
Abstract
Background:
Drug inhalation is common mode of treatment for chronic obstructive pulmonary disease (COPD). The aim of this study was to evaluate the efficiency of aerosol devices in a simulated COPD adult lung model using five commercially available hand-held mesh nebulizers.
Materials and Methods:
Five nebulizers (PARI VELOX®, Omron NE-U22, Aeroneb® Go, APEX PY001, and Pocket Air®) were tested with a unit dose of 5.0 mg/2.5 mL salbutamol. An in vitro lung model (compliance: 0.06 L/cm H2O, resistance: 20 cm H2O/L/sec) was constructed to simulate parameters (tidal volume of 500 mL, respiratory rate of 15 breaths/min, inspiratory time of 1 second) of an adult patient with COPD. A bacterial filter was attached at the bronchi level for drug collection, referring as inhaled mass. After nebulization, the inhaled mass (%), dose remaining on each component (%), particle size characteristics, and nebulizer performances were analyzed. Particle size characteristics were analyzed using an 8-stage Anderson Cascade Impactor. The salbutamol particles deposited were eluted and analyzed using a spectrophotometer at 276 nm. The inhaled mass (%), dose remaining on each component (%), particle size distribution, and nebulizer performance were statistically analyzed using analysis of variance (ANOVA) with Sheffee post hoc tests.
Results:
Pocket Air and APEX PY001 showed the greatest inhaled mass and the lowest dose in the mouthpiece connection. The largest and smallest mass median aerodynamic diameters were found with Omron NE-U22 and PARI VELOX, respectively. In addition, the output rate and inhaled aerosol rate (IAR) of PARI VELOX were higher than those of other nebulizers.
Conclusions:
This study showed that the performance of commercially available mesh nebulizers varied. Aerosol particles deposited on different auxiliary equipment directly influenced the output rate and IAR of the mesh nebulizer. Clinical validation of the drug IAR is necessary to avoid overdose and reduce drug wastage.
Introduction
According to the World Health Organization, ∼65 million people have chronic obstructive pulmonary disease (COPD) and it is estimated to become the third leading cause of death by 2030.(1) COPD involves high treatment costs when hospital care is required, and incurs economic losses owing to disability and incapacity.(2) Drugs inhalation is often necessary,(3) and shows a rapid onset and higher therapeutic index.(4,5) Therefore, choosing an appropriate inhalation device is a critical clinical consideration.(6)
Current commercial nebulizers are classified into three main categories: (1) jet nebulizers (JNs), (2) ultrasonic nebulizers, and (3) vibration mesh nebulizers (VMNs).(7,8) The main disadvantage of JNs and ultrasonic nebulizers is the large proportion of residual dose. Other common problems include noise generated by JNs and degradation of the drug by heated aerosols in ultrasonic nebulizers.(2,9,10)
The key technology of the VMN is a central aperture plate perforated with several hundred to several thousand precisely formed holes, the hole size can be adjusted according to the clinical requirements.(5,11,12) They are efficient, generate less noise, require short usage time, have minimal residual volume (<0.2 mL), comply with active drug compounds without produce heat,(13) and are portable (battery operated).(9,10,12,14)
Ari et al. compared the inhaled mass % of a VMN with a JN in a simulating adult breathing model. Drug delivery was shown to be greater for the VMN than JN when using a mouthpiece or a valved mask; however, it was similar when using an aerosol mask.(15) Hickin et al. also reported that the VMN delivered salbutamol at a significantly higher rate than the JN in a simulated adult COPD model.(16) In a human study, Alcoforado et al. compared radio-aerosol (99m Tc-DTPA) using VMN or JN with mouthpiece in spontaneously breathing healthy volunteers. They found that the VMN achieved greater pulmonary deposition efficiency than the JN.(17)
Hand-held VMN, such as the PARI eFlow® and Aerogen Ultra®, incorporates a mouthpiece or aerosol mask for spontaneous breathing patients.(15,18,19) However, evidence regarding delivery efficiencies of VMN using different interfaces, especially the mouthpiece in adults with spontaneous breathing, is limited. The purpose of our study was to evaluate the performances of different commercial hand-held VMN in a simulated adult COPD lung model through a mouthpiece readily available in the market.
