
Abstract
Background:
Inhalation and deposition of particles in human airways have attracted considerable attention due to importance of particulate pollutants, transmission of infectious diseases, and therapeutic delivery of drugs at targeted areas. We summarize current state-of-the art research in particle deposition on airway surface liquid (ASL) influenced by mucociliary clearance (MCC) by identifying areas that need further investigation.
Methodology:
We aim to review focus on governing and constitutive equations describing MCC geometry followed by description of mathematical modeling of ciliary forces, mucus rheology properties, and numerical approaches to solve modified time-dependent Navier–Stokes equations. We also review mathematical modeling of particle deposition in ASL influenced by MCC, particle transport in ASL in terms of Eulerian and Lagrangian approaches, and discuss the corresponding mass transport issues in this layer. Whenever required, numerical predictions are contrasted with the pertinent experimental data.
Results:
Results indicate that mean mucus and periciliary liquid velocities are strongly influenced by mucus rheological characteristics as well as ciliary abnormalities. However, most of the currently available literature on mucus fiber spacing, ciliary beat frequency, and particle surface chemistry is based on particle deposition on ASL by considering a fixed value of ASL velocity. The effects of real ASL flow regimes on particle deposition in this layer are limited. In addition, no other study is available on modeling nonhomogeneous and viscoelastic characteristics of mucus layer on ASL drug delivery.
Conclusion:
Simplification of assumptions on governing equations of drug delivery in ASL influenced by MCC leads to imposing some limitations on numerical results.
Introduction
Mucus
Mucus is a slippery hydrogel fluid substance produced by mucosal tissues of human body, including airways,1,2 gastrointestinal tract,3,4 genitourinary tract,5,6 and ocular membrane. 7 Airway surface fluid (ASL), which contains mucus, is a thin fluid layer that covers the conducting airways of the respiratory tract and is essential for tissue lubrication, homeostasis of the hydrated epithelial layer, and nutrition of the underlying epithelium. ASL is also a first-line defense against pathogens and foreign substances.8,9 Mucus is mainly composed of cross-linked and entangled mucin fibers and is secreted by goblet cells and submucosal glands.10–12 Its branched chains create a three-dimensional (3D), covalently linked mesh-like network (Fig. 1).13,14
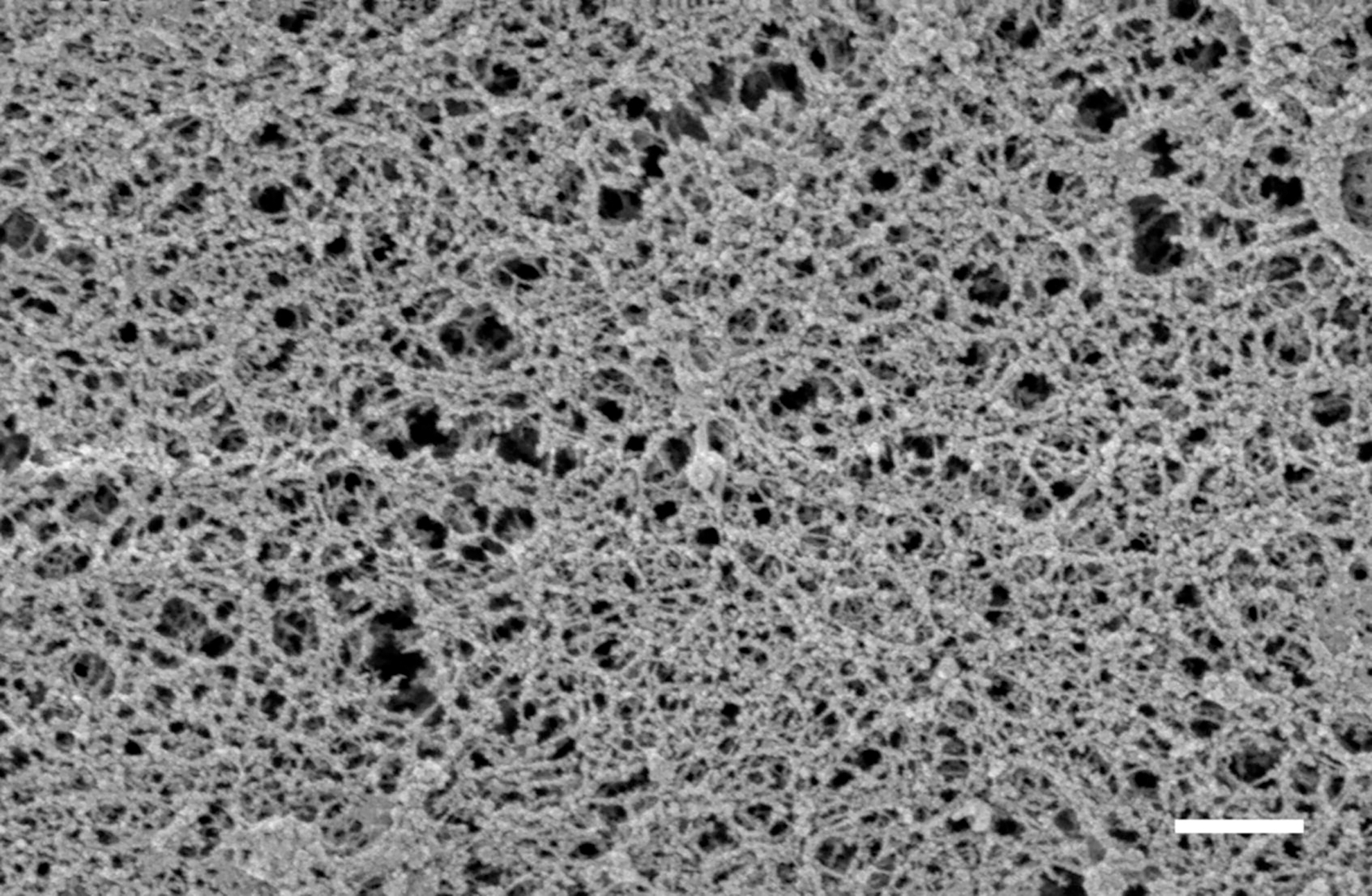
Respiratory mucus sample image using scanning electron microscopy shows that a mucus sample has a meshwork architecture (Scale bar shows 500 nm). Reproduced with permission from Schuster et al. 14
Mucosal layer is an important protective barrier against inhaling pathogens and other particles that enter this hydrogel matrix.
