
Abstract
Background:
Inhalation of hypertonic saline (HS) is standard of care in patients with cystic fibrosis (CF). However, it is unclear if adding salbutamol has—besides bronchodilation—further benefits, for example, on the mucociliary clearance. We assessed this in vitro by measuring the ciliary beating frequency (CBF) and the mucociliary transport rate (MCT) in nasal epithelial cells (NECs) of healthy volunteers and patients with CF.
Aims:
To investigate the effect of HS, salbutamol, and its combination on (muco)ciliary activity of NECs in vitro, and to assess potential differences between healthy controls and patients with CF.
Methods:
NECs obtained from 10 healthy volunteers and 5 patients with CF were differentiated at the air–liquid interface and aerosolized with 0.9% isotonic saline ([IS] control), 6% HS, 0.06% salbutamol, or combined HS and salbutamol. CBF and MCT were monitored over 48–72 hours.
Results:
In NECs of healthy controls, the absolute CBF increase was comparable for all substances, but CBF dynamics were different: HS increased CBF slowly and its effect lasted for an extended period, salbutamol and IS increased CBF rapidly and the effect subsided similarly fast, and HS and salbutamol resulted in a rapid and long-lasting CBF increase. Results for CF cells were comparable, but less pronounced. Similar to CBF, MCT increased after the application of all the tested substances.
Conclusion:
CBF and MCT of NECs of healthy participants and CBF of patients with CF increased upon treatment with aerosolized IS, HS, salbutamol, or HS and salbutamol, showing a relevant effect for all tested substances. The difference in the CBF dynamics can be explained by the fact that the properties of the mucus are changed differently by different saline concentrations.
Introduction
Cystic fibrosis (CF) is a genetic disease with reduced airway clearance, resulting in longer contact of the mucosa with entrapped pathogens and thus leading to chronic airway inflammation and infection.1,2 The mucociliary clearance is reduced due to modifications of mucus' viscoelasticity because of a nonfunctional CF transmembrane conductance regulator (CFTR) protein. 2 The CFTR protein is an ion channel that, among other functions, transports chloride through the cell membrane and thus helps to maintain the homeostasis of the airway-surface-liquid (ASL) layer in the respiratory tract. 3 A dysfunctional CFTR causes lower epithelial chloride secretion and higher sodium adsorption, what results in dehydration of mucus.
Furthermore, this process can remove the water from the periciliary layer and result in the depletion of this layer, 4 which is usually followed by a collapse of the cilia.5–7 Both mucus dehydration and ciliary collapse result in an impaired mucociliary transport and hence inefficient cleaning of lungs from pathogens. The efficacy of the mucociliary clearance depends among other factors, such as the viscoelasticity of mucus and the thickness of the periciliary layer, on the ciliary beating frequency (CBF).
Standard of care in CF patients, especially concerning airway clearance, includes airway physiotherapy and inhalation with secretolytics (such as hypertonic saline [HS]) and/or bronchodilators (such as salbutamol). 8 The inhalation of HS has been shown to improve lung function in children with CF. 9 In vivo and in vitro studies delivered important information about the mechanisms of the effect of HS as it enhances the mucociliary clearance by creating an osmotic gradient and thus increasing the hydration of the ASL, further increasing CBF.10–13 However, there are also some in vitro studies suggesting that HS decreases CBF of healthy individuals in the first hour after application, 14 whereas other studies did not find any effect on CBF.
Bronchodilators, such as the short-acting β-adrenergic agonist salbutamol, are frequently used in CF and have been shown to improve lung function. Nevertheless, more studies are needed to provide evidence on their efficacy and mode of action, especially to clarify effects beyond the known bronchodilation, such as effects on the CBF or the mucociliary clearance.15–18 Recently, our group reported about a short-term improvement in lung function and perfusion assessed by functional lung magnetic resonance tomography (MRI) in patients with CF after salbutamol inhalation. 19
However, while bronchodilation is the most plausible effect for the short-term improvement of lung function, there may be additional effects on intensifying the mucociliary clearance mechanism. Several studies have shown that salbutamol increases CBF in vitro14,20 and in vivo.10,11,21,22 However, so far, there is no evidence that adding salbutamol to HS has a superior effect on the ciliary activity and/or mucociliary clearance compared to HS alone. In addition, the information on the effect duration is sparse and heterogeneous and while the effect of HS and salbutamol has been studied in cells of healthy individuals,14,23 their effects on cells of patients with CF or their combined effects have not been investigated yet.
