
Abstract
Background:
Suboptimal use of pressurized metered dose inhaler (pMDI) remains a major barrier to inhaled therapy success. Verbal inhaler technique training (VT) fails to maintain patients' good pMDI use, thus training tools might help. Trainhaler® (THR device) and Flo-Tone® CR (FTCR device), two novel pMDI technique training tools, were evaluated and compared in terms of relative lung and systemic bioavailability and oropharyngeal deposition of salbutamol inhaled from Ventolin® Evohaler® (GlaxoSmithKline) either alone following THR or connected to FTCR.
Methods:
Sixteen healthy adults inhaled 2 × 100 μg salbutamol puffs (1 minute apart) from Ventolin using the THR device or FTCR device in a two-period, randomized crossover study. A 7-day washout separated THR and FTCR approaches. Immediately after each puff inhalation, each subject gargled with 20 mL water for oropharyngeal deposition determination. Urine samples were collected 0.5 hour (pre-inhalation) and 0.5, 1.0, and 2.0 hours post-inhalation. Urine was then pooled till 24-hour post-inhalation. The relative lung bioavailability (0- to 0.5-hour urinary salbutamol excretion—USAL0.5) and relative systemic bioavailability (0- to 24-hour urinary excretion of salbutamol and its metabolite—USALMET24) were determined.
Results:
The mean (standard deviation [SD]) USAL0.5 of the THR and FTCR groups was 5.70 (6.43) and 11.39 (9.67) μg, respectively. The mean (SD) oropharyngeal deposition was 11.11 (4.37) and 6.09 (1.89) μg, respectively. The THR and FTCR devices were statistically significantly different in USAL0.5 and oropharyngeal deposition (p < 0.001), whereas there was no statistically significant difference in USALMET24.
Conclusion:
The THR device and the FTCR device showed positive impact on inhaled pMDI delivery. Indeed, the FTCR device doubled the relative lung bioavailability and minimized the unwanted oropharyngeal deposition of inhaled salbutamol. In practice, these pMDI trainers would complement and maintain VT.
Study Registration:
The study was registered on the ISRCTN registry (Reference: ISRCTN88332465-06/12/2017 [Prospectively Registered]).
Introduction
Patients' correct inhaler technique has been linked to various clinical outcomes of the inhaled therapy, including the level of respiratory disease control, risk of exacerbation, and frequency of hospitalization.1–3 Reading the manufacturer's inhaler use instructions can help; however, these instructions are not always clear to the patients and do not specify the critical nitty-gritty for adequate lung deposition. Verbal inhaler technique training (VT), by a health care professional either during clinic visits or when collecting the prescription from the pharmacy, has always been the traditional approach to refine and rectify the patients' inhaler technique.4–6