15
Mucus is mainly composed of water (∼95%), mucins (∼0.2%–5.0%), globular proteins (∼0.5%), salts (∼0.5%–1.0%), lipids (1%–2%), deoxyribonucleic acid (DNA
Pore size (mesh network size), viscoelasticity, pH, ionic strength, and charge are the main physicochemical key parameters influencing drug delivery across mucus barrier. 16 For instance, mucus viscoelasticity, which significantly affects the mucus filtering mechanism, creates a mesh network filter that reduces particle penetration and diffusion rates.17,18 Complex non-Newtonian and viscoelastic mucus behavior results from viscous (flow) and elastic (resistance to deformation) components. 9 Studies show that mucus behaves as a shear thinning fluid, and at low shear rates, viscosity of the mucus is 100–10,000 times higher than water. In contrast, at higher shear rates, mucus has a viscosity comparable to water. 19
In addition to its protective properties, mucosal surface shows promise in delivery of aerosolized medicines in diseases such as chronic obstructive pulmonary disease (COPD), asthma, cystic fibrosis (CF), and lung cancer,20–23 even though passage of nanoparticles of a drug through the barrier can be technically challenging because of its protective nature. There are studies on the effect of particle size and surface chemistry on mobility of nanoparticles in respiratory mucus in healthy state14,24–28 or diseases such as CF,29–31 chronic rhinosinusitis, 32 COPD, 33 and lung cancer. 34
Newby et al. showed that 100 nm and smaller drug-loaded nanoparticles, as well as pure drug powders or drug solutions, can easily diffuse through the mucosal layer by Brownian motion, and mucosal mesh does not have a great impact on the motion of these particles in mucus. However, there are challenges in mucosal drug delivery with larger drug-loaded nanoparticles that are comparable to, or larger than, mucus pore size (∼200 nm) where diffusion is not by simple Brownian motion and is typically slower. In this regard, advanced particle tracking of drug-loaded nanoparticles or computational modeling is necessary to estimate particle trajectories (Fig. 2). 35
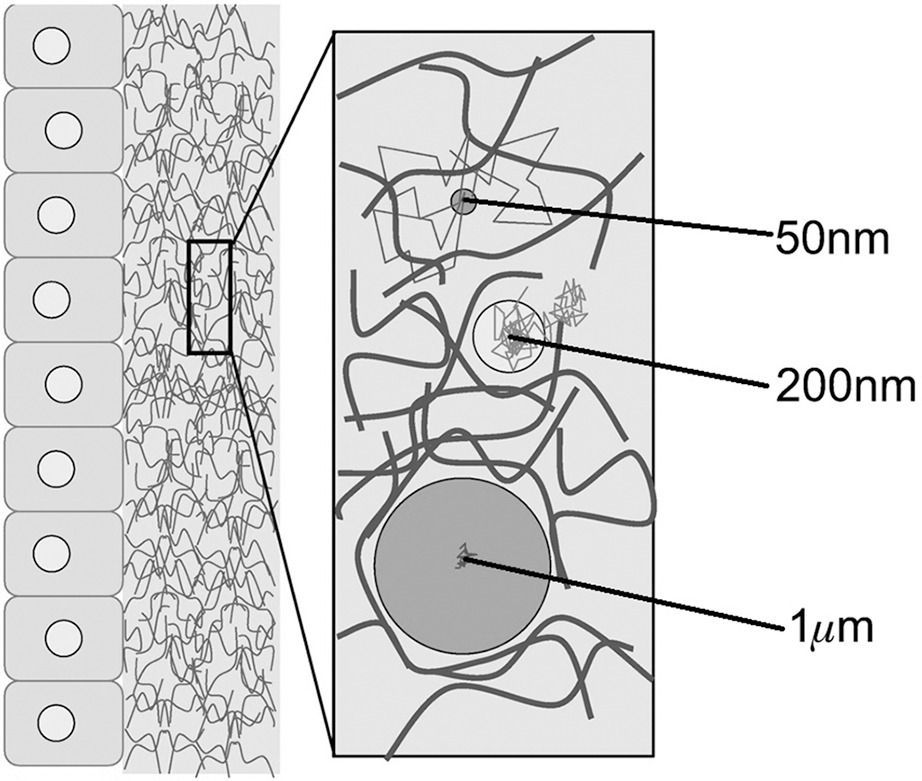
Schematic illustration of 3D mucus meshwork structure and effect of particle size on transport in mucus layer by Brownian and non-Brownian motion. Blocks on the left show epithelium and ciliated cells. Reproduced with permission from Newby et al. 35 3D, three dimensional.
ASL and mucociliary clearance
Tracheobronchial tree of lung consists of a conducting region formed by the trachea and tracheal bronchi and a gas exchange region formed by respiratory bronchioles, alveolar ducts, and finally, alveoli, where gas exchange between the atmosphere and capillaries occurs. Trachea and bronchi are covered by ASL, which is produced by a variety of cells, including ∼50% by ciliated cells, 12% by secretory cells (mostly goblet), 20%–30% by basal cells, and some by undifferentiated cells.36,37 As the airways continue to branch out into bronchioles and decrease in diameter, there is a decrease in the density of mucus-producing and basal goblet cells, while goblet cells, which produce aqueous secretions, are more common in small airways; however, the density of ciliated cells remains almost constant in various generations of bronchioles.
38
Due to shear thinning behavior of ASL, this multiphase fluid is reported to have two main sublayers:
(a) Aqueous periciliary liquid (PCL) layer: it has a depth of about 5–10 μm in upper airways of bronchi, trachea, and nasal cavity,
39
and provides an environment for beating of a carpet of motile microstructures called cilia as well as cell surface lubrication.
40
This layer has a watery characteristic due to ciliary forces and a high shear rate in this region. (b) Sticky, high-viscosity, gel-like and viscoelastic mucus layer
41
: it captures foreign particles such as dust, fungi, bacteria, and other environmental particles. This layer has a depth of 5–15 μm in nasal cavity,42,43 10–30 μm in trachea, and 2–5 μm in bronchi.18,44,45 Mucus has a high viscosity and relaxation time at low shear rates,
46
which leads to movement above PCL resembling solid state.
About 2 × 1012 of motile cilia,47,48 each with a length of 5–7 μm, 49 beat in a coordinated wave-like motion within PCL, and propel inhaled foreign particles trapped in mucosal layer toward the trachea and eventually outside of respiratory tract. This process is known as mucociliary clearance (MCC). 50
Figure 3 shows a schematic diagram of ASL showing ciliary motion, mucus, and PCL layer, as well as the fate of soluble and insoluble particles after deposition in ASL, which rely heavily on characteristics of noncellular pulmonary barrier; this barrier is composed mostly of an ASL blanket in upper and central segments or bronchi, or a pulmonary surfactant layer in distal branches and alveoli, the latter is devoid of mucus in a healthy subject. 51 The peripheral lung has a large surface area (100 m2) and very thin epithelial layer (0.2–0.7 μm), resulting in excellent sink conditions and a desirable environment for gas exchange and high blood perfusion.52,53

Schematic illustration of ASL and MCC and fate of an aerosol after deposition in ASL blanket in upper and central segments or bronchi (left panel) or pulmonary surfactant layer in distal branches and alveoli (right panel). (1) First contact of deposited particles with ASL. (2) Penetration of soluble or ultrafine nanoparticles into pulmonary epithelium and blood. (3) Clearance of large and undissolved particle. Reproduced with permission from Ruge et al. 51 ASL, airway surface liquid; MCC, mucociliary clearance.
