
Abstract
Background:
Acinetobacter baumannii-mediated bacterial pneumonia is a common disease that is harmful to human health. Dipalmitoylphosphatidylcholine (DPPC) is the major lipid component of the pulmonary surfactant (PS) found in the alveolar space; the PS helps to keep surface tension low, which allows for improved oxygen delivery. Resveratrol (RE) is a phytoalexin found in plants that is released in response to injury or infection. The therapeutic effect of Re is limited due to its low solubility and bioavailability. In this study, we report pulmonary delivery of Re-loaded DPPC liposomal large porous microparticles (RDLPMs) for treatment of A. baumannii-induced pneumonia.
Methods:
Novel RDLPMs were prepared by rotary evaporation and a freeze-drying method in this study. RDLPMs were evaluated by the particle size, electric potential, in vitro release, and particle size distribution. A rat model of A. baumannii-mediated pneumonia was established and used for pharmacodynamic evaluations.
Results:
The Re-loaded DPPC liposomes (RDLs) consisted of Re/DPPC (1:3, mol/mol) and DPPC/cholesterol (3:1, w/w), with a hydration time of 15 minutes. The RDLs had a high encapsulation efficiency of 69.8% ± 1.6%, a mean size of 191.5 ± 4.5 nm, and a high zeta potential of 12.4 ± 1.5 mV. The RDLPMs were composed of mannitol/large porous microparticles/RDLs (1:4:2, w/w/w) and had a loading efficiency of 2.20% ± 0.24%. The RDLPMs had an aerodynamic diameter (2.73 ± 0.65 μm), a good fluidity (28.30° ± 6.13°), and demonstrated high lung deposition (fine particle fraction = 43.33%). Surprisingly, while penicillin showed better microbial inhibition than the RDLPMs and Re groups in vitro, the RDLPMs were more effective in vivo.
Conclusion:
The RDLPMs showed good powder properties for pulmonary delivery. The RDLPMs may inhibit the nuclear factor kappa-B pathway and downregulate the expression of cytokines downstream of tumor necrosis factor-α and interleukin-1β. As well as, RDLPMs demonstrated some antibacterial properties against A. baumannii bacteria. Re, when delivered in RDLPMs as a dry powder inhaler, is a promising substitute for antibiotics in the treatment of A. baumannii pneumonia.
Introduction
Bacterial pneumonia is a disease commonly found in clinic and may be fatal in at-risk patients, such as the elderly, children, and immunocompromised.1–3 Bacterial pneumonia can be caused by various bacteria, such as Staphylococcus aureus, 4 Klebsiella pneumoniae, 5 and Acinetobacter baumannii. 6 A. baumannii is an important human pathogen and a leading cause of nosocomial infections, especially for bacterial pneumonia. 7 As multidrug-resistant A. baumannii are frequently identified as the cause of outbreaks of clinical infections,8,9 few antibiotics are effective for treating infections caused by this pathogen. Therefore, it is urgent that research to find new antimicrobial substances and develop new drug delivery systems is carried out.
Resveratrol (Re) was first discovered as a phytoalexin and has recently been of interest to the medical community. 10 Re has multiple pharmacological properties.11–15 In terms of antibacterial activity, previous studies have reported that Re has a strong inhibitory effect on both cocci and bacillus. 16 In our previous study, it was found that Re had more antibacterial effect on A. baumannii than on S. aureus. However, low water solubility, poor oral absorption, and less than 30% oral bioavailability limit its therapeutic effect.17,18 Whether Re can be inhaled into the lungs to prevent A. baumannii pneumonia and its related complications needs to be further studied.
Pulmonary surfactant (PS), dipalmitoylphosphatidylcholine (DPPC), is a lipoprotein secreted by alveolar type II cells. The main function of the surfactant is to establish an extreme reduction in surface tension; this is achieved when this DPPC is incorporated into the air–water interface. 19 DPPC could be used to avoid alveolar effusion and maintain the fluid balance in the lung. Because lung surfactant is composed of DPPC, the exogenous DPPC can carry drugs through the lung surface active layer and promote drug absorption in the lung. In addition, DPPC also establishes a local barrier that prevents exogenous infection and particle infiltration.20,21
Previous studies have reported that insulin encapsulated by DPPC liposomes can increase drug concentration at the alveolar surface and improve drug absorption. 22 Tagami et al proved that the inhalation of doxorubicin DPPC liposomes was beneficial for drug absorption and improved the compounds efficacy in the treatment of lung cancer. 23 Therefore, DPPC was selected as a lipid biological carrier to supplement the PS lost by bacterial pneumonia infection and improve drug absorption.
Dry powder inhalers (DPIs) can deliver stable, high drug loads, while maintaining patient compliance due to ease of use.24,25 Nanoparticles, microspheres, and microcapsules can act as carriers in DPIs; their use can prolong the release of drugs,26,27 improve drug absorption, and reduce toxic drug-mediated effects in the lung. However, the average diameter of nanoparticles is less than 1 μm; due to this, they are quickly cleared by pulmonary macrophages. Microspheres or microcapsules with a high density and large size are difficult to deposit deep in the lung. Therefore, the application of nanoparticles and microspheres in pulmonary drug delivery systems is limited.28,29
Large porous microparticles (LPMs) can be inhaled by the lungs while avoiding macrophage-mediated phagocytosis; this is due to their small density (<0.1g/cm3) and large geometric particle size30,31 (>10 μm). In addition, LPMs can control the release of drugs and improve therapeutic effects.32,33
In this study, novel Re-loaded DPPC liposomal large porous microparticles (RDLPMs) were prepared to identify the properties required to prolong and sustain drug release; they acted as biocompatible carriers and increased pulmonary bioavailability. The formulation and preparation methods of RDLPMs were screened and evaluated. The pharmacodynamic effects of RDLPMs on A. baumannii pneumonia were explored in a rat model; the relevant mechanisms were also discussed. The prospect of development of Re and RDLPMs was discussed, especially in relation to the fight against resistant A. baumannii pneumonia based on its immunoregulatory function. The study provides a new therapeutic drug and means for patients with A. baumannii infection or drug resistance.