Although VT improves inhaler use, up to 90% of patients fail to remember the correct inhaler technique shortly after the training session.4–9 Pressurized metered dose inhalers (pMDIs) are key inhalers in the management of patients with obstructive respiratory conditions. 10 The variability among patients with poor pMDI critical maneuvers (specifically the inability to synchronize the start of a slow and deep inhalation through the inhaler with canister actuation, followed by up to a 10-second breath holding period) can, however, range between 10% and 95%. 11
Incorrect pMDI technique with quick inhalation flows would adversely result in higher oropharyngeal deposition and less than optimal lung delivery of inhaled medicines.10,12 The acceptable, slow inspiratory flow rates through pMDIs range between 30 and 60 L/min. 13 An ERS/ISAM task force consensus statement recommended that slow and deep inhalation through a pMDI should take an adult patient around 4–5 seconds. 14 Approximately one third of patients with asthma, however, had inhalation flow rates >60 L/min through their pressurized inhalers.15,16 Other studies showed that the majority of patients used their pMDIs with peak inhalation flows (PIFs) >100 L/min.4–6,8 This pMDI misuse is clinically associated with poor asthma control.8,16,17
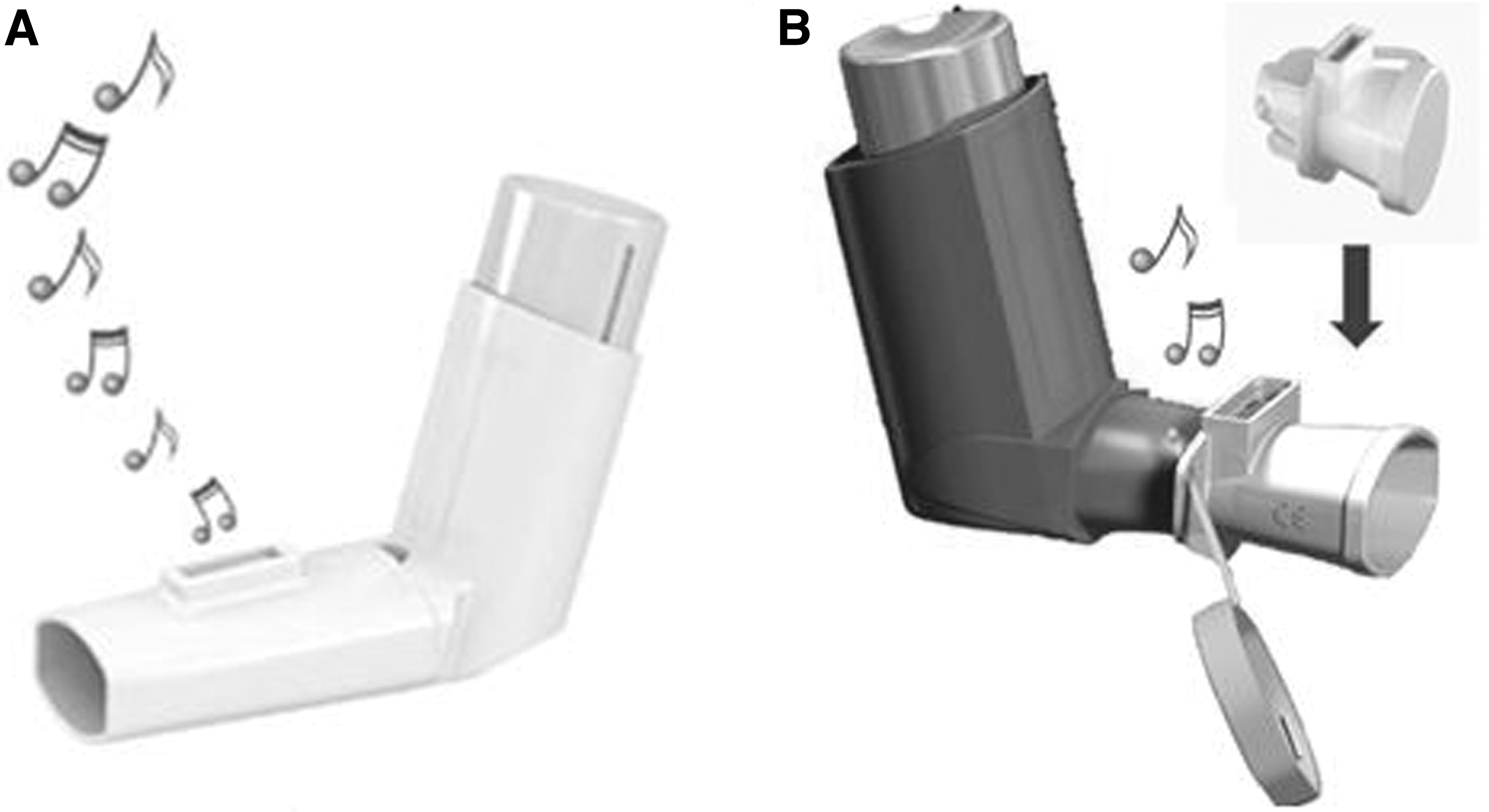
Various inhaler technique educational strategies, including repeated VT, have not improved the patients' inhaler use over the past 40 years. 18 Inhaler technique training tools designed with visual 19 and audible4,5,8 feedback mechanisms that reassure the patients and their caregivers of a correctly performed inhalation technique and flow rate through pMDIs have been shown clinically valuable.4–6,8,20,21 In this reference, Trainhaler® (THR device) and Flo-Tone® CR (FTCR device) (Clement Clarke International Limited, United Kingdom) (Fig. 1A and B, respectively) are two novel pMDI inhalation technique training devices (https://www.haag-streit.com/clement-clarke/products/inhaler-technique). The THR device produces two audible feedback sounds: a “whoosh” noise mimicking that of a real puff released from an actuated pMDI and a whistle sound when the correct, slow inhalation flow through the THR device is achieved. Patients are then instructed to simulate the THR device training when using their real pMDI. However, the FTCR device is designed as both a mini-spacer and pMDI trainer. Once attached to the mouthpiece of the inhaler, the FTCR device produces a whistle sound when the patient starts a slow inhalation through the pMDI giving the feedback signal to actuate the pMDI canister. The patient is trained to keep the whistle sound going throughout a slow and deep inhalation via their “pMDI plus FTCR device” setup. The FTCR device is designed with built-in controlled resistance that removes variability of the pMDIs internal resistance so the guidance whistle will respond at the same inhalation flow rate in all pMDIs irrespective of their individual resistance.
