
Abstract
Modeling particle deposition in the human lung requires information about the morphology of the lung in terms of simple geometric units, e.g., characterizing bronchial airways by straight cylindrical tubes. Five different regional deposition models are discussed in this section with respect to morphometric lung models and related mathematical modeling techniques: 1) one-dimensional cross-section or “trumpet” model, 2) deterministic symmetric generation or “single-path” model, 3) deterministic asymmetric generation or “multiple-path” model, 4) stochastic asymmetric generation or “multiple-path” model, and 5) single-path computational fluid and particle dynamics (CFPD) model. Current deposition models can predict the following regional deposition quantities relevant for the administration of medical aerosols: 1) regional bronchial and alveolar deposition, 2) generational lung deposition, 3) lobar deposition, 4) generational lobar deposition, and 5) generational surface deposition. Although deposition fractions predicted by the different models depend on the selection of a specific morphometric lung model and a specific set of analytical deposition equations, all models predict the same trends as functions of particle diameter and breathing parameters. In general, the overall agreement between the modeling predictions obtained by the various deposition models and the available experimental evidence indicates that current deposition models correctly predict regional and generational deposition.
Introduction
The diagnostic or therapeutic administration of medical aerosols requires information on regional and local deposition patterns within the lungs. For example, it is necessary to target certain disease-specific regions in the lungs, such as the bronchial airways in the case of asthma or the alveolar region in the case of emphysema. Currently available experimental data on total and regional deposition refers to specific adult volunteers and specific inhalation conditions. However, particle deposition is needed for all members of the public and for all relevant particle sizes and breathing conditions. Because of the apparent limitations of the experimental determination of regional and local deposition fractions, this information can only be provided by particle deposition models.
Modeling Particle Deposition in the Lungs
Modeling particle deposition in the human lung requires information about biological and physical parameters affecting particle deposition in human airways. Biological factors are the lung morphology, which defines the airway geometry as a system of cylindrical airways, and respiratory parameters, which determine airflow and velocities of particles entrained in the airstream. Physical factors are the fluid dynamics of the inhaled air volume, which determine airflow patterns throughout the lung, and particle properties and physical deposition mechanisms, which allow the calculation of deposition fractions in specific airway generations.
Morphometric lung models
The human respiratory tract is commonly divided into three major regions(1): 1) the extrathoracic (ET) region, 2) the tracheobronchial (TB) region, and 3) the alveolar (A) region. Morphometric lung models always refer to the lung (thoracic region), consisting of the TB and A compartments, while the ET region is considered merely a filter which determines the fraction of particles actually reaching the lung.
In all morphometric lung models, parent airways branch into two daughter airways at each bifurcation, either in a simplified symmetric fashion(1–3) or considering the experimentally observed asymmetric branching scheme.(4,5) While conductive airways in the TB region are represented by straight cylindrical tubes, alveoli attached to the respiratory airways in the alveolar region can be approximated by truncated spheres.(6) Such geometric simplifications are necessary to obtain analytical solutions of the deposition efficiency equations for the governing physical deposition mechanisms. The spatial location of individual airways within the lung relative to the trachea, is characterized by an assigned airway generation number, starting with generation 0(1,2) or 1(3,4) for the trachea.
The two most extensive morphometric data sets of the bronchial tree geometry have been provided by Weibel(2) and by Raabe and colleagues.(7) For modeling purposes, these morphometric data were subsequently utilized to define bronchial tree models, such as the Weibel model A,(2) later modified by Haefeli-Bleuer and Weibel,(8) the Yeh and Schum model,(3) the International Commission on Radiological Protection (ICRP)(1) Human Respiratory Tract Model (HRTM), adapted from the models of Weibel,(2) Yeh and Schum(3) and Phalen and co-investigators,(9) and the stochastic lung model of Koblinger and Hofmann.(4)
In the measurements of Raabe and coworkers,(7) the diameters, lengths, branching and gravity angles of the bronchial tree were recorded for the trachea and all bronchial airways down to about generation 10, while only 10–25% of bronchiolar airways down to terminal bronchioles were measured. The simplest and computationally most convenient method to complete the bronchiolar airway structure is to calculate the arithmetic means for all structural parameters of the bronchiolar airway system, assuming that the measured fraction is also representative of the airway geometry of the missing airways. This averaging procedure leads to the construction of symmetrically branching deterministic lung models,(1–3) where each inhaled particle follows the same path. Therefore, these models are commonly called “single path” or “typical path” models.
Despite their simplicity and computational convenience, these deterministic symmetric lung models cannot consider the asymmetry of the airway branching pattern. Thus, instead of using average values for the bronchial airway dimensions, Koblinger and Hofmann,(4,10) developed a stochastic asymmetric lung model based on the Raabe and colleagues data.(7) Airway diameters, lengths, branching and gravity angles in bronchial and bronchiolar airways(7) were statistically analyzed in terms of frequency distributions and correlations among several parameters, e.g., between parent and daughter cross-section. Thus, the bronchiolar airway system was completed by assuming that the parameter distributions and correlations in the missing airways are the same as those in the measured airways. The experimentally observed branching asymmetry and variability of airway dimensions leads to highly variable path lengths from the trachea to a given generation. Deterministic versions of the stochastic lung model were also used in the deterministic asymmetric or “multiple-path” model proposed by Asgharian and co-investigators.(5)
It is important to note that current morphometric models of the human tracheobronchial tree are based on a few lung casts, which raises the question of intersubject variability.(11) Indeed, measurements of bronchial airway lengths, diameters and branching angles in different human lung casts revealed significant differences among subjects.(12)
While the first measurements of alveolated airways were reported by Hansen and Ampaya,(6) the most extensive data set of pulmonary airways were supplied by Haefeli-Bleuer and Weibel.(8) Average values for airway diameters and lengths were eventually implemented into a revised Weibel model.(8) In the stochastic lung model,(10) these data were again statistically analyzed to define a stochastic, alveolar airway geometry, which considers the additional variability in the number of alveolated airway generations along a given pathway and the linear dimensions in each airway.