Materials and Methods
Lung model
The in vitro lung model consisted of a teaching mannequin (Laterdal Airway Management Trainer; Laerdal Medical®/Stavanger, Norway) with an upper airway that was attached to a collecting filter (VADI Medical Technology Co., Taoyuan, Taiwan) at the bronchi level.(20,21) A dual-compartment passive test lung (Michigan Instruments, Inc., Grand Rapids, MI) consisting of two compartments connected with a clip and a breath-simulation module, which inflates one compartment that lifts the other compartment, simulating a spontaneous breathing pattern (Fig. 1). The model was set to simulate parameters of an adult patient with COPD as follows: tidal volume of 500 mL, respiratory rate of 15 breaths/min, inspiratory time of 1 second, lung compliance of 0.06 L/cm H2O, and airway resistance of 20 cm H2O/L/sec.(22)

Experimental apparatus set-up of the study using the vibrating mesh nebulizer.
Delivery system
Five new mesh nebulizers, with their own design mouthpieces, were chosen for testing: (1) PARI-VELOX® (PARI Medical Limited, West Byfleet, United Kingdom), (2) Pocket Air® Portable Nebulizer (Microbase Technology Corp., Taoyuan City, Taiwan), (3) APEX PY001 mesh portable nebulizer (Apex Medical Corp., New Taipei City, Taiwan), (4) Aeroneb® GO (Aerogen Ltd., Galway, Ireland), and (5) Omron NE-U22 (Omron Healthcare, Ltd, Milton Keynes, United Kingdom). A standard unit dose of salbutamol sulfate (GlaxoSmithKline, Victoria, Australia), containing 5.0 mg in 2.5 mL, was placed into the drug reservoir without further dilution. Nebulization time was recorded when no visible aerosol could be seen. The mouthpiece of the nebulizer was securely attached to the mouth of the teaching mannequin to minimize leakage. All experiments were performed using the same nebulizers and were repeated five times. (n = 5).
Measurement of drug delivery and nebulizer performance
Salbutamol sulfate deposited in the collecting filter, drug reservoir, mouthpiece, and mouthpiece connection (the space where the mouthpiece is connected to the nebulizer, or the aerosol reservoir chamber of PARI VELOX and Aeroneb GO) (Fig. 2) were eluted using distilled water, with gentle shaking for 3 minutes. All samples were measured using an ultraviolet spectrophotometer (ThermoFisher Scientific, Inc., Waltham, MA) at a wavelength of 276 nm. The drug concentration in the sample solution was calculated from the absorption–concentration standard curve (R2 = 0.9999). Because of the difference of nebulization time, we calculated the inhaled aerosol rate (IAR; defined as the inhaled mass in percentage divided by nebulization time) for the drug delivery capacity per unit of time.(23) In addition, output rate (defined as the mass of drug and determined by weighing the nebulizer before and after use) converted to aerosol per unit time was calculated.
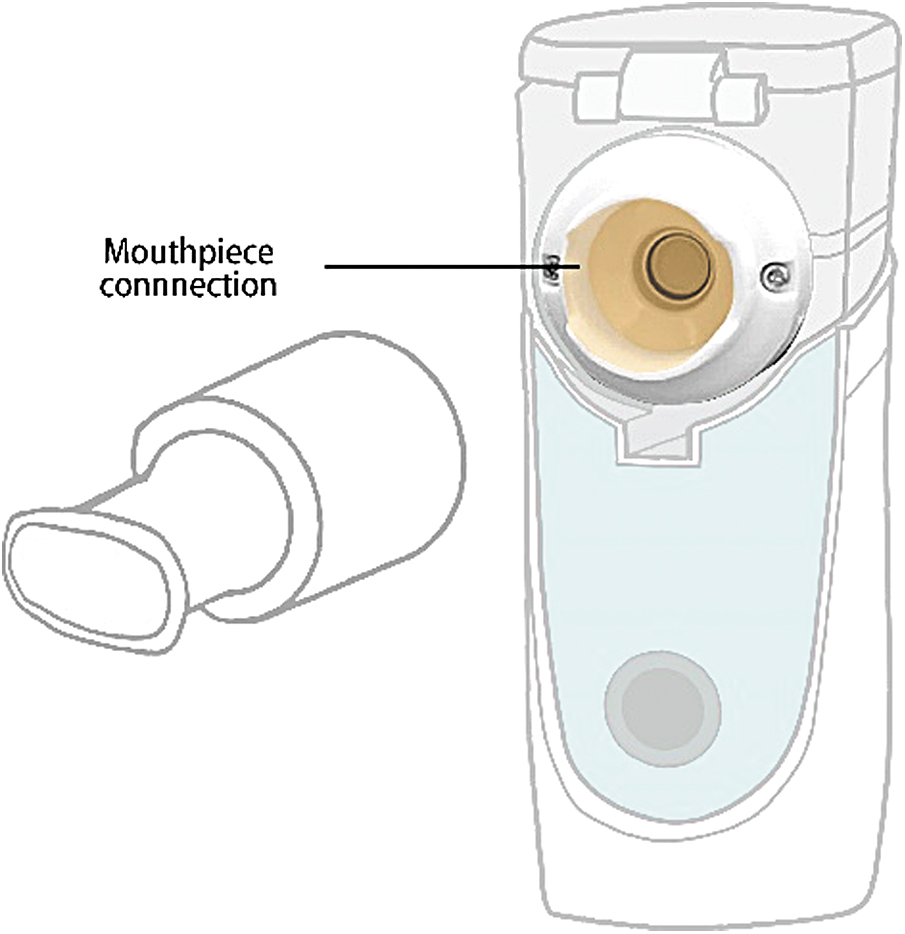
Mouthpiece connection (light orange color) of a nebulizer. Color images are available online.