The THR
Clinically, both the THR and FTCR devices improved the overall pMDI technique, including the critical hand–lung coordination and slow inhalation flow maneuvers of asthmatic patients. 6 However, impact of the THR and FTCR devices use on relative lung and systemic bioavailability of inhaled products has not previously been investigated. The objective of the current study was, therefore, to evaluate and compare the THR device with the FTCR device in terms of the relative lung and systemic bioavailability of salbutamol inhaled by healthy adults from Ventolin® Evohaler® (GlaxoSmithKline) following training with the THR device or when connected to the FTCR device. Additionally, the oropharyngeal deposition of salbutamol was determined immediately after THR and FTCR inhalation.
Materials and Methods
Healthy, adult male subjects participated to help evaluating the THR device and the FTCR device pMDI technique training tools in a two-period, two-sequence, randomized, crossover pharmacokinetic study by assessing the relative lung and systemic bioavailability as well as the oropharyngeal deposition of salbutamol inhaled from a pMDI either following THR device training or when connected to FTCR device. Ventolin Evohaler (100 μg salbutamol per puff; GlaxoSmithKline) was used as the pMDI. A 1 week washout period separated the THR and FTCR training approaches. The study was conducted according to the ICH/Good Clinical Practice Guidelines. The subjects' inclusion and exclusion criteria, fundamental procedures, and methods in the current study protocol were similar to those used previously 22 ; however, the novel inhalation devices (the THR and FTCR devices) tested in the current work were different.
Our previous 22 and current study protocols were submitted for regulatory and ethical approvals under one application, hence the same approval and study registration reference numbers. The Jordan Food and Drug Administration (JFDA) (Ref.: 2/4/37/32225) and its Institutional Review Board (IRB) (Ref.: 694-2017/V04-12/03/17) approved the study. Moreover, the study was prospectively registered at the ISRCTN clinical study registry (Reference: ISRCTN88332465). All study participants gave written informed consents.
In summary, the study included adult (aged 18–50 years), male, nonsmoker, and healthy subjects. Subjects were excluded if they had any health-related issues, were using regularly any medications, nutritional or herbal products, and/or if it was difficult for them to follow the study procedures. The study subjects were not allowed to drink or eat alcohol-, caffeine-, and xanthine-containing products 48 hours before study drug administration and until the end of each study period. Additionally, food supplements and over-the-counter drugs were not allowed 1 week before the study participation began and until the study was complete. For pharmacovigilance purposes, body temperature, heart rate, and blood pressure were measured 1 hour (pre-drug) and 15, 45 and 120 minutes post-drug administration. Adverse effects throughout the study (if any) were documented. The lung function of the subjects was assessed (forced expiratory volume in 1 second as percent predicted [FEV1% predicted]) 1 hour (pre-) and 2 hours after salbutamol administration.
The study procedures involved subjects' confinement at the study site ∼12 hours before and until 24 hours after salbutamol administration. The subjects were rigorously trained on their assigned pMDI technique training tool (THR device or FTCR device) and were allowed to demonstrate their trained inhalation approach using a placebo pMDI either alone (following training with the THR device) or connected to FTCR device (according to study randomization) until satisfactory inhalation technique was achieved. The subjects' PIF through the pMDI was then measured using an In-Check Dial® flow meter (Clement Clarke International Limited) to evaluate the given inhaler training approach in terms of a slow inhalation between 30 and 60 L/min. Subjects randomized to the THR device were verbally trained according to the THR device manufacturer's instructions and the recommended pMDI technique steps.4,5,8
In summary, after shaking the inhaler and exhaling gently to empty their lungs, the subjects were instructed to depress the pMDI canister immediately after starting a slow and deep inhalation maneuver through the inhaler till their lungs were full of air. They were then asked to remove the inhaler from their mouth, close their lips tightly, and hold their breath as long as they can (up to 10 seconds if possible) before breathing out gently. To ensure a slow and deep inspiration, the subjects were trained to count slowly to 5 seconds during the inhalation maneuver. 14 Subjects randomized to the FTCR device were trained to use the pMDI connected to FTCR device according to the manufacturer's instructions focusing on the slow and deep inhalation (counting slowly to 5 seconds) and the subsequent breath holding maneuvers.
