
Abstract
Background:
The lung dose of nebulized drugs for spontaneous breathing is influenced by breathing patterns and nebulizer performance. This study aimed to develop a system for measuring breath patterns and a formula for estimating inhaled drugs, and then to validate the hypothesized prediction formula.
Methods:
An in vitro model was first used to determine correlations among the delivered dose, breath patterns, and doses deposited on the accessories and reservoirs testing with a breathing simulator to generate 12 adult breathing patterns (n = 5). A pressure sensor was developed to measure breathing parameters and used along with a prediction formula that accounted for the initial charge dose, respiratory pattern, and dose on the accessory and reservoir of a nebulizer. Three brands of nebulizers were tested by placing salbutamol (5.0 mg/2.5 mL) in the drug holding chamber. Ten healthy individuals participated in the ex vivo study to validate the prediction formula. The agreement between the predicted and inhaled doses was analyzed using the Bland–Altman plot.
Results:
The in vitro model showed that the inspiratory time to total respiratory cycle time (Ti/Ttotal; %) was significantly directly correlated with the delivered dose among the respiratory factors, followed by inspiratory flow, respiratory rate, and tidal volume. The ex vivo model showed that Ti/Ttotal was significantly directly correlated with the delivered dose among the respiratory factors, in addition to the nebulization time and accessory dose. The Bland–Altman plots for the ex vivo model showed similar results between the two methods. Large differences in inhaled dose measured at the mouth were observed among the subjects, ranging from 12.68% to 21.68%; however, the difference between the predicted dose and inhaled dose was lower, at 3.98%–5.02%.
Conclusions:
The inhaled drug dose could be predicted with the hypothesized estimation formula, which was validated by the agreement between the inhaled and predicted doses of breathing patterns of healthy individuals.
Introduction
Nebulizers deliver high doses of prefilled solutions or prescribed drug and work for a wide range of medications such as bronchodilators, vasodilators, antibiotics, and newly developed drugs.1,2 The two common choices of nebulizers are pneumatic jet nebulizers and vibrating mesh nebulizers. Compared with a jet nebulizer, a vibrating mesh nebulizer operates silently, is smaller in size, and has a lower residual dose with high delivery efficiency, all of which have contributed to its popularity for the past two decades.2,3
The delivery of nebulized drugs to patients with spontaneous breathing is affected by numerous factors, such as breathing pattern, pulmonary disease status, and nebulizer performance, which includes residual dose (the amount of drug remaining in the nebulizer), accessory design, and nebulizer design.4–7 Breathing patterns, which refer to the combination of tidal volume, respiratory rate, inspiratory time, and inspiratory flow, have been identified as the primary factors that alter the delivered dose.7–10
Bennett et al. evaluated the impact of breathing pattern on inhaled drug dose, and found that the inspiratory to expiratory (I:E) ratio was the primary influencing factor rather than the inspiratory volume or respiratory rate. 11 Whereas the EN International Organization for Standardization (ISO) 27427:2013 requires a test with a breathing simulator to generate a respiratory rate of 15 breaths/min, a tidal volume of 500 mL, and I:E ratio of 1:1, referring to 50% of inspiratory time to total respiratory cycle time (Ti/Ttotal; %). Byron et al. compared the nebulizer delivery dose for four different breathing patterns with Ti/Ttotal ranging from 50% to 25%.12,13 Bosco et al. compared inhaled drug doses using prerecorded simulated breathing patterns in 20 adult subjects. 14 Studies have shown that designing a reservoir in a nebulizer system increases the inhaled drug dose.5,15
Previous studies have illustrated the relationship between inhaled dose and respiratory parameters, and researchers have attempted to predict aerosol deposition for the past two decades.16–18 Nazir et al. used an artificial neural network to successfully predict the pattern of aerosol deposition using monodisperse and polydisperse particles.16,17 However, the inhaled drug dose is difficult to predict due to differences in breathing patterns, nebulizers, and accessory design. Our previous study showed a wide range of drug depositions in terms of the delivered drug dose, residual dose, and drug on accessories between a jet nebulizer and mesh nebulizer with two- and fivefold difference in the residual dose.6,19
The development of an inhaled drug prediction method is desirable for personalized and accurate drug dose estimations. The prediction must account for influencing factors such as breathing pattern, residual dose, deposited dose in the accessories, and nebulizer performance (including particle size and nebulizer output). Therefore, this study aimed to develop a system for measuring breath patterns and a formula for estimating inhaled drugs, and then to validate the hypothesized prediction formula.
