
Abstract
Background:
Inhaled drug delivery can be limited by heterogeneous dose distribution. An additive that would disperse drug over the internal surfaces of the lung after aerosol deposition could improve dosing uniformity and increase the treated area. Our previous studies demonstrated that surfactant additives can produce surface tension-driven (Marangoni) flows that effectively dispersed aerosol-delivered drugs over mucus surfaces. Here we sought to determine whether the addition of a surfactant would increase transport of an aerosol between lung regions and also improve dosing uniformity in human lungs.
Methods:
We compared the deposition and postdeposition dispersion of surfactant (10 mg/mL dipalmitoylphosphatidylcholine; DPPC) and saline-based liquid aerosols, admixed with Technetium 99m (Tc99m) diethylenetriaminepentaacetic acid, using gamma scintigraphy. Deposition images were obtained ex vivo in eight pairs of ventilated human lungs. The trachea was intubated and the mainstem bronchi were alternately clamped so that saline was delivered to one lung and then DPPC to the other (sides alternated). The lungs were continually imaged for 15 minutes during delivery. We assessed transport of the deposited aerosol by quantifying the percentage of Tc99m in each of four lung quadrants over time. We quantified dose uniformity within each lung quadrant by measuring the coefficient of variation (CV = standard deviation of the pixel associated radioactive counts/mean of the counts within each quadrant).
Results:
There was no change in the percentage of Tc99m in each quadrant over time, indicating no improvement in transport with the addition of the surfactant. The addition of surfactant was associated with a statistically significant decrease in CV in the lower inner lung quadrant at each of the three time points, indicating an improvement in dosing uniformity.
Conclusion:
These preliminary results indicate the possible utility of adding surfactant to aerosols to improve drug distribution uniformity to lower inner lung regions.
Introduction
Inhaled drug delivery can be valuable for treating the lung because it provides locally high concentrations of drug at sites of the disease. Aerosol conveyance and deposition are controlled by aerodynamics within the lung that may impose limitations for effective and uniform drug distribution.(1) Obstructive lung diseases can make it especially challenging to deliver drugs peripherally.(1–3) Partial obstructions in the airways can cause regions of high local aerosol deposition and decreased ventilation to downstream segments, limiting the delivery of inhaled medication to these zones. A drug additive that could improve the transport of an inhaled medication over the internal surfaces of the airways after aerosol deposition could improve distribution uniformity and possibly enhance the efficacy of the drug by providing therapeutic doses to more sites of the disease. This article expands upon previous research on using surfactant compounds as inhaled drug additives to generate surface tension-driven flows to disperse drug after aerosol deposition.(3–9)
Many lung diseases, such as asthma and cystic fibrosis, occur within airways that are lined with airway surface liquid (ASL). The ASL is composed of two layers: an ∼10 μm thick periciliary liquid layer that includes an aqueous layer that resides on the surface of the airway epithelium and contains active cilia, and a 10–70 μm thick viscoelastic mucus layer, typically composed of 95% water, 2% glycoproteins, 1% lipids, and 1% inorganic salts.(4,10–12) Marangoni transport is a surface tension-driven convective flow that occurs when a gradient in surface tension is present along an interface.(4,6) Marangoni flows can modify liquid flows on and near surfaces with only minimal variations in surface tension.(4,5) A shear stress along the interface is caused by the gradient, inducing a fluid motion from areas of low surface tension to areas of high surface tension, with a velocity proportional to the surface tension gradient.(4–6,13,14) Our previous studies have demonstrated that Marangoni flows can effectively and substantially disperse aerosol delivered drugs over porcine gastric mucus layers and primary human bronchial epithelial cells.(3,4,6–9,15) Other studies have measured the surfactant-based dispersion of drugs within the lungs of animals, generally demonstrating improved distribution, and in some cases, improved efficacy.(16–21)
To generate a Marangoni flow in the airways, the surface tension of the deposited aerosol would have to be lower than that of the airway surface.(6) Club cells on the airway surface produce endogenous lung surfactant proteins.(22) Endogenous surfactant produced within the alveoli may also enter the airways, possibly driven by Marangoni flows. Endogenous surfactant could potentially prevent or halt initial spreading of surfactant delivered by aerosol.(23,24) Only a very limited number of in vivo measurements of surface tension in the airways have been performed,(25) indicating values between that of pure water and the very low surface tensions found in the alveoli.(26) When selecting candidate surfactants, we sought compounds that provide low surface tensions and are likely to be safe in the lungs. Dipalmitoylphosphatidylcholine (DPPC) is a lipid surfactant that meets these criteria. DPPC is a component of endogenous lung surfactant and therefore is likely to be safe in the lungs. Our previous work showed that surface tensions as low as 1 nM/m can be attained when DPPC dispersions are atomized and delivered onto liquid surfaces.(15) Atomization deaggregates the multilaminar vesicles that are normally formed by DPPC allowing for the formation of a lipid monolayer at the liquid surface, which very effectively lowers surface tension. A radioisotope added to the preparation provides a drug analog that can be externally detected and quantified using nuclear imaging cameras.(27) In this study we used gamma scintigraphy to compare the postdeposition transport and distribution uniformity of aerosols containing the radioisotope Technetium 99m-diethylenetriaminepentaacetic acid (Tc99m-DTPA) and either DPPC + saline or saline alone in ex vivo lungs. To our knowledge this represents the first use of ex vivo human lungs for aerosol deposition studies. Ex vivo human lungs provide realistic architecture and allow for the testing of solutions with unknown safety.
