
Abstract
Background:
Idiopathic pulmonary fibrosis (IPF) is a serious lung disease characterized by lung scarring, which results in breathing difficulty. Currently, patients with IPF exhibit a poor survival rate and have access to very limited therapeutic options. Interferon beta (IFN-β) has been approved by the U.S. Food and Drug Administration (FDA) for the treatment of relapsing forms of multiple sclerosis, and it has also been shown to exhibit therapeutic potential in IPF. However, clinical use of IFN-β did not lead to improved overall survival in IPF patients in existing studies. One possibility is the limited efficiency of IFN-β delivery through intravenous or subcutaneous injection.
Materials and Methods:
The aerosol particle size distribution was determined with a laser diffraction particle size analyzer to characterize the droplet size and fine particle fraction generated by three types of nebulizers: jet, ultrasonic, and mesh. A breathing simulator was used to assess the delivery efficiency of IFN-β, and the temperature in the medication reservoirs was monitored with a thermocouple during nebulization. To further evaluate the antifibrotic activity of IFN-β pre- and postnebulization, bleomycin (BLM)- or transforming growth factor-beta (TGF-β)-treated human lung fibroblast (HLF) cells were used. Cell viability was measured by 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) assay. Transwell migration assay and Q-PCR analysis were used to evaluate cell migration and the myofibroblast differentiation ability, respectively. IFN-β protein samples were prepared using sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE) sample loading buffer, and the expression of IFN-β was assessed by western blotting.
Results:
Among the current drug delivery systems, aerosolized medication has shown increased efficacy of drug delivery for treating respiratory diseases when compared with parenteral drugs. It was found that neither the structural integrity nor the biological function of nebulized IFN-β was compromised by the nebulization process of the mesh nebulizer. In addition, in BLM dose–response or TGF-β-induced lung fibroblast proliferation assays, these effects could be reversed by both parenteral and inhaled IFN-β nebulized with the mesh nebulizer. Nebulized IFN-β with the mesh nebulizer also significantly inhibited the migration and myofibroblast differentiation ability of TGF-β-treated HLF cells.
Conclusions:
The investigations revealed the potential efficacy of IFN-β in the treatment of IPF with the mesh nebulizer, demonstrating the higher efficiency of IFN-β delivered through the mesh nebulizer.
Background
Idiopathic pulmonary fibrosis (IPF), which is considered the most common type of idiopathic interstitial pneumonia, is a progressive chronic disease characterized by irreversible lung scarring that results in the destruction of the alveolar architecture in the lungs.1–3 The worldwide incidence rate of IPF has increased over the past few decades.4–6 Patients with this disease have been found to have a median survival rate between 2.5 and 3.5 years after diagnosis. 6 The persistent proliferation of fibroblasts observed in IPF patients is the main cause leading to alveolar scarring. With the progression of fibroblast proliferation, the scarring extends to adjacent alveolar sacs, enhancing extracellular matrix deposition, and generating dead space characterized by hypoxia. 7
Since the discovery of its pathogenesis, the treatment of IPF has shifted from initial attends, which handled the condition as a chronic inflammatory disease, to recent therapies that focus on molecular pathways to halt the expansion of fibrosis progression while alleviating some of the symptoms. 8 Nintedanib is a tyrosine kinase inhibitor that was approved for the treatment of IPF in the United States and in the EU. 9 Some recent approaches based on antifibrotic remedies involving pirfenidone, interferon-gamma (IFN-γ), and interferon-beta (IFN-β) show promise, especially when combined with one another.10–14 Among the three abovementioned approaches, IFN-γ is the most well-studied agent for IPF treatment. IFN-β has been shown to assist in the reduction of fibroblast proliferation and, therefore, could be highly beneficial in the treatment of IPF. 15 It has also been reported that IFN-β is able to exert antifibrotic effects by inhibiting transforming growth factor-beta (TGF-β) and attenuating procollagen mRNA expression and collagen synthesis. 10
Although most treatments involving biologic drugs are administered by parenteral injection, new therapies have demonstrated that the selection of an effective delivery route is crucial for achieving the targeted therapeutic effects.16,17 Nebulizers are pulmonary delivery systems that aerosolize liquid medications. They can be categorized into three main groups with regard to their operational mechanism: jet nebulizers, ultrasonic nebulizers, and vibrating mesh nebulizers.18,19 Jet and ultrasonic nebulizers are devices that were launched several decades ago and can convert liquid medications into aerosols by using compressed air and high-frequency sound waves, respectively.20,21 The newer mesh nebulizers, initially marketed in 1993, use a mesh membrane that contains thousands of small pores; aerosolization of liquid medications is driven by a piezoelectric component, generating a fine mist that can be deeply inhaled and deposited into the lungs. 19