Materials and Methods
In vitro study
An in vitro model was first used to determine correlations among the delivered dose, breath patterns, and doses deposited on the accessories and reservoirs. A breathing simulator (ASL5000; Ingmar Medical, Inc., Pittsburg, PA) with fixed compliance of 50 mL/cmH2O and a resistance of 6.0 cmH2O/(L·s) was used to generate tidal volumes of 700 and 500 mL, respiratory rates of 15 and 30 breaths/min, and the Ti/Ttotal of 50%, 33%, and 25% for a total of 12 breath patterns, as shown in Table 1. The breathing simulator was connected to the sensing module and a drug-collecting filter (Vadi Medical Technology Corp., Taoyuan, Taiwan) by a silicon adaptor and a mouthpiece. Figure 1A shows the configuration of the apparatus used in this in vitro study.
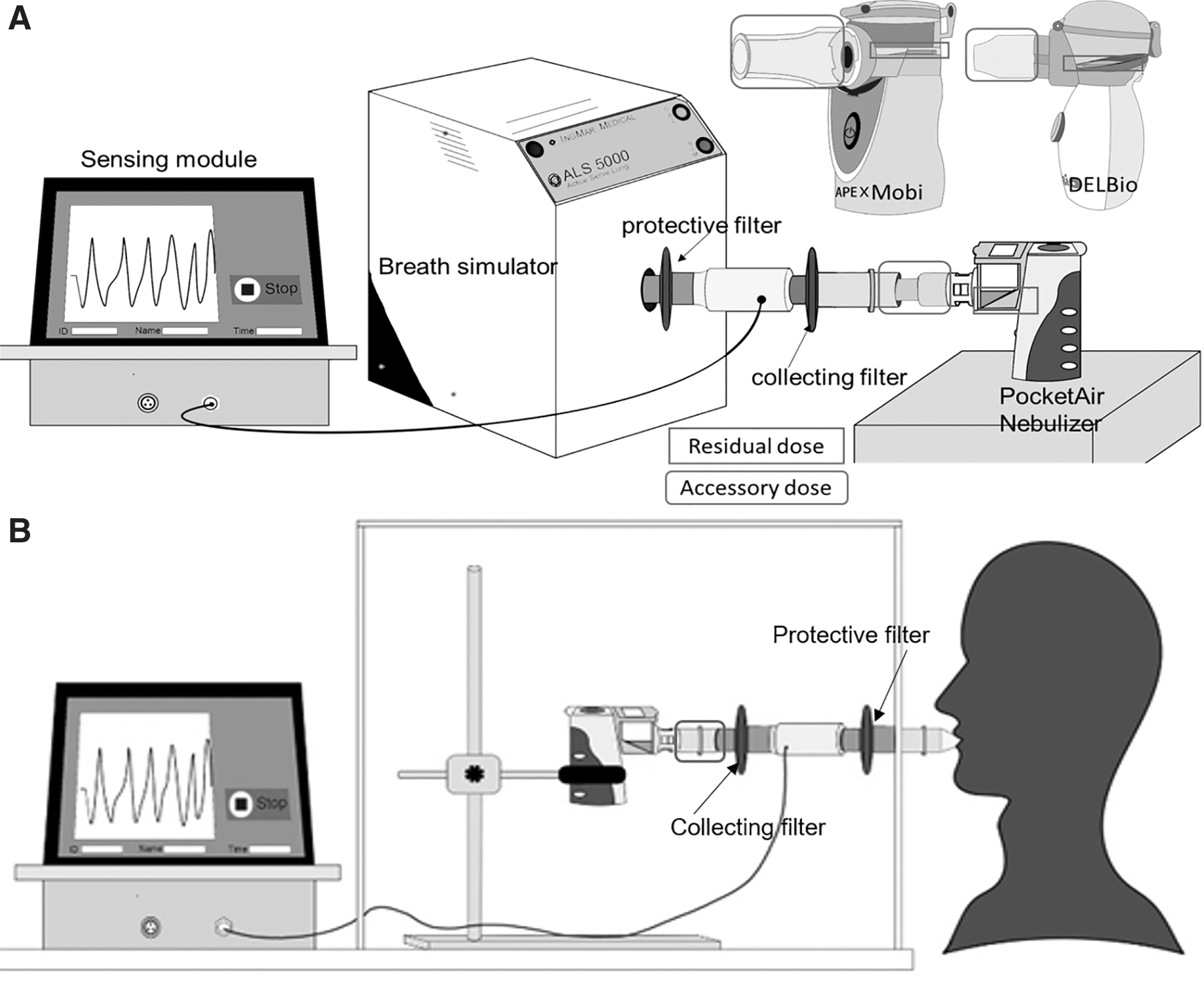
Experimental apparatus of the in vitro
Inspiratory Flow Under Various Respiratory Parameters in the In Vitro Model
With a respiratory rate of 15 breaths/min, inspiratory time was set at 2 seconds for inspiratory time to total cycle time (Ti/Ttotal) 50%, 1.2 seconds for Ti/Ttotal 33%, and 0.8 seconds for Ti/Ttotal 25%. With a respiratory rate of 30 breaths/min, inspiratory time was set at 1 second for Ti/Ttotal 50%, 0.67 seconds for Ti/Ttotal 33%, and 0.5 seconds for Ti/Ttotal 25%.
First, a vibrating-mesh nebulizer (PocketAir™ nebulizer; Microbase Corp., Taoyuan, Taiwan) was tested. A unit dose of salbutamol containing 5 mg/2.5 mL (GlaxoSmithKline Corp., Victoria, Australia) was placed in the drug-holding cup, and then nebulization carried out until 30 seconds after no aerosol was visible. The delivered drug doses on the accessories and reservoirs (accessory dose) were eluted and analyzed. The experiments for each breathing pattern were repeated five replicates.
Development and validation of prediction formula
With a constant-output mesh nebulizer, the aerosolized drug is inhaled during the inspiration phase. Most nebulizers retain a certain portion of the drug in the solution-holding element, which is called the residual dose; therefore, the total nebulized dose can be calculated as the initial charged dose minus the residual dose. An interface (such as a mask) or a mouthpiece (as an accessory) is required to connect a nebulizer to the