The goal of these studies was to determine whether adding a surfactant to a nebulized medication would increase drug transport and the uniformity of drug distribution within human lungs. We assessed transport of the deposited aerosol by quantifying the radioactive counts in each of four lung quadrants over time. We assessed dose uniformity by measuring the coefficient of variation (CV) of the radioactive counts within each quadrant over time. An additive that improved transport of an aerosolized drug over the internal surfaces of the lung by spreading aerosol away from initial sites of deposition and improved uniformity of distribution on the lung surface could potentially improve the overall efficacy of the treatment.
Materials and Methods
General
We compared the deposition and postdeposition dispersion of 10 mg/mL DPPC and 0.9% saline-based liquid aerosols using deposition scintigraphy in ex vivo ventilated human lungs. A small amount of the gamma emitter Tc99m-DTPA in saline was added to both solutions as a small molecule drug analog. The lungs were intubated and mainstem bronchi were alternately clamped so that saline was delivered to one lung and then DPPC was delivered to the other. Gamma camera imaging was used to depict and quantify regional aerosol delivery and distribution over a 15-minute period, during and after aerosol delivery. Then, computed tomography (CT) images of the lung pairs were acquired to document the absence, or presence, of lung disease. Eight lung pairs were studied. Each pair was used for a single experiment. In four pairs, DPPC was delivered to the left lung and saline was delivered to the right. In the other four pairs, DPPC was delivered to the right lung and saline was delivered to the left.
Solutions
The saline solution included 1 mCi (37 MBq) of Tc99m-DTPA in a total volume of 4 mL in the nebulizer. The surfactant solution included 1 mCi Tc99m-DTPA in a minimal volume of saline (1 mL or less) with 10 mg/mL DPPC suspension added to a total volume of 4 mL. The DPPC was obtained from Avanti Polar Lipids (Alabaster, AL) in the lyophilized form (>99% purity). This concentration was selected based on previous successful in vitro experiments. DPPC suspensions were vortex mixed for 30 seconds within an hour of the experiment.(15) Water for the DPPC suspensions was ultrapurified to 18 MΩ cm resistivity by a Barnstead Nanopure Diamond system (ThermoFisher, Pittsburgh, PA). Tc99m-DTPA solutions were produced by the local Cardinal Health Radiopharmacy (Pittsburgh, PA). Tc99m-DTPA was added to the DPPC solution in the nebulizer immediately before delivery.
Ex vivo lungs
The experiments included left and right lungs with the mainstem bronchi intact and with partial tracheas. Lung pairs used were removed from donors for use in lung transplantation but, for unknown reasons, were found to be unsuitable upon arrival at the center. The lungs were stored under refrigeration until preparation could be made for the experiments (usually within 24 hours). The lungs had no known disease, which was verified through examination of the organs and a CT scan. The lungs were not perfused. Ahead of the experiment, the lungs were intubated and ventilated for 30 minutes. Normal saline was nebulized into the lungs during this ventilation period with ∼10 mL delivered over ∼20 minutes. We speculated that this would help to ensure normal hydration of the airway surfaces after the storage period. The lungs were positioned on a hard-plastic surface on the gamma camera cot during aerosol delivery and imaging. The chest wall was not simulated. The protocol was approved by the University of Pittsburgh Committee for Oversight of Research and Clinical Training Involving Decedents (CORID).