Measurement of aerosol particle size
The mass median aerodynamic (MMAD) and geometric standard deviation (GSD) were determined from the amount of drug deposited on the impactor plates and the throat using an 8-stage Andersen Cascade Impactor (ACI; Thermo Fisher Scientific, Inc.), at an air flow of 28.3 L/min for each nebulizer. Before each test, the vacuum flow was validated using a flowmeter (TSI Inc., Shoreview, MN). The nebulizers were placed at the inlet of the throat, and operated until no aerosol was visible (n = 5). The ACI was disassembled after each test, and the drug mass was eluted from the throat and each stage with 10 mL of distilled water, followed by gentle shaking for 3 minutes. The MMAD, GSD, fine particle fraction (FPF%, 0.43 to 4.7 μm), and coarse particle fraction (CPF%, 5.8–9.0 μm) were calculated using the Copley Inhaler Testing Data Analysis Software v3.10 (Copley Scientific Ltd, Nottingham, United Kingdom).
Statistical analysis
Statistical analyses were performed using SPSS version 22.0 (SPSS, Inc., Chicago, IL). The mean ± standard deviation was calculated for each component of the drug mass eluted from the collecting filter, drug reservoir, mouthpiece, and the mouthpiece connection as well as the nebulization time. A one-way analysis of variance (ANOVA) with the post hoc test was carried out to identify differences within groups for continuous variables, and p < 0.05 was used to indicate statistical significance.
Results
Drug deposition and dose remaining in each component (%) of different nebulizers
The results of aerosol deposition in the inhaled mass filter and parts of each nebulizer system are given in Figure 3. Significant differences were noted among the nebulizers regarding the inhaled mass, drug reservoir, mouthpiece, and mouthpiece connection (p = 0.001). There was no significant difference in inhaled mass between the Pocket Air and APEX PY001 (19.81% ± 1.61% vs. 21.42% ± 1.8%, p = 0.124). However, both showed an inhaled mass significantly greater than that with other nebulizers (PARI-VELOX:14.60% ± 0.39%; Omron NE-U22:11.42% ± 0.13%; Aeroneb GO:16.22% ± 0.16%) (p ≤ 0.001).