In symmetric deposition models, alveoli are commonly incorporated into the pulmonary airway models by determining effective channel diameters, obtained by enlarging the diameters of alveolar ducts by the volume of adjacent alveoli,(13) or by an effective alveolar volume per generation in the case of one-dimensional cross-section models.(14) In the stochastic lung model(10,15) and the serial bolus model,(16) deposition in single alveoli is computed for each respiratory airway generation, assuming identical alveoli (truncated spheres),(6) multiplied by the frequency of the number of alveoli per generation.(2)
To illustrate the structure of whole lung airway models, the number of airways, diameters, lengths, branching and gravity angles, and related parameters of the typical path model of Yeh and Schum(3) are compiled in Table 1. Since it is a deterministic symmetric airway model, all airway generations from 1 (trachea) to 16 (terminal bronchioles) form the bronchial tree, while alveolar airways range from generation 17 (first respiratory airway) to generation 24 (alveolar sac), and all alveoli are lumped together in generation 25. The listed airway diameters and lengths refer to a total lung volume of about 5500 cm3.
Morphometric Airway Parameters of the Typical Path Model of the Human Lung Proposed by Yeh and Schum(3)
Terminal bronchioles, **Alveoli, n = generation number, N = number of airways, D = airway segment diameter, L = airway segment length, θ = branching angle, ϕ = gravity angle with 90o corresponding to a horizontal tube, S = cross-sectional area, V = volume, ΣV = cumulative volume.
Since the measured bronchial airway dimensions in the Raabe and co-investigators(7) study reportedly refer to total lung capacity (TLC),(3) all bronchial airway diameters and lengths have to be scaled down to a standard functional residual capacity (FRC) of 3300 cm3 for an adult male (or 2680 cm3 for an adult female)(1) by applying a constant scaling factor defined as the cube root of the ratio of standard FRC to TLC. The same scaling procedure can be used for the extrapolation from the standard FRC to an individual FRC,(11) derived from pulmonary function tests. Upon inspiration of a defined tidal volume VT, each airway, except for trachea and main and lobar bronchi, is assumed to expand at the same rate until reaching a lung volume of FRC + VT at the end of inspiration, and likewise to contract to FRC at the end of expiration, which can be approximated by an average constant lung volume of FRC + VT/2,(5) to which airway diameters and lengths are finally rescaled.
Modeling assumptions and related input parameters
The main respiratory parameters determining particle deposition are the breathing frequency f and the VT. Standardized values for different physical activities for men, women and children of different ages are listed in the ICRP report.(1) Additional breathing parameters for modeling purposes are the inspiration, expiration and breath-hold times. The corresponding physical parameters determining particle deposition are the inspiratory flow rate or the corresponding particle velocity in a given airway.
The transport of inhaled particles through the whole lung is based on the fundamental principle that particles contained in a given air volume travel with the same velocity as the air volume (“convective transport”). For small particles, however, the axial velocity of these particles may deviate from the convective transport velocity (“axial diffusion”), which can be expressed by an effective diffusion coefficient.(17,18) Flow-induced alveolar mixing, which can lead to a mixing of the inhaled tidal air with the residual air in the alveoli,(19) can be considered by empirical mixing factors, derived from experimental data.(18)
In contrast to the symmetric flow splitting in symmetrically branching typical path models, flow splitting at airway bifurcations in asymmetrically branching lung models is commonly assumed to be proportional to the distal lung volume which is supported by either daughter airway.(18,20) Nonuniform ventilation of the lung can be modeled by lobe-specific ventilation coefficients and time-dependent ventilation functions.(18) While nonuniform ventilation plays only a minor role for normal breathing in a healthy lung, it may become important for hypergravity, high breathing rates, or airway diseases.(20)
The main parameter of an inhaled particle with respect to deposition is its diameter, such as the thermodynamic diameter in the diffusion domain and the aerodynamic diameter for the impaction and sedimentation regimes. However, particle diameters may change upon penetration into the lung due to hygroscopic growth or evaporation of volatile compounds in the humid environment of the lung.(21–24) The magnitude of deposition mechanisms in lung airways varies with particle parameters (particle diameter, density and shape), morphometric parameters (airway diameter and length, branching angle and gravity angle), and breathing parameters (flow rate).
Particle Deposition Models
Five different regional deposition models will be discussed in the following section with respect to morphometric lung models and related mathematical modeling techniques(25): 1) one-dimensional cross-section or “trumpet” model, 2) deterministic symmetric generation or “single-path” model, 3) deterministic asymmetric generation or “multiple-path” model, 4) stochastic asymmetric generation or “multiple-path” model, and 5) single-path computational fluid and particle dynamics (CFPD) model. Particle deposition in the first four models is determined by analytical deposition equations for specified idealized flow profiles, while the last model uses CFPD methods, thereby coupling flow and individual particle transport for realistic flow profiles.(25)
One-dimensional cross-section or “trumpet” model
In this model, the human airway system is approximated by a one-dimensional, variable cross-section channel, where the cross-sections are functions of the generation number of a given symmetric lung model, typically Weibel's model A.(2,14,16) In the peripheral alveolated generations, additional volume for the alveoli encircles the channel. The cross-sectional area increases sharply with distance from the trachea, adopting a trumpet-like shape, hence the name “trumpet” model.
The transport of inhaled particles by convection and axial diffusion, their deposition along the channel, and mixing between tidal air and reserve volume are described mathematically by a time-dependent mass balance differential equation with different loss terms for the various loss and deposition mechanisms.
Initially developed by Taulbee and Yu,(14) the trumpet model was further developed by Nixon and Egan(26) and Darquenne and Paiva.(27) Recently, this model was extended by Robinson and Yu,(28) Mitsakou and coworkers,(29) and Choi and Kim(16) by incorporating dynamic processes affecting the size of the inhaled aerosol, such as hygroscopic growth, coagulation, electrical charge, and gas phase chemical reactions.
A significant limitation of this approach is the rather crude airway geometry, which refers to generational airway volumes without internal structure. Consequently, trumpet models cannot simulate asymmetric effects of airway geometry and related flow rates. On the other hand, a positive feature of such models is the clean mathematical formulation and solution of differential equations describing transport and deposition phenomena, and the computationally convenient way to include several simultaneously acting mechanisms by simply adding specific loss terms.