Aerosol delivery and imaging
Volume controlled ventilation was used during testing. A clamp was placed on the mainstem bronchus so that only one lung was ventilated at a time. A Nellcor Puritan Bennett 840 Ventilator (Medtronic, Minneapolis, MN) was used. Ventilator settings were adjusted until the ventilated lung appeared to fully inflate and then deflate to a consistent volume based on visual inspection. Single-lung tidal volumes ranged from 165 to 300 mL at respiratory rates of 7–10 breaths/min and peak flows (Vmax) of 14.5–19.9 L/min. Saline + Tc99m-DTPA was delivered to the ventilated lung for 15 minutes during continuous imaging and then the clamp was switched, and DPPC + Tc99m-DTPA was delivered to the other lung for 15 minutes during continuous imaging. Aerosol was generated using an Aerogen Solo nebulizer (Aerogen, Galway, Ireland) placed in the inlet vent line and run continuously. The imaging system used was a GE Discovery 630 SPECT/CT (GE Healthcare, Chicago, IL). Dynamic planar imaging was performed first that included 15 sequential 1-minute images from both the anterior and posterior gamma camera heads, then a CT scan was acquired. Particle size distributions for solutions containing DPPC + saline + Tc99m-DTPA and saline + Tc99m-DTPA were not determined, but the volume median diameters of 10 mg/mL DPPC and 0.9% saline solutions delivered with the Aerogen nebulizer were previously reported as being 5.7 ± 0.1 and. 4.3 ± 0.1 μm, based on laser diffraction measurements.(15)
Image analysis and statistics
Image analysis was performed using ImageJ (NIH, Bethesda, MD). Posterior images of both the right and left lung were used for primary analysis. Region of interests (ROIs) were generated using the Tc99m-DTPA images by encompassing the whole lung perimeter with a box (based on visual observation) and quartering that box into 4 rectangular quadrants: upper inner, upper outer, lower inner, and lower outer. Quadrant ROIs were created by copying the original outline box and then moving its perimeter lines to shrink the box to half its height and half its width. See Figure 1 for an illustration of the quadrants. The ROIs were used to determine the regional radioactive counts at each time point of the imaging period. Radioactive counts were corrected for radioactive decay based on the time of the first image. No background correction was performed. In comparing the regions, time points of early, middle, and late were created. The time points correspond to the average of early, 1–4 minutes; middle, 6–9 minutes; and late, 11–14 minutes, images.

Posterior gamma camera images showing aerosol delivery of saline + Tc99m-DTPA to the left lung at t = 3 minutes
Transport between quadrants and distribution uniformity of the saline and DPPC aerosols were quantified by analyzing the gamma camera images collected over a 15-minute time period during aerosol delivery. The effect of the DPPC additive on drug transport was determined by comparing the dose percentage in each quadrant, with and without surfactant, over time. Dose percentage (dose %) was calculated at each time point as the number of counts in each quadrant divided by the total number of counts in all four quadrants. Changes in dose percentage over time indicated transport between quadrants. Similar dose percentages between quadrants over time indicated lack of transport. The effect of the DPPC additive on dose uniformity within the quadrants was determined by comparing postdeposition CV with saline versus DPPC. CV was calculated at each time point as the standard deviation of the pixel-associated radioactive counts in each quadrant divided by the mean of the counts in the quadrant. A lower CV indicated more uniform distribution of the radiolabel within the quadrant.
Comparisons were made between averaged dose % and CV values for DPPC and saline by quadrant, over time, and between matched quadrants on the same testing day (right vs. left, saline vs. DPPC) (n = 8 lung pairs). Hypothesis testing was conducted using p-values determined from Wilcoxon matched-pairs signed-ranks test (paired, nonparametric) (STATA, College Station, TX). Values of p < 0.05 were considered statistically significant.
Results
Figure 1 shows representative posterior gamma camera images depicting the deposition of saline + Tc99m-DTPA aerosol in the left lung over 15 minutes (A–C) followed by the deposition of DPPC +Tc99m-DTPA in the right lung over 15 minutes (D–F). The different colors represent different numbers of radioactive counts with white being the highest followed by orange, green, and blue. The final panel approximates the four quadrants used for analysis. Increased aerosol deposition was apparent in the endotracheal tube and what are assumed anatomically to be larger airways.
Figure 2 compares the average dose percentages by quadrant for the saline versus DPPC aerosols over time. The highest dose percentages were in the upper inner quadrant. Average values for the eight lung pairs at each time point were used. Rapid changes in dose percentage occurred during the first 3 minutes of delivery. However, from t = 3–15 minutes, no quadrant changed on average by >4% with saline or surfactant, indicating no significant transport of drug between quadrants during that time period.