Mathematical modeling indicates that efficiency of the MCC is affected by many parameters such as ciliary abnormalities, which can be related to ciliary beat frequency,54–61 ciliary density,55,59,60,62,63 ciliary length,58,59,61,64,65 ciliary beat pattern,55,59,65,66 ciliary beat orientation,67–69 missing ciliary regions,55,59 phase difference between cilia,55,61 cilia lattice geometry,55,61 and metachronal waves produced by cilia. 70 MCC can also be affected by ASL and airway characteristics such as mucus rheology,46,71–77 mucus and PCL viscosity,56,64,74,78 depth of PCL and mucosal layers,56–58,60,61,64,79 mucus production rate, 79 stiffness transition between PCL and mucosal layers,56,65,78 high expiratory airflow rates above mucus,80–87 mucosal dehydration,88–90 or even airway pressure gradient. 91 Other physiological factors (e.g., sex, posture, age, sleep, exercise etc.) can also influence MCC by changing properties of mucus, PCL, and even cilia, individually or in combination. 92 The available voluminous literature on biological fluid characteristics in scores of mucus is reviewed thoroughly by Spagnolie. 93
Mathematical modeling of inhaled particle deposition on ASL influenced by MCC is critical to evaluate proper drug delivery on ASL to treat common respiratory diseases. Numerical modeling has been regarded as a key tool to achieve this goal. Our review mainly focuses on recent advances in numerical simulation of effect of various parameters on MCC in health and disease followed by mathematical modeling of particle deposition on ASL, which are influenced by MCC.
Numerical Modeling of MCC
Numerical simulation of MCC has been studied extensively 94 and various aspects of pulmonary ASL modeling were reported by Levy et al. 95 However, due to the unsteady nature of this problem, small grid and time spacing, a partially large value of ciliary consecutive beat cycle, as well as high computational cost of simulation of ciliary forces and mucus as a viscoelastic fluid, almost all previous studies simulated geometry of MCC in bronchi, which have minimal ASL thickness. From a numerical point of view, there are three major challenges in modeling such complicated geometry: (1) interaction mechanism between cilia and ASL, (2) considering mucus viscoelasticity by employing a proper constitutive equation and, (3) employing an accurate numerical method to solve governing and constitutive equations. Each component will be reviewed in detail.
Ciliary modeling
Mucus clearance is facilitated by unidirectional transport of mucus over an underlying bed of beating cilia. By studying ciliary beat cycle in rabbit trachea,
96
Fulford and Blake
50
represented position of each cilium (

where s measures length of arc from base of cilium, σ is the angular beat frequency, and an and bn are the Fourier coefficients, which were previously reported by Fulford and Blake.
50
They also represented location of an array of cilia by
50
where a and b are the spacing of cilia in the x and z directions, respectively, and
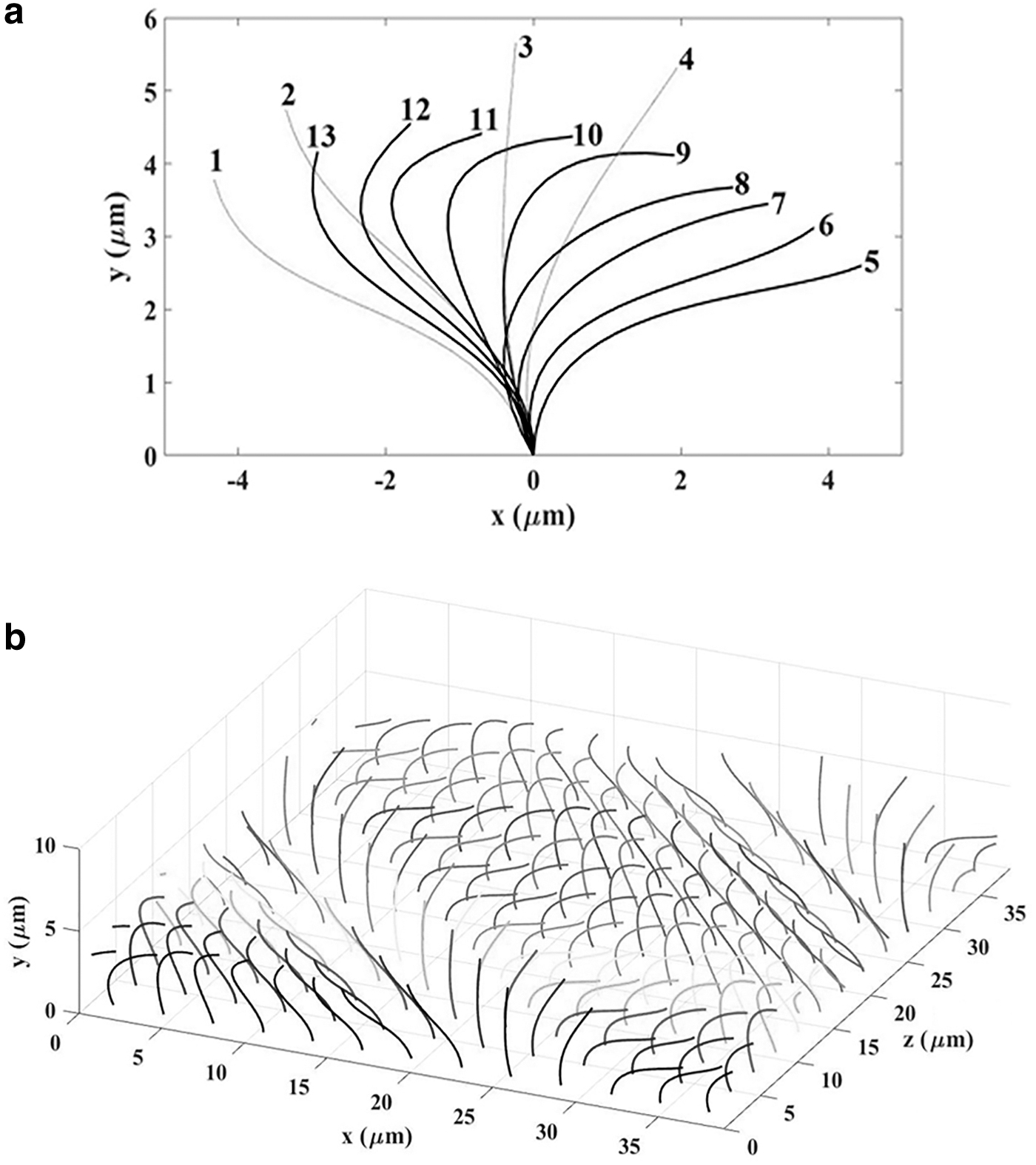
In effective stroke phase (states 1–4 in Fig. 4a), cilia impose the maximum force during the forward motion, which leads to forward flow of ASL. On the other hand, in the recovery stroke phase (states 5–13 in Fig. 4a), cilia slowly move backward by bending down to the epithelial surface, which minimizes their retarding impact on the ASL flow. 98 The work performed during the effective stroke is magnitudes higher than amount of work done during the recovery stroke. 98
Due to the complex nature of ciliary motion, as well as the significant effect of ciliary forces on MCC, modeling of ciliary motion and forces has been challenging in the study of this complicated geometry. Barton and Raynor were seemingly the first to model ciliary forces in MCC problem. 99 They assumed cilium as a rigid rod that is long in effective stroke and becomes short in recovery stroke. They used simplified resistance/drag coefficients to evaluate the effect of ciliary tips on fluid to obtain mucus velocity profile. 99 Although they calculated realistic mucus flow rates, erroneous depiction of ciliary motion, ignoring effect of PCL and epithelial surface on velocity profile, and coordination wave on an array of cilia are the most important shortcomings of this study. 100
Blake introduced an “active porous medium” model to study ciliary propulsive force by considering cilia as a porous media in the fluid and reported a simplified formulation for velocity profile. 101 Other mathematical approaches to study ciliary forces include slender body theory, 102 traction layer model,74,103,104 continuous envelope moving boundary model, 105 and hybrid grid-particle method. 106 A detailed review of modeling techniques of cilia-ASL interactions, including continuum ciliary modeling and discrete ciliary modeling with its relative merits and demerits, has been recently reviewed thoroughly by Vanaki et al. 94
