage of DPI; (3) for V100%: height, FEV1%pred, the presence of expiratory flow limitation; and (4) for T100%: FEV1%pred, the presence of expiratory flow limitation, the previous usage of DPI.
Results of the Multiple Regression Model to Predict PIFinh in Asthma Group for Maximal Exhalation Before Inhalation
For the full model, R2 = 0.70 (p < 0.002). b* denotes standardized coefficient of regression, b denotes coefficient of regression, R2 denotes coefficient of determination.
Results of the Multiple Regression Model to Predict tPIFinh in Asthma Group for Maximal Exhalation Before Inhalation
For the full model, R2 = 0.28 (p < 0.16). b* denotes standardized coefficient of regression, b denotes coefficient of regression, R2 denotes coefficient of determination.
Results of the Multiple Regression Model to Predict V in Asthma Group for Maximal Exhalation Before Inhalation
For the full model, R2 = 0.74 (p < 0.00009). b* denotes standardized coefficient of regression, b denotes coefficient of regression, R2 denotes coefficient of determination.
Results of the Multiple Regression Model to Predict T in Asthma Group for Maximal Exhalation Before Inhalation
For the full model, R2 = 0.65 (p < 0.003). b* denotes standardized coefficient of regression, b denotes coefficient of regression, R2 denotes coefficient of determination.
Discussion
We demonstrated that the most important descriptive parameters of inhalation through a representative low-resistance, cyclohaler-type DPI are related to spirometric measures both in asthma patients and in healthy adults. We also proposed spirometric predictors of the inhalation profile through a cyclohaler-type DPI. Incomplete exhalation before inhalation through a cyclohaler-type DPI was shown not to affect PIFinh and corresponding tPIFinh in asthma patients.
Our study includes some novelties. We used spirometry in-house software (SpiroMon), which enabled us to determine reference levels of the depth of exhalation for each patient to simulate the effect of incomplete exhalation. We also constructed an experimental setup consisting of a DPI in an airtight housing connected to a pneumotachograph. It allowed us to measure standard spirometric parameters and parameters characterizing inhalation profiles through a DPI using the same spirometer. To the best of our knowledge this is the first study in which parameters of inhalation profiles through a DPI were compared between asthma patients and healthy adults, and analyzed in relation to the optimal and suboptimal inhalation technique.
After full exhalation (100%), PIFinh >90 L/min was achieved by all healthy subjects and by 75% of asthmatic patients (18 of 24). A halfway to RV exhalation (50%) preceded inhalation with PIFinh >90 L/min in 93.75% of healthy subjects (15 of 16) and in 87.5% of asthma patients (21 of 24). A significant link between asthma occurrence and the ability to produce PIFinh >90 L/min was only observed in the case of 100% exhalation before inhalation, and not observed in the case of 50% exhalation (Pearson's chi-square p = 0.03 vs. p = 0.52, respectively). We may hypothesize that shallower exhalation before inhalation may facilitate higher PIFinh acquisition; a more thorough analysis should be undertaken in the future. Determination of pulmonary function indices, which may predict the value of PIFinh through a low-resistance cyclohaler-type DPI, could help confirm the usefulness of this type of inhaler for a specific patient. As turbulence kinetic energy is a product of inhalation flow and inhaler resistance, PIFinh through a low-resistance inhaler needs to be relatively high (>90 L/min) to produce sufficient energy to deagglomerate drug particles during inhalation.(15) Lower values of PIFinh are required for MDIs and high-resistance DPIs. However, appropriate use of MDIs requires good actuation–inhalation coordination, which is impossible for some patients, especially children and elderly.(15) On the contrary, some patients with dyspnea, despite being able to achieve required PIFinh through high-resistance DPIs, may not be able to achieve sufficient inhalation volume through a high-resistance inhaler.(53)
PIFinh is reported to be the key parameter predicting the effectiveness of the drug inhalation from DPI. The following parameters are influenced by the PIFinh: the dose emitted by a DPI, the fine particles fraction, and the dose deposited in the lower airways.(22) Inspiratory flow through an inhaler, which has an intrinsic resistance, could not be measured in routine practice. Spirometric measurement of PIF is obtained at zero resistance and does not directly reflect the value of PIFinh.(23) However, our results indicate that spirometric measures are well correlated with measures of inhalation profile through a low-resistance cyclohaler-type DPI. We demonstrated that PIFinh through a low-resistance DPI and inhalation volume were well correlated with spirometric measures both in asthma patients and in healthy participants. On the contrary, inhalation time and time to PIFinh seemed to be somewhat less correlated with spirometric measures. Also, based on the multiple regression analysis (presented in Tables 5, 6, and 8) it is clear that patient's history of DPI usage was found to be significant, since it affected dynamics of inhalation technique, namely PIFinh, tPIFinh, and T values. Using DPI in the past and/or at the moment is correlated with quicker and more forceful maneuver of higher PIFinh with both lower tPIFinh and T.