With this study, we therefore aim to assess (1) the in vitro effect of combined HS and salbutamol on CBF compared to the use of both substances alone throughout 72 hours in differentiated nasal epithelial cells (NECs) and (2) differences in CBF between NECs of healthy persons and CF patients. We also assessed the effect in patients with primary ciliary dyskinesia (PCD); however, due to that data not providing significant additions to the findings of this study, we present them in the Supplementary Data.
Materials and Methods
Study population
We included healthy volunteers and patients with CF. The study was approved by the ethics committees of the University Children's Hospital Bern and canton Bern, Switzerland (Ref. No. 2018-02155). Written informed consent was obtained from every participant or her/his legal guardian.
Cell culture
NECs were obtained from participants by nasal brushings and cultured as described previously. 24 Briefly, cells were proliferated using PneumaCult-Expansion-Plus medium, seeded on 12-well Transwells® permeable supports (surface of 1.21 cm2, 12 mm diameter) and exposed to the air–liquid interface (ALI) using PneumaCult ALI medium. Experiments were performed after >4 weeks of ALI exposure.
Cell culture preparations for experiments
One day (roughly 24 hours) before the aerosolization of the substances, the medium was replaced and the NECs were washed apically with phosphate-buffered saline (PBS) containing Ca/Mg (500 μL for 15 minutes at 37°C) to remove accumulated mucus. Furthermore, to increase humidification and temperature stability during the experiments, every Transwell was placed in one of the central wells of a separate 12-well plate and the surrounding wells were filled with 1 mL PBS.
Substance preparation
HS was used as a 6% solution, as delivered by the manufacturer (Mucoclear 6%, #03352840; Pari GmbH, Starnberg, Germany). Salbutamol (250 μL, VENTOLIN Inhal Lös 0.5%, GlaxoSmithKline, Brentford, United Kingdom) was diluted in 0.9% NaCl (2 mL) resulting in 0.06% salbutamol solution. Isotonic saline ([IS] negative control; 0.9% NaCl, #29554 B. Braun Medical, Sempach, Switzerland) was used as obtained from the manufacturer. In addition, a combination of 25 μL 6% HS and 25 μL 0.06% salbutamol was used to investigate the effect of the combined treatment.
Substance aerosolization
The substances were aerosolized to NECs with a MicroSprayer® Aerosolizer (Model IA-1C; Penn–Century, Philadelphia, PA, USA) and a high-pressure syringe (FMJ-250; Penn–Century) (Fig. 1). The administration of precise drug volumes in 25 or 50 μL doses was possible due to a set of dosing spacers. The distance between the tip of the MicroSprayer and the NEC surface was 9 mm for every experiment (ensured by placing PARAFILM® 63 mm from the tip and by cutting off the end of a 10 mL advanced Combitip (#0030089570; Eppendorf, Schönenbuch, Switzerland). The tip of the MicroSprayer was then placed through the end of the Combitip (Fig. 1A), which could not move further than the PARAFILM®. Twenty-five microliters of 6% HS, 0.06% salbutamol, and IS was aerosolized onto the NECs apically (Fig. 1B, C). In addition, 50 μL of the HS-salbutamol combination and the corresponding control (50 μL IS) were used.
Aerosolization device.
Assessment of the mucociliary transport rate
For the measurement of the mucociliary transport rate (MCT), we sprayed 1–2 puffs of dry puff ball spores (from calvatia excipuliformis) with an average diameter of about 3.5 μm onto the apical surface of the cell cultures and waited 30 minutes (incubation at 37°C) until the baseline was recorded.
Imaging setup, CBF and MCT measurements
CBF of the NECs was determined by high-speed videomicroscopy. The ciliary activity and the mucociliary transport of NECs were recorded on an inverted transmitted light microscope (Olympus IX73) equipped with a heating plate and a digital CMOS high-speed camera (Grasshopper 3 GS3-U3-32S4M-C, USB 3.0; FLIR, Wilsonville, Oregon, USA). Finally, a 219 × 164 μm field of view, represented by 640 × 480 pixels, was imaged by using a 10 × phase objective and recorded at 300 frames (CBF) or 30 fps (MCT) per second for 2 seconds (CBF) or 10 seconds (MCT). For CBF, always the same three spots in the insert were analyzed, and for the mucociliary transport, always two areas with moving particles were recorded.