The introduction of mesh technology has made it possible to deliver a wider range of medications with enhanced drug delivery efficiency, which requires droplet sizes within the respirable range of 1–5 μm in diameter, and a reduced residual volume. 22 Mesh nebulizers are also favored for their advantages of quiet operation and portability. 23 With regard to nebulizing biologic drugs, mesh nebulizers have been praised for their capabilities. However, particular attention should still be devoted to the existence of detrimental forces, such as heat and shear forces, because they may lead to aggregation and denaturation of biologic drugs. 24 These issues were initially reported with jet and ultrasonic nebulizers.25–27 Consequently, formulation development also plays a key role in drug–device combination assessment. 28
In the past decade, several drugs for administration with mesh nebulizers have been approved by the U.S. Food and Drug Administration (FDA) and other regulatory agencies as combination products to treat respiratory diseases. This is due to customization capabilities within the device platforms that allow control of aerosol characterization. This study focused on investigating the aerosol performance of three nebulizers in the delivery of an IFN-β formulation and examining the biologic drug's stability and bioactivity postnebulization from collected aerosols compared with those of the control. It has previously been reported that a temperature increase can be observed in ultrasonic nebulizers; thus, to evaluate factors that could be detrimental to biologic formulations, such as IFN-β, the temperature change was assessed when nebulizing with all three devices. 29
Bleomycin (BLM), an anticancer chemotherapy drug known for inducing pulmonary fibrosis in vitro and in vivo, was added to the medium to culture a fibroblast cell line and induce proliferation as the testing model.30–32 Nebulized and non-nebulized IFN-β were used to treat the different groups of cell lines to measure its capability to inhibit fibroblast proliferation as an attempt to improve the treatment of IPF.
Materials and Methods
Materials
REBIF® (132 μg/1.5 mL per vial), an IFN-β-1a solution for injection (Merck, Feltham, UK), was used to perform aerosol characterization studies and temperature change assessment after dilution from 88 to 14.66 μg/mL with water for injection. BLM was purchased from Selleck Chemicals (Pittsburgh, PA). Recombinant human TGF-β was purchased from PeproTech (Rocky Hill, NJ). Trypsin-EDTA solution (0.25%) was purchased from Thermo Fisher Scientific (Waltham, MA). The 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) and dimethyl sulfoxide (DMSO) were purchased from Sigma-Aldrich (Burlington, MA).
Aerosol characterization
Three nebulizers, a PARI LC® Sprint in combination with a PARI BOY® SX compressor (jet nebulizer; PARI Pharma GmbH, Starnberg, Germany), an APEX San-up 3042 (ultrasonic nebulizer; APEX, Argentina), and an HCmed Pulmogine® (mesh nebulizer; HCmed Innovations Co., Ltd., Taipei, Taiwan), were loaded with 2 mL of 14.66 μg/mL IFN-β-1a for each run. Three replicates were conducted to assess aerosol characterization with a Malvern Spraytec laser diffraction size analyzer (w/o inhalation cell; Malvern Instruments Ltd., UK) to record the median particle size by volume (DV50), fine particle fraction (FPF; the proportion of emitted particles that have a particle size of less than 5 μm in diameter), and geometric standard deviation (GSD). A Copley BRS2000 breathing simulator (Copley Scientific, Munich, Germany) was used to determine the delivered dose (DD), total output rate (TOR), treatment time (TT), and residual mass (gravimetrically) with the three nebulizers in triplicate and in accordance with the U.S. Pharmacopoeia <1601> for the adult breathing pattern (volume: 500 mL; frequency: 15 cycles/min; waveform: sinusoidal; inspiration/expiration ratio = 1:1).
For assessment of the DD, each filter membrane in the holder connected to the breathing simulator was removed and washed with 0.9% saline solution. The amount of IFN-β-1a in the collected samples was assessed using high-performance liquid chromatography (HPLC).
Assessment of temperature inside nebulizer reservoirs
A thermocouple connected to a portable digital thermometer (Maxthermo® S-506, Maxthermo, New Taipei, Taiwan) was used to measure the temperature inside the medication containers every 30 seconds throughout the treatment period. For the jet nebulizer, the thermocouple was placed inside the medication handset in direct contact with the formulation. For the ultrasonic and vibrating mesh nebulizers, the thermocouple was placed in direct contact with the crystal and stainless steel plates, respectively. Tests of the three nebulizers were conducted in triplicate. The heating rate was computed as a function of the recorded temperature values against the TT.