Deterministic symmetric generation or “single-path” model
In the frequently used symmetric lung models,(1–3) all airways in a given airway generation have identical linear dimensions (Table 1). Because of the symmetric branching, the inhaled airflow and entrained particles are equally distributed among all airways in a given generation, leading to identical deposition fractions in each airway.
For particle deposition calculations, airway generations are treated as a series of filters through which particles are passing during inspiration and expiration. Each of these generational filters is defined by the fraction of particles reaching that generation and by the deposition efficiencies for the specific deposition mechanisms.
Current deterministic, symmetric deposition models differ primarily by the implementation of different morphometric lung models and analytical deposition equations developed for specific fluid dynamics profiles. Starting with the pioneering effort of Findeisen,(30) subsequent developments by Yeh and Schum,(3) Hofmann and colleagues(31) and Martonen,(32) among others, reflect the ever-increasing availability of more detailed morphometric information on lung structure and airway dimensions and more realistic analytical deposition equations.
The major practical advantage of such single or typical path models is their geometric simplicity because a single average path does not require detailed knowledge of the branching structure and the ventilation of the lung. However, this morphometric simplicity limits the application of such models for the prediction of realistic deposition patterns in asymmetric and variable lung structures.
Deterministic asymmetric generation or “multiple-path” model
Multiple-path models are more realistic than single-path models because they are based on actual measurements of single airways and their branching structure rather than on average values. In the multiple-path particle deposition (MPPD) model of Asgharian and co-investigators,(5) the bronchial airway geometry is represented by structurally different multiple-path models derived from the stochastic lung model.(5,10) These bronchial trees were either supplemented by attaching identical acini to each terminal bronchiole(3) or by the stochastic alveolar model.(11) Since the MPPD model considers the branching asymmetry of airways and related flow rates, it permits the calculation of lobar deposition, which cannot be predicted by symmetric lung models.
At an airway bifurcation, the airflow in each asymmetrically branching airway is assumed to be proportional to its distal volume and is computed by a procedure known as “tree traversal.”(33) For each airway of the lung, particle concentrations as a function of time are determined for the proximal and distal ends. Knowing the concentration of particles at the proximal end of an airway, the concentration at its distal end is calculated by considering the deposition efficiencies for the various deposition mechanisms.
The main advantages of such multiple-path models over the commonly used symmetric models are that exact solutions of the mass balance equations can be obtained in a realistic, i.e., asymmetric lung structure, and the asymmetry of the lung geometry allows the determination of intrasubject variations in individual airway generations or lung regions, and among different lobes.
Stochastic asymmetric generation or “stochastic multiple-path” model
A fully stochastic deposition model, simulating the trajectories of single particles was originally developed by Koblinger and Hofmann(10) and Hofmann and Koblinger(15) and further extended by Hofmann and coworkers.(11,18,34,35) In the stochastic particle deposition model IDEAL (
The main favorable feature of a stochastic deposition model is the application of a realistic lung structure in terms of dimensional variability and branching asymmetry, which allows the calculation and quantification of the distributions of deposition fractions due to intra- and intersubject variability, rather than only related average values.
Single-path CFPD model
While the above deposition models utilize analytical deposition equations for straight and bifurcating tubes, CFPD methods allow the simulation of the random paths and deposition of individual particles in bronchial airways(36–42) under realistic flow conditions. For example, Zhang and coworkers(42) simulated deposition of micron-sized particles in a bronchial airway model consisting of a sequence of parallel adjustable triple bifurcation units based on Weibel's lung model.(2) Computed generational deposition fractions agreed very well with predictions obtained with analytical deposition equations, although considerable differences were observed for local deposition patterns. A more realistic bronchial airway model was developed by Tian and colleagues,(43,44) based on the Yeh and Schum model,(3) considering also branching asymmetry and gravity angles, coupled to a mouth-throat model.
The apparent advantage of CFPD models over analytical deposition models is the consideration of realistic flow conditions and individual particle trajectories, which allow the calculation of localized deposition patterns. On the other hand, the primary limitation of such models is that they are currently restricted to inspiratory deposition in the bronchial tree, excluding deposition in the alveolar region and in the bronchial airways during expiration.
Regional Deposition Patterns
Regional particle deposition in human lungs is commonly expressed in terms of deposition fractions during a single breath, defined as the deposition efficiency for a given airway generation, multiplied by the fraction of inhaled particles reaching that generation. Deposition fractions may be related either to the inhaled number of particles (number deposition) or to the inhaled mass (mass deposition). Furthermore, they may be normalized to the entrance of the trachea, if only the relative distribution within the lungs is required, or to the entrance of the nose or the mouth, if absolute values and/or the distribution within the whole respiratory tract is needed.
Current deposition models can predict the following regional deposition quantities relevant for the administration of medical aerosols in the lung: 1) regional bronchial and alveolar deposition, 2) generational lung deposition, 3) lobar deposition, 4) generational lobar deposition, and 5) generational surface deposition. Results of such deposition calculations are illustrated in Figures 1–6.