Immersed boundary method (IBM) has been regarded as one of the most efficient methods to model stationary and moving bodies in fluid. Peskin appears to be the first to propose IBM and to solve blood flow around heart valves by using this method.
107
In this technique, fluid is represented on the Eulerian domain and moving or stationary boundary immersed in the fluid is represented on Lagrangian points. Force on the immersed object [
where
where
Due to efficacy and simplicity of implementation of IBM as well as its robustness when dealing with moving and flexible boundaries, especially in the case of infinitely thin structures, this method has been regarded as a popular technique to couple interaction between cilia and fluid. Thereby, many recent numerical studies have used this method to simulate ciliary forces.54–61,65,75,110–115 Because of high computational cost of ciliary modeling, most previous investigations used one-way interaction of cilia on ASL and the effect of ASL flow on ciliary beat pattern was not taken into calculations. However, Loiseau et al. suggested a 2D model that predicts a phase diagram of mucus transport, which influences ciliary beating direction. 69 Their results showed that cilia/mucus hydrodynamic interactions control collective dynamics of ciliary beat directions.
Modeling of mucus viscoelasticity
Mucus is perceived as a viscoelastic and nonhomogenous fluid. 116 Although viscoelastic properties of mucus play a vital role in its flow,46,74,75,110 due to numerical challenges, many earlier investigators considered mucus as a Newtonian,60,61,65,111,115 or non-Newtonian (shear-thinning)64,78,106,117 fluid. There are limited studies on viscoelastic behavior of mucus. Smith et al. are seemingly the first to report a numerical study of viscoelastic behavior of mucus by considering it as a linear Maxwell viscoelastic fluid. 74
Linear viscoelastic models could be useful to simulate viscoelastic fluids in small deformations (<2%–3%) 118 and their results are not usually correct for large deformations and fluid flow, and these models are widely used in solid mechanics and polymer engineering for problems in which the size of deformation is very small. 119 Due to not satisfying the principle of frame invariance, equations of linear viscoelasticity are not valid for large deformations. To remedy this issue, a set of frame-invariant coordinates are presented to define time derivatives in frames that deform with the material elements. 119 Thereby, some recent studies by using this coordinate simulated mucus as quasilinear viscoelastic models, such as upper-convected Maxwell 87 or Oldroyd-B model,54,56,75,110,114 to study the effect of mucus viscoelasticity.
Although these semilinear models such as the Oldroyd-B model can capture the fundamental viscoelastic property of mucus at large deformation, several drawbacks such as assumption of constant viscosity and first normal stress differences coefficient, as well as inability to model second normal stress differences of fluid in shear
119
remain challenging in simulating this fluid. Besides, mucus typically has nonlinear rheology properties at greater strains.
46
Therefore, the nonlinear characteristics and behaviors of these biological systems as a function of shear rate are important factors in numerical simulation.
120
To study the effect of nonlinear behavior of mucus, Vasquez et al. reported a comprehensive equation of mucus.
46
They used a five-mode nonlinear Giesekus model in approximating the experimentally verified relaxation spectrum of mucus. In this model, the elastic contribution of stress tensor (

Each mode of the Giesekus model can be calculated as follows 121 :

where,

In addition, in Equation (6),  is upper convected derivative defined as follows:
is upper convected derivative defined as follows:

Nonlinear mobility term in the Giesekus model [Eq. (6)] is a key parameter to capture the shear-thinning behavior of mucus, as well as second normal stress difference, 119 while these behaviors are ignored in some semilinear models such as Oldroyd-B model. Due to ability of the Giesekus model to capture shear thinning viscosity and first and second normal stress difference in shear, 121 this model can be a desirable model to simulate mucus viscoelasticity. Table 1 presents values of parameters based on the five-mode Giesekus model of mucus in healthy state. 46 Our group recently used this model to replicate 2D 58 and 3D55,57 simulation of MCC geometry.
Numerical simulation of governing equations
Recent investigations have elucidated that PCL contains a fine matrix network that prevents mucus from penetrating it.
40
Thereby, in most previous numerical investigations, ASL is modeled as two-phase immiscible fluids with different properties.