Materials and Methods
Materials
Re was provided by the Meryer Chemical Technology Co., Ltd. (Shanghai, China). Poly (lactic-co-glycolic) acid (PLGA, lactide/glycolide, 50:50, mol/mol, and molecular weight 10 kDa) was produced by the Jinan Daigang Biomaterial Co., Ltd. (Shandong, China). Mannitol was purchased from the Coolaber Science & Technology Co., Ltd. (Beijing, China). DPPC was purchased from Avanti Polar Lipids, Inc. A. baumannii (19606; ATCC) was purchased from the Luwei Technology Co., Ltd. (Shanghai, China). Anti-P-NF-κB p65 bodies were from the Cell Signaling Technology, Inc. (Danvers). All other chemicals and solvents were of analytical grade or high performance liquid chromatography (HPLC) grade.
Animals
Male Sprague Dawley rats (180–200 g) from the Laboratory Center of the Yangpu Hospital were used. All the animal handling and surgical procedures were conducted strictly in accordance with the Guiding Principles for the Use of Laboratory Animals. This study was approved by the Animal Care Committee of the Yangpu Hospital. The rats were euthanized to obtain lung tissue for the pharmacodynamic study.
Preparation of RDLs
The RDLs were prepared using the film dispersion method. 34 Briefly, DPPC and cholesterol were dissolved in a mixed solution of ether and ethanol (1:15, v/v) with Re. The solution was evaporated in a rotating evaporator at 60°C for 1 hour. The liposomes were hydrated for 30 minutes with phosphate-buffered solution (PBS, pH 7.4) and then sonicated for 15 minutes. The prescription was screened using the orthogonal test (Supplementary Table S1).
Encapsulation and loading efficiencies in RDLs
The RDLs were separated through a Sephadex G-25 gel column, with purified water used as the eluent. The eluent was collected and dissolved in ethanol. The encapsulated Re was analyzed using HPLC. A Phenomenex C18 column (150 × 4.6 mm, 5 μm) was used. The mobile phase was 22% acetonitrile in water, at a flow rate of 1 mL/min. The detection wavelength was 306 nm. Encapsulation efficiency (EE) and drug loading efficiency (DLE) were calculated using Equations (1) and (2), respectively.
Characterization of RDLs
RDLs were observed on a transmission electron microscope (TEM; 80 kV, H-7650; Hitachi, Japan). The samples were negatively stained using a sodium phosphotungstate solution (pH 7.2). Dynamic light scattering (DLS) was performed on a Zetasizer Nano ZS (Malvern, United Kingdom) at 25°C to measure the particle size, size distribution, and the zeta potentials of the RDLs.
Preparation of LPMs
The LPMs were prepared using the water-in-oil-in-water (w/o/w) emulsion solvent evaporation method.35,36 PLGA (300 mg) was dissolved in methylene chloride (2 mL) and then mixed with a NH4HCO3 solution (1.5%, 0.4 mL). A 70-W probe type sonicator was used to ensure that the w/o emulsions were mixed with a polyvinyl alcohol (PVA) solution (1%, 25 mL); these were then homogenized for the preparation of w/o/w emulsions. Organic solvents were removed from the emulsions after overnight stirring. Solid microparticles were collected after high-speed centrifugation, washed with water, and then lyophilized (Supplementary Fig. S1).
Preparation of RDLPMs
The RDLs were dissolved in an optimized solvent. The lyoprotectant (mannitol) and LPMs were added to the RDLs at a 1:4:2 (w/w/w) ratio in 30 mL of deionized water before being stirred for 15 minutes. The mixed liquid was freeze-dried using a lyophilizer (Scientz-10N; Ningbo Scientz Biotechnology Co., Ltd., China). The optimal preparation process was chosen after comparing the particle properties (Supplementary Table S2).
Characterization of RDLPMs
The powder volume diameters were measured using a particle size analyzer (BT2001; Bettersize Instruments Ltd., Dandong, China), based on the laser light diffraction method. The surface morphology of the RDLPMs was observed using a scanning electron microscope (SEM, S-4800; Hitachi). The RDLPMs were mounted on metal stubs with an adhesive carbon tape, sputter-coated with gold, and examined under the microscope at an acceleration voltage of 10 kV. The angle (°) of repose of the RDLPMs was calculated using the funnel method. The bulk density was calculated using the graduated flask method. The theoretical estimates of the aerodynamic diameter (AD) of the RDLPMs was defined as d (ρ/ρ0X)1/2, where d is the geometric mean diameter (the D50 value obtained from the measurement of volume diameters), ρ0 is a reference density of 1 g/mL, X is the dynamic shape factor (1 for a sphere), and ρ is the tapped density (also the bulk density). 37 All the measurements were made in triplicate at a constant temperature of 25°C.
Aerosol size distribution
In vitro particle size distribution was determined using the Next Generation Impactor (NGI; Copley Scientific Limited, United Kingdom), at an airflow rate of 60 L/min. The aerosolization performance of the 20 mg powders, which had been filled into size 3 hard capsules, was investigated with a linker (powder inhaler; Aptar (Suzhou) Dispensing Systems Co., Ltd., China) to the NGI. The powders collected at each stage were dissolved in deionized water, diluted with ethanol, and analyzed via HPLC.
The effective aerodynamic cutoff diameters in the various NGI impaction stages were 8.06, 4.46, 2.82, 1.66, 0.94, 0.55, 0.34, and 0.24 μm for stages 1–7 and micro-orifice collection, respectively. The mass median aerodynamic diameter (MMAD) was calculated using the Copley Inhaler Testing Data Analysis Software (CITDAS). The fine particle dose (FPD), fine particle fraction (FPF), emitted dose (ED), and proportion of inhaled powders out of the capsules of RDLPMs were calculated according to Equations (3)–(5).
In vitro release study
RDLPMs (10 mg) were suspended in simulation lung fluid (SLF, 50 mL) containing 0.02% Tween 80. 38 The suspension was shaken at 60 rpm at 37°C. At predetermined time points, an aliquot (1 mL) of the suspensions was withdrawn and centrifuged at 5000 rpm for 10 minutes. Fresh SLF of an equal volume was added to the suspension following pipetting. The supernatant was filtered through 0.45 μm filters and analyzed using HPLC. More details about the equipment can be found in the Supplementary Data. The experiments were performed in triplicate.