The relationship between spirometric measures and parameters of inhalation through DPI has previously been assessed mainly in COPD patients. Broeders et al.(25) observed that MEF50 was a significant predictor for PIFinh through Diskus® inhaler, and inspiratory capacity (IC) was a significant predictor for PIFinh through Turbuhaler® in patients with an acute exacerbation of COPD. These authors found an average increase of PIFinh of 7.3 (±2.1) L/min per 1 L/s increase in MEF50 for Diskus and of 8.6 (±7.5) L/min per liter increase in IC for Turbuhaler.(25) We did not observe significant correlation between MEF50 and PIFinh through a low-resistance DPI in patients with asthma and in healthy participants.
Sarinas et al. demonstrated the lack of correlation between PIFinh and FEV1%pred in patients with COPD and cystic fibrosis.(24) In contrast, we found a significant correlation between the above parameters in healthy participants (R = −0.58 for full exhalation and R = −0.55 for halfway exhalation), but not in asthma patients. One recent paper reported moderate-to-strong significant correlations (R = 0.55–0.60) between PIFinh and native PIF in COPD patients for three different DPIs (Breezhaler®, Genuair®, Turbuhaler), which is in line with our findings.(22) Similarly to our findings, the study by Farkas et al. showed only a weak-to-moderate correlation between PIFinh and FEV1 (R = 0.23–0.40 for different DPIs).(22) In terms of the relationship between PIFinh and FVC, our study showed a moderate-to-strong correlation in asthmatics, whereas Farkas et al. demonstrated only weak correlation in COPD patients.(22)
Price et al. measured PIFinh after COPD exacerbation using In-Check DIAL® (Clement Clarke International LTd., Harlow, UK), a portable inspiratory flow meter, intrinsic resistance of which was set to simulate characteristics of Aerolizer® (inhaler similar to RS01 with identical resistance of 0.017 kPa 0.5 L/min), medium-resistance Diskus and medium/high-resistance Turbohaler®.(23) The authors observed significant univariate associations between PIF measured with settings simulating Aerolizer, Diskus, and Turbohaler inhalers and FEV1 (R2 values 0.109, 0.172, and 0.230, respectively) and PEF%pred (R2 0.133, 0.134, and 0.294). In multivariate analysis, they observed that FEV1 was the only variable retained for prediction of PIF through Aerolizer and Diskus (R2 values as above), and the best model for prediction of PIF for Turbohaler included FEV1 and PEF%pred (R2 = 0.374). They also reported small positive correlation between PIFinh and PEF%pred for different resistance settings (correlation coefficient range 0.1–0.5) and FEV1 (correlation coefficient range 0.3–0.5), as well as a negative correlation between PIF through inhaler and age (the absolute value of correlation coefficient range 0.2–0.4). Noteworthily, associations between both clinical and spirometric measures and PIF through an inhaler recorded by Price et al. were weak, and authors suggested that PIFinh against resistance should be measured directly.(23)
Multiple regression models used in our study showed that in asthma patients PIFinh measured during inhalation after full exhalation could be predicted by BMI, PIF, and the previous usage of DPI, independently from PEF%pred. Interestingly, in the regression model PIFinh was found to be inversely related to PEF%pred (standardized coefficient of regression b* = −0.59, p = 0.06). However, it should be emphasized that PEF%pred was not found to be a significant predictor of the PIFinh unlike other proposed variables introduced into the model. Possible explanation of this counterintuitive observation could be related to the small sample size and the fact that relatively high numerical value of flow rates, despite decreased PEF%pred, could be observed in the young and tall subjects with a high predicted value. We also showed that inhalation volume could be predicted by patient's height; FEV1%pred and the presence of expiratory airflow limitation, independently from age and BMI. We also showed that inhalation time could be predicted by FEV1%pred, the presence of expiratory airflow limitation, and the previous usage of DPI, independently from using pMDI currently/in the past. Furthermore, we demonstrated that the only significant predictor of time to PIFinh through a low-resistance, cyclohaler-type inhaler in asthma patients is DPI's usage.