The recordings were analyzed using the Cilialyzer software, 25 which computes the area-averaged power spectral density of the entire field of view. CBF is finally determined as the weighted average frequency within the main peak of the area-averaged power spectral density (see Fig. 2 for an example of power spectra and Supplementary Videos S1 and S2 files for an example video). The MCT was analyzed using the particle tracking module of the Cilialyzer software. We tracked usually at least two particles per video. Mathematical details considering CBF computation and particle tracking have recently been reported. 25
Example of the analysis with the Cilialyzer software.
Experimental setup
For each donor we used one transwell per condition (25 and 50 μL IS, HS, salbutamol, and HS&salbutamol) and separate transwells for CBF and MCT measurements. Thus, we cultured 5 transwells for CF patients for the measurement of CBF only and 10 transwells for healthy volunteers for the assessment of CBF and MCT.
Recordings of the cilia for the CBF measurements were taken before (baseline) and 15 minutes, 30 minutes, 1 hour, 2 hours, 4 hours, 8 hours, 24 hours, 32 hours, 48 hours, and 72 hours after the aerosolization of cells with the substances. At each time point, recordings at the same three spots on the insert were taken. CBF of each time point corresponds to the mean of these three areas on the inserts. For the duration of the measurements, the heating plate of the microscope was set to 37°C, and in between every recording, the plates were placed back into a 37°C incubator (also for mucociliary transport recordings).
For the measurement of the MCT, baseline transport speed was measured 30 minutes after spraying the dry puff ball spores on to the cell cultures. After aerosolization of the substances, we repeated the recordings at the following time points: 30 minutes, 4 hours, 24 hours, and 48 hours. For each time point, we recorded two spots of the insert with moving particles. We used the data of five healthy volunteers for the analysis as for the other donors, there was at least one missing data point.
Statistical analysis
The following three main outcomes were defined: (1) CBF change over 72 hours, (2) differences in CBF between the different treatment options at specific time points, and (3) differences in CBF between healthy and CF NECs. Since the data did not pass the D'Agostino normality test, nonparametric tests were used. Differences in CBF and MCT were compared by using (1) Friedman and Dunn's multiple comparisons test (pairing corresponds to the NECs from one person) for comparison of one treatment over time and (2) Wilcoxon matched-pairs signed rank test for differences between IS versus HS and HS versus HS plus salbutamol at each time point. p values <0.05 were considered statistically significant. Analyses were performed using GraphPad Prism Version 8.0.11 and 9.0.2 (Graphpad Software, San Diego, CA, USA).
Results
Study population
In total 18 participants were recruited for the main part of this study: 10 healthy subjects and 8 patients with CF. Samples from 15 participants could be finally included in the study (demographic details see Table 1). We had to exclude the NECs of one healthy volunteer for the CBF analysis since one well was damaged during aerosolization and of three healthy volunteers for the mucociliary transport analysis, as we could not obtain speed values for all time points. Samples of three CF patients could not be included since the cells did not grow successfully.
Demographic Details of the Study Population
CF, cystic fibrosis; SD, standard deviation.
Differences in CBF in healthy individuals
No significant difference was found between baseline CBFs for all cultures used (mean of 6.42 Hz [standard deviation; SD 0.35, range 5.87–6.8]). All used treatment options led to a roughly twofold CBF increase (Table 2 and Fig. 3). Significant CBF changes compared to the baseline were found after 15 minutes for IS, 8 hours for HS, 30 minutes for salbutamol, and 60 minutes for HS and salbutamol. IS (25 and 50 μL) and salbutamol roughly doubled the baseline CBF after 15 minutes, after which a plateau was reached. Four hours after aerosolization, CBF increase started to wear off and after 24 hours, CBF had returned to near baseline. HS increased CBF slower and its effect lasted longer: CBF reached its plateau after 2 hours and its maximum after 8 hours, and was still higher than baseline after 72 hours.
Evolution of CBF (Hz) in differentiated NECs of healthy volunteers over 72 hours for different substances. Data are shown as mean, N = 6, one cell culture per condition for each donor. CBF, ciliary beating frequency; NECs, nasal epithelial cells.
Ciliary Beating Frequency Over Time and Upon Aerosolization with Different Substances in Nasal Epithelial Cells of Healthy Volunteers
Data are shown as mean in Hz. In bold are statistically significant differences with p values <0.05 compared to baseline measurements using Friedman and Dunn's multiple comparisons test.
HS, hypertonic saline; SD, standard deviation.