In vitro antimicrobial study
The antimicrobial activities of Re and RDLPMs were detected against A. baumannii (1 × 106 Colony-Forming Units/mL (CFUs/mL); 19606; ATCC). Penicillin was selected as the positive control. A. baumannii was incubated with various concentrations (4.00, 2.00, 1.00, 0.50, 0.25, and 0.13 mg/mL) of Re powder, RDLPMs, and penicillin. These experiments were performed in Luria–Bertani culture medium for 24 hours at 200 rpm and 37°C. The above cultures were used for inoculation by dipping a clean inoculating ring into the culture and spreading it onto agar plates; these were cultured for 24 hours at 37°C. Colony growth was observed and counted. The minimum inhibitory concentration (MIC) was calculated. The experiments were performed in triplicate.
Pharmacodynamic study
According to previous studies, 39 A. baumannii (19606; ATCC) was selected as the microbial model. A laryngoscope (MJ MediTech, Jiangsu, China) was used to visualize the tracheal opening. Rats were divided into five groups, with six rats in each group. 108 CFUs/mL microbial suspensions were sprayed into the rat lung using an intratracheal aerosolizer (IA-1B; Penn-Century, Inc., PA). A dose of 0.2 mL was given to each rat to prepare the bacterial pneumonia model. Therapy was initiated 6 hours after inoculation. The healthy rats were intratracheally administered with saline solutions at a dose of 0.2 mL for each rat. The Re powder (10 mg each rat, Re/lactose 1:9, w/w), the RDLPMs (20 mg each rat, containing about 1 mg Re), and the penicillin solution (48 mg/rat) were administered to the lungs of rats using the insufflator (DP-4M; Penn-Century, Inc.) and the intratracheal aerosolizer through the trachea without anesthesia. The administrations were repeated 24 and 48 hours after the first dose.
An aliquot (20 μL) of blood was withdrawn via tail vein and deposited into an ethylenediaminetetraacetic acid-coated (EDTA) tube containing isotonic diluents (2 mL; ISOTONAC3), 12 hours after the final administration. The samples were analyzed using an automated hematology analyzer (MEK-7222K; Nihon Kohden, Tokyo, Japan) to measure leukocytes. The rats were deeply anaesthetized with isoflurane before the lungs were exposed. The right lungs were ligated. Bronchoalveolar lavage fluids (BALFs) in the left lungs were collected and centrifuged for 10 minutes at 3000 rpm at 4°C. The resulting supernatants were stored at −80°C before use in an enzyme-linked immunosorbent assay (ELISA). The right lungs were removed, and three lobes were prepared for histopathology, immunofluorescence, and a bacterial count, respectively.
Histopathology
The middle lobe of the left lung was immersed in a 10% formalin solution and embedded in paraffin. Five-micrometer-thick pathological sections were stained with hematoxylin and eosin. The sections were observed under a microscope.
Immunofluorescence
Sections of the left lung, initially embedded in paraffin, were deparaffinized, rehydrated, and microwave-heated for 15 minutes in an EDTA antigen retrieval solution (pH 8.0). A 3% H2O2 solution was used to block endogenous peroxidase activity. The tissues were further blocked with bovine serum albumin (BSA). A primary antibody for P-NF-κB p65, diluted with a 3% BSA solution, was added to the above tissues and incubated overnight at 4°C. The sections were washed with PBS three times. A cyanine 3 (CY3) fluorescent secondary antibody was applied for 30 minutes at room temperature with interval PBS washing. A dye, 4′6-diamidino-2-phenylindole, was included in the final wash to stain the nuclei. Images of CY3 and 4,6′-diamidino-2-phenylindole (DAPI) fluorescence were observed using a fluorescent microscope (Nikon, Japan).
Leukocyte measurement
Aliquots (20 μL) of blood were withdrawn, via the tail vein of each rat, into the EDTA-coated tubes containing isotonic diluents (2 mL; ISOTONAC-3), 12 hours after the final administration. The samples were analyzed with an automated hematology analyzer (MEK-7222K; Nihon Kohden) for leukocyte measurement.
Lung homogenates for counting bacteria
The upper lobe of the left lung was homogenated with saline (1 mL, 4°C) using a glass tissue homogenizer. After an appropriate dilution, the bacteria in the homogenates were counted following inoculation and cultured for 20 hours at 37°C.
Measurement of tumor necrosis factor-α, interleukin-1, and total protein
Total protein (TP), tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) were used as markers of acute inflammatory response. The concentrations of TNF-α, IL-6, and TP in the supernatants of BALFs were measured with ELISA kits (Neobioscience Technology Co., Ltd., China) and protein kits (Beyotime Biotechnology Co., Ltd., China), according to the manufacturer's instructions.
Statistical analysis
One-way analysis of variance (GraphPad InStat Software Demo) was used to determine significance. All error bars represent standard deviations. Statistical significance was determined when p < 0.05 or p < 0.01.
Results
Optimal formulation of RDLs
The formulation screening process is specified in the orthogonal test (Supplementary Table S1). The molar ratio of Re and DPPC (A), DPPC/cholesterol (w/w) (B), and hydration time (C) was selected as influencing factors. The order of factors was A>B>C, and the optimal level of each factor was A3B2C1. The optimal formulation of RDLs was Re/DPPC (1:3, mol/mol), DPPC/cholesterol (3:1, w/w), with a hydration time of 15 minutes. When using the optimal formulation, the EE was 69.8% ± 1.6% and the drug loading was 7.1% ± 0.7%.
Characteristics of RDLs
The RDLs were clear and translucent in solution (Fig. 1A), and the TEM images indicated that RDLs existed as spherical vesicles (Fig. 1B). The size and zeta potentials of the RDLs, as measured by DLS, were 191.5 ± 4.5 nm and 12.4 ± 1.5 mV, respectively (Fig. 1C, D). A relatively narrow size distribution was observed, with a polydispersity index (PDI) of 0.30 ± 0.05. The RDLs small size and high dispersion could enhance their pharmacological activity after pulmonary delivery.