The study procedures to determine the salbutamol oropharyngeal deposition following inhalation were similar to those previously used. 22 Ventolin pMDIs were first prepared for use according to the manufacturers' instructions. Each subject inhaled 2 × 100 μg puffs from a Ventolin Evohaler separated by ∼1 minute using the assigned THR or FTCR approach. Immediately after each puff inhalation, the subject mouth-washed and gargled with 20 mL bottled water (Nestle® Pure Life; Ghadeer Mineral Water Co., Jordan), which were combined together, stored at −20°C, and then analyzed for salbutamol to determine its oropharyngeal deposition.
The relative lung and systemic bioavailability of salbutamol post-inhalation were determined based on a previously developed and validated urinary salbutamol excretion pharmacokinetic method. 23 This pharmacokinetic method has been widely used to investigate optimal inhaler technique through pressurized13,24 and dry powder inhalers, 25 compare different spacer devices, 26 compare spacer with jet nebulizer devices, 27 and has been extended to evaluate the relative lung and systemic bioavailability of inhaled terbutaline. 28 More recently, this urinary salbutamol excretion method was used to evaluate an improved spacer device engineered with a special polymer that incorporates silver ion antimicrobial technology. 22 Similar to the protocol of that work, 22 each subject in the current study emptied their bladder 0.5 hour before drug administration (pretreatment urine sample).
Urine samples were then collected 0.5, 1.0, and 2.0 hours post-salbutamol inhalation. Subsequently, each subject pooled their urine 2- to 24-hour post-salbutamol inhalation. The volume and pH of each urine sample were recorded. All urine samples were stored at −20°C until extracted and analyzed by a previously, in-house developed and validated high-performance liquid chromatography–tandem mass spectroscopy technique. 22 The salbutamol excreted in urine within 30 minutes post-inhalation (USAL0.5) represents the relative lung bioavailability. While the total amount of parent salbutamol and its sulfate ester metabolite excreted in urine 0- to 24-hour post-inhalation (USALMET24) represents salbutamol's relative systemic bioavailability.
The same subject group that participated in our previous study 22 has been approached and agreed to take part in the current study, hence the identical reported subjects' descriptive data (mean [standard deviation, SD] age, height, weight, and body mass index) to those in the previous work. 22 Those same individuals were invited to participate in the present study because they fulfilled the protocol inclusion criteria, were previously educated on Ventolin pMDI (pharmacological indications and potential adverse effects), and inhaled salbutamol without any adverse effects being reported in the previous study they participated in. Moreover, those subjects were already familiar with the general protocol environment and procedures including the need to be confined at the clinical site throughout each of the two study periods, and that they appreciated how the urine samples collection and time intervals were critical to the study results.
In this context, recruiting the same subject group minimized the chances of subjects' withdrawal from the study. However, the tested inhaler technique training interventions/devices in the two studies were completely different; traditional verbal pMDI technique training versus Able® Spacer device in the previous study. 22 While the tested devices in the current study were the THR device versus the FTCR device. Despite repeated inhaler technique training, many patients prescribed inhaler therapy forget the correct inhaler use with time after the training session. 14 In the current study, the subjects were trained on their assigned tested devices by using the manufacturer's instruction in the package inserts. Moreover, the study subjects were healthy and inhaler technique naive; thus, it was unlikely that there was a training effect across the study periods that would have affected the study results.
The IBM SPSS for Windows software (version 20) was used for the statistical analysis of the study results. A p-value of <0.05 was considered statistically significant for any differences.
Results
A total of 16 healthy male subjects participated in this study. Their mean (SD) age, height, weight, and body mass index were 29.4 (9.7) years, 1.80 (0.1) m, 81.4 (15.2) kg, and 25.4 (3.7) kg/m2, respectively. All subjects had normal medical, physical, and laboratory examinations at both study enrolment and completion. No adverse effects were reported throughout the study. The mean (SD) PIFs through pMDI following the THR device and FTCR device training were 50.4 (9.0) and 46.6 (9.4) L/min, respectively, with no significant difference [paired samples t-test: t(15) = 1.351, p = 0.197].