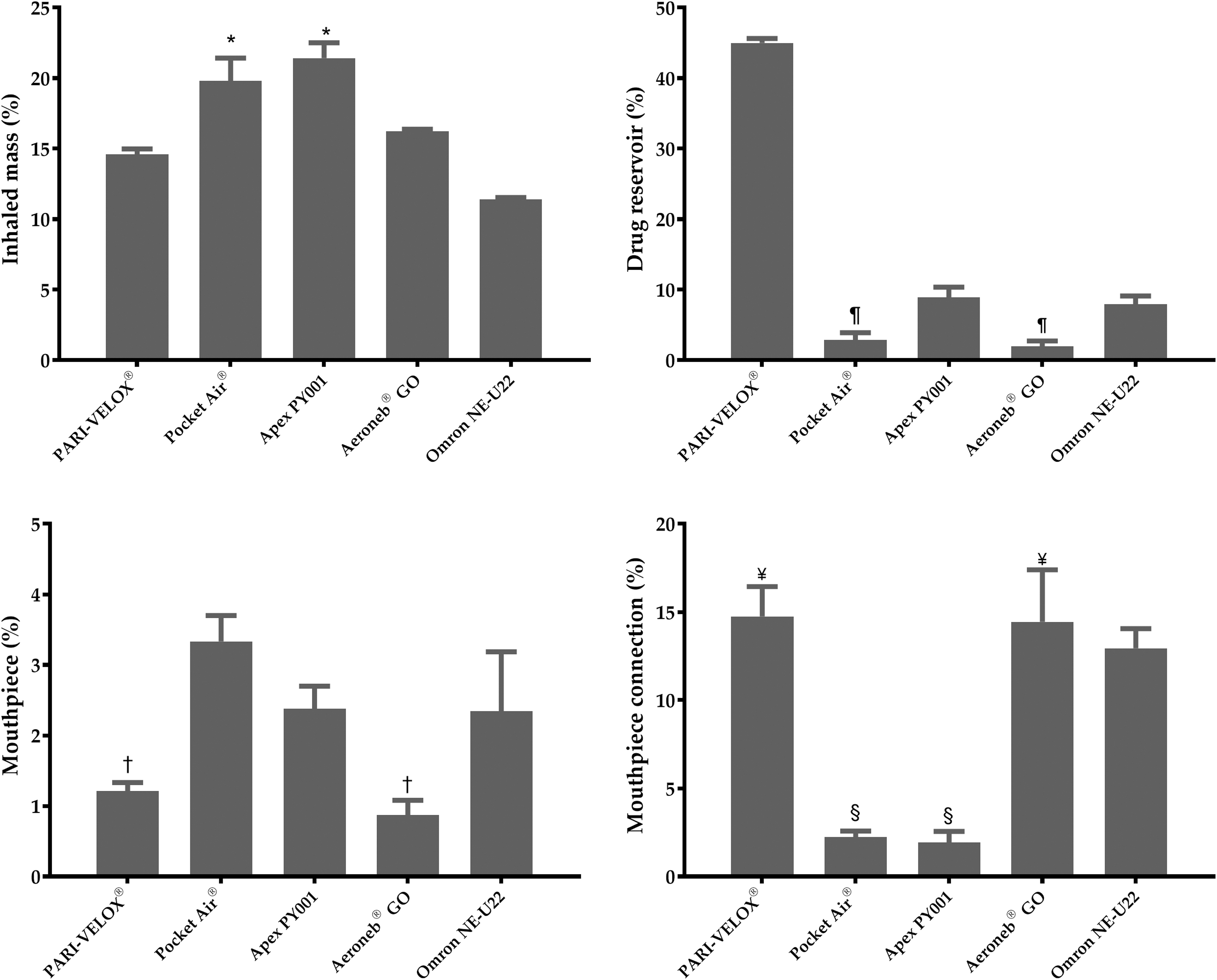
Drug deposition as % of the total dose among five nebulizers. *Significant high inhaled mass (%) with Pocket Air® and APEX PY001. ¶Significant low drug reservoir (%) with Pocket Air® and Aeroneb® GO. †Significant high mouthpiece (%) with PARI-VELOX® and Aeroneb GO. ¥Significant high mouthpiece connection (%) with PARI-VELOX and Aeroneb GO. §Significant low mouthpiece connection (%) with Pocket Air and APEX PY001.
PARI-VELOX (1.21% ± 0.12%) and Aeroneb GO (0.87% ± 0.21%) showed the lowest deposited drug remaining within the mouthpiece, but the highest dose in the mouthpiece connection (14.74% ± 1.70% vs. 14.44% ± 2.95%). Pocket Air (2.83% ± 1.06%) and Aeroneb GO (1.94% ± 0.78%) had the lowest dose in the drug reservoir (p ≤ 0.001), followed by Omron NE-U22 (7.95% ± 1.17%) and APEX PY001 (8.91% ± 1.46%). In contrast, the PARI-VELOX had the highest proportion of the dose in the drug reservoir (44.98% ± 0.65%) than others (p ≤ 0.001).