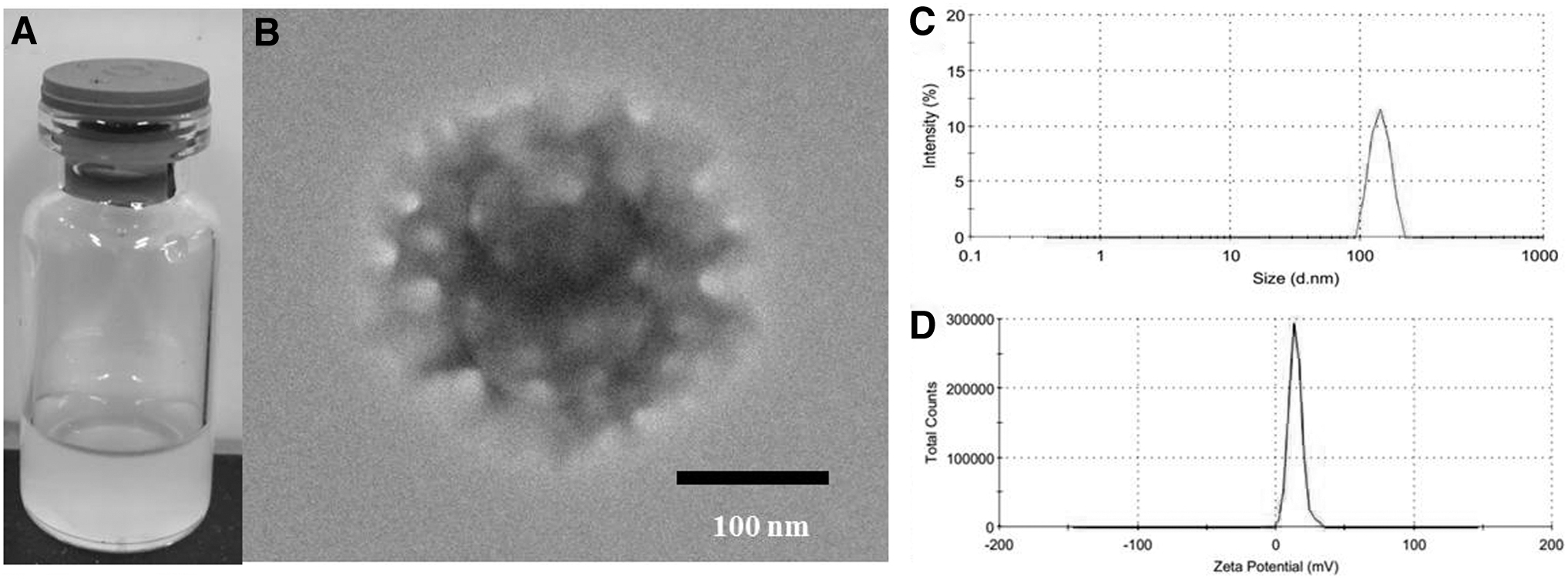
Appearance of Re-loaded DPPC liposomes
Optimal preparation process of RDLPMs
The different proportions of mannitol and LPMs were compared according to the states and parameters of the samples (Supplementary Fig. S1). More details are described in the Supplementary Data. The optimal formulation of RDLPMs consisted of mannitol/LPMs/RDLs (1:4:2, w/w/w); this obtained a loading efficiency of 2.20% ± 0.24%. Concurrently, the RDLPMs satisfied the parameters for appearance and good fluidity.
Characteristics of RDLPMs
The RDLPMs existed as spheres with multiple surface pores, according to SEM imaging (Fig. 2A). The average geometric diameter of the RDLPMs was 12.59 ± 3.01 μm (D50), according to the laser light scattering measurement (Fig. 2B), and the angle of repose, tapped density, and AD of RDLPMs were 28.30° ± 6.13°, 0.04 ± 0.01 g/mL, and 2.73 ± 0.65 μm, respectively. The RDLPMs favored lung deposition, while the NGI experiment indicated that the RDLPMs had been effectively emitted from the DPI device (MMAD = 5.324 μm, FPF = 43.33%, ED = 92.61%; Fig. 3). Based on the above study, the RDLPMs were found to be suitable for use in the pulmonary delivery system.