The combination of HS with salbutamol led to a quick and long-lasting increase in CBF: the plateau was reached 60 minutes after aerosolization and CBF was still higher than baseline after 72 hours. There were significant differences in CBFs at specific time points between the substances applied to NECs (Table 3). CBFs from IS-treated NECs (25 μL control) were significantly higher than HS after 15 minutes and, however, lower after 24, 32, and 48 hours. Significant higher CBFs were also found for HS and salbutamol compared to HS alone after 60 minutes and 4 hours.
Differences in Ciliary Beating Frequency Between (a) Isotonic and Hypertonic Saline and (b) Hypertonic Saline Alone and Its Combination with Salbutamol in Nasal Epithelial Cells of Healthy Volunteers
Data are shown as mean difference between two treatments. Second mentioned treatment was subtracted from the first mentioned treatment, resulting in positive values if the second mentioned treatment was lower and negative values if the second mentioned treatment was higher than the first one. In bold statistically significant differences with p values <0.05 calculated using the Wilcoxon matched pairs signed rank test. N = 6.
CI, confidence interval; HS, hypertonic saline.
Differences in CBF in CF lung disease
All used substances increased CBF over 72 hours (Table 4 and Fig. 4). The mean baseline CBF for all experiments with CF cells was 7.14 Hz (SD 0.87, range 6.26–8.18) with no significant difference at baseline. Significant changes in CBF compared to the baseline measurements were found after 15 minutes for IS, 2 hours for HS, 30 minutes for salbutamol, and 8 hours for HS plus salbutamol (Table 4).
Evolution of CBF (Hz) in re-differentiated NECs of patients with CF over 72 hours for different substances. Data are shown as mean, N = 5, one cell culture per condition for each donor. CBF, ciliary beating frequency; CF, cystic fibrosis; NEC, nasal epithelial cells.
Ciliary Beating Frequency in Nasal Epithelial Cells of Patients with Cystic Fibrosis Upon Aerosolization with Different Substances
Data are shown as mean in Hz. In bold statistically significant differences with p values <0.05 compared to baseline measurements calculated using the Friedman and Dunn's multiple comparisons test.
HS, hypertonic saline; SD, standard deviation.
All substances roughly nearly doubled baseline CBF after 15 minutes, after which a plateau was reached. CBF increase started to wear off 4 hours after aerosolization for 25 μL IS and salbutamol and 32 hours for 50 μL IS, and reached roughly baseline after 72 hours. CBF was still increased after 72 hours by HS alone and HS with salbutamol. There was no significant difference in CBFs at specific time points between the distinct substances applied to CF NECs (Table 5). However, HS showed higher CBFs than IS after 48 and 72 hours and HS combined with salbutamol showed higher CBFs than HS alone after 30 minutes, 60 minutes and 8 hours (p = 0.063 for all comparisons).
Differences of Ciliary Beating Frequency Between (a) Isotonic and Hypertonic Saline and (b) Hypertonic Saline Alone and Its Combination with Salbutamol in Nasal Epithelial Cells of Patients with Cystic Fibrosis
Data are shown as mean difference between two treatments. Second mentioned treatment was subtracted from the first mentioned treatment, resulting in positive values if the second mentioned treatment was lower and negative values if the second mentioned treatment was higher than the first one. In bold statistically significant differences with p values <0.05 calculated using the Wilcoxon matched pairs signed rank test. N = 5.
CI, confidence interval.
Increased MCT after aerosolization of all substances in cells of healthy individuals
The MCT was increased 4 hours after the aerosolization of all substances (Fig. 5), although the difference to baseline was not significant for all conditions. The speed was lower already 24 hours after substance application and almost back to baseline 48 hours later. There was no significant difference between substances.