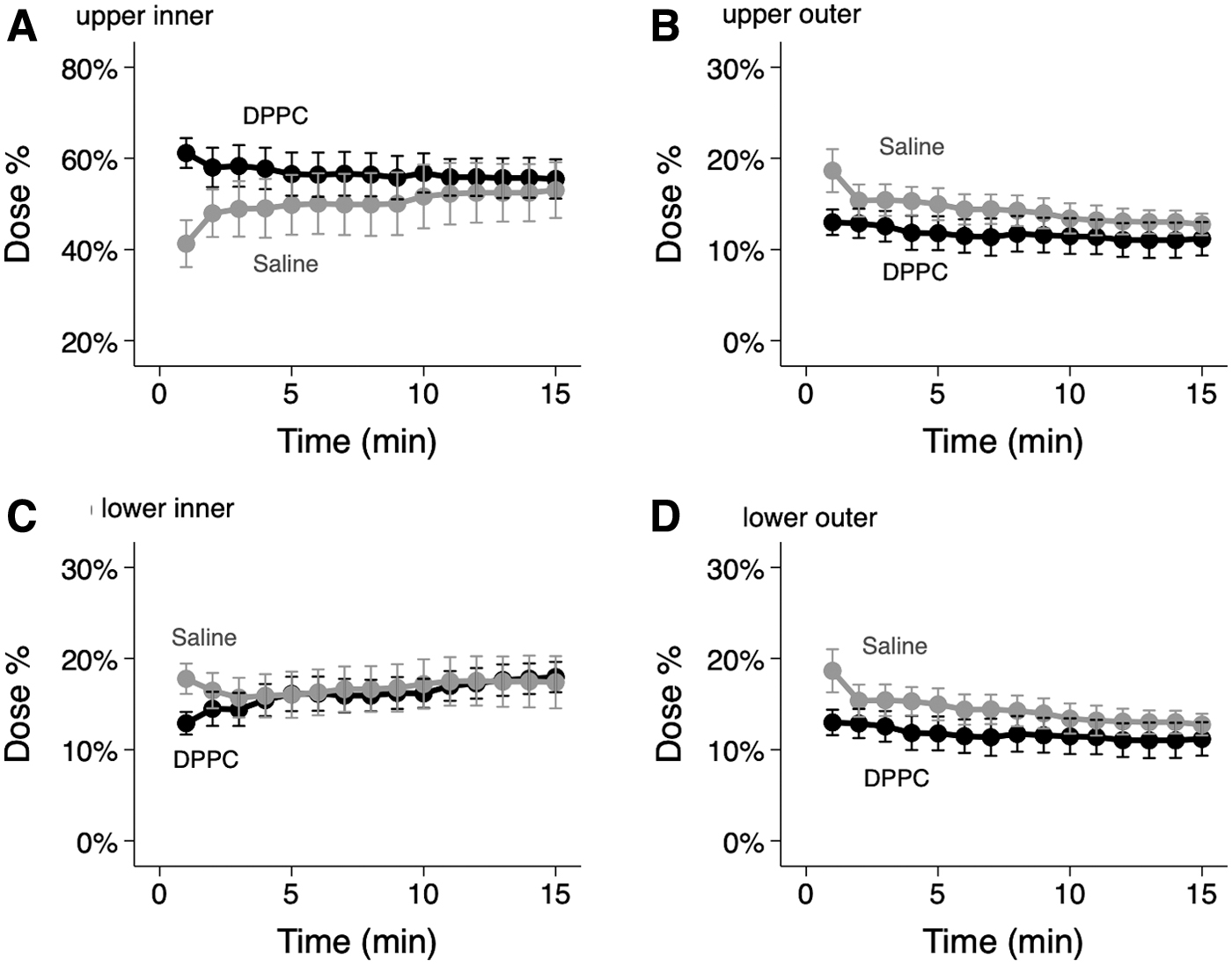
Average dose percentage by region over time. Dose percentage is the sum of the radioactive counts in each quadrant divided by the sum of the counts in all quadrants at that time. Average values for the eight lung pairs at each time point are used. Error bars are standard error of the mean.