Preparation of nebulized IFN-β for treating human lung fibroblast cells
Human lung fibroblast (HLF) cells were purchased from Lonza (Walkersville, MD). HLF cells were cultivated in fibroblast growth medium-2 (FGM-2) (Lonza), and cells at passages 3 to 10 were used in this study. Cells were incubated at 37°C in a humidified incubator containing 20% O2 and 5% CO2. Nebulization of IFN-β was performed with three different types of nebulizers: a jet nebulizer, an ultrasonic nebulizer, and a mesh nebulizer. Nebulized IFN-β was collected by spraying into a 50-mL centrifuge tube containing FGM-2. After brief centrifugation and gentle mixing, HLF cells were cultured in FGM-2 with the indicated doses of nebulized IFN-β. In vitro functional assays were performed to study the effects of nebulized IFN-β on the cell proliferation, migration, and myofibroblast differentiation abilities (Fig. 3A).
Cell proliferation assay
HLF cells were seeded at a density of 5000 cells/well in 96-well plates and maintained for 14–16 hours in the incubator before treatment with the test compounds. After 48 hours of incubation, the cells were washed with phosphate-buffered saline (PBS), and FGM-2 containing MTT reagent at a final concentration of 0.5 mg/mL was added for a 4-hour incubation. Then, the medium was replaced with medium containing 200 μL of DMSO for 30 minutes of incubation. The absorbance at 570 nm was measured in a multiwell plate reader. The half-maximal inhibitory concentration (IC50) for cell death was calculated with SigmaPlot (version 10; Systat Software, San Jose, CA).
Transwell migration assay
HLF cells were suspended in serum-free FGM-2 and placed in the upper chamber of the culture insert. Complete FGM-2 was added to the lower chamber, and the cells were incubated at 37°C for 24 hours. The cells attached to the lower surface of the membrane were stained with Crystal Violet, and cells in 5–10 randomly selected fields were counted. Three independent experiments were performed. Quantification was carried out by ImageJ analysis software (National Institutes of Health, Bethesda, MD).
Real-time polymerase chain reaction
Total RNA was isolated using TRIzol reagent. Reverse transcription into cDNA was performed with 2 μg of total RNA using oligo-dT primers. Real-time PCR was performed with cDNA samples using the ABI Prism 7900 Sequence Detection System (Applied Biosystems, Waltham, MA). Expression levels were normalized to GAPDH.
Western blot analysis
Electrophoresis was carried out using 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE). Nebulization of IFN-β was performed with three different types of nebulizers: a jet nebulizer, an ultrasonic nebulizer, and a mesh nebulizer. Aerosol droplets were collected in polypropylene tubes. The concentration of IFN-β was measured by Protein Assay Dye Reagent Concentrate (Bio-Rad Laboratories, Hercules, CA). A standard curve was generated using a series of IFN-β standards in the 0.01 to 1 μg/mL range. IFN-β protein samples (0.385 μg) were prepared for SDS-PAGE using 4X SDS-PAGE sample loading buffer (Bio-Rad Laboratories), and the mixtures with 4X SDS-PAGE sample loading buffer were heated at 95°C for 10 minutes in a heat block before being loaded onto an SDS polyacrylamide gel. Immunoblotting was performed using an antibody specific for IFN-β (ABclonal Technology, Woburn, MA) to evaluate the expression of IFN-β. Western blotting images were acquired using the UVP BioSpectrum Imaging System (Thermo Fisher Scientific).
Statistical analyses
SPSS (SPSS, Inc.) was used for statistical analyses, which included Student's t-test, with statistical significance defined as p < 0.05 (* or #), p < 0.01 (** or ##), and p < 0.001 (***or ###). The data shown are representative of at least three independent experiments. Quantitative data are presented as the mean ± standard deviation (SD) values.
Results
Aerosol characterization
The mean values and SDs of the parameters measured with the laser diffraction particle size analyzer are shown in Table 1. The mean DV50 value obtained with the mesh nebulizer was 4.019 μm, which is within the respirable range of 1 to 5 μm; however, the mean DV50 values obtained with the jet and ultrasonic nebulizers were slightly above the respirable range: 5.491 and 5.433 μm, respectively. The FPF for the mesh nebulizer was higher than the values for the other two devices, as the FPF is inversely proportional to the DV50, whereas the mean GSD values of all devices ranged between 1.668 and 1.980, with lower GSDs for the jet and mesh nebulizers.