Measurement of particle size by the ACI
The characterization of the aerosol particles was determined by MMAD, GSD, FPF%, and CPF%. There was a significant difference in MMAD (p ≤ 0.001). The MMAD ranged from 2.28 ± 0.13 μm for the PARI-VELOX to 3.71 ± 0.09 μm for Omron NE-U22, with Pocket Air at 3.16 ± 0.06 μm, APEX PY 001 at 2.61 ± 0.13 μm, and Aeroneb GO at 2.84 ± 0.21 μm (Fig. 4). The lowest GSD was 1.56 ± 0.04 with PARI VELOX, and the others ranged from 1.79 to 1.85 μm (Pocket Air: 1.82 ± 0.02; APEX PY001: 1.79 ± 0.02; Aeroneb GO: 1.85 ± 0.45; Omron NE-U22: 1.80 ± 0.01). In addition, significant differences were observed in the FPF% of all five nebulizers (p ≤ 0 6.001). Nevertheless, the FPF% from PARI VELOX (97.96% ± 2.040%, p ≤ 0.001) exceeded 1.38 times more than others (Pocket Air: 72.86% ± 0.62%; APEX PY001: 84.58% ± 3.23%; Aeroneb GO: 79.46% ± 5.84%; Omron NE-U22: 70.64% ± 2.41%). Moreover, CPF% for Pocket Air, APEX PY001, Aeroneb GO, and Omron NE-U22 (27.14% ± 0.62%, 15.42% ± 3.23%, 20.54% ± 5.84%, and 29.36% ± 2.41%, respectively) differed from PARI VELOX (2.04% ± 1.38%, p ≤ 0.001).

Characterization of the aerosol particles. *Significant low MMAD with PARI-VELOX®. **Significant high fine particle fraction (%) with PARI-VELOX. ***Significant low coarse particle fraction (%) with PARI-VELOX. MMAD, mass median aerodynamic.
Nebulizer performance assessment on delivery with salbutamol sulfate
As given in Figure 5, significant differences were observed in the performances (nebulization time, output rate, and IAR) of all five nebulizers (p ≤ 0.001). Omron NE-U22 had the longest nebulizer time (10.35 ± 0.27 minutes), which was approximately two and three times longer than that of Pocket Air (5.59 ± 0.44 minutes) and PARI-VELOX (3.17 ± 0.13 minutes), respectively. In contrast, PARI-VELOX (0.45 ± 0.02 μL/min) and Pocket Air (0.43 ± 0.03 μL/min) had the greatest nebulizer output rate, which was two times greater than that of Omron NE-U22 (0.22 ± 0.00 μL/min). PARI-VELOX (4.61% ± 0.14%/min) had significant and the highest IAR than other nebulizers (p ≤ 0.001).
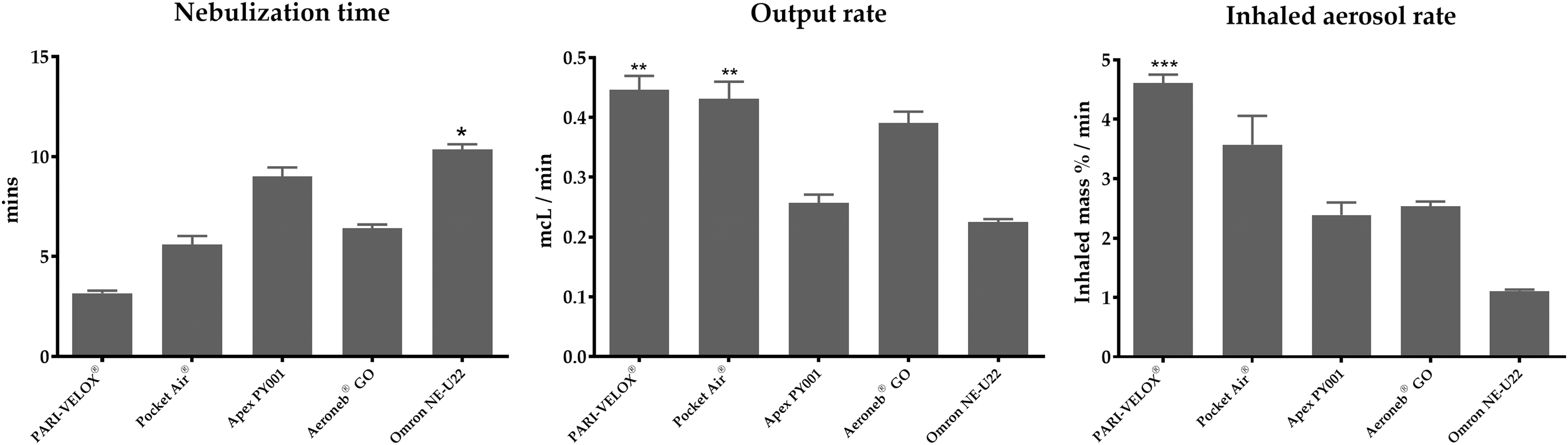
Nebulizer performance on delivery of salbutamol sulfate. *Significant long nebulizer time with Omron NE-U22. **Significant high output rate with PARI-VELOX® and Pocket Air®. ***Significant high inhaled aerosol rate (%) with PARI-VELOX.