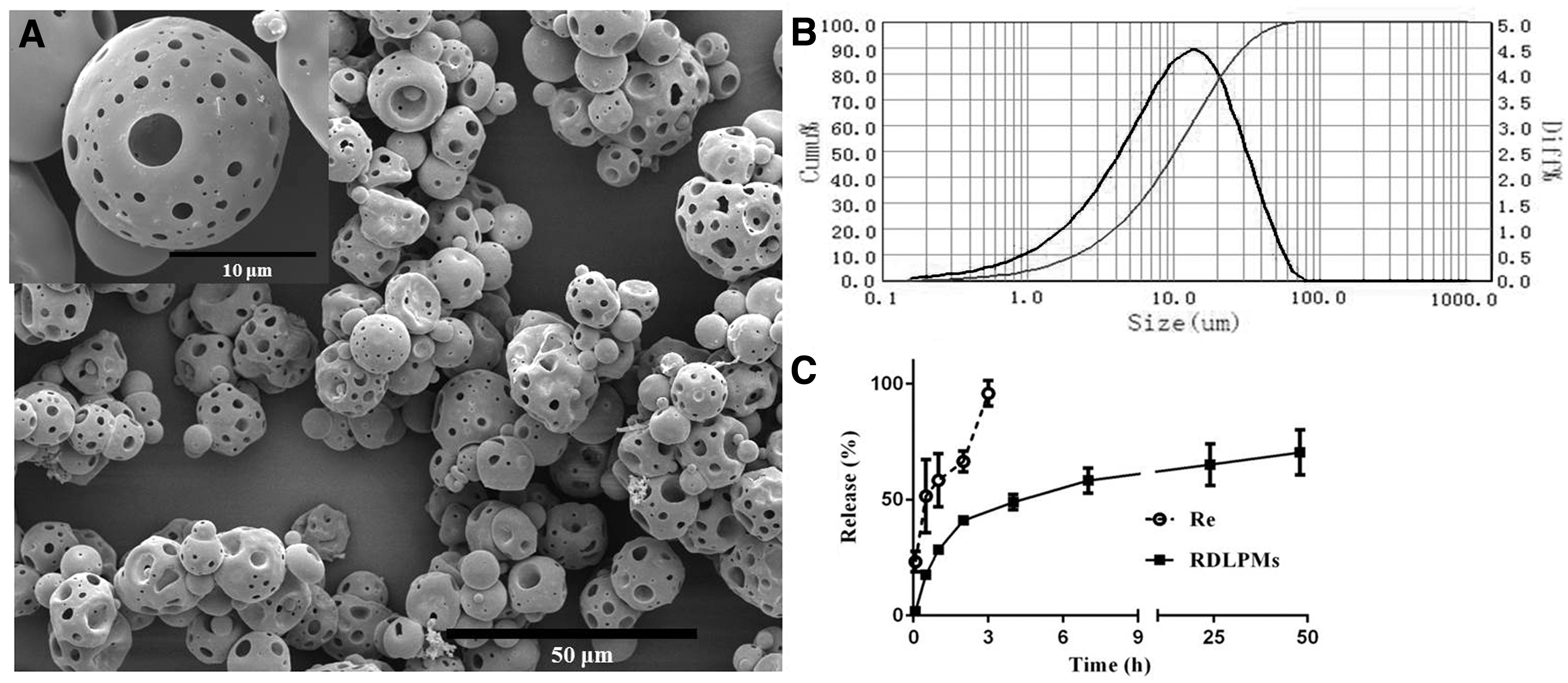
Morphology and surface structure of RDLPMs by SEM
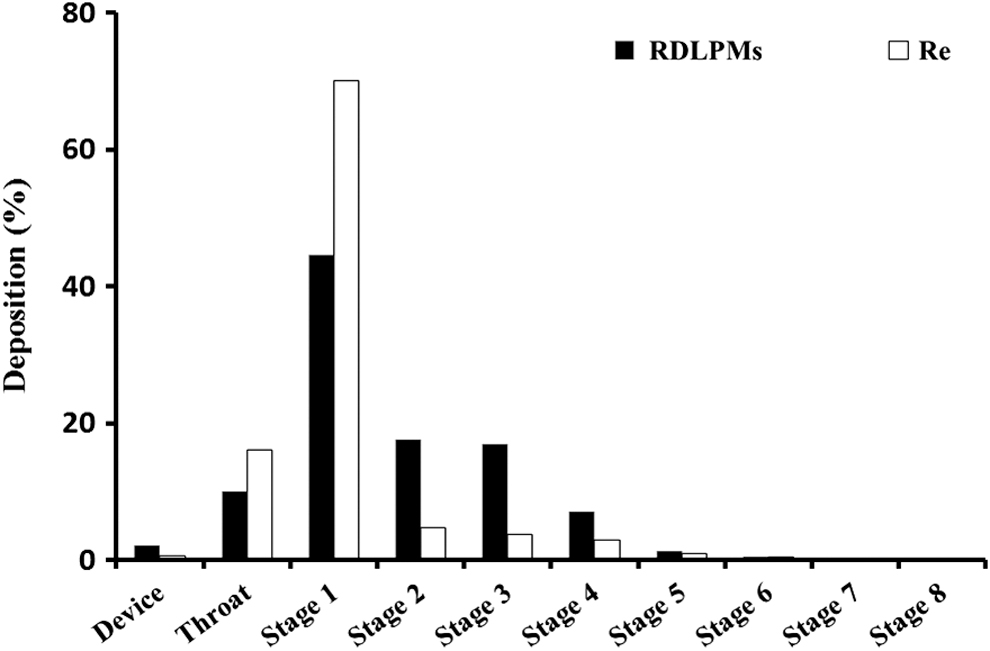
Distribution of RDLPMs and Re by the Next Generation Impactor. The deposition (%) is based on different stage dose collected in impactor/total dose collected in impactor.
It was found that a free Re solution had a monophasic release pattern, releasing most of the drug within 3 hours (95.84% ± 5.53%) (Fig. 2C). However, the RDLPMs showed a biphasic release pattern, and the initial burst release (47.92% ± 2.76% for 1 hour) was followed by a sustained release profile (70.38% ± 9.69% for 48 hours). The mechanism of drug release from the RDLPMs was determined by different mathematical models, for example, zero order, first order, Higuchi kinetics, and Ritger–Peppas. The Ritger–Peppas model (R 2 = 0.7894) was suitable to describe the release profile of the RDLPMs. The model results suggest that Re release was mainly due to a combination of diffusion and PLGA erosion. More details regarding the equipment are described in the Supplementary Data.
Little antimicrobial effect of RDLPMs in vitro
Penicillin exhibited strong anti-A. baumannii activity at an MIC of 0.25 mg/mL (Fig. 4). However, Re exhibited a minimal anti-A. baumannii effect at a high concentration of 4 mg/mL (Fig. 4). The antimicrobial activity of RDLPMs at an MIC of 2 mg/mL was higher than free Re, but still markedly less than penicillin. This suggested that Re-loaded DPPC liposomes should be easily cell-internalized via endocytosis and promote the antimicrobial effect of the drug.