Regional bronchial and alveolar deposition
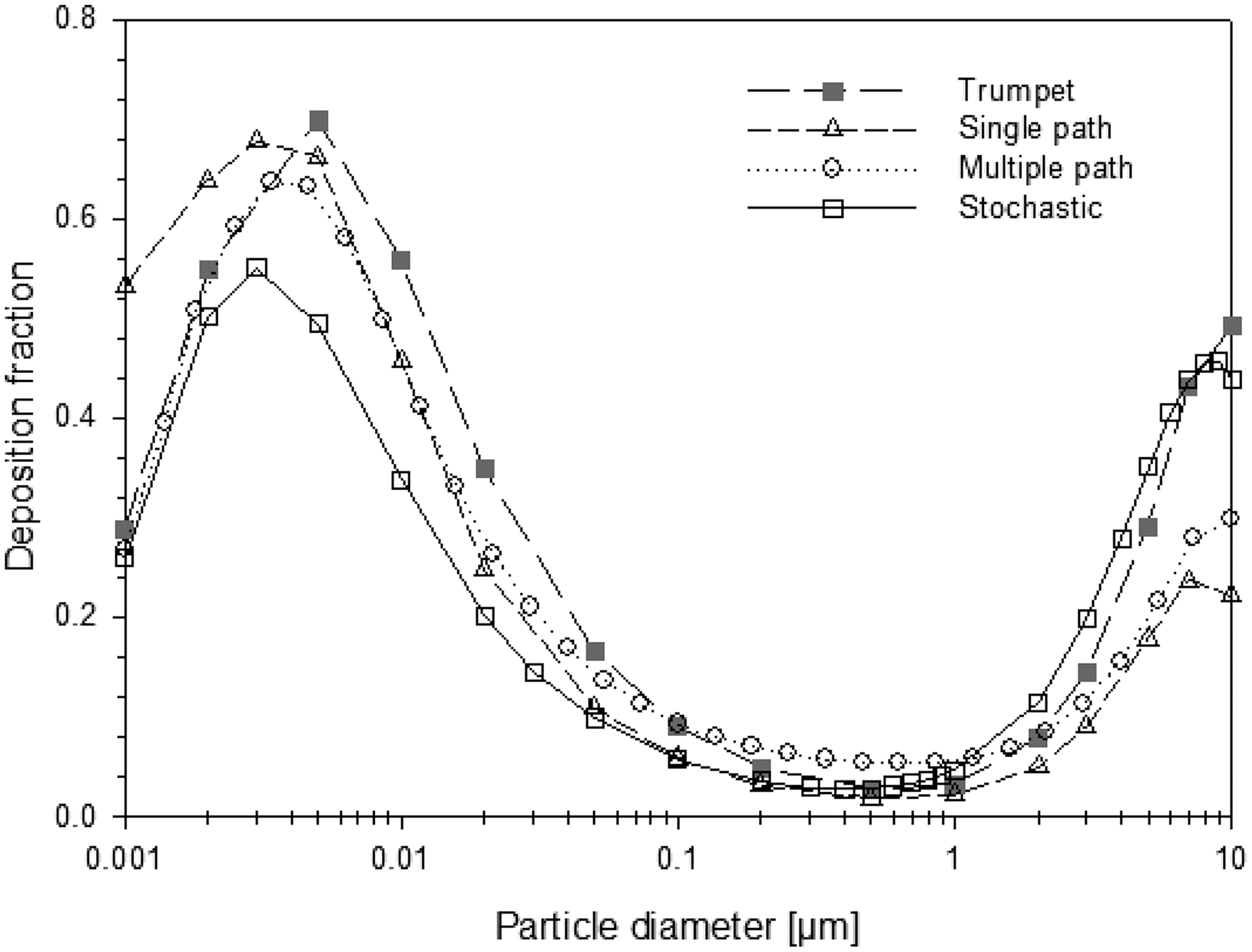
Deposition fractions of unit density particles, ranging from 1 nm to 10 μm, in the bronchial region predicted by the different analytical deposition models discussed in the preceding section are plotted in Figure 1 for sitting physical activity(1) of an adult male inhaling through the mouth (f = 12 min−1 and VT = 750 ml).
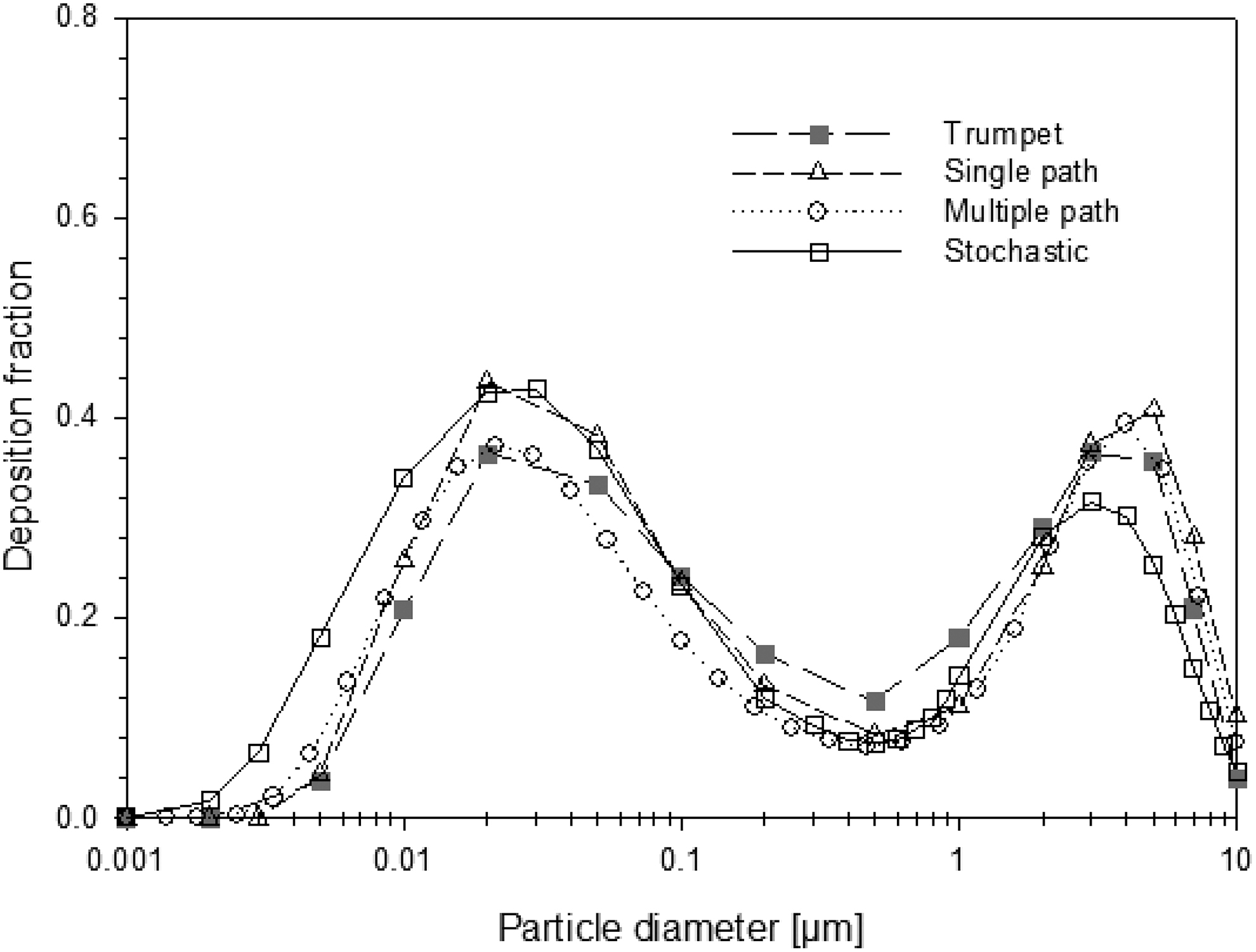
Deposition fractions in the bronchial region form a saddle-shaped curve with two peaks. Below the nano-sized peak and above the micron-sized peak, deposition fractions drop rapidly to smaller values due to the high extrathoracic filtering efficiency of small and large particles. Corresponding deposition fractions for the alveolar region are shown in Figure 2. Again, deposition in the alveolar region exhibits a saddle-shaped curve with two peaks. The apparent reduction of deposition fractions at very small and large particle diameters is caused not only by high extrathoracic deposition efficiencies but also by the relatively high TB deposition efficiencies for these particle sizes. Note that differences in nasal filtration efficiency equations are partly responsible for the observed differences in bronchial and alveolar deposition fractions among the various models. However, all models exhibit the same functional relationship with particle diameter.