In reference to the lung function, the mean (SD) baseline FEV1% predicted before the THR device and FTCR device salbutamol inhalation was 95.4% (3.1) and 95.9% (2.7), respectively. The mean (SD) FEV1% predicted measured 2 hours post-inhalation was 98.7% (2.5) and 98.7% (2.7), respectively. The FEV1% predicted pre- and post-salbutamol administration showed no statistical difference within the THR and FTCR devices; Paired samples t-tests were: t(15) = −1.89 (p = 0.079) and t(15) = −1.49 (p = 0.157), respectively. The pH of all urine samples ranged between 5.0 and 8.0.
Table 1 summarizes the recovered unchanged salbutamol amounts deposited in the oropharyngeal region, as well as that was renally excreted 0.5, 1.0, and 2.0 hours and subsequently until 24 hours post-THR and FTCR inhalations. Table 2 presents the mean (SD) of total salbutamol (salbutamol and its metabolite) excreted in urine 0.5 to 24 hours post-salbutamol inhalation. Figures 2, 3, and 4 demonstrate each participant's oropharyngeal deposition, USAL0.5, and USALMET24 following THR and FTCR, respectively. Wilcoxon comparisons between the THR and FTCR devices showed significant differences in oropharyngeal deposition (Wilcoxon Z = −3.21; p < 0.001) and in USAL0.5 (Wilcoxon Z = −3.46; p < 0.001). The THR and FTCR devices, however, resulted in no statistical difference for the USALMET24 (Wilcoxon Z = −0.57; p = 0.569).
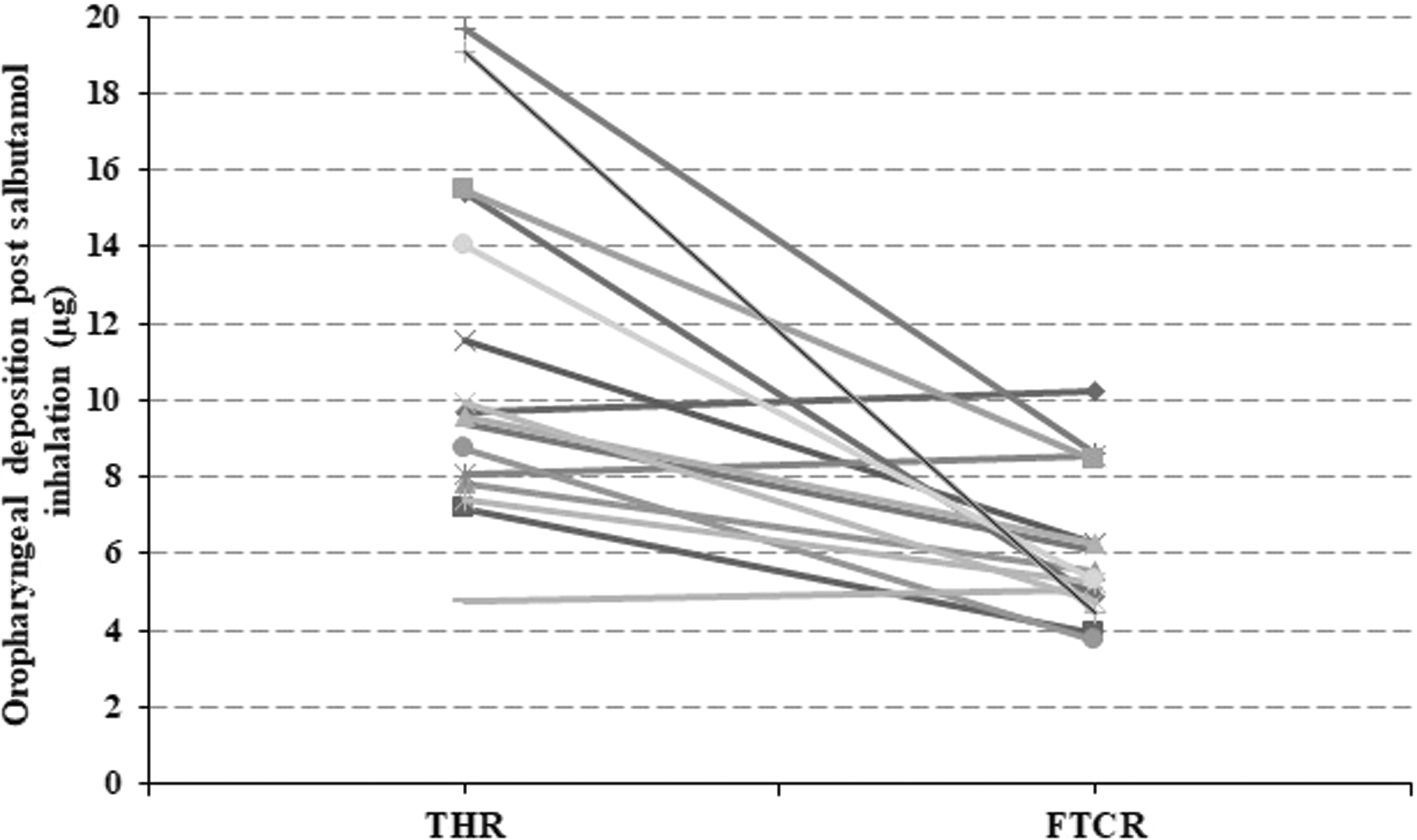
Individual oropharyngeal deposition of salbutamol post-inhalation.

Participants' relative pulmonary salbutamol bioavailability (USAL0.5).

Participants' relative systemic salbutamol bioavailability (USALMET24).
Mean (Standard Deviation) Amount (μg) of Unmetabolized Salbutamol Recovered in the Samples of 16 Healthy Subjects After Inhaling 2 Puffs (100 μg Each) of Salbutamol
USAL0.5 represents relative lung bioavailability of inhaled salbutamol.
FTCR, Flo-Tone® CR; SD, standard deviation; THR, Trainhaler®.
Total Salbutamol (Salbutamol Plus Its Metabolite) Renally Recovered After Inhaling Two Puffs (100 μg Each) of Salbutamol
USALMET24 = USAL0.5+USALMET0.5–24 (which represents the relative systemic bioavailability of inhaled salbutamol).