In another study, Grabowski et al. used In-Check DIAL (Clement Clarke International LTd.) to simulate characteristics of Aerolizer, Diskus, and Turbuhaler, and assessed PIFinh in patients during and after exacerbation of COPD and asthma.(54) PEF and FEV1 measured by spirometry in COPD patients during exacerbation correlated significantly with PIF through the valve simulating above devices (R values 0.87–0.89 and 0.75–0.82, respectively). Interestingly, the authors found a slightly weaker correlation when postexacerbation measurements were analyzed.(54) In patients with asthma exacerbation PEF correlated significantly with PIFinh through valves imitating all of the above devices (R 0.72–0.79), whereas no significant correlations were found between FEV1 and PIFinh. In stable asthma, PIFinh through Aerolizer, Diskus, and Turbuhaler correlated with PEF with the R value of 0.72–0.83, whereas PIFinh through above devices correlated with FEV1 with the R value of 0.57–0.70. For both spirometric measures and parameters of inhalation through the valve simulating Aerolizer, the authors reported slightly higher R values compared with our results. In another study, which included asthma patients, Prime et al. demonstrated significant correlations between spirometric measures and inhaler-specific (Ellipta® DPI, medium resistance) inhalation parameters. These included the following: FEV1 and PIFinh (R = 0.52); FEV1 and inhaled volume (R = 0.6); FVC and inhaled volume (R = 0.62); PEF and PIFinh (R = 0.66); and PIF and PIFinh (R = 0.69).(29) Furthermore, Prime et al. did not observe statistically significant difference in PIFinh between healthy subjects and asthma patients.(29)
The failure to exhale before inhaling through a DPI is one of the most frequent errors in the inhalation technique with reported frequency of 12%–77%.(13,18) The ideal inhalation through a DPI should be preceded by the exhalation to the RV.(15) However, concerns are raised that full exhalation to RV may cause temporary collapse of some airways and reduce the drug delivery.(55) Exhalation to the functional residual capacity (FRC), which is less likely to provoke cough and more comfortable for patients, was reported to be an acceptable alternative.(13,56) We observed that the exhalation halfway to RV before inhalation did not significantly affect PIFinh and tPIFinh in asthma patients. As expected, inhalation time and inhalation volume were significantly decreased when measured after incomplete exhalation. However, the values of inhalation volume and time observed after exhalation halfway to RV seemed sufficient for a DPI to deliver the aerosol to the lower respiratory tract. In our cohort minimal values of inhalation time and inhalation volume after incomplete exhalation in asthma patients were 1.2 seconds and 1.8 L, respectively. For a DPI, a volume of 500 mL inhaled after reaching the minimum required PIFinh and inhalation time >1 second are reported to be sufficient for drug delivery to the lower respiratory tract.(57,58)
Only scarce data on the impact of incomplete exhalation on the parameters of inhalation through DPIs have been published. Engel et al. compared the efficacy of terbutaline inhalation from Turbuhaler using different techniques, including inhalation preceded by exhalation to RV and inhalation preceded by exhalation to FRC.(56) They reported comparable PIFinh, level of bronchodilatation induced by terbutaline, amount of drug deposited on viral filters included in the experimental set, and plasma terbutaline concentrations when the above techniques were used. Although we confirmed that exhalation halfway to RV instead of full exhalation to RV does not impair PIFinh and tPIFinh in asthma patients, we cannot exclude that decreased inhalation time and volume after incomplete exhalation may impair drug deposition in the lower airways. Presented study on the suboptimal inhalation technique should be treated as the beginning of research within this area, which is of great interest for researchers conducting clinical trials, compendial inhaler's testing, while developing novel DPI designs. Further studies are needed to assess the impact of inhalation profile parameters on drug deposition in airways. The effect of type of exhalation before inhalation (with severity of asthma as categorical factor) on these secondary inhalation variables (and also PIFinh and tPIFinh) will be assessed using repeated-measures analysis of variance. This issue will be elaborated further as the continuation of the presented work.
We acknowledge that our study has several limitations. First, we included relatively small number of participants, which might have affected the strength of our findings. Therefore, the results should be treated as a preliminary quantification rather than as a definitive outcome. We also used empty drug capsule in RS01 inhaler, instead of placebo-filled capsule, which may have slightly influenced intrinsic resistance of the inhaler. Furthermore, patients with severe stages of asthma and significant impairment of lung function were under-represented in our study. Finally, we only included patients with stable, well-controlled asthma, whereas we could speculate that associations between pulmonary function parameters and parameters of inhalation through low-resistance DPI may change during exacerbation of the disease.
Conclusions
In conclusion, there are significant relationships between spirometric indices and parameters of inhalation through low-resistance, cyclohaler-type DPI. Most important parameters of inhalation through low-resistance DPI could be predicted by spirometric indices. Both exhalation to RV and incomplete exhalation halfway to RV preceding inhalation allow for effective usage of low-resistance DPI.
Footnotes
Author Disclosure Statement
The authors have no conflicts to declare. Supplies and equipment were purchased from commercial sources. No conflicts of interest exist.
Funding Information
This study was supported by the National Science Centre, Poland (project no. 2017/25/N/ST8/00809).
Reviewed by:
Tim Corcoran