Comparison of total recovery rate of aerosol (%)
Figure 6 provides the total recovery rate of aerosol (%); the differences among five devices varied significantly (p < 0.001). In addition, PARI-VELOX (75.54% ± 0.61%) exceeded two-fold more than others (Pocket Air: 28.20% ± 0.93%; APEX PY001: 34.64% ± 0.70%; Aeroneb GO: 33.48% ± 1.39%; Omron NE-U22: 34.63% ± 0.55%) and showed a statistically significant difference (p < 0.001).
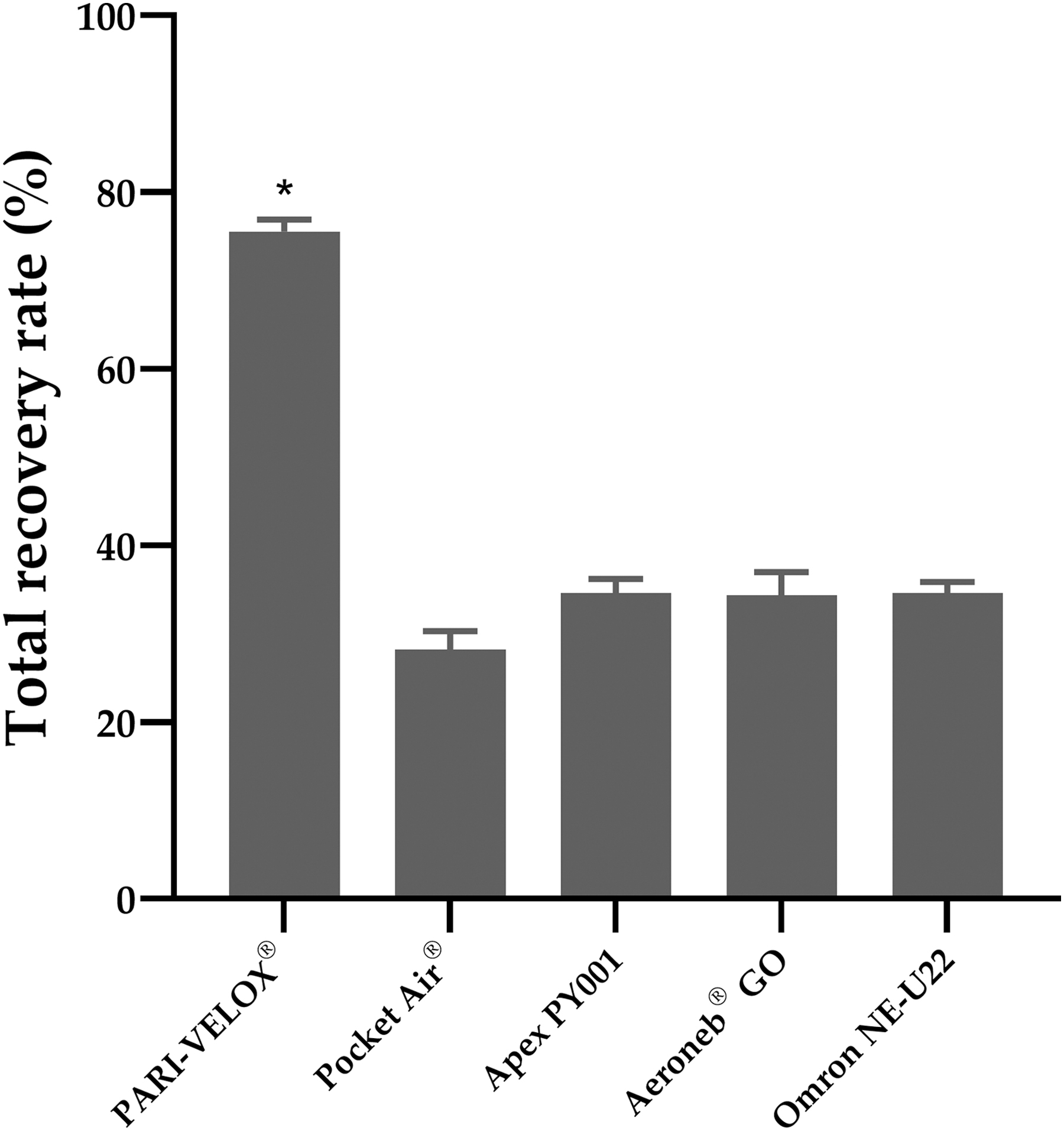
Total recovery rate of aerosol (%) among the five nebulizers. *Significant high total recovery rate (%) with PARI-VELOX®.