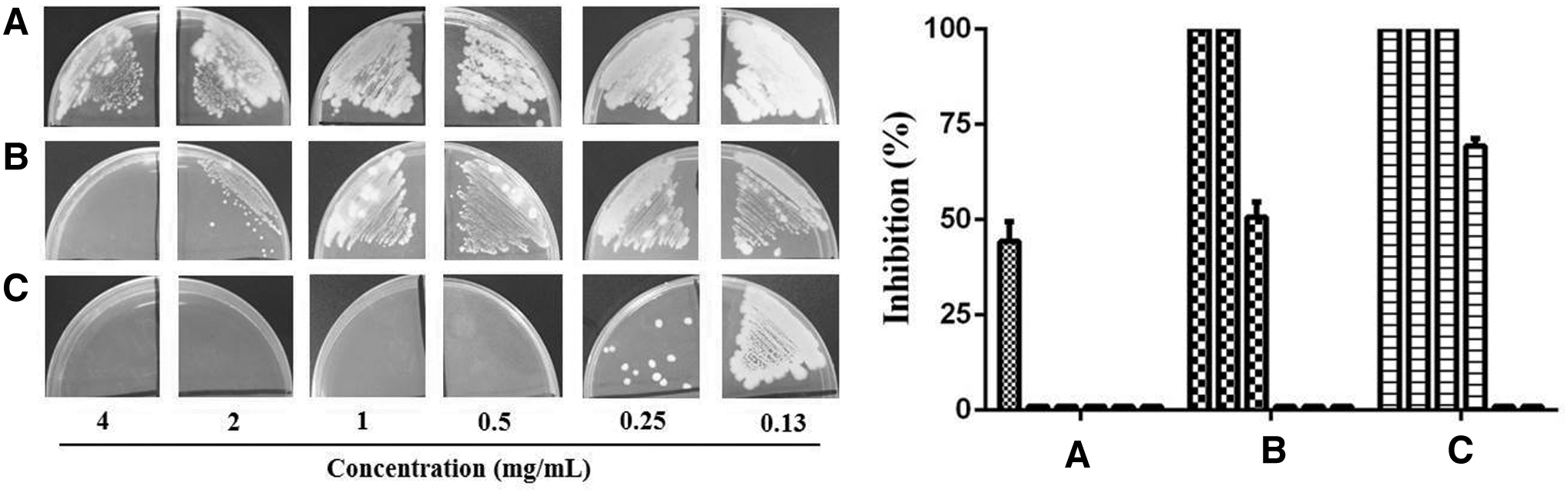
The anti-Acinetobacter baumannii effects of Re powders
High anti-A. baumannii pneumonic effect of RDLPMs
The pathological sections of the pneumonic model group expressed obvious edemas, hemorrhaging, and copious monocyte infiltration (Fig. 5B). A lot of diffuse exudates appeared in the bacterial-infected lungs. Re powder treatment reduced the number of diffuse exudations, although hemorrhaging persisted (Fig. 5C). RDLPM treatment showed a marked alleviation of pulmonary edema, with less edema fluid exudation than sections from the Re powder and penicillin solution treatment groups (Fig. 5D). Therefore, RDLPMs exhibited more potent antibacterial effect than Re, resulting from the DPPC vehicle.
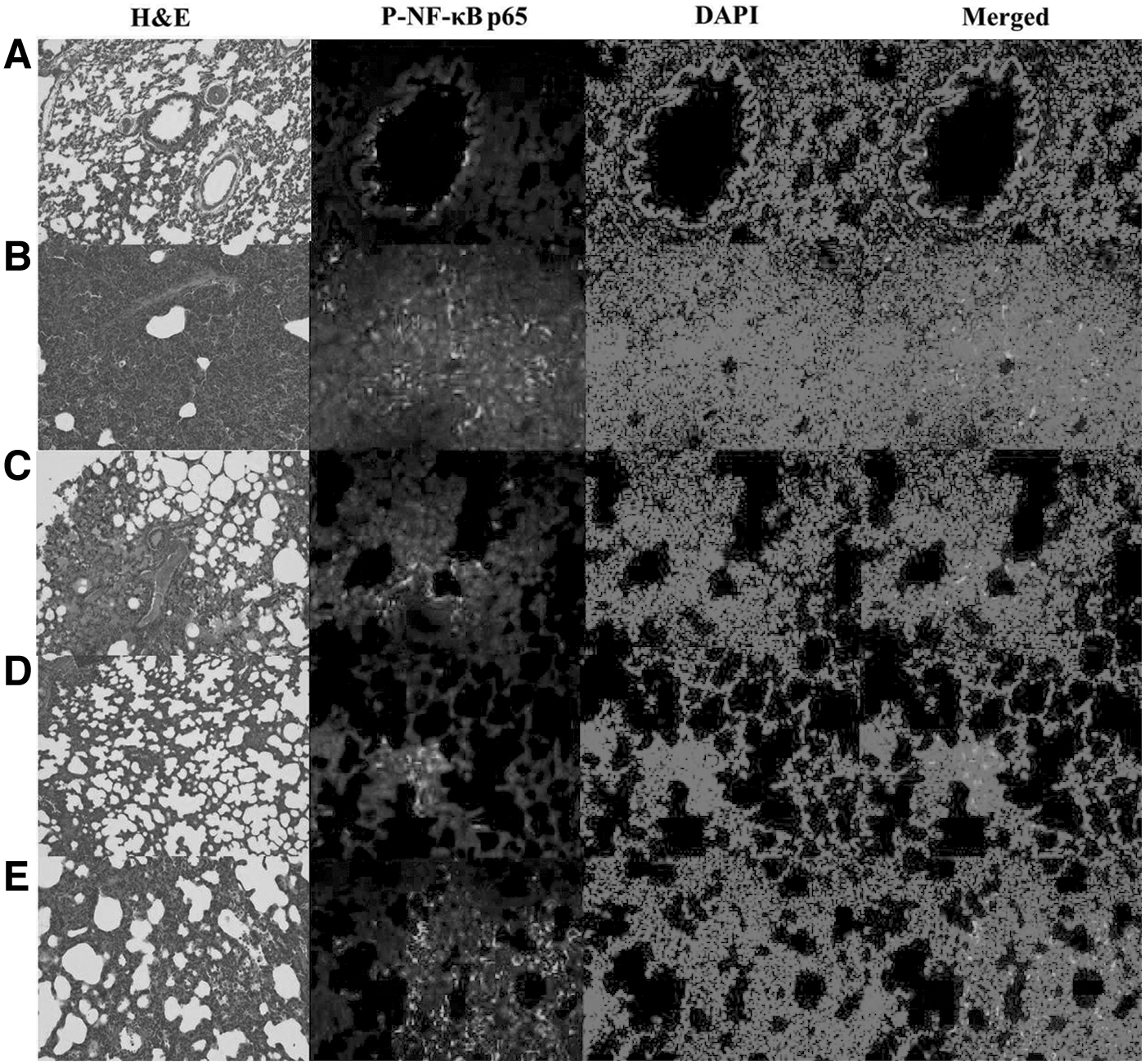
Lung histological section pictures (100 × ) and immunofluorescence images (200 × ) of the normal rats
Clearance of A. baumannii in vivo
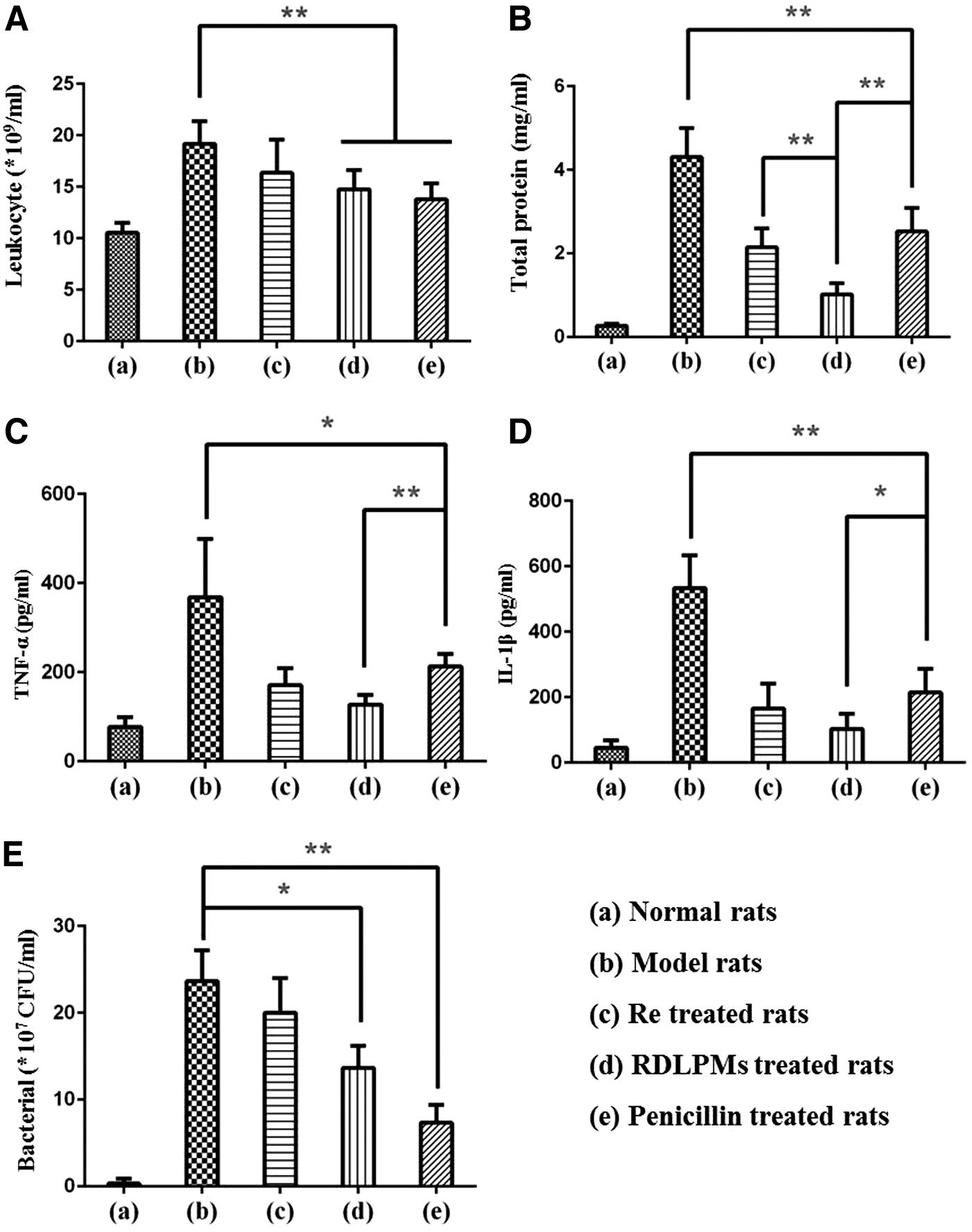
Killing bacteria is one of the key methods in the treatment of bacterial pneumonia. Bacterial CFUs were explored in rat lung homogenates following treatment. In the previous experiment, penicillin demonstrated a strong anti-A. baumannii activity in vitro (Fig. 4). In vivo, the RDLPM and penicillin group inhibited the growth of A. baumannii in rats, with significant differences in growth when (p < 0.05, p < 0.01) compared with control rats (Fig. 6E). Furthermore, penicillin