Figure 3 compares dose percentages by quadrant within individual lung pairs. Here the p-values were calculated by comparing the dose percentage for DPPC with that of saline in the same quadrant of the opposite lung at early, middle, and late time points. A high p-value would indicate similar percentages of the total deposited dose in matched quadrants for DPPC and saline. Decreases from high-dose quadrants and increases in low-dose quadrants would be anticipated if DPPC was causing significant redistribution. Here there were no significant differences in distribution between the four quadrants with DPPC versus saline at any time point, except for the early time point in the upper outer quadrant that is driven by a single measurement. Taken together these data indicate that DPPC did not cause significant postdeposition transport of Tc99m-DTPA between quadrants during the study period.

Dose percentage by quadrant at early, middle, and late time points. Saline + Tc99m-DTPA was delivered to one lung and DPPC + Tc99m-DTPA was delivered to the other. Paired quadrants were compared. The time points correspond to the average of early, 1–4 minutes; middle, 6–9 minutes; late, 11–14 minutes after the start of aerosol delivery. Saline is left (first point). DPPC is right (second point). If dose percentage is higher with saline, a gray line is used. If dose percentage is higher with DPPC, a black line is used. Hypothesis testing was conducted using p-values determined by Wilcoxon matched-pairs signed-ranks test (paired, nonparametric).
Figure 4 compares the average CV by quadrant for the saline versus DPPC aerosols over time. CV decreased with time for both aerosols in all quadrants. The decrease in CV was greatest within the first 5 minutes. Decreases in CV indicate that pixel values of radioactive counts within the quadrant were more similar relative to the mean—an indication of increased dose uniformity within the quadrant. Average values for the eight lung pairs at each time point were used.
Average CV by region over time. CV is the standard deviation of the radioactive counts associated with each pixel in the quadrant divided by the mean of the counts in the quadrant. A lower CV indicates more uniform distribution of radioactivity. Error bars are standard error of the mean. CV, coefficient of variation.
Figure 5 compares CV by quadrant within individual lung pairs. Here the p-values were calculated by comparing the CV value for DPPC with that of saline in the same quadrant of the opposite lung at early, middle, and late time points. Lower CV values were associated with increased dose uniformity within that quadrant. Values of p > 0.05 indicated similar levels of dose uniformity with DPPC versus saline aerosols. There were no differences in dose uniformity between the two aerosols in the lower and upper outer quadrants. DPPC was associated with significantly deceased CV (i.e., increased dose uniformity) at all time points in the lower inner quadrant (early: p = 0.01, middle: p = 0.02, and late: p = 0.02). In the upper inner quadrant, the DPPC aerosol was associated with a significant decrease in CV at the middle time point only (p = 0.02).
CV by quadrant at early, middle, and late time points. Saline + Tc99m-DTPA was delivered to one lung and DPPC + Tc99m-DTPA was delivered to the other. Paired quadrants were compared. The time points correspond to the average of early, 1–4 minutes; middle, 6–9 minutes; and late, 11–14 minutes after the start of aerosol delivery. Saline (SAL) is left (first point). DPPC is right (second point). If CV is lower with DPPC (improved uniformity), a gray line is used. If CV is higher with DPPC (decreased uniformity), a black line is used. Hypothesis testing was conducted using p-values determined by Wilcoxon matched-pairs signed-ranks test (paired, nonparametric).
Discussion
Previous studies have demonstrated that Marangoni flows can be induced through the delivery of surface tension-lowering (surfactant) additives in an aerosol and that these flows can increase the treated area reached by a drug or drug analog delivered in the aerosol. These studies were conducted in in vitro simulations of airway surfaces(3,7–9,15) or in small animals.(16–20) Neither of these models are ideal. The in vitro surface models lack the complex architecture and the range of surface conditions that may be present within the lung, and the animal lungs do not accurately depict deposition in the human lung based on differences in airway size and specific anatomy. Therefore, there was reason to seek testing in human lungs. A small clinical study by our group that attempted to disperse radiolabeled particulate in the lungs of cystic fibrosis patients using an aerosolized surfactant replacement therapy included small numbers and was largely indeterminate.(28) In vitro studies performed after that clinical study provided much better guidance for selecting and delivering surfactants to the airways in a manner that could optimize spreading and those lessons were applied in this study.(9,15)
We measured the percentage of radioactive counts (dose) in four lung quadrants during delivery as an assessment of dose distribution. This distribution should vary by quadrant based on the relative ventilation and factors affecting aerosol deposition. A surfactant carrier that caused postdeposition transport over large length scales would be expected to make the dose percentage more uniform between quadrants over time. Dose percentage in the present experiments was highest in the upper inner quadrant, likely owing to increased impaction in the large airways caused by unusual aerodynamics resulting from the clamping of the individual lungs. Paired comparisons of dose percentage at three different time points (Fig. 3) showed that there were no significant differences between the saline and DPPC aerosols, indicating that there was no increase in postdeposition transport between quadrants with DPPC compared with saline.