Discussion
Previous studies have shown that greater bronchodilator delivery by hand-held VMN with facemask in patients with COPD may hasten the improvement in the pulmonary functions and Borg breathlessness score.(16,24) However, very few studies have explored the application of hand-held VMN using mouthpiece. Our study focused on different performances of commercial hand-held VMN, and the results showed two-fold difference on inhaled dose and varied nebulizer performance.
Previous studies investigated the nebulizer performances and aerosol delivery characteristics of commercial VMN. Simmons et al. reported that the respirable mass (% by MMAD) tended to be greater for Aeroneb GO (31% ± 4%) than Omron NE-U22 (28% ± 2%). Treatment time for Aeroneb GO (6 minutes) was half that of Omron NE-U22 (12 minutes).(25) Another study by Simmons et al. showed similar MMAD (3.1 ± 1.6 vs. 3.8 ± 1.7 μm) and treatment time (6 vs. 5 minutes) of Aeroneb GO and PARI LC® Plus JN. However, the inhaled mass (22% ± 3% vs. 18% ± 3%) and respirable mass (20% ± 2% vs. 13% ± 1%) were significantly high with Aeroneb GO,(26) a finding that was consistent with the one reported by Fink and Simmons.(27) In addition, similar MMAD and FPF% were reported for PARI-VELOX (160.0 kHz) and PARI eFlow Rapid (117.0 kHz), although their resonant frequencies were different.(28)
VMN has lower residual volume 0.1–0.5 mL; approximately 4%–20% of total charged dose than JN and ultrasonic nebulizer (1–1.5 mL).(2,6,29,30,31) In our experiments, residual dose ranged from 1.94% to 8.90% (volume of 0.04–0.21 mL), which is consistent with a previous study. In addition, we observed greater residual volume in the drug reservoir when using PARI-VELOX. PARI-VELOX has been designed to a retain ∼1.0 mL drug solution and has the highest IAR. It is possible that the high residual volume was purposely designed to deliver similar drug dose as other VMN. In addition, Pocket Air and APEX PY001 resulted in significantly greater inhaled masses than Aeroneb GO and Omron NE-U22. It is speculated that Pocket Air and APEX PY001 have designed air entrainment holes on the mouthpiece that allows ambient air to cross through it during inhalation to transport the aerosol to the patient.(9)
The mouthpiece and mouthpiece connection, which are the auxiliary equipment of VMN, retained aerosol particles deposition during nebulization. Vecellio proposed that the ambient air from the nebulizer holes (close to the mesh) can push the continuously generated aerosol particles out of the nebulizer during the exhalation period and reduce aerosol particles in the mouthpiece connection.(9) Those designs, such as the use of valves to entrain air into the device, incorporated breath-activated features to further improve drug delivery and reduce drug wastage.(30) However, the aerosol particles produced by Omron NE-U22 were relatively large, causing more drugs to be deposited in the mouthpiece connection. Studies have reported that the deposited aerosol particles condensates, which blocked the aperture plate and resulted in sudden disrupted nebulization.(20,32) Therefore, when using VMN, it may be necessary to examine any blockage of the central aperture plate that may cause interruption of nebulization or may affect the efficiency of the nebulizer.
The optimal MMAD for obstructive lung disease is 1–5 μm, also referred to as the respirable particle range,(6) which greatly reduces oropharyngeal deposition and local adverse reactions during treatment.(11,12,33) Hickin et al.(16) and Cushen et al.(24) reported that patients with asthma and COPD, use a small-particle aerosol by VMN to improve the functional small airways, thereby supporting this benefit. However, Zanen et al.(34) demonstrated that in patients with mild-to-moderate asthma, the 2.8 μm particle size aerosol produced superior bronchodilation than the 1.5 and 5 μm. In addition, it was reported that the optimal particle size for β2 agonist or anticholinergic aerosols is ∼3 μm in patients with severe airflow obstruction.(35) This suggests that small particles penetrate more deeply into the lungs and more effectively dilate the small airways than larger particles. However, the 1.5 μm aerosol induced significantly less bronchodilation than the 2.8 μm aerosol, as fine aerosols may deposit particles too peripherally to be effective as smooth muscles are not present in the alveolar region. In our study, PARI-VELOX had significant smaller MMAD with near 100% FPF%, which indicated that all the drug can be delivered to the lower airways.