Generational lung deposition
Distributions of deposition fractions of 2 μm unit density particles among bronchial and alveolar airway generations computed by the different analytical deposition models are illustrated in Figure 3 for sitting breathing conditions,(1) normalized to the number of particles entering the trachea. The shapes of the distributions indicate that most of the inhaled particles are deposited in the peripheral alveolated airways. Although deposition efficiencies increase upon penetration into the lung, the number of particles actually reaching these airways dramatically drops due to filtration in preceding airways. While all four analytical deposition models predict the same shape of the deposition curve, differences in the proximal and peripheral airways can be observed.
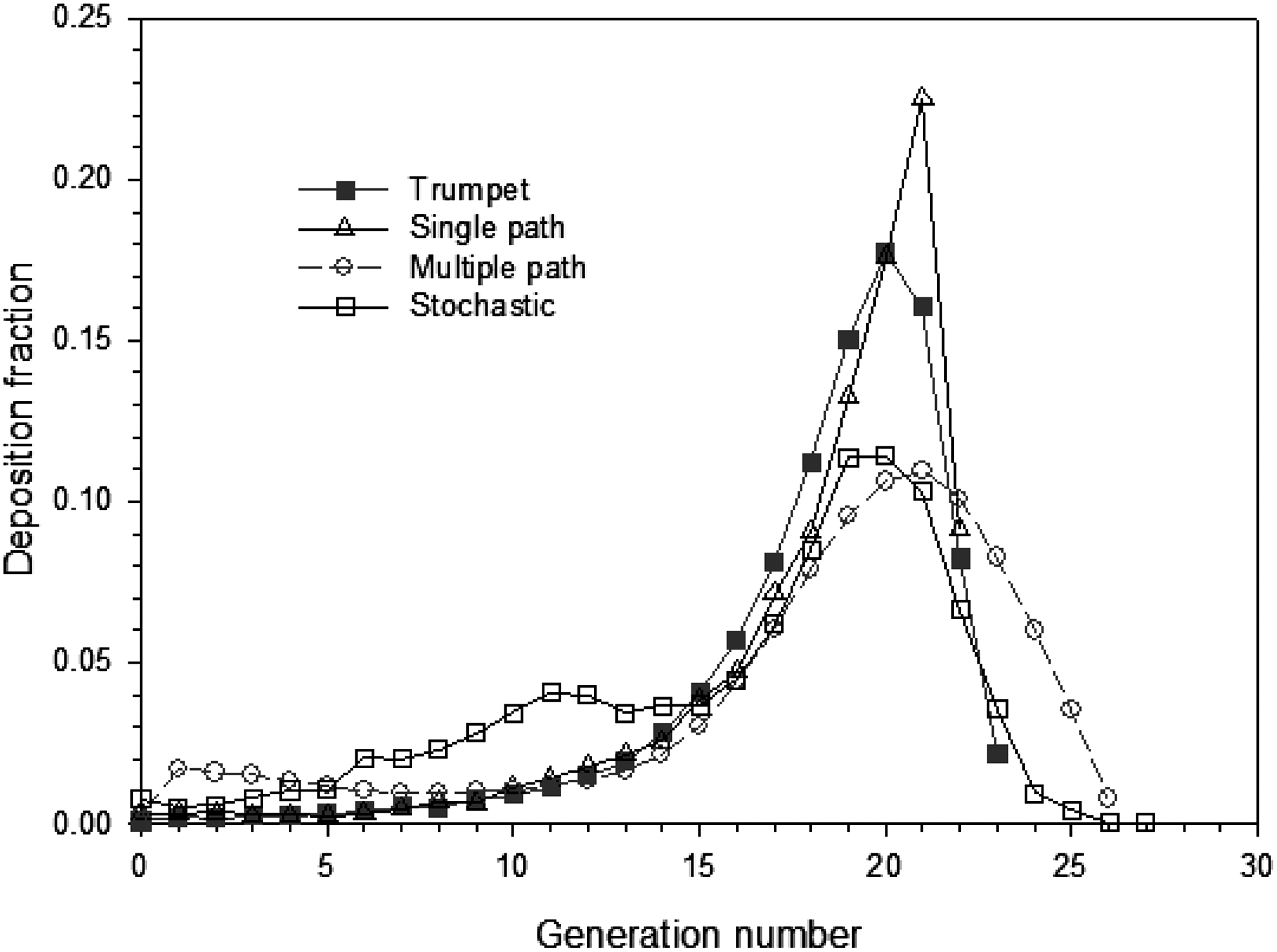
Comparison of model deposition fractions among human airway generations for the inhalation of 2 μm unit density particles under sitting breathing conditions, normalized to the number of particles entering the trachea, predicted by different analytical deposition models: trumpet,(16) single path,(31) multiple path,(5) and stochastic(10) (Note: all model predictions start with the trachea as generation 0).