Discussion
The fate of orally inhaled products is generally split between oropharyngeal impaction, central, and peripheral lung deposition. Improving the latter would maximize the pharmacotherapeutic benefit of the inhaler therapy. 29 Whereas local and systemic adverse effects are linked substantially to the oropharyngeal and upper respiratory tract drug deposition following inhalation.29,30 In this regard, it is crucial that patients remember to use their pMDIs correctly and consistently including a slow and deep inhalation flow (≤60 L/min) through the inhaler.1,11 Unfortunately, the majority of patients inhale at much faster speeds through their pressurized inhalers5,9,15 despite having received repeated VT. 31
The present study subjects were trained to use two novel pMDI technique and inhalation training devices in an investigational, two-period, crossover, randomized comparative study. Both the relative lung and systemic bioavailability were compared following salbutamol inhalation using the previously, well-established urinary salbutamol excretion pharmacokinetic method.13,23,26 Within the pH range (5.0–8.0) of the urine samples, it is unlikely that salbutamol exhibits significant pH-dependent renal clearance.23,32 Additionally, the salbutamol oropharyngeal deposition was measured immediately following the THR device and FTCR device approaches.
The subjects' mean PIF through the pMDI was sufficiently slow and comparable after the THR device and FTCR device training: 50.4 and 46.6 L/min, respectively. In this respect, it has been recently shown that the verbal pMDI technique training, THR device and FTCR device significantly improved and comparably maintained the acceptable inhaler use, including the PIF through the pMDI, in asthmatic patients. 6 Moreover, inhaler technique training tools complemented the conventional pMDI VT in patients with asthma.4–6 Thus, the THR and FTCR tools can have a useful role in maintaining the correct inhaler use of patients particularly with the limited access to health care settings since the COVID-19 pandemic has impacted consultation.