74
For this purpose, a proper boundary condition should be applied at the interface of the PCL and mucus layers. The modified Navier–Stokes equations, including immersed boundary force term (to simulate ciliary and PCL-mucus membrane forces) as well as elastic stress tensor (to estimate viscoelastic behavior of the mucus), have been presented as governing equations of this geometry as follows
60
:
where
where
In Equations (12a) and (12b),  is a unit tangential vector to PCL-mucus membrane interface. Arc lengths s and s0 are measured along current and initial configuration of membrane interface, respectively. Scalar T0 describes stiffness constant, which shows elastic characteristics of flexible boundary. A few studies in 2D numerical simulations considered effect of surface tension at PCL-mucus interface by computing boundary membrane force explained in Equation (11).56,60,65,75 However, previous experimental and numerical investigations have shown that interface force between mucus and PCL does not have a significant effect on mucus and PCL velocities56,60,74,96,122; therefore, most numerical studies ignored the effect of membrane interface between PCL and mucus layers by assuming a flat interface between these two layers and imposing a continuous fluid velocity and stress across interface in their numerical modeling.
is a unit tangential vector to PCL-mucus membrane interface. Arc lengths s and s0 are measured along current and initial configuration of membrane interface, respectively. Scalar T0 describes stiffness constant, which shows elastic characteristics of flexible boundary. A few studies in 2D numerical simulations considered effect of surface tension at PCL-mucus interface by computing boundary membrane force explained in Equation (11).56,60,65,75 However, previous experimental and numerical investigations have shown that interface force between mucus and PCL does not have a significant effect on mucus and PCL velocities56,60,74,96,122; therefore, most numerical studies ignored the effect of membrane interface between PCL and mucus layers by assuming a flat interface between these two layers and imposing a continuous fluid velocity and stress across interface in their numerical modeling.
In most previous studies, a symmetric segment of ASL (Fig. 4b) with following boundary conditions has been investigated:
ASL flow is considered periodic in x and z directions. 74
Bottom boundary is assumed to be a no-slip wall. 60
Top boundary is perceived to be a slip wall. 123
This two-phase model has the advantage of simulating mucus and PCL layers as a unique domain with different properties simultaneously. It can also estimate penetration of cilia into moving mucus layer reported in previous investigations.50,96,124–127
Table 2 represents a summary of 2D and 3D numerical investigations of MCC along with a detailed numerical method, ciliary modeling method, and mucus rheology model. As this table indicates, due to the complex nature of this geometry, bulk of literature is limited to 2D flow regimen. However, 2D MCC overestimates mean mucus velocity since fluid is not allowed to flow around cilia. 57
Summary of Studies Available on the Two-Dimensional and Three-Dimensional Numerical Simulations of Mucociliary Clearance
The numerical method include FDM, FEM, FVM, and LBM.
FDM, finite difference method; FEM, finite element method; FVM, finite volume method; IBM, immersed boundary method; LBM, lattice Boltzmann method.
Due to the unsteady nature of this problem, a partially large value of ciliary consecutive beat cycle (about 0.1 seconds in healthy state), small grid, time spacing of geometry, and high computational cost of numerical methods to simulate ciliary forces and mucus viscoelasticity, the 3D simulation of this complex geometry, even in Newtonian mucosal fluid, has not been extensively researched. Jayathilake et al., in 3D numerical simulation, studied the effect of various parameters on PCL flow. 61 They used IBM to simulate ciliary forces and finite difference projection method to simulate PCL as a Newtonian fluid.
Their results showed that maximum PCL velocity happens if cilia have phase differences in both stream-wise and span-wise directions. They also showed that PCL velocity is linearly dependent on ciliary beat frequency, while average PCL velocity decreases with increasing PCL height. Furthermore, shortened cilia significantly reduce PCL velocity, while changing PCL viscosity does not substantially affect PCL velocity.
Vanaki et al. did a study with the same approach by studying some ciliary abnormalities found in various chronic respiratory diseases, for example, ciliary beat frequency, ciliary length, ciliary beat pattern, ciliary density, and missing ciliary region on the PCL transport. 59 Their results showed that PCL surface velocity and flow rate are significantly affected by changes in ciliary beat frequency and ciliary length observed in COPD patients. They also showed that stiff planar and wiper ciliary beat patterns in primary ciliary dyskinesia patients significantly reduce PCL surface velocity and flow rate.
Furthermore, these ciliary abnormalities decrease PCL velocity and flow rate compared to a healthy state. Although these two studies59,61 have been considered two of the most comprehensive 3D numerical simulations of PCL geometry, they did not consider mucus layer as an integral part of this geometry in their mathematical modeling. Our group has recently studied 3D simulation of MCC geometry by considering PCL as a Newtonian and mucus as a nonlinear Giesekus viscoelastic fluid. 57
In our study, the projection finite difference method was used to solve governing and constitutive equations of fluid flow. In addition, to simulate ciliary forces more accurately, IBM was employed. Ciliary configuration at t = 0 seconds as well as computational domain of this study are shown in Figure 5. As this figure indicates, cilia have cyclic motion according to truncated Fourier series, as reported by Fulford and Blake 50 [Eq. (2) and Fig. 4a]. Values for standard parameter set (parameters used in a healthy state) of mucus rheology properties and ASL characteristics employed in this 3D simulation are represented in Tables 1 and 3, respectively. Some numerical simplifications have been used in this modeling, which include the following:

Schematic geometry of 3D MCC in study of Sedaghat et al. 57 Reproduced with permission.
PCL, periciliary liquid.
Air-mucus and PCL-mucus interfaces are considered to be flat. 74 Furthermore, this force is neglected due to minimal membrane force between PCL and mucus layers.56,60,74,96,122
The cilia move in evenly spaced filament-like structures with a constant beat frequency.59,61,112
One-way interaction of cilia on ASL is considered, which means propulsive impact of cilia on ASL is taken into consideration; however, cilia are made to move in a predefined beat pattern and influence of ASL flow on cilia was ignored. 69
Due to limited height of PCL and mucus layer, the effect of ASL gravity force would be negligible compared to the ciliary forces. 128
No mass transfer is present at the bottom epithelial cell wall.
Three-dimensional simulation in a healthy state predicts mean mucus and PCL velocities of 44.33 and 20.49 μm/s, respectively, which agree with experimentally determined clearance rates.129,130 In contrast, our 2D simulation 58 with the same approach and rheology properties for mucus showed ∼2.5-fold larger clearance rates with respect to 3D models. This is mainly due to neglecting ciliary spacing in the z-direction in 2D simulation, which overestimates mucus and PCL velocities since fluid is not allowed to flow around cilia in the z-direction. 3D numerical results 57 also showed that for PCL layer, even though flow direction mainly changes along the z direction, PCL has a 3D flow structure because of localized ciliary forces.