Previous study performed the total recovery of aerosol determination in which all aerosol is accounted during a close system, such as using a mechanical ventilator model.(36) However, fewer study investigate in a spontaneous breathing model. In our experiment, it may not be possible to take this into account due to the opening in the system setup. We found the recovery rate of PARI-VELOX is the highest (75.54% ± 0.61%), moreover 44.98% ± 0.65% in the drug reservoir accounts. As mentioned assume PARI-VELOX deliberately reserves the volume to partially compensate for it, and high yield and reduce the chance of delivering too much drug. In addition, Packet Air has a lowest recovery rate, but it is showed that high inhaled mass, and the amount of drug deposition in the mouthpiece, mouthpiece connection, and drug reservoir were minimum. It is speculated that much aerosol escaped into the atmosphere during the exhalation, or were deposited inside the airway of the manikin, and could not be recovered for measurement.
Previous studies have shown that drug characteristics, such as ionic strength, density, surface tension, and viscosity, affect the output rate of VMN.(37) Kuo et al. and Hu et al. proposed that VMN design, such as resonant frequency, driving voltage, outlet diameter, and delivery efficiency, directly affect the outcome of clinical treatment.(38,39) Moreover, studies have reported that the nebulization rate increased with the increase in the driving voltage and micro-tapered aperture diameter.(40) Particle size decreased as the resonant frequency increased, but the extent was less than expected.(38) In our experiment, we did not obtain information about the design of APEX PY001 and Pocket Air from the manufacturer, but we found opposite trends between the devices regarding nebulization time and output rate or IAR. Further studies are required to design a nebulizer with different drug characteristics to achieve the best clinical treatment effect.
Effective inhalation therapy depends on several factors, such as device, drug, and patient-related factors.(10) The information provided by the manufacturer includes the MMAD and nebulization rate. However, data related to the inhaled mass when using the interface are not provided, and there are very few such scientific studies. In our experiment, we found that PARI-VELOX showed better nebulizer performance and aerosol particle characterization. However, during nebulization, drug blockage within the central aperture plate disrupts nebulization or prolong treatment time when using Omron NE-U22.
Overall, not only the proper tidal breathing,(6) but also the VMN technology, and characterization of the accessories of hand-held nebulizer through a mouthpiece affects the performance and characterization of the aerosol particles. In addition, the information provided by our experiment could be a reference for the design and could be applied to manufacturing of the device. VMNs have become the first choice for new nebulized pharmaceutical drug developments.(41) As device performance varies, it is important to ensure that the most appropriate device is chosen for the intended drug to ensure optimal drug delivery to the patient population.(30)
This study has certain limitations. Our study used one set of breathing patterns, which provided a consistent flow, volume, and frequency during aerosol therapy. We could not provide specific guidance on the wide range of breathing parameters that may be encountered in clinical situations. Moreover, highly viscous or suspended liquid drugs affect the VMN performance(5,6,10); however, we used salbutamol as a surrogate for drug quantification. In addition, previous study demonstrates that variability of the VMN randomly interrupted with a wide range of retained volumes.(32) However, our experiment only uses one sample of each device brand. Our experiment was an in vitro study and the results could differ when reproduced in a clinical setting with considerable biological variability. In addition, our findings may help in guiding clinical research and supporting clinical management strategies.
Conclusions
In summary, commercially available VMN produced two-fold differences in inhaled mass, but with a similar MMAD. However, the differed amount of aerosol particles deposited on auxiliary equipment directly influenced the performance of the VMN. These performance characteristics and the reproducibility may be considered when selecting a commercially available VMN for home use by a COPD patient. The results of this study may allow clinicians to select VMN based on the demonstrated performance rather than solely on convenience and cost.
Footnotes
Acknowledgments
The authors acknowledge the support from the Department of Respiratory Therapy, College of Medicine, Chang Gung University, Taoyuan, Taiwan for providing the experimental equipment.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
No funding was received for this article.
Reviewed by:
Arzu Ari
Michael McPeck