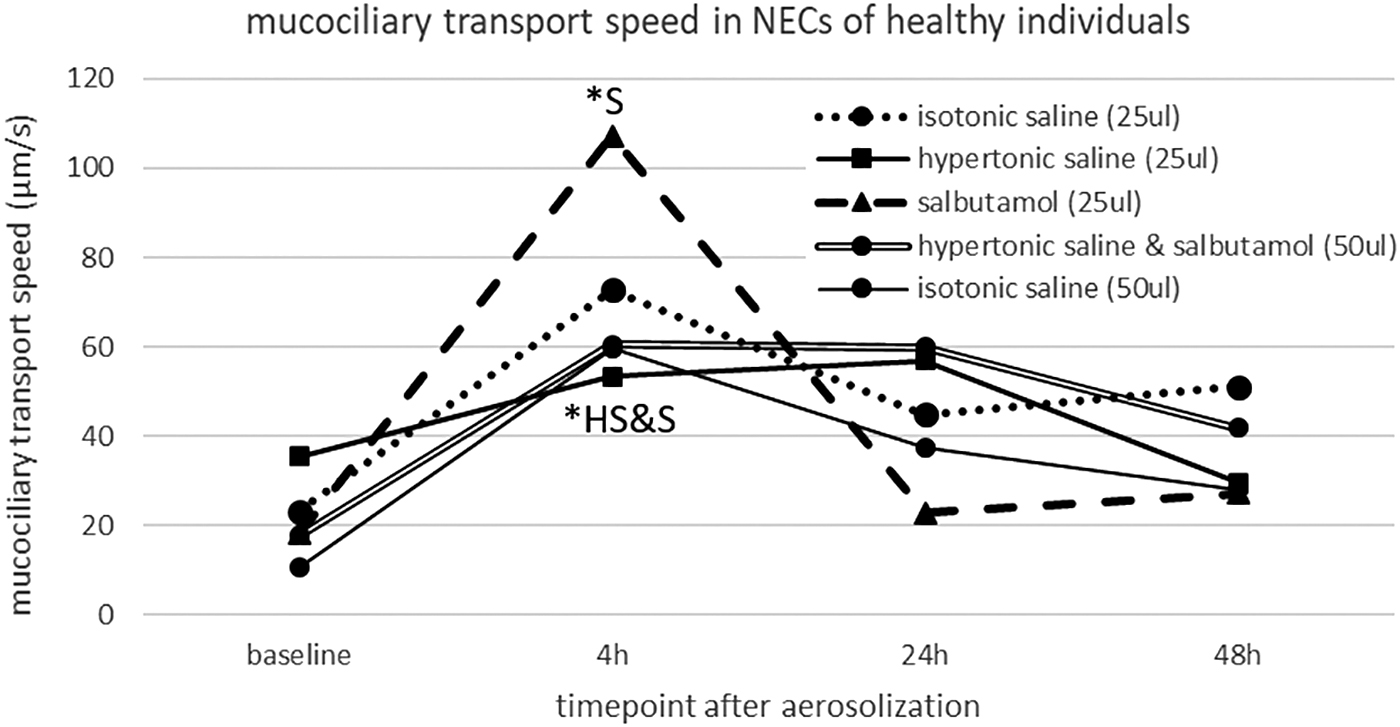
Increase of the mucociliary transport speed in differentiated NECs of healthy volunteers after aerosolization of different substances over 48 hours. Data are shown as mean, N = 5, one cell culture per condition for each donor. *Significant difference (p < 0.05) compared to baseline measurements calculated using the Friedman and Dunn's multiple comparisons tests. HS, hypertonic saline; NECs, nasal epithelial cells; S, salbutamol.
Saline concentration defines the dynamics of the CBF increase
To investigate the role of saline concentration on CBF increase, we aerosolized NECs of healthy volunteers with 0.9% (IS), 3.5% (1:1 mixture of IS and HS), and 6% (HS) saline. The overall dynamic was similar as observed for IS, HS, salbutamol, and HS and salbutamol (Fig. 6): a rapid increase of CBF to roughly the double of the baseline and a slow decline back to almost baseline after 72 hours. The increase of HS was slightly slower compared to IS or IS&HS, although not statistically significant. There was no significant difference during the decline between the different saline concentrations.