Particle Size Distribution Analysis Summary
FPF, fine particle fraction; GSD, geometric standard deviation.
The DD from the three nebulizers was assessed with a breathing simulator and quantified by HPLC. The mean values and SDs recorded during testing with the breathing simulator are shown in Table 2. The TT for the jet and ultrasonic nebulizers was recorded from the moment the nebulizers were started until a sputtering noise began. However, the mesh nebulizer relied on a liquid detector to stop aerosol generation at the end of each treatment. The shorter TT of the jet and ultrasonic nebulizers could be associated with the lower nebulized volume—between 45% and 60% of the total volume, compared with the 95% achieved with the mesh device. The DD assessed using HPLC revealed that the ultrasonic nebulizer delivered only 6.26% of the loaded API, while the jet and mesh nebulizers delivered more than three times more API.
Breathing Simulation Testing to Assess Delivered Dose (Fill Volume: 2 mL)
DD, delivered dose; TOR, total output rate; TT, treatment time.
Temperature testing
The thermocouple was placed close to the aerosol generation source to assess temperature changes during nebulization, as shown in Figure 1. Temperature testing showed that the jet nebulizer did not cause any temperature increase during nebulization. The mean temperature of the replicates decreased by 5.9°C. In contrast, for the ultrasonic and mesh nebulizers, the temperature increased by 12.7°C and 7.2°C, respectively. The temperatures during testing are shown in Figure 2. The initial recorded reservoir temperatures after loading the formulation in the jet, ultrasonic, and mesh nebulizers were 23.4°C, 22.6°C, and 22.9°C, respectively.

Thermocouple position during temperature testing.
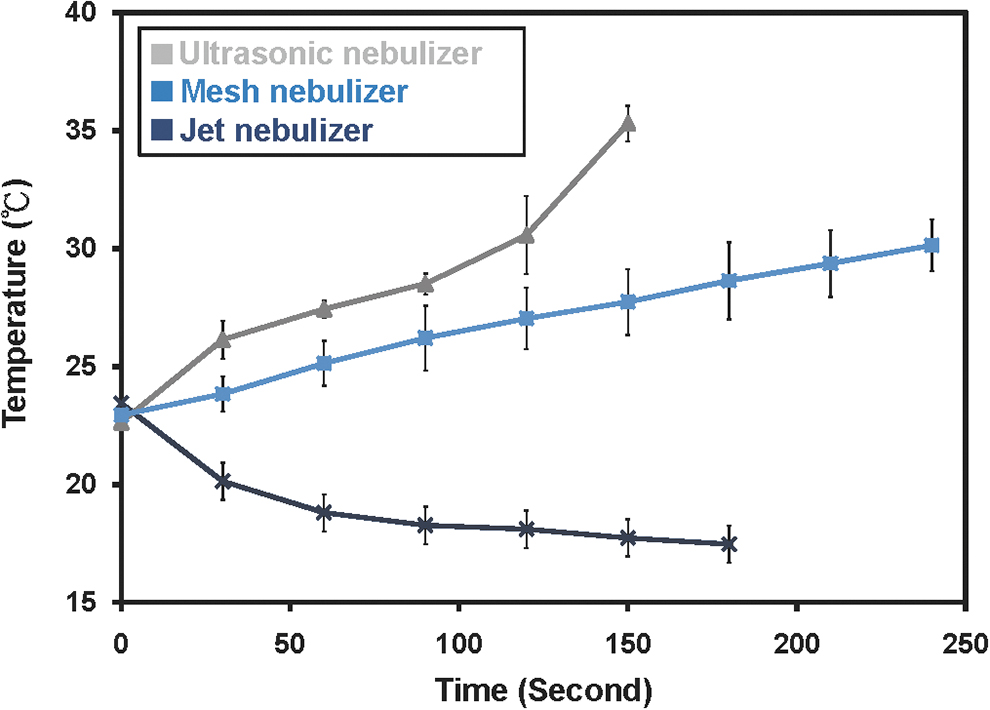
Temperature change during nebulization with the jet, ultrasonic, and mesh nebulizers.
Suppression of human lung fibroblast proliferation by IFN-β
To investigate the therapeutic effects of nebulized IFN-β of lung fibrosis, the three different types of nebulizers and HLF cells were used (Fig. 3A, B). Parenteral IFN-β (non-nebulized) treatment reduced the proliferation of HLF cells in a dose-dependent manner (Fig. 3C, D). Notably, the mesh nebulizer increased the therapeutic effects of IFN-β on HLF cells, whereas IFN-β nebulized using the jet and ultrasonic nebulizers reduced the effects of IFN-β on suppressing HLF cell proliferation (Fig. 3B, C).