patient; however, aerosols are also deposited on the accessories and reservoirs during nebulization. A nebulizer with a reservoir and an internal space retains aerosols during the inspiratory pause and expiratory phase, which is inhaled during the next inspiration.5,20 Considering these factors, the predicted inhaled dose can be calculated as
Based on the aforementioned equation, the residual dose and retained dose must be obtained, and the inspiratory time must be measured simultaneously during nebulization. Thus, a sensor module was developed to measure the tidal volume, respiratory rate, and percentage of inspiratory time in the respiratory cycle. A prediction formula was developed according to the aforementioned equation. The predictive formula calculated the delivered dose based on the acquired respiratory parameters and predetermined residual and accessory doses. The estimated inhaled drug dose was calculated as a percentage of the initial dose for each test.
To further validate the prediction formula with different brands of vibrating mesh nebulizers, we evaluated two additional nebulizers, namely the DELBio™ (Philips Corp., PA) and Mobi™ (Apex Corp., Taipei, Taiwan) nebulizers, which were designed with a different drug-holding chamber, mouthpiece, and aerosol exit adaptor (shown in Fig. 1A).
The simulator was used to deliver a normal breathing pattern with a tidal volume of 500 mL and respiratory rate of 15 breaths/min, according to the ISO guidelines, with Ti/Ttotal of 50%, 33%, and 25%. The experiments for each nebulizer were repeated five times. After obtaining the doses at each component for each nebulizer from the in vitro model, the prediction formula was modified accordingly.
Ex vivo study
The accuracy of the modified prediction formula was validated in an ex vivo study. Healthy adults, aged >20 years, were recruited for this study. The exclusion criteria were as follows: (1) history of pulmonary disease, asthma, allergic rhinitis, or arrhythmia; (2) use of β-blocking agents such as propranolol; (3) tobacco use; and (4) diagnosis of tuberculosis. This study was approved by the Chang Gung Memorial Foundation Institutional Review Board (approval no. 202002614A3). Informed consent was obtained from participants before the experiment.