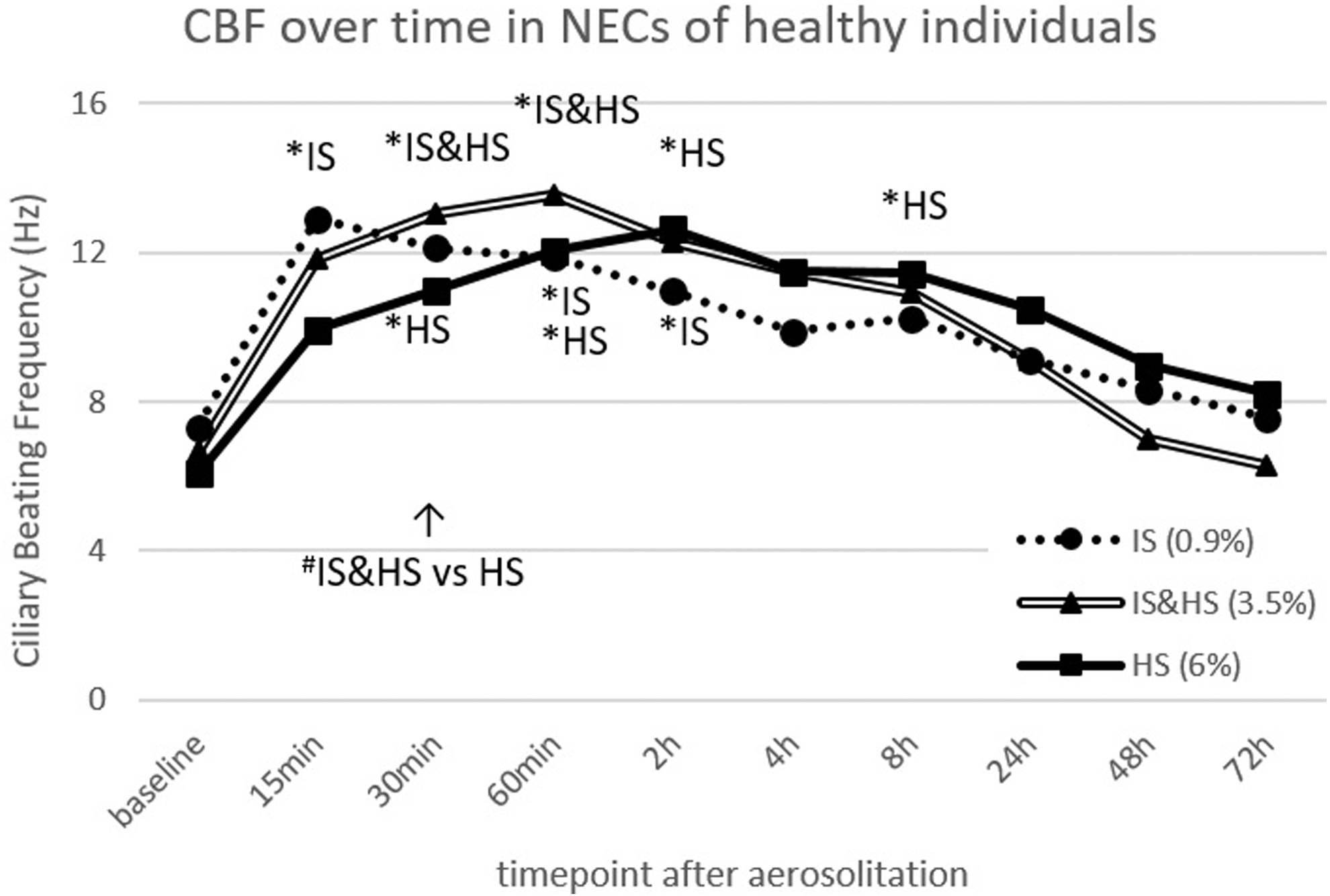
Evolution of CBF (Hz) in re-differentiated NECs of healthy volunteers after aerosolization of different concentrated saline solutions. Data are shown as mean, N = 5, one cell culture per condition for each donor. */#Significant difference (p < 0.05) compared to baseline (*) or between saline solutions at specific time points (#). CBF, ciliary beating frequency; HS, hypertonic saline; IS, isotonic saline; NECs, nasal epithelial cells.
Discussion
Our study assessed the effect of various commonly used inhaled substances on CBF in healthy and—for the first time also—in CF airway epithelial cells. Aerosolization of different concentrated saline solutions, salbutamol and the combination of both roughly doubled baseline CBF in NECs of healthy volunteers and patients with CF. While both IS and salbutamol had an immediate, but finite effect on CBF, HS had a delayed, but longer-lasting effect on CBF. The combination of HS and salbutamol lead to an immediate and long-lasting increase in the CBF. The effects were similar between healthy and CF NECs; however, for CF, differences between substances were less pronounced, CBF took longer to return to baseline, and the CBF increase by HS was faster. The MCT increased in a similar pattern to the CBF, following the application of all substances.
Comparison with literature
Our data are in line with parts of previously published studies, which also found an increased CBF in NECs of healthy individuals after the treatment with HS or salbutamol.23,26 However, data are incongruent, since other studies showed a decrease in CBF 5–10 minutes after HS application.14,27 These contradicting findings are mostly due to different experimental settings and/or volumes of test substances added to the cell cultures. The samples used for these studies were gained through surgical procedures and used directly without re-differentiation (cultivation for 4–6 days or used after thawing cryopreserved mucosa). Moreover, a study by Boek et al. 27 used submerged cells, with a submerged exposure corresponding less to the in vivo situation. In addition, secondary effects due to mechanical manipulation of cells before conducting the experiments cannot be fully excluded.