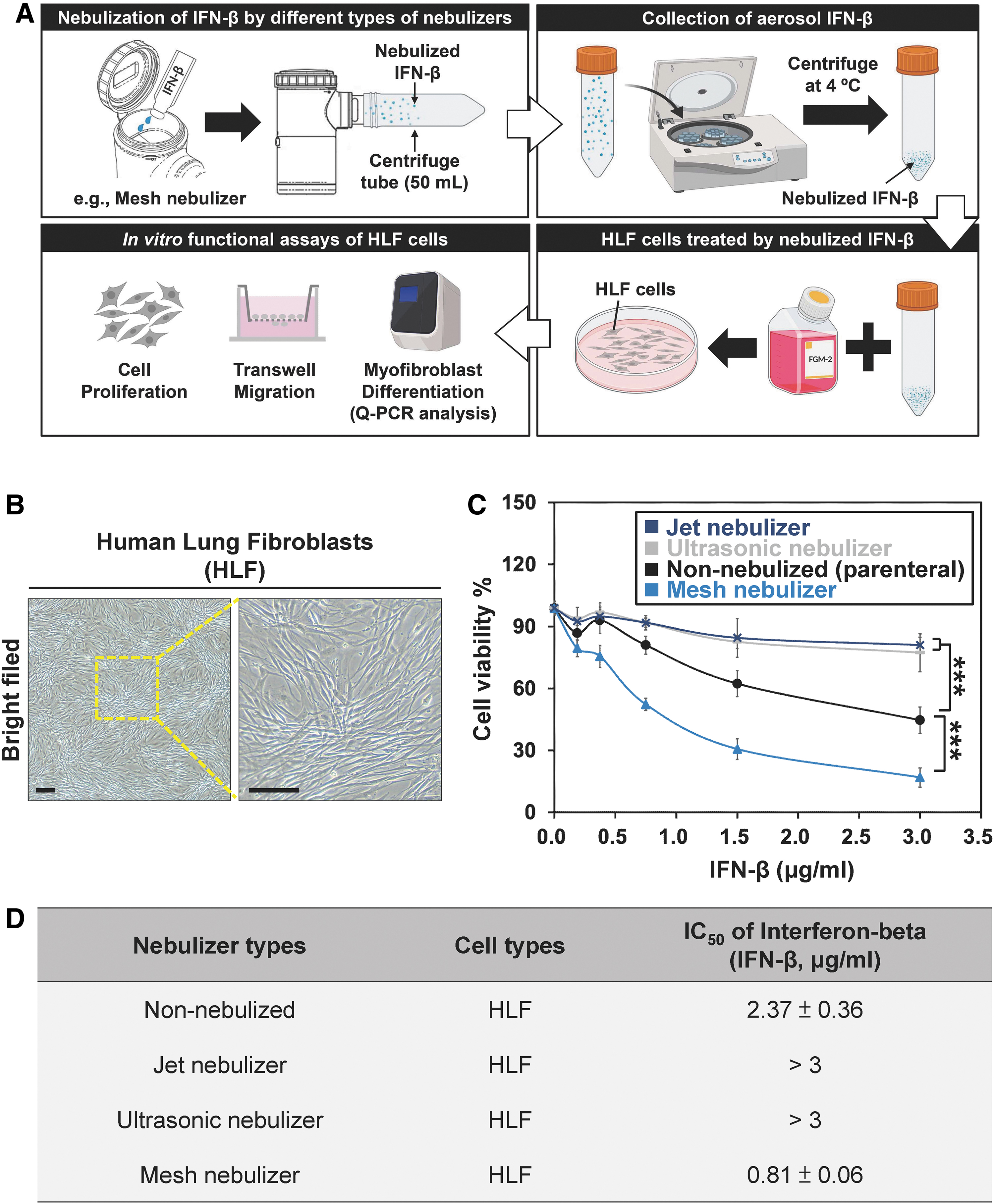
Effects of parenteral and nebulized IFN-β on the proliferation of human lung fibroblast cells.