Lobar deposition
Deposition fractions of inhaled 2 μm unit density particles among the five lobes of the human lung, calculated with the stochastic IDEAL deposition model, are plotted in Figure 4 for sitting breathing conditions,(1) normalized to the number of particles entering the trachea. Consistent with the U-shape of total and regional deposition,(25) the dependence of lobar deposition fractions on particle diameter follows the same pattern. Over the whole range of particle diameters, deposition fractions are significantly higher in the two lower lobes than in the two upper lobes and smallest for the right middle lobe. While this general pattern is consistent with their respective lobar volumes, differences between the lower and upper lobes and between the right lower lobe and the left lower lobe are not borne out numerically by their lobar volumes, indicating the effect of nonuniform lobar ventilation.
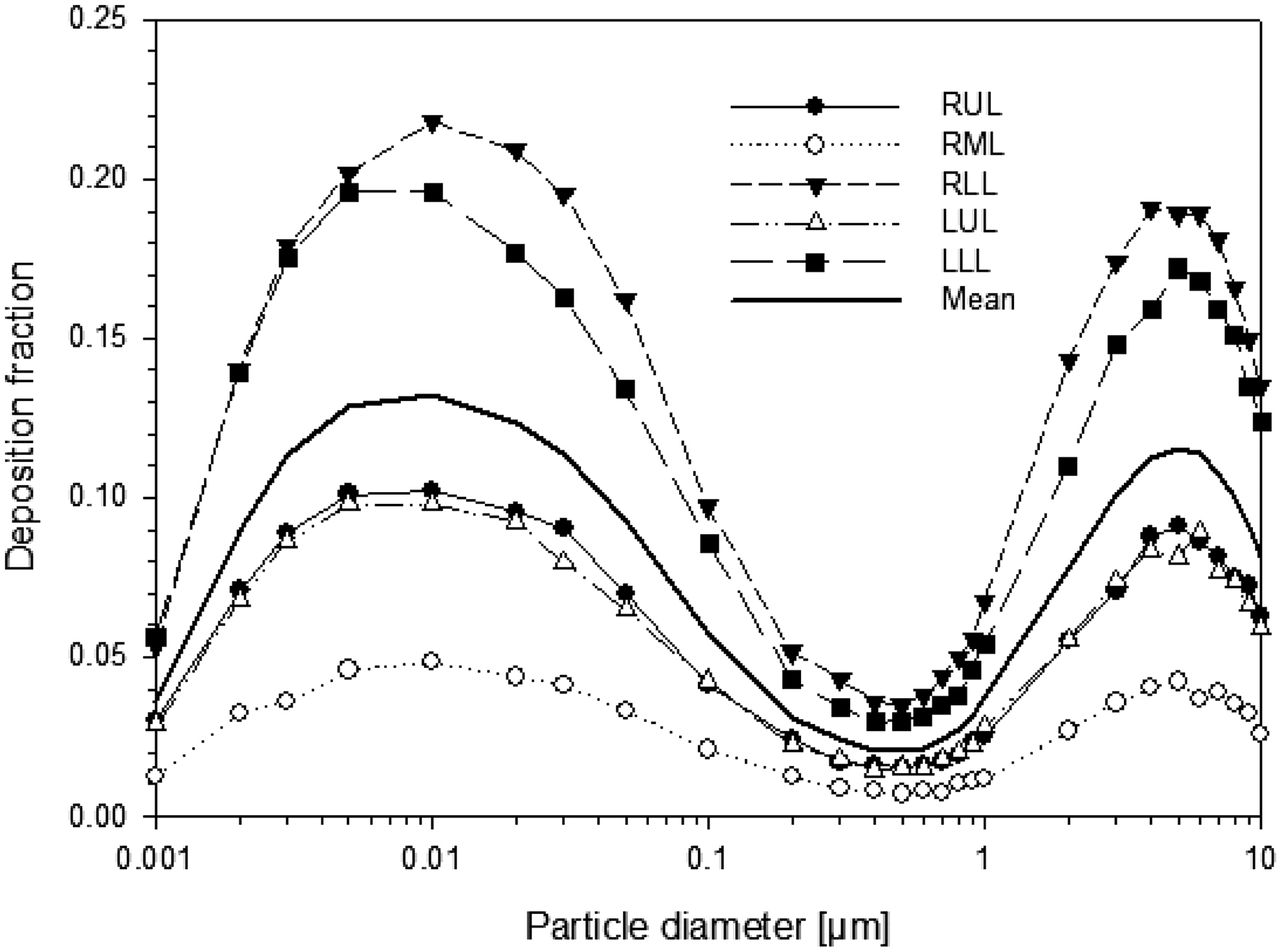
Deposition fractions of inhaled unit density particles, ranging from 1 nm to 10 μm, in the five lobes of the human lung for sitting breathing conditions and oral inhalation. RUL: right upper lobe, RML: right middle lobe, RLL: right lower lobe, LUL: left upper lobe, LLL: left lower lobe, Mean: average over all lobes.
Generational lobar deposition
Generational deposition patterns of 2 μm unit density particles within the different lobes, generated by the stochastic IDEAL deposition model, are plotted in Figure 5, corresponding to the deposition fractions shown in Figure 3. While lobar deposition fractions differ among the various lobes, consistent with the lobar deposition illustrated in Figure 4, their relative distribution among the airways of a given lobe is practically the same in all lobes. Differences in path lengths within each lobe are caused by differences in corresponding lobar volumes.