Another study by Boon et al. 14 used a sophisticated nebulization procedure using an aerosol chamber and a nebulizer head. Due to the very different approaches, it is not possible to directly compare our concentrations or volumes aerosolized with the ones in Boon et al.'s study. In our study, we used ALI cultures, which build a robust system with differentiated cells that are present in the conducting part of the human respiratory tract. In addition, due to the cultivation period of 5–6 weeks before starting the experiments, secondary effects could mostly be excluded. Our results on the mucociliary transport are in line with already published studies with CF patients showing that HS and IS increase mucociliary clearance.11,29,30
Mechanistic explanation attempt
We observed that the overall CBF changes were similar for all substances tested, including the control experiment with different saline concentrations: a rapid increase is followed by a slower decline. The same behavior was found for the MCT. We speculate that this behavior can mostly be explained by changes in the rheological properties of the mucus, including viscosity and elasticity; however, our study does not deliver the proof for this as this would have exceeded the scope of this project. Mucus is primarily composed of water and mucin proteins and its rheology is determined by mucus hydration and mucin secretion rates. 32
The initial CBF increase results from mucus dilution (hydration) due to apical substance aerosolization. This dilution process lowers the fluid drag encountered by the cilia, which in turn is thought to increase CBF. The deposition of large volumes of liquid on the apical sides of the cell culture increases the thickness of the ASL and the cells aim to restore the optimal ASL volume. To achieve this, the cells increase the sodium absorption by epithelial sodium channel (ENaC) clearance, 32 resulting in absorption of water into the cells and thus withdrawal of water from the ASL and mucus layer.33,34 Furthermore, the homeostatic mucus properties can be restored by increasing the mucin concentration through the release of more mucin granules that undergo a swelling process and (re-) thicken the mucus.32,33
These two mechanisms together might be responsible for the decline in CBF after the initial increase. Moreover, the first described mechanism may explain the differences we observed between the substances used in our studies as they had different saline concentrations. Substances with higher saline concentrations (e.g., HS) add more sodium ions to the mucus and thus the absorption of those ions by ENaC and the following water adsorption takes longer compared to substances with lower saline concentrations (as IS and salbutamol—according to literature are hypo-osmolar as stock solution and isotonic when mixed with 0.9% saline 35 ).
This might explain the longer duration of the CBF increase and thus later decline found for HS (6% saline concentrations) and HS and salbutamol or HS&IS (3.5% saline concentration) compared to IS or salbutamol (both 0.9% saline concentration) (see Figs. 3 and 4).
Besides the differences in CBF decline, we also observed differences in CBF increase: the increase was faster for substances with lower saline concentration (IS, salbutamol) compared to intermediate saline concentration (3.5%, HS and salbutamol in Fig. 3 and IS&HS in Fig. 4) or HS. These dynamic differences at the initial stage may be driven by the rate of mucus dilution (or mucus hydration) and the mixing process of the mucus with the aerosolized substance, which is most likely primarily determined by the rate of diffusion. We suppose that the initial diffusion-driven mucus dilution is faster for substances with lower salinities since the osmotic gradient between mucus and the substance is greater, resulting in faster mixing by diffusion.
To summarize, we see different overlaying cellular and physiological processes that determine the mucus properties and are likely responsible for the CBF changes observed in this study. Those processes probably cover potential effects of salbutamol found in previously published studies.10,11,14,20–22
Strengths and limitations
This study has several major strengths. The experiments were performed with primary cells of healthy individuals and patients with CF cultured and re-differentiated at the ALI, mimicking the in vivo situation very closely. ALI cell cultures represent the respiratory mucosa by ciliated epithelial cells as well as mucus-producing goblet cells displaying the intrinsic characteristics of healthy and patient cell cultures.
Furthermore, any kind of secondary influence, for example, through harvesting, infections, or environmental exposure, can be eliminated. The various substances tested were applied onto the cells by aerosolization in exact dosages to ensure even distribution mimicking inhalative drug application and therapy in the clinical setting. In addition, the experiments were performed over a time span of 48–72 hours to assess the long-term course on CBF and the mucociliary transport. With the assessment of the MCT, we studied the physiological relevant factor for the airway clearance.