On the other hand, in the mucus layer, effects of ciliary motions have been mainly dampened and velocity change in z direction is much less than that in PCL due to significantly higher mucus viscosity and elasticity. Our 3D results 57 showed that mean mucus and PCL velocities enhance linearly with ciliary beating frequency. However, the effect of this parameter on mucus velocity is more than PCL velocity. Furthermore, with increasing ciliary length, from 5 to 6.5 μm, mean mucus velocity almost doubled. In contrast, PCL velocity was much less affected, resulting from cilia penetration into the mucus layer. Numerical results also indicated that changes in PCL depth and mucus depth have little effect on mucus and PCL velocities.
In another 3D numerical investigation with the same approach, our group has recently studied the effect of cilia abnormalities such as phase difference between cilia, cilia beat pattern, cilia beat frequency, cilia lattice geometry, missing cilia regions, and cilia density on MCC. 55 Results indicated that some cilia abnormalities, such as cilia density, cilia beat pattern, and cilia beat frequency, have a dominant effect on MCC and 3D structure of the fluid, and some abnormalities, such as missing cilia regions and phase differences between cilia, have a moderate influence on that.
Numerical Simulation of Particle Deposition on ASL
Simulation of particle transport and deposition in various parts of human airways have been extensively studied and bulk of the literature has been reviewed recently.131,132 However, there needs to be more numerical activity on the fate of particles deposited on ASL by considering the effect of MCC. The protective nature of mucus against foreign particles and efficient inhaled drug delivery makes it challenging to tackle this issue from a computational standpoint.
Experiments showed that proteins and viruses <100 nm in diameter, such as h-lysozyme (3.5 nm), horse myoglobin (3.8 nm), chicken lysozyme (4.1 nm), porcine pepsin (4.5 nm), h IgM Fab (6 nm), horse ferritin (12 nm), and viruses, including polio (28 nm), Norwalk (38 nm), hepatitis B (43 nm), human papillomavirus (55 nm), adenoviruses (60–90 nm), and rotavirus (75 nm), could easily penetrate mucus.11,12 Influenza virus (100 nm) can also penetrate mucus unless strongly immobilized by adhesive interactions with mucosal components. 14
The concentration distribution of soluble particles or trajectories of insoluble particles in ASL are affected by ASL velocity profile, as well as various forces. Gravity, drag, lift, and Brownian forces are regarded as important forces that influence particle motion. There are two main methods for studying particle deposition in airways: Eulerian and Lagrangian approaches. Eulerian method, which is based on solving classical mass diffusion equation, is appropriate for the simulation of soluble or very small nanoparticles where the Brownian effect of particle is dominant. 133 On the other hand, Lagrangian method, which is based on solving particle equation of motion, is more efficient for simulation of insoluble larger particles where particle inertia effect is more important. 134 In the following sections, numerical studies dealing with simulation of particle transport on ASL influenced by MCC using these two approaches will be reviewed.
Eulerian modeling
Nanoparticle transport based on Eulerian modeling is the most used model to simulate solutes or ultrafine particles; the motion and deposition are dominated by their Brownian forces. In this condition, Lagrangian trajectory analysis becomes inefficient since the particle relaxation times are very small and a large number of particles need to be traced for precise estimation of local particle deposition. 135 In addition, simplicity, low computational cost, and rapid evaluation of particle deposition rates are some other characteristics of Eulerian simulation compared to Lagrangian modeling.
To simulate particle deposition on ASL based on Eulerian method, by assuming dissolution of particles in mucus and using velocity distribution of the ASL, classical mass diffusion equation at ASL needs to be solved and the concentration of inhaled particles at various parts of ASL versus time is obtained. Equation of mass diffusion of an inhaled particle can be presented as follows:
where c is ASL particle concentration (mass of particle/volume of ASL) and
Olmsted et al. reported diffusion coefficient of various proteins and viruses with different sizes in human cervical mucus.
143
Yang et al. also calculated diffusion coefficient of the swine influenza virus in porcine mucus.
144
Although diffusion characteristics are affected by particles' size and shape, globular or chain-like solutes can adopt themselves in a 3D configuration in fluid medium.
145
Desai et al. reported effective diffusion coefficients of various solutes through aqueous and porcine mucus layers.
146
One of the preferred mathematical models of diffusion coefficients of solute in mucus layer was reported as the Obstruction-Scaling model
138
:
In Equation (14a),
In the Eulerian approach, mass conservation boundary condition at the interface separating layers should be imposed to obtain the concentration of particles in the multilayer domain. For example, between PCL and mucus layer, this boundary condition is given by the following equation:
The same equation can simulate mass conservation between air-mucus 149 or PCL-epithelium149,150 layers.
There have been a few studies dealing with simulation of particle deposition in ASL solved by Eulerian method. In some of these studies, an attempt has been made to simulate particle transport in both airway and ASL; however, due to numerical complexities arising from this geometry, there are some simplifications in the simulation of ASL flow. Corley et al. studied inhaled acrolein concentration in various parts of rat, monkey, and human respiratory tract by considering steady-state inhalation. 151 Their results showed that regional acrolein uptake was influenced by airway geometry, airflow rates, inhaled acrolein concentrations, ASL diffusion coefficient, ASL thickness, and maximum rate of metabolism.
In another study, they extended their previous findings by considering transient breathing patterns for predicting kinetics of three reactive constituents of cigarette smoke: acrolein, acetaldehyde, and formaldehyde. 152 Yoo and Ito used an integrated model of actual shape of human body geometry with a virtual airway of a realistic human respiratory tract to simulate time-dependent inhaled formaldehyde concentration, including adsorption distributions, that is, heterogeneous tissue dosimetry in respiratory tract (Fig. 6). 149 As this figure indicates, they used Eulerian approach to study formaldehyde adsorption/deposition flux or equilibrium concentration in a three-layer model of airway, mucus, and subepithelium. Their results showed that over 50% of inhaled formaldehyde was adsorbed by ASL at nasal cavity.