proved to have better microbial inhibition ability than RDLPM and the Re group. These results are the same as experiments in vitro. These findings suggest that the inhibition and killing of bacteria are not the main mechanisms of Re in the treatment of bacterial pneumonia.
The treatment effects of the preparations on the leukocyte
Effects of Re on inflammatory reactions
The major damage mechanisms of pneumonia are inflammatory reactions. 40 Generally, the TP amount was found to be increased in inflammatory exudates. RDLPM and Re powder treatment led to statistically lower TP levels than in control group lung BALFs; the protein levels were lower following RDLPM treatment compared with Re powder treatment (p < 0.01, Fig. 6B). Leukocyte levels and the levels of the cytokines TNF-α and IL-1β were selected as markers of inflammation; the reduction of the levels of these was used to assess treatment efficacy. All the treatments, including Re, RDLPM, and penicillin, significantly decreased the number of leukocytes compared with the control group. RDLPM and penicillin treatment showed similar levels of leukocyte attenuation (Fig. 6A). TNF-α was downregulated to a greater extent in the RDLPM group compared with the penicillin group (p < 0.01, Fig. 6C). This was mirrored with IL-1β levels (p < 0.05, Fig. 6D). Therefore, RDLPM treatment effectively suppressed the inflammatory responses and improved drug efficacy.