Our studies revealed that the CBF and the transport speed showed the same behavior following the aerosolization of different substances. However, possible drawbacks of our study also have to be acknowledged. The in vitro study design does not entirely reflect in vivo conditions: (1) there is no clearance of the drug inside the transwells as in the nasal cavity and airways, presumably leading to a longer lasting effect in our experimental setting compared to in vivo. (2) Our cell cultures consist of different types of epithelial cells (mucus-producing goblet cells, and ciliated and basal cells), but do not include immune cells.
Furthermore, even though the here used NECs are thought to be a good proxy for the lung epithelium36–39 and NECs have been shown to have a similar CBF compared to bronchial epithelial cells, 37 our study does not provide the proof for an effect in the lower airways. (3) The volumetric dosage of applied substances in the used setup does not match the in vivo situation entirely. Due to technical limitations, we had to use a bigger volume as done for the inhalation. Furthermore, it is not possible to compare our drug dosage directly with in vivo inhalation as the actual drug concentrations on the airway surface after inhalation are not known. In addition, (4) the sample size for the CF patients is small due the low number of people affected by CF.
However, overall, we are convinced that the combination of our realistic cell culture model and the aerosolization method is ideal to investigate the effect of inhaled substances on the respiratory epithelium.
Clinical relevance of our findings
The substances and the experimental setup were chosen based on the current standard of therapy in our (and many other) clinical center(s) for patients with CF. Regularly used inhaled HS and salbutamol improve pulmonary symptoms.9,19 However, there is no consensus among clinicians whether the addition of salbutamol to HS is beneficial. Our findings show that the aerosolization of any kind of saline solution leads to a quick CBF increase in healthy and CF cells, independent of the addition of salbutamol.
Therefore, from a clinical point of view, we found no additional effect of salbutamol regarding CBF at single time points. Thus, a potential positive effect of salbutamol inhalation on clinical symptoms or lung function (as shown in Kieninger et al. 19 ) may not be related to changes in CBF. However, considering the combination of a quick increase and long-lasting effect of the combination of HS and salbutamol, the frequency of inhalations could be adapted from, for example, bi-daily to a single daily inhalation. This is a point that should be addressed in future clinical studies and something that should be kept in mind, as the clinical picture of CF patients will change and improve with the broad use of modulator therapies.
Conclusion
This study shows that aerosolized IS, HS, salbutamol, and the combination of HS and salbutamol increase CBF of NECs of healthy subjects and patients with CF in vitro and the MCT of NECs of healthy subjects. However, our results do not indicate a clear superior effect of the addition of salbutamol to HS on the level of CBF, even though the CBF effect lasted longest in the cells treated with the combination of HS and salbutamol. Given the in vitro study design and the small number of study participants, our data cannot be generalized and should be further investigated in larger in vitro and in clinical studies.
Footnotes
Acknowledgments
We would like to thank all participants of this study for donating their nasal cells and Andrea Stokes (University Children's Hospital Bern) for her valuable help with cell culturing. Study authors participate in the BEAT-PCD clinical research collaboration (CRC), supported by the European Respiratory Society. Our PCD-UNIBE diagnostic center participates at the European Reference Network (ERN) Lung PCD core as a supporting member.
Authors' Contributions
A.E. performed nasal brushings, cell culturing, experiments, data analysis, prepared the figures and tables, and wrote the main article. E.K. helped with study design, data interpretation, and article writing. S.D.G. performed and analyzed the control experiments with different saline concentrations. S.T.S. performed nasal brushings and cell culturing, and helped with the development of the study design and article writing. M.S. developed the software for CBF measurement, analyzed mucociliary transport videos, and helped with data interpretation and article writing. S.A.T. helped with the development of the software for CBF measurements, data interpretation, and article writing. M.F. helped with data interpretation and article writing. P.L. helped with developing the project idea and study design and with data interpretation. C.C. came up with the original project idea and helped with study design and data interpretation. L.M. designed the study, performed nasal brushings and cell culturing, and helped with data analysis and article writing. All authors reviewed and approved the final version of the article.
Author Disclosure Statement
E.K. reports personal fees from Sanofi-Aventis, outside the submitted work. P.L. reports personal fees from Gilead, Novartis, Polyphor, Roche, Santhera, Sanofi-Aventis, Schwabe, Vertex, Vifor, and Zambon, outside the submitted work. All other authors have no conflicts of interest to disclose.
Funding Information
This study was partially funded by the Gottfried and Julia Bangerter-Rhyner-Foundation.
Reviewed by:
Matthias Salathe
Tim Corcoran
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.