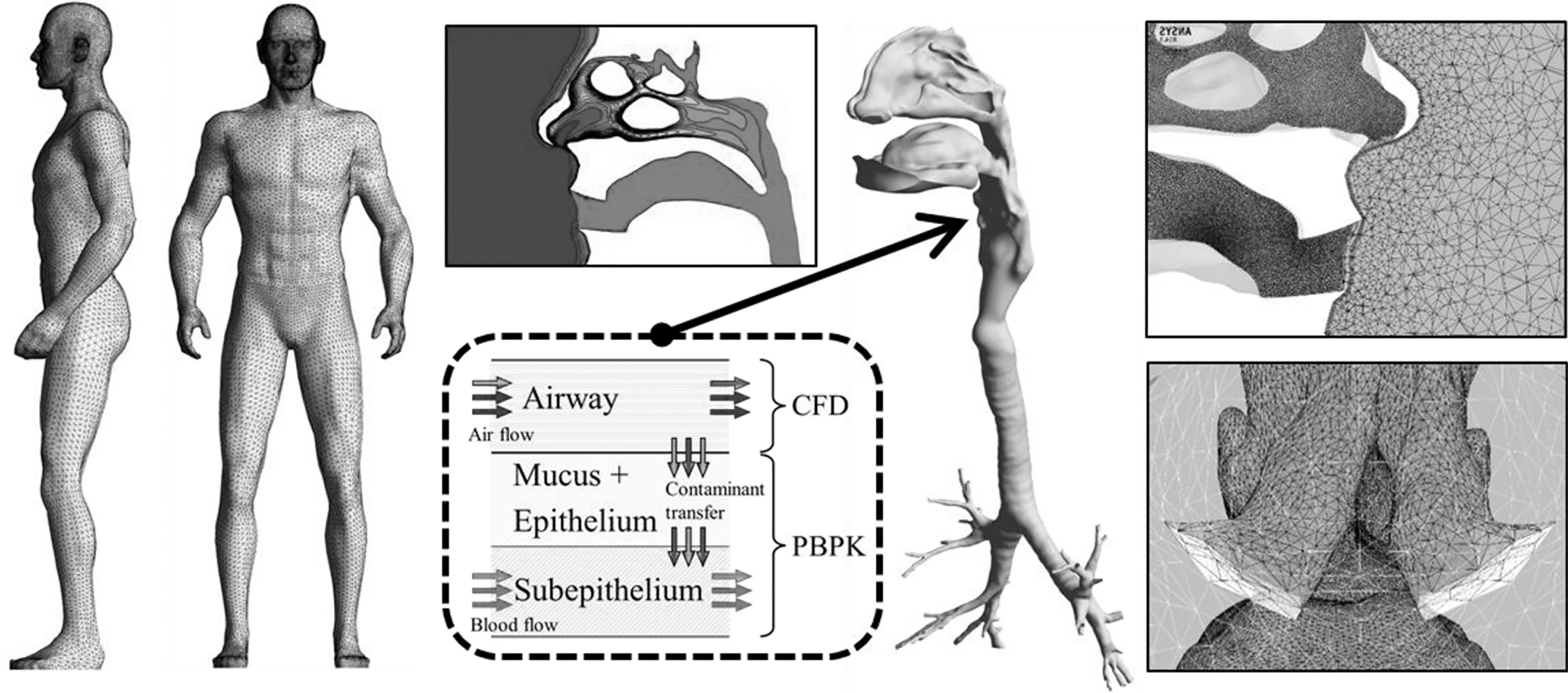
A schematic geometry of numerical model in study of Yoo and Ito, 149 which was done by PBPK-computational fluid dynamics (CFD) hybrid model. Reproduced with permission. CFD, computational fluid dynamics; PBPK, physiologically based pharmacokinetic.
Rygg and Longest 153 and Rygg et al.154,155 studied dissolution, absorption, and clearance of drug aerosols in nasal mucus. In their studies, a flat 2D surface of inner nasal wall is considered to study particle deposition in a 10-micron mucus layer. The study also investigated dissolution of three different drugs on nasal mucus layer, as well as penetration of particles into epithelial surface over time. Shang et al. extended these works by considering mucus as a 3D surface-shell model. 156 Considering ASL as a single fluid with an average viscosity, as well as ignoring drug adsorption by epithelium are important limitations of this study. In addition, in studies by Rygg and Longest, 153 Rygg et al.,154,155 and Shang et al., 156 a uniform mass flow rate is defined to impose a fixed axial velocity in the ASL layer.
Recently Chari et al. simulated a realistic 3D nasal cavity airway model of nose of a healthy nonsmoker person. 150 They employed a cutting-edge 3D meshing technology that enables smooth capture of mucus layer at a micrometer scale and comparatively large air-flow domain (Fig. 7). To obtain a more precise velocity profile of ASL results from beating of cilia, a wall-driven velocity assumption at interface between mucus and PCL layer was employed. They studied influence of partition coefficient, particle size, drug solubility, as well as particle distribution on mucus and its uptake in epithelium. They showed that drugs with a higher partition coefficient or solubility can be taken up easier in the epithelium. At the same dose, smaller particles with their relatively large surface areas dissolve faster and are absorbed easier in ASL compared to larger ones.

A schematic geometry of nasal geometry and mucosal layer in study of Chari et al. 150 Mucosal layer (black) separates airflow of nasal surface (dark gray) from epithelial layer (light gray). Reproduced with permission.
Ariane et al. used a discrete multiphysics method to simulate diffusive and convective drug delivery in PCL. 148 In this study, ASL and cilia were simulated by smoothed particle hydrodynamics (SPH) and mass-spring models, respectively, in a 2D simulation. They studied effects of ciliary flexibility, ciliary beat frequency, and drug diffusion on PCL drug delivery. Results showed that at a low-frequency regime, cilia hinder drug delivery. In contrast, diffusion is dominant drug delivery mechanism at an intermediate-frequency regime. Cilia play a vital role in mass transfer in ASL at a high-frequency regime due to convection mechanism.
It should be noted that in some of these studies, for simplicity, particles were assumed to dissolve immediately into mucus after depositing on upper surface of ASL layer.149,157 However, some investigations studied particle size reduction owing to dissolution and later absorption in mucus layer148,150,153–155 according to Noyes–Whitney mass diffusion equation:
where m is mass of the drug, A is surface area of the particle, Dm is diffusion coefficient of the dissolved drug in the mucus layer, Cs is solubility of the drug, Cb is concentration of the dissolved drug in bulk phase, and h is diffusion layer thickness.
The above numerical studies to study particle dissolution in ASL assume either constant mucus velocity or some simple assumption for ciliary forces. Accurate simulation of governing equation in ASL, to obtain more precise velocity distribution in PCL and mucus layers, which leads to calculation of convective term in diffusion equation, is scarce in literature.
Lagrangian modeling
In this method, individual particles are tracked within ASL flow field. The primary advantage of this approach is that the effect of effective forces such as gravity, drag, inertia, and Brownian forces are directly considered in the motion of the particle. In addition, accurate velocity and location of particles, as well as percentage of particles that deposit on ciliary or epithelial walls can also be estimated by this method.