Inhibition of P-NF-κB p65 activation expression in the lung by Re
Nuclear factor kappa-B (NF-κB) participates in immunoreactions, inflammatory reactions, apoptosis, and tumor genesis by regulating the expression of multiple genes. P-NF-κB p65 plays a crucial role in the NF-κB signaling pathway. The influence of the different treatments on the phosphorylation state of NF-κB p65 was evaluated by immunofluorescence. In the saline group, there was no significant activation of P-NF-κB p65 in the lung tissue (Fig. 5A). In the lung tissue of the penicillin group, P-NF-κB p65 was highly expressed (Fig. 5B) in the nucleus of endothelial and inflammatory cells around the bronchiolar epithelium. However, Re and RDLPM treatment significantly reduced the expression of P-NF-κB p65 compared with the positive control (Fig. 5D). Therefore, Re may be involved in the inhibition of the NF-κB pathway by preventing NF-κB p65 phosphorylation, whereas penicillin may have little effect.
Discussion
Re has multiple pharmacological properties. It has been demonstrated to act as an antioxidant, as well as possessing antibacterial, anti-inflammatory, antitumor, and immunomodulatory properties.12–14 DPPC is the most important component of the PS, which helps drugs to overcome the barrier imposed by the surfactant layer and enter cells.20,21
In this study, the optimal RDL formula was discovered to consist of Re/DPPC (1:3, mol/mol) and DPPC/cholesterol (3:1, w/w). The maximum EE was 69.8% ± 1.6%, and the drug loading score was 7.1% ± 0.7%. The small size (191.5 ± 4.5 nm) and high dispersion (PDI 0.25 ± 0.04) could enhance the pharmacological activity of the RDLs.
In this study, it was demonstrated that the optimal RDLPM formula consisted of mannitol/LPMs/RDLs (1:4:2, w/w/w); this formula lead to a loading efficiency of 2.20% ± 0.24%. LPMs and mannitol, as the carriers of the RDLPMs, had good fluidity and high lung deposition. This may be explained by the lyoprotectant improving the glass transition temperature of the RDLPMs and forming hydrogen bonds with polar groups of the DPPC in the surfactant.41,42 The SEM analysis revealed that the RDLPMs were spheres with rough porous surfaces. The angle of repose, tapped density, and AD of the RDLPMs were 28.30° ± 6.13°, 0.04 ± 0.01 g/mL, and 2.73 ± 0.65 μm, respectively. RDLPMs had a small AD and good fluidity, which favored deposition into the lung. The in vitro deposition experiment proved that RDLPMs were effectively emitted from the DPI device (FPF = 43.33%, ED = 92.61%). Based on the powder properties and features of the PS, RDLPMs were found to be suitable for use as the pulmonary delivery device of Re.
The process of Re release from the RDLPMs was explored in this study. The Ritger–Peppas model (R 2 = 0.7894) was most suitable for use in the description of the release profile of RDLPMs. The results suggest that the drug release profile was due to a combination of diffusion and PLGA erosion.
The anti-A. baumannii pneumonia mechanism of RDLPM treatment was further studied in vivo. Although the antibacterial effect of RDLPM treatment was inferior to penicillin in vitro, RDLPMs demonstrated better therapeutic promise in the treatment of A. baumannii-mediated pneumonia, than penicillin, in vivo. An analysis of the histopathological lung sections from the study suggested that RDLPM treatment markedly alleviated pulmonary edema, with less fluid exudation, compared with the other treatments used. In addition, it has been suggested that A. baumannii pneumonia directly stimulates leukocytosis in the blood.43,44 The RDLPMs significantly reduced the leukocyte levels compared with the control group.
In addition, it was found that RDLPMs significantly downregulated the expression of key inflammatory cytokines, TNF-α and IL-1β. This downregulation was significantly greater than rats treated with penicillin. Although penicillin showed better microbial inhibition than RDLPMs and Re in vivo, this was not the main mechanism by which Re treated A. baumannii pneumonia. To investigate the main mechanism by which Re treated bacterial pneumonia, the activation of the NF-κB pathway was explored. NF-κB, the nuclear transcription factor, is a key regulator of genes involved in response to infection, inflammation, and stress.45,46 NF-κB p65 is a dipolymer, combining with NF-κB. 47 The phosphorylation of p65 in the NF-κB pathway was markedly inhibited in the RDLPM and Re treatment groups; this led to lower levels of red fluorescence than the control group.
Penicillin seemed to have no significant effect on the phosphorylation of p65. This indicated that Re inhibits the NF-κB pathway and downregulates the expression of cytokines downstream of TNF-α and IL-1β. RDLPMs effectively enhanced Re's cellular bioavailability, as DPPC was able transform Re into the epithelial lining fluid and improve Re's cellular internalization. DPPC acts as a therapeutic agent by helping to improve the dysfunctional endogenous surfactant during infection; in addition, it worked as an excipient that helps the drug to pass through the PS. Meanwhile, the powder properties of the RDLPMs also helped the drug be effectively deposited in the lung. Therefore, RDLPMs may effectively improve drug delivery and become a therapeutic for A. baumannii-mediated pneumonia.
Conclusions
A novel, RDLPM, inhalable therapeutic was prepared for this study. The RDLPMs were small in size and showed a good fluidity and a low tapping density, which resulted in the appropriate ADs needed to achieve high levels of lung deposition. DPPC transmitted Re through the PS layer and improved lung absorption. Importantly, the RDLPMs showed higher in vivo anti-A. baumannii pneumonia effects than in vitro. Inhibition of NF-κB and inflammatory cytokines may be a major anti-A. baumannii pneumonia mechanism. These observations provide proof of the potential function of RDLPMs in the treatment of A. baumannii-mediated pneumonia. The RDLPMs will be appropriate for toxicological evaluation nonclinically and pharmacology evaluation to determine prophylactic versus therapeutic delivery in the future.
Footnotes
Data Availability
Supplementary Data associated with this article can be found in the online version (![]() ).
).
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
The work was supported by Shanghai Municipal Commission of Health and Family Planning (20184Y0227), Shanghai Natural Science Foundation (19ZR1450600), and Shanghai Yangpu Hospital Foundation (Se1202101).
Reviewed by:
Philip Kuehl
Tim Corcoran
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.