Figure 1B illustrates the apparatus used in the ex vivo experimental setup. The participants were randomly assigned to test the three vibrating mesh nebulizers. A bacterial filter was used to capture aerosols at mouth and a preventive filter was used to prevent contamination between participants. The sensor was placed between the two filters to measure the respiratory parameters.
Ten participants were enrolled and first trained to use each nebulizer filled with 3 mL normal saline before data collection. They were encouraged to breathe through their mouths using a nose clips. Participants tended to breathe with large tidal volumes during the training period. Thus, each participant's favorite program was played on a smartphone to divert their attention from breathing during testing. A unit dose of salbutamol 5 mg/2.5 mL was placed into the selected nebulizer and powered until 30 seconds after no aerosol was visible during nebulizer tests.
Drug assay
The collecting filter, silicon adaptor, mouthpiece, and drug-holding chamber were disassembled for the drug assays after each test. The aerosolized drug deposited on each component was eluted using distilled water with gentle agitation for 2 minutes. The absorbance of each drug sample was measured using an ultraviolet spectrophotometer (Thermo Fisher Scientific, Inc., Waltham, MA) with a wavelength at 276 nm. There was a linear relationship between the absorption and concentration of salbutamol between 2.0 and 250 μg/mL, with a slope of 0.0068 (r 2 = 0.9999). The mass of salbutamol was calculated from the absorption–concentration standard curve.
Statistical analysis
Descriptive statistics, including the mean and standard deviation, were calculated. Data were analyzed using the Statistical Package for the Social Sciences (version 24.0; IBM, Inc., New York, NY). The amount of drug deposited on the filter and each component was expressed as a percentage of the intimal charge. Drug delivery among nebulizers was compared using a one-way analysis of variance of the delivered drug dose, nebulization time, residual dose, and accessory dose among three nebulizers. A one-sample t-test and Pearson correlation analyses were conducted to compare drug depositions with different tidal volumes, respiratory rates, and two experimental models. The Bland–Altman plot was conducted for the agreement between delivered and predicted doses. Statistical significance was set at p < 0.05.
Results
In vitro study
Table 2 shows the doses delivered for various breath parameters. The delivered drug dose was significantly influenced by all the parameters (F = 336.1; p < 0.001). The delivered drug dose was significantly higher with Ti/Ttotal 50%, followed by 33% and 25% (p < 0.001). For the same Ti/Ttotal percentage, we observed that the influence of the respiratory rate was greater than that of the tidal volume. For example, with Ti/Ttotal of 50% and tidal volume of 500 mL, the delivered dose decreased by 6.3% after adjusting the rate from 15 to 30 breaths/min. Adjusting the tidal volume from 500 to 700 mL at a fixed rate of 15 breaths/min decreased the delivered dose by only 1.9%. Pearson's tests showed a strong correlation with Ti/Ttotal (Fig. 2A; r2 = 0.888, p < 0.001) and inspiratory flow (Fig. 2D; r2 = 0.861, p < 0.001), a moderate correlation with the respiratory rate (Fig. 2B; r2 = 0.424, p = 0.001), and a low correlation with tidal volume (Fig. 2C; r2 = 0.155, p = 0.225).