By facilitating the proliferation of HLF cells by BLM or TGF-β treatment, the therapeutic effects of IFN-β on cell growth in HLF cells were then studied. For this study, IFN-β at a concentration of 187.5 ng/mL, which demonstrated no significant cytotoxic effects on HLF cell proliferation, was chosen for cotreatment with BLM or TGF-β. This concentration also represents a clinically relevant concentration of IFN-β. 33 BLM was found to dose dependently increase cell proliferation in HLF cells, and parenteral IFN-β rescued the BLM-mediated effects (Fig. 4A, B). IFN-β nebulized using the mesh nebulizer showed more potent rescue effects than parenteral IFN-β, while IFN-β nebulized using the jet or ultrasonic nebulizer did not inhibit HLF cell proliferation (Fig. 4B). In addition to BLM, TGF-β is one of the most potent inducers of lung fibrosis. 34 TGF-β stimulation dose dependently induced the proliferation of HLF cells (Fig. 4C). Parenteral IFN-β treatment also abolished the effects of TGF-β (Fig. 4D).
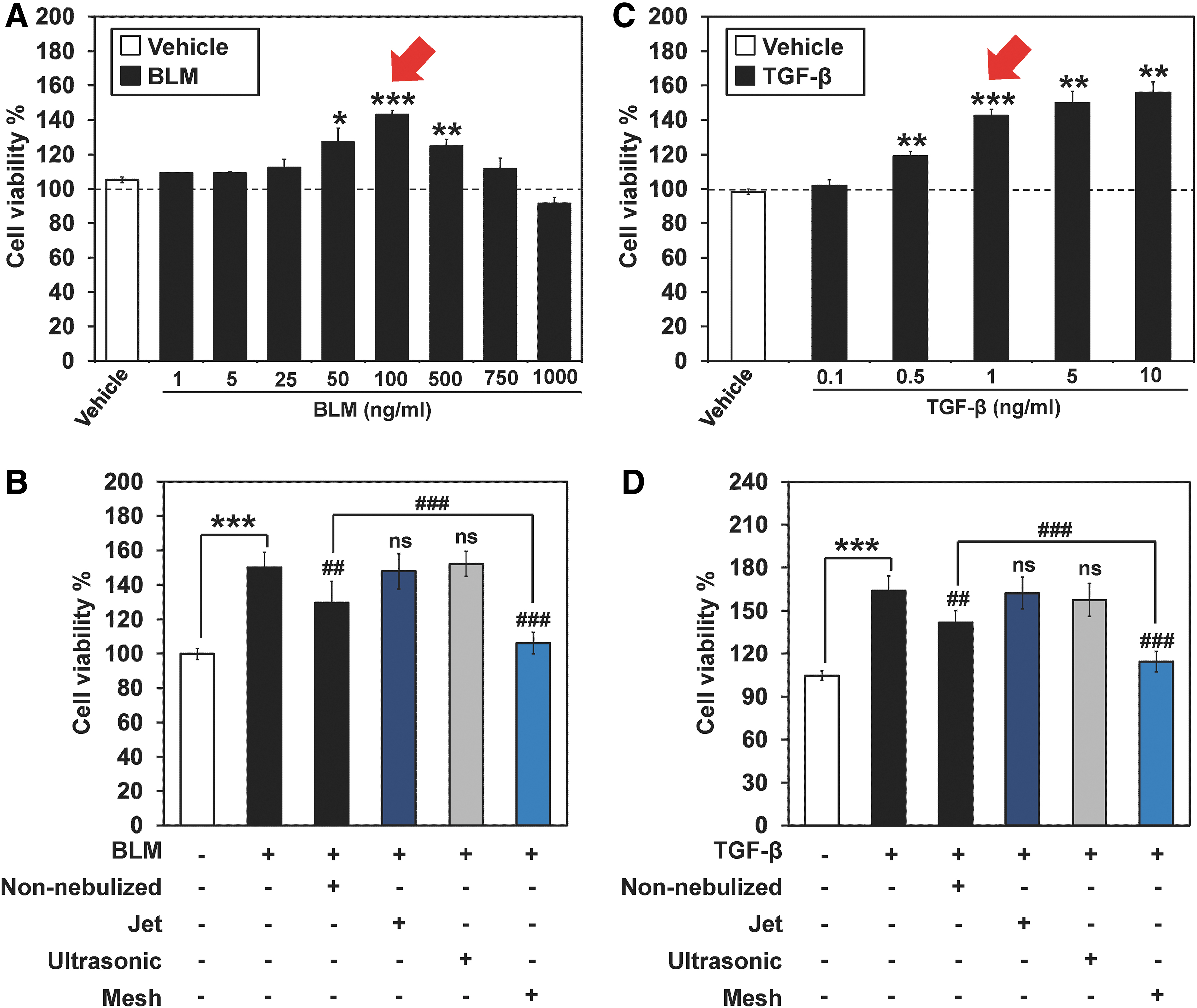
Effect of IFN-β on the viability of human lung fibroblast cells under BLM treatment or TGF-β stimulation.