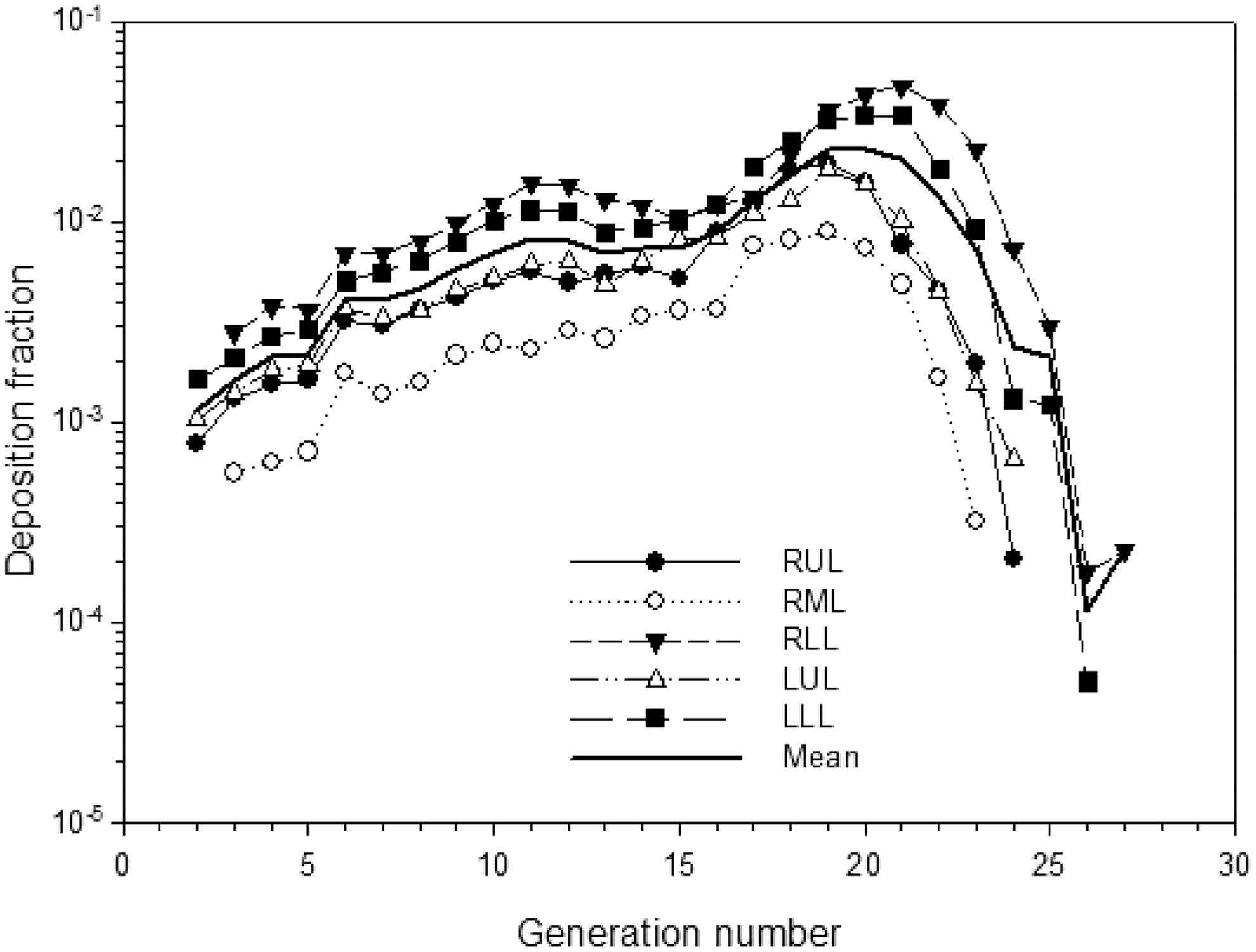
Lobar generational deposition fractions of 2 μm unit density particles under sitting breathing conditions, normalized to the number of particles entering the trachea. RUL: right upper lobe, RML: right middle lobe, RLL: right lower lobe, LUL: left upper lobe, LLL: left lower lobe, Mean: average over all lobes (Note: lobar airways start with generation 2 in the IDEAL model).
Generational surface deposition
For the inhalation of pharmaceutical aerosols, generational surface deposition (or “dose”),(35) obtained by dividing generational deposition fractions by the corresponding surface areas, may be more relevant than deposition fractions. Surface deposition fractions of 2 μm unit density particles in bronchial airway generations, computed with the stochastic IDEAL deposition model, are displayed in Figure 6 together with the corresponding deposition fractions. While deposition fractions steadily increase with penetration into the lung, surface deposition fractions continuously decrease throughout the bronchial tree due to ever-increasing airway surface areas (Table 1). Since initial deposition patterns are subsequently redistributed by mucociliary action, it might be necessary to combine generational deposition models with compatible mucociliary clearance models(45) to correctly predict surface concentrations of pharmaceutical aerosols.(46,47)
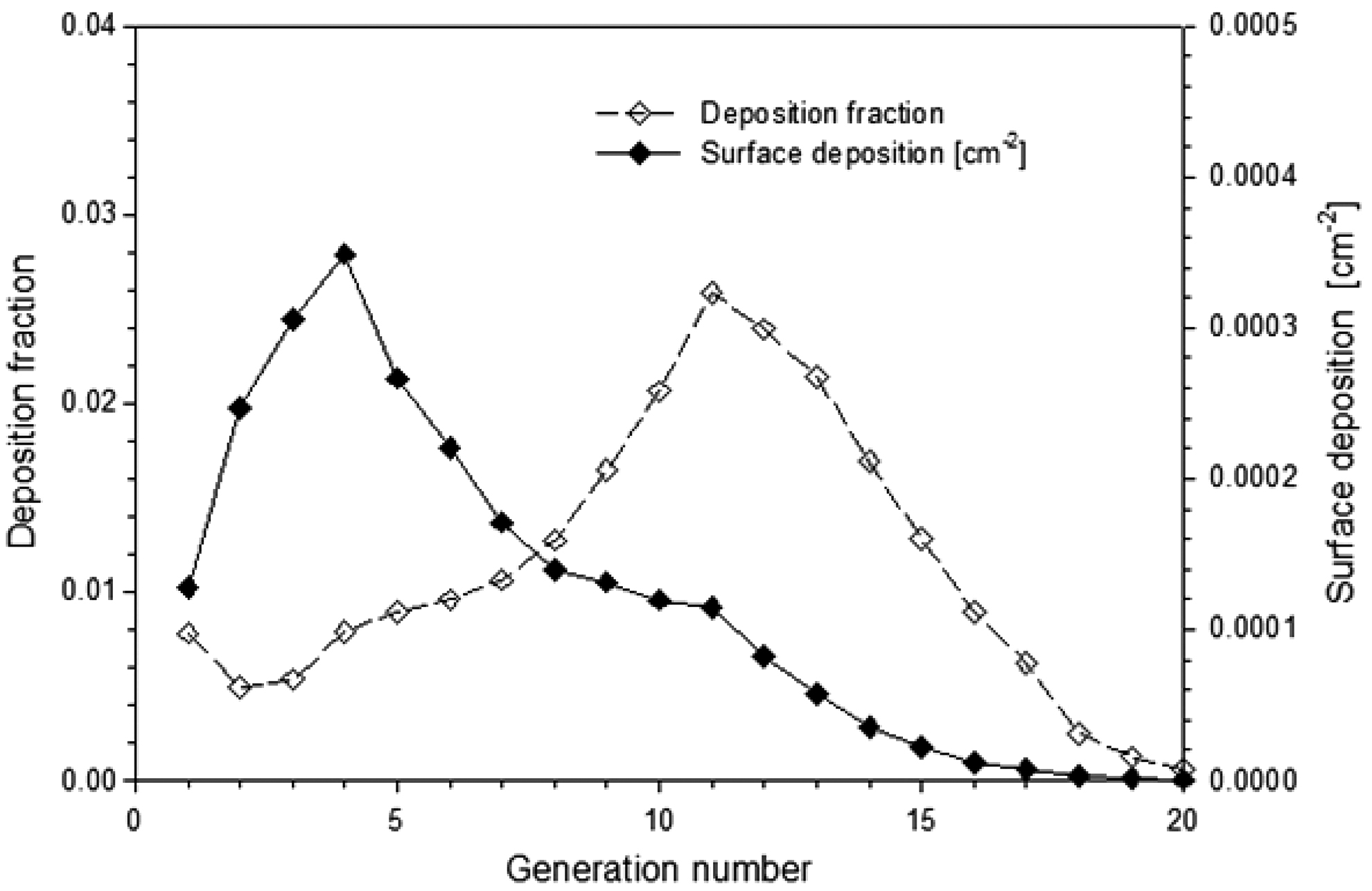
Generational surface deposition fractions and corresponding deposition fractions of 2 μm unit density particles in bronchial airway generations under sitting breathing conditions, normalized to the number of particles entering the trachea.