Following the THR device training, the oropharyngeal deposition of inhaled salbutamol was 5.56% of the nominal Ventolin Evohaler dose. Previous, rigorous VT training, however, resulted in comparable oropharyngeal deposition (5.67%) following Ventolin Evohaler inhalation by the same subject group. 22 However, inhalation through the FTCR device connected to the Ventolin Evohaler did halve the oropharyngeal deposition (3.0% of the nominal dose) compared with either the THR device or VT alone. Even with optimal pMDI use, a great percentage (∼80%) of the inhaled aerosol dose potentially impacts on the back of the mouth and the pharynx contributing to both local and systemic adverse effects. 33 Valved holding chambers (VHC) and spacer devices connected to pMDIs, however, reduce the oropharyngeal deposition and thus minimize these unwanted adverse effects. 34 Privileged with its mini size, the FTCR device offers the benefit of a spacer device 22 without having the bulky size that most patients complain about when carrying around their spacer devices. 35
The THR device trainer resulted in a relative lung bioavailability (% nominal dose) of 5.70 μg (2.85%). Previous 30-minute urinary salbutamol pharmacokinetic studies showed that thoroughly verbally trained and closely observed subjects did not have statistical difference in relative lung bioavailability after Ventolin pMDI inhalation: 2.83% 26 and 2.68% 22 of the nominal dose. It is well documented, however, that the VT patients receive on the correct inhaler technique decays gradually with time,5,18,3637 hence the advantage of having an inhaler technique training tool, such as the THR device, around to improve and maintain the patients' correct inhaler use regularly and in between routine clinic visits.
Training the subjects to inhale through the FTCR device connected to Ventolin Evohaler significantly doubled the relative lung bioavailability of inhaled salbutamol (mean USAL0.5 [% nominal dose]: 11.39 μg [5.69%]). Our findings are in line with previously reported relative lung bioavailability of salbutamol inhaled through Ventolin pMDI connected to a VHC: Volumatic® Spacer (16.4 μg [8.2%]), 38 AeroChamber Plus® spacer (14.8 μg [7.4%]), 38 and recently Able Spacer (12.80 μg [6.4%]). 22
Both the THR and FTCR devices resulted in comparable relative salbutamol systemic bioavailability identified by USALMET24 alone and when oropharyngeally deposited salbutamol was included. Moreover, the relative systemic bioavailability of salbutamol following THR and FTCR use was not statistically different from those achieved previously following VT (25.0% of nominal dose, p = 0.078) and Able Spacer (33.1% of nominal dose, p = 0.352) inhalation, 22 respectively. Inhalation through large Volumatic and small AeroChamber Plus VHC showed no difference in the relative salbutamol systemic bioavailability compared with inhalation from Ventolin pMDI alone. 38
Conclusion
The efficacy, safety, and patient compliance of pMDI therapy are adversely impacted by suboptimal or incorrect pMDI technique and inhalation flow. Despite improving the patients' pMDI technique, VT is effort/time-consuming and consistently fails to maintain correct inhaler use. THR and FTCR tools complement VT. Moreover, as personal pressurized inhaler trainers, both the THR and FTCR devices have the privilege of sustaining good pMDI technique including the critical hand–lung coordination and slow inhalation flow maneuvers. The FTCR device, as a mini-spacer, has shown comparable performance to the bulky spacer devices in terms of minimizing the oropharyngeal deposition and maximizing the relative lung bioavailability.
The prospect of being able to reduce unwanted oropharyngeal deposition while simultaneously providing acoustic inhaler technique guidance makes the FTCR device a potentially useful add-on for routine treatment. The impact of this on retention of good inhaler technique could be explored in future studies.
Footnotes
Authors' Contributions
W.G.A.: Conceptualization, study design, project administration, data acquisition, statistical analysis and interpretation, and drafting original article. M.S.: Study design, logistical resources, and drafting and critically revising original draft. All authors approved the final article version.
Acknowledgments
Thank you to all the subjects who took part in this study and to the medical and technical staff for their assistance. The authors would also like to thank Al-Ahliyya Amman University, Jordan and Clement Clarke International Limited, United Kingdom, for their supportive roles.
Author Disclosure Statement
W.G.A. is an Academic Researcher in the inhaled respiratory medicine and inhaler devices areas. He has received unconditional travel grants from Clement Clarke International Limited to present his research work at ATS, BTS, ERS, and ISAM conferences. M.S. was the Chief Technology Officer at Clement Clarke International Limited, United Kingdom, now retired.
Funding Information
This academically initiated, designed, and conducted research study was unconditionally supported by Clement Clarke International Limited, United Kingdom.
Reviewed by:
Kurt Nikander
Henry Chrystyn