CV is a measure of the uniformity of pixel-associated radioactive counts within each quadrant. More uniform distribution of radiotracer in the quadrant would be associated with a lower CV. Uniformity increased over time during aerosol delivery. Comparisons between saline and DPPC indicated significantly increased uniformity with the DPPC aerosol at all time points in the lower inner quadrant and at one of three time points in the upper inner quadrant (Fig. 5). Increased uniformity would be expected if DPPC was causing postdeposition dispersion over small length scales within the airways. Because dispersion is driven by surfactant gradients, this effect may have been more pronounced in the inner zones because they contain the large airways where heavy aerosol deposition often occurs over small areas. Such effects might be less pronounced in the outer zones where the DPPC aerosol was deposited over the larger surface area of the smaller airways. Additional research is needed to test this hypothesis. All quadrants contained alveoli where spreading may be limited by high concentrations of endogenous surfactant.
Limitations of these experiments included the time between lung removal and performance of experimentation (most typically 24 hours) and the lack of lung perfusion during this period. It is unknown how airway surface conditions may change during this period of cold preservation. Experiments were also performed at room temperature without warming the lungs to normal body temperature that may also affect surface conditions. The nuclear imaging techniques used did not provide absolute tracking of the drug analog. Such tracking could be performed using a fluorescent drug analog and precision slicing of lungs although careful technique would be required to prevent redistribution of the probe during processing. It is possible that that some amount of Tc99m-DTPA was absorbed into the epithelium after delivery making it unavailable for transport. We believe that the potential for this effect was minimized by not perfusing the lungs. The resolution provided by the nuclear imaging techniques was not sufficient to resolve differences in distribution within specific airway groups. The lungs were not substantially diseased and results from lungs harboring obstructive disease or infection could be quite different. Such lungs could potentially become available as lung explants and may be considered for future experiments. No aerosol sizing data were available for the exact combinations of saline, Tc99m-DTPA, DPPC, and saline used in these experiments. However, previous studies(15) demonstrated that the Aerogen nebulizer produced larger droplets with DPPC than saline (5.7 vs. 4.3 μm), which may have created differences in the initial deposition patterns of the aerosols. We tested only a single DPPC concentration in these studies, although this choice was based on significant in vitro study. Our study was also limited by small numbers based on the limited availability of lungs for testing in this pilot study.
The portion of airway surface area reached and treated with inhaled medications is largely unknown. The surface area of the small airways is particularly large. Both aerosol dosing and therapeutic effect are difficult to evaluate in this zone that has the potential to harbor latent infection, obstruction, or untreated inflammation. Techniques are available for targeting aerosol deposition to lung zones through specific combinations of aerosol size and breathing pattern,(29,30) but drugs delivered through conventional methods have no mechanism for dispersion over airway surfaces after deposition except for concentration-driven diffusion and mucociliary clearance, both of which occur over long time scales during which absorption is likely to occur. Previous studies on model airway surfaces demonstrated that liquid aerosols containing tobramycin and DPPC can rapidly and uniformly disperse over distances ∼8 cm even when the model surface includes an “endogenous” layer of DPPC.(9) This was likely a consequence of the very low surface tensions generated through the aerosolization techniques used both here and in our previous experiments, which are of the order 1–5 mN/m.(9,15) Although surface conditions in the small airways remain mostly unknown, the use of a very low surface tension additive increases the chances that useful dispersion can be attained. DPPC is also attractive as a candidate because it is the principal component of lung surfactant and thus has a limited potential for toxicity.
These preliminary studies indicated that a DPPC additive did not increase the dispersion of deposited aerosol between lung quadrants. DPPC did appear to increase dose uniformity consistently within one lung quadrant (lower inner). We speculate that this quadrant may have contained mostly larger airways with smaller surfaces areas that facilitated higher DPPC concentration gradients and more effective dispersion. Future experiments are likely to incorporate diseased lungs and fluorescent probes to allow for dispersion tracking within individual lung slices after sectioning.
Footnotes
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
National Heart, Lung, and Blood Institute (NHLBI) NIH R01 HL105470-01.
Reviewed by:
Beth Laube
Joseph Brain