Second law of Newton governs dynamics of particle motion and for each particle, it can be represented as follows
134
:
where
Drag force can be calculated as follows
158
:
where dp is particle diameter,
Particle mass diffusivity in ASL can be obtained as follows
159
:
where K is the Boltzmann constant and T is fluid temperature. Based on the above equation, drag force for a small spherical particle in ASL can be calculated as follows:
Diffusion coefficient of a particle in the ASL (
Shear lift force can be calculated from a generalized expression of Saffman lift force, shown as follows
160
:
where
Brownian force per unit mass of particles can also be calculated as follows
162
:
In Equation (22a),
There have been a few studies dealing with simulation of nanoparticle deposition in ASL by Lagrangian trajectory analysis approach. Kirch et al. simulated deposition of deposited particles in ASL and clearance of these particles in a 2D domain.163,164 Mucus flow velocity was calculated by solving 2D steady-state equations of motion of fluid in Eulerian domain analytically.
By solving time-dependent Lagrangian equation of motion of nanoparticles, velocity components and location of each particle in ASL were estimated. Their results showed that ASL velocity distribution plays a vital role in the fate of nanoparticles in ASL, while sedimentation, diffusion, and impaction seem to have little effect on particle transport. Also, intrinsic plasticity of mucus slabs and collision of such slabs increase particle translocation toward epithelium. Two-dimensional simulation, ignoring the effect of Brownian forces of nanoparticles, and using an inaccurate model to simulate ciliary forces and ASL velocity distribution are main shortcomings of these studies.163,164
Ernst et al., by considering mucus as a porous structure of Newtonian fluid-filled random-sized cells, calculated subdiffusion of particles in mucus layer (human sputum taken from CF patients), by measuring mean squared displacements of the particles. 165 They considered the effect of Brownian diffusion of particles in permeable membrane domain. The foundation of this strategy is modeling of particle trajectories in the presence of Robin boundaries. 166 They showed that only particles with a diameter of <40 nm can pass through a mucosal layer by passive Brownian motion. This finding contradicts results of previous studies that imply 100 nm and smaller particles can easily diffuse through mucosal layer through Brownian motion regardless of mucus mesh spacing. 35
Bajd and Serša 167 modified the method presented by Ernst et al. 165 and used bond-fluctuation model to simulate motion of different-size and chain-like particles through mucus as a porous media with three different 2D restrictive-scaffold geometries (isotropic, anisotropic, and random). Their results showed that steric interactions play a vital role in the motion of chain particles in confining mucus fluid. The main shortcoming of the above two studies is not taking into effect the ASL velocity on particles' motion and velocity.165,167
Vanaki et al. simulated deposition of nanoparticles in 3D ciliary arrays interacting with PCL. 168 They used IBM to estimate ciliary forces and location versus time and also projection method for solving a 3D Navier–Stokes equation in ASL and a particle tracking method to simulate transport of inhaled particles deposited onto the PCL in healthy and diseased lungs. Although this study was the first that solved complete 3D Navier–Stokes equations in ASL to address velocity and location of particles more accurately, it had two main drawbacks. First, it did not consider mucus layer in simulation, while mucus has been perceived as one of the most important protective barriers against inhaling particles. Second, it used small nanoparticles in simulations and effect of particle Brownian motion was not studied, while Brownian force is dominant force in this situation.
An essential step in simulating more accurate circumstances for both healthy and diseased states is developing a 3D model that can depict interaction of MCC and mucus-deposited inhaled particles. While micron-sized particles seem to be cleared by the mucus effectively, specific nano-sized particles have been shown to penetrate ASL into and beyond PCL. 25 These particles have both therapeutic (retention of hazardous particles in lungs for an extended period of time) and toxicological consequences (leveraging of mucus-penetrating nanoparticles for drug delivery to bronchial epithelium), which can only be simulated with a 3D cilia configuration and ASL model. However, 3D simulation studies of mucus and PCL layers by considering effect of ciliary motion and simulation of particle motion by considering impact of effective forces [explained in Eq. (17)–(22)] are indeed scarce.
Conclusion and Outlook
Numerical simulation of MCC as well as particle deposition in human airways have been studied extensively. Current state-of-the-art is only limited to study particle deposition in human airway combined with ASL, which is influenced by MCC. Findings shed further light into drug deposition as well as penetration of harmful particles into human respiratory system.
Studies reveal that three key parameters have influenced numerical simulation of MCC, including ciliary forces, mucus rheology properties, and numerical method, to solve time-dependent modified Navier–Stokes equations. The effect of various parameters on both mucosal and PCL velocities has been reported in previous numerical investigations by overcoming these three issues. In this regard, IBM , one of the most effective cilia modeling techniques many researchers use, is extensively reviewed. The five-mode nonlinear Giesekus model in approximating experimentally verified relaxation spectrum (reported by Vasquez et al. 46 ) has been explained as one of complete constitutive equations of mucus used in some recent numerical studies.
Protective nature of mucus against large particles as well as efficient inhaled drug delivery have been controversial research issues. A small percentage of current literature addresses particle deposition in human airways influenced by MCC. Two main approaches have been used to study particle transport in ASL: Eulerian and Lagrangian. Eulerian approach, which is based on solving classical mass diffusion equation, is appropriate for the simulation of dissolved nanoparticles (<100 nm) in mucosal layer. It has some advantages compared to Lagrangian method, which includes simplicity, low computational cost, and rapid evaluation of particle deposition rates.
Most studies have used Eulerian method to simulate particle deposition on ASL. Lagrangian method is based on solving particle equation of motion by considering effect of inertia, drag, lift, gravity, and Brownian forces imposed on each particle. This method is more efficient for simulation of larger particles where the effect of particle inertia is more significant. Tracing exact velocity and location of each particle as well as exact location of deposited particles (i.e., cilia, epithelium wall, etc.) are advantages of this method. However, there have been few studies dealing with particle deposition on ASL using this method.
Reliable results based on Eulerian and Lagrangian approaches for studying distribution of dissolved drug powders or drug solutions in ASL are available up to using fixed value of ASL velocity. The effect of real ASL flow regime on drug distribution in this layer is still not well studied. Nonhomogeneous and viscoelastic behavior of mucus layer as well as consideration of mucus shear-thinning viscosity may also influence particle deposition rate. Considering an accurate velocity, distribution of ASL can lead to a significant effect on particle distribution in this layer. Most of this literature is based on numerical simplifications of governing differential equations in this area and 3D numerical results are scarce.
Footnotes
Authors' Contributions
M.H.S.: conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing original draft, and writing review and editing. M.B.: project administration, writing review and editing, and investigation. O.A.: data curation, investigation, methodology, project administration, supervision, and writing review and editing. All three authors approved the final version.
Author Confirmation Statement
First author (M.H.S.) is from Technical and Vocational University (Tehran, Iran) and the third author (O.A.) is from Shiraz University (Shiraz, Iran); both institutions are primarily involved in education or research.
Author Disclosure Statement
The authors declare they have no conflicting financial interest.
Funding Information
No funding was received for this article.
Reviewed by:
Georg Dietze
Tim Corcoran