Similarly, nebulization with the mesh nebulizer increased the therapeutic effects of IFN-β under TGF-β stimulation, whereas nebulization with either the jet nebulizer or the ultrasonic nebulizer reduced the effects of parenteral IFN-β on HLF cells.
Inhibition of human lung fibroblast migration and myofibroblast differentiation by IFN-β
To further study the effect of nebulized IFN-β on the migration ability of HLF cells, a Transwell migration assay was performed. It was found that IFN-β nebulized with the mesh nebulizer significantly inhibited the migration ability of TGF-β-treated HLF cells (Fig. 5A, B). Morphological changes in HLF cells were studied using an inverted optical microscope. Myofibroblast phenotypes, such as cell flattening and swelling of the cytoplasm, were observed in HLF cells treated with TGF-β (Fig. 5C). Typical thin and elongated adherent fibroblasts were observed after nebulized IFN-β treatment (Fig. 5C). α-Smooth muscle actin (α-SMA) has been used not only as a differentiation marker but also as a functional marker for myofibroblasts. 35 In addition, vimentin is considered a nonspecific fibroblast and myofibroblast marker. 36 The test results revealed that nebulized IFN-β reduced the expression of α-SMA and vimentin in HLF cells under TGF-β stimulation (Fig. 5D).
Effect of IFN-β on the migration and myofibroblast differentiation abilities of human lung fibroblast cells under TGF-β stimulation.
Western blot analysis
The acquired western blot image, in which the non-nebulized IFN-β is compared with the collected postnebulization samples from the three nebulizer technologies are compared, is presented in Figure 6. IFN-β is a globular protein with a predicted molecular weight of 22 kDa. No specific protein bands were observed on the SDS-PAGE gel for the jet nebulizer and the ultrasonic nebulizer tests, which could be attributed to conformational changes in IFN-β after nebulization. On the other hand, for the mesh nebulizer test, the 22 kDa band was found. In addition, a shift of protein band at 48 kDa was observed. This observation can be understood to indicate that a larger portion of IFN-β remained intact postnebulization, thus maintaining its functionality.

Assessment of IFN-β stability postnebulization with the jet, ultrasonic, and mesh nebulizer technologies.
Discussion
Aerosol characterization studies are widely used as a standard method to estimate aerosol lung deposition when using inhalation devices. Generation of aerosol droplets within the respirable range is the preferred target when particles are expected to reach the distal bronchi and peripheral lung. In this study, the tested mesh nebulizer was able to produce a higher percentage of droplets within the expected range with less variation in particle size, whereas the jet and ultrasonic nebulizers produced slightly larger particles with a wider particle size distribution. Moreover, the observed residual mass in the jet and ultrasonic devices was much larger than that in the mesh nebulizer, as expected from the information described in the literature. 22 The TOR calculated from the three nebulizers was similar; thus, when combined with the residual mass computations, it was confirmed that the higher nebulized mass was the main factor influencing the longer TT of the mesh nebulizer (∼6 minutes). In contrast, the jet and ultrasonic nebulizers only aerosolized approximately half of the loaded mass in half of the time required by the mesh device.
Biologic drugs, including IFN-β, have widely been documented to be more susceptible to heat than nonbiologics. Temperature testing revealed that among the three nebulizers, only the jet nebulizer showed a drop in temperature during the nebulization period, which could be attributed to the air delivered from the compressor to the reservoir cap to generate the aerosol, as the thermocouple was positioned close to the aerosol generation site. A temperature increase was recorded with both the ultrasonic and mesh nebulizers. On the one hand, the temperature of the ultrasonic nebulizer reservoir was recorded to exceed 35°C close to the end of the treatment. The higher temperature generated by the ultrasonic nebulizer may have contributed to its delivery of the lowest dose among the three devices. IFN-β is a globular protein with a predicted molecular weight of 22 kDa. In this study, the 22 kDa band was found after mesh nebulization. Interestingly, we observed a shift in the protein band to ∼48 kDa. This may be due to the dimerization of IFN-beta after mesh nebulization. Dimerization effects on IFN-γ have been reported. 37 Covalent dimerization of recombinant human IFN-γ was found during storage. 38
Other research groups have reported that covalently linked IFN-γ dimers can exhibit enhanced antiviral activity and receptor binding activity compared with parenteral IFN-γ. 39 To the best of our knowledge, dimerization of IFN-β has not been reported. Dimerization of IFN-β by mesh nebulizers may affect antibody responses, alter the host immune system and cause adverse effects in IPF patients. Animal model efficacy and safety testing of inhaled IFN-β is needed before its use in clinical studies in the future. A long-term follow-up study of the effects of nebulized IFN-β treatment on the immune response also needs to be conducted.