Model Validation
To ensure that particle deposition models correctly predict regional deposition, they must be validated by comparison with the available experimental evidence. At present, direct experimental in situ determination of particle deposition in human subjects is limited to total deposition, either inhaling through the mouth or the nose, for a wide range of particle sizes and flow rates.(1,25) However, total deposition is only of limited use for the verification or falsification of specific deposition models, as different generational or regional deposition fractions may fortuitously produce the same total deposition.
Regional, i.e., bronchial and alveolar deposition(1) as a function of particle size and flow rate can only be derived indirectly via subsequent retention measurements of radiolabeled aerosols,(1,48) attributing the fast-cleared fraction to TB deposition and the slow-cleared fraction to alveolar deposition.(48,49) An alternative experimental method to determine bronchial and alveolar deposition is the serial bolus technique,(50,51) where regional deposition is related to volumetric depths based on Weibel's(2) symmetric model A. Since these bronchial and alveolar deposition predictions hinge upon the application of a specific lung model, these data represent only semi-experimental information.
At present, particle deposition in specific airway generations cannot be obtained experimentally. However, there are two experimental approaches, which indirectly allow the experimental determination of deposition fractions in airway generations: 1) the serial bolus technique,(16,52) and 2) the three-dimensional reconstruction of radiolabeled aerosol deposition patterns measured by Single Photon Emission Computed Tomography (SPECT)(53,54) or Positron Emission Tomography (PET).(55,56)
Since generational deposition predicted by the serial bolus technique depends on the application of a specific lung model, and the measured SPECT and PET data are converted to deposition fractions in a series of concentric, semi-spherical shells, validated by post-imaging autoradiography in the large airways of the canine lung,(56) both data sets do not represent genuine experimental information.
In general, the overall agreement between the modeling predictions obtained by the various deposition models and the available experimental data indicates that current deposition models correctly predict regional deposition, although minor differences still exist(25) specifically in case of microgravity, where models consistently underpredict deposition.(57,58)
Limitations of Current Regional Deposition Models
The two major differences between the modeling predictions produced by the different deposition models are: 1) predicted deposition fractions depend on the selection of a specific morphometric lung model and a specific set of analytical deposition equations, although all models predict the same trends as functions of particle diameter and breathing parameters; and 2) only asymmetric multiple-path or stochastic morphometric lung models can predict deposition in different lobes and the variability of deposition fractions in individual airway generations and related regions or lobes.
Despite the documented success of the deposition models described above, the following limitations of current regional deposition models must be recognized: 1) models cannot, at present, be validated by comparison with experimental in vivo data at the single airway or airway generation level, although limited information can be obtained by the serial bolus technique(16,51) and by SPECT(53,54) and PET(55,56) data analysis; 2) most models do not consider the movement of airway walls, most pronounced in the alveoli, due to volume changes during breathing; 3) models typically use extrathoracic deposition equations obtained for normal breathing conditions, which may not be applicable to the specific flow conditions encountered in metered-dose and dry powder inhalers; and 4) analytical deposition models cannot provide information on deposition patterns within airways or airway bifurcations. The latter requires the application of CFPD models.(25,36–44)
Summary
Modeling particle deposition in the human lung requires the description of the morphological structure of the human lung as a sequence of bifurcating cylindrical tubes.
Five different regional deposition models are discussed in this section: 1) one-dimensional cross-section or “trumpet” model, 2) deterministic symmetric generation or “single path” model, 3) deterministic asymmetric generation or “multiple-path” model, 4) stochastic asymmetric generation or “multiple-path” model, and 5) single-path CFPD model.
Current deposition models can predict the following regional deposition quantities: 1) regional bronchial and alveolar deposition, 2) generational lung deposition, 3) lobar deposition, 4) generational lobar deposition, and 5) generational surface deposition.
Differences between deposition fractions predicted by the different models can be attributed primarily to the application of different morphometric lung models and of different analytical deposition equations.
The overall agreement between the modeling predictions obtained by the various deposition models and the available experimental evidence indicates that current deposition models correctly predict regional deposition, despite still existing minor differences, such as in the case of microgravity.
Footnotes
Acknowledgments
The author gratefully acknowledges the contributions of Renate Winkler-Heil, Bahman Asgharian and Chong Kim for providing results for the comparison of deposition fractions between of the different deposition models discussed in the text.
Author Disclosure Statement
The author declares that no conflicts of interest exist.