BLM, a chemotherapy drug useful in the treatment of Hodgkin lymphoma, non-Hodgkin lymphoma, squamous cell carcinoma, and testicular carcinoma, is known to cause pulmonary fibrosis in patients and in marine models.40–43 BLM has also been reported to increase lung fibroblast proliferation in in vitro cell-based models.31,44 The cell viability assay after treating HLF cells with parenteral and nebulized IFN-β showed that the collected samples from the jet and ultrasonic nebulizers had a significantly lower ability to suppress fibroblast viability, which could be the result of IFN-β degradation. The sample collected from the mesh nebulizer presented the highest viability suppression, consistent with the larger proportion of intact molecules after nebulization observed by western blot analysis. However, it was particularly notable that the non-nebulized IFN-β had a lesser effect on reducing the viability of HLF cells, considering that the formulation was not exposed to any procedure that could affect its stability. It is thought that the potentially higher amount of excipients or issues regarding the concentration of IFN-β samples postnebulization may have played a role in these findings.
During initial treatment of the HLF cell lines with BLM to induce fibroblast proliferation, similar patterns were observed after treatment with non-nebulized and nebulized IFN-β. ABLM concentration of 100 ng/mL was selected to treat HLF cells, as this concentration was shown to induce greater cell proliferation, whereas 1 ng/mL was chosen as the concentration of TGF-β to generate a second set of proliferated fibroblasts after confirming that this concentration induced the same level of cell viability as the selected concentration of BLM. In this section, it was also seen that the effect on the reduction in HLF cell viability was higher for IFN-β nebulized with the mesh nebulizer.
The limitation of this study was that only marketed IFN-β for injection could be used. For the development of an inhaled IFN-β formulation, it is also highly important to select suitable excipients to ensure safe and smooth delivery of the medication into the lungs while avoiding irritation throughout the airways. Furthermore, in the case of biologics, excipients can help control formulations' physical properties and, at the same time, protect the API from detrimental forces that may affect drug delivery efficiency, as in the case of the heat generation described in this study. In addition, HLF cells were cultured using the traditional two-dimensional (2D) method in this study. However, 2D cultures may have several limitations. For example, 2D cultures do not mimic the natural structure of the lungs, and it is difficult to model drug distribution in a 2D culture system. Therefore, animal model efficacy and safety testing of inhaled IFN-β is needed before its use in clinical studies in the future.
Conclusions
The development of new inhalation treatments for IPF is indispensable to offer alternatives to patients with this condition. The therapeutic effect of biologic drugs, especially when directly delivered to the lungs, could provide new opportunities to treat rare diseases once the pathological mechanism is well understood. In the case of IPF, IFN-β may be considered an approach to reduce the fibroblast proliferation characteristic of the disease. The in vitro tests in this study demonstrated the feasibility of delivering IFN-β through three nebulizer technologies. Aerosol characterization values and DD performance were assessed, and the findings indicated that the deposition of IFN-β delivered through mesh technology in the lungs might outperform that achieved through jet and ultrasonic technologies, based on the aerosol particle size distribution and stability. Moreover, the efficacy of the delivered IFN-β in reducing fibroblast proliferation was further confirmed, cementing the path for further investigation in the field. Obtaining a better understanding of the role of IFN-β in IPF is crucial to evaluate its therapeutic effect in patients in future stages.
Footnotes
Authors' Contributions
E.H.C.B. designed the study, analyzed the data, created the figures, and wrote the article. Y.M.H. supervised the research, analyzed the data, and revised the article. T.T.W. supervised the research and wrote the article. Z.Y.H., C.T.W., D.J.C., S.K.N., and Y.H.L. performed the experiments, analyzed the data, and created the figures. All authors read and approved the final article.
Author Disclosure Statement
The authors declare that they have no known conflicting financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This work was supported by the National Taiwan University College of Medicine (110M122), the Taiwan Ministry of Science and Technology, and HCmed Innovations Co. Ltd.
Reviewed by:
Foda Hussein
Rajiv Dhand