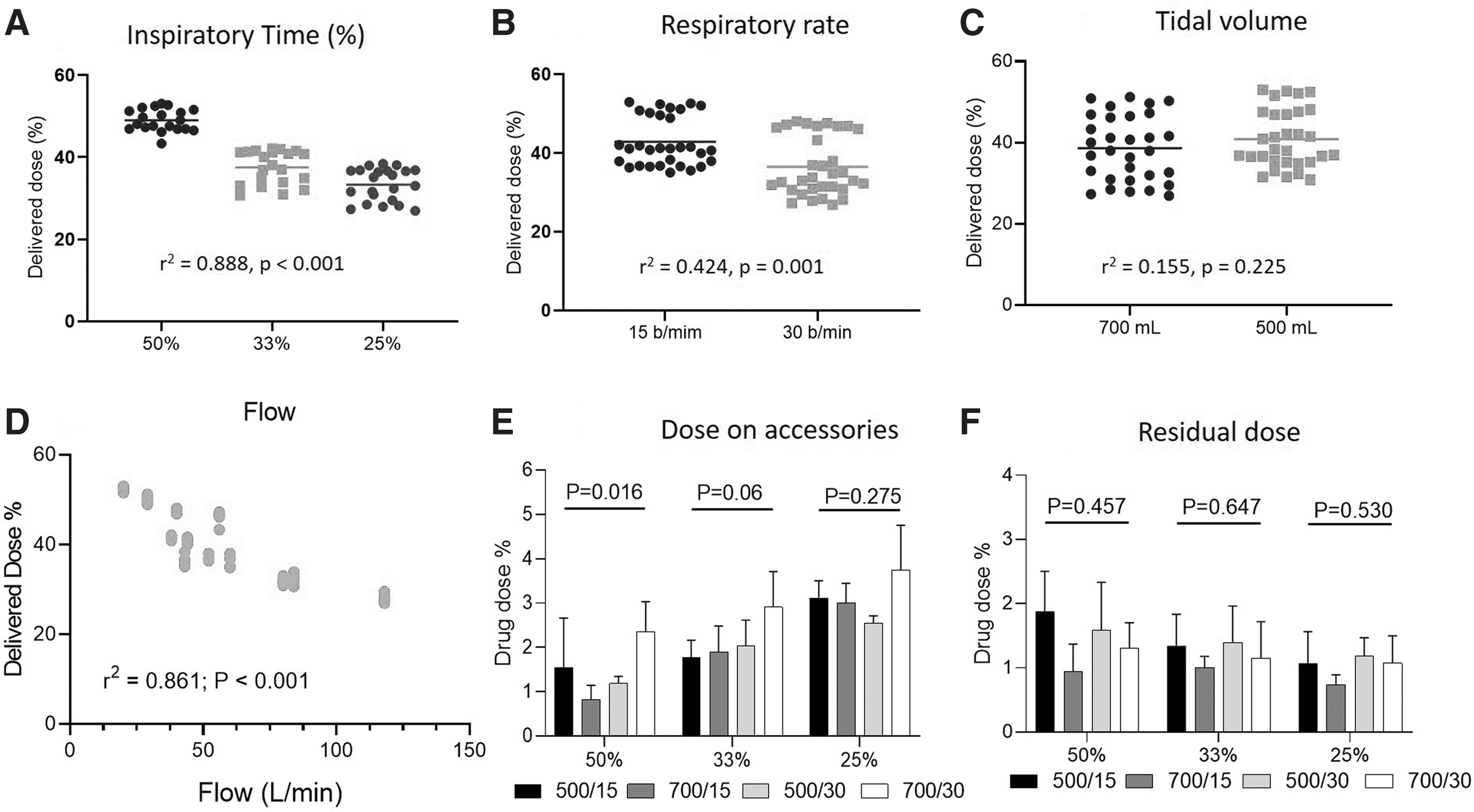
Comparisons of drug depositions with respiratory parameters. Note: 500/15 represents a tidal volume 500 mL with respiratory rate 15 breaths/min; 700/15 represents a tidal volume 700 mL with respiratory rate 15 breaths/min; 500/30 represents a tidal volume 500 mL with respiratory rate 30 breaths/min; 700/30 represents a tidal volume 700 mL with respiratory rate 30 breaths/min.
Delivered Dose with Various Parameters
Ti/Ttotal: inspiration time to total cycle time %.
Comparison of tidal volume with t-test; p < 0.001.
Comparison of respiratory rates using t-test; p < 0.001.
Comparison of inspiratory to expiratory ratio using ANOVA; p < 0.001.
ANOVA, analysis of variance.
Drug deposition on the accessory was significantly influenced by Ti/Ttotal (p < 0.001; Fig. 2E). Under a 50% Ti/Ttotal, a greater deposited dose occurred with a tidal volume of 700 mL and respiratory rate of 30 breaths/min. The residual dose in the nebulizer was similar across all settings, as shown in Figure 2F (p = 0.512).
Development of prediction formula with differently designed nebulizers
Figure 3 shows a comparison of the three nebulizers with different variables (Fig. 3A–C). Ti/Ttotal significantly affected the delivered dose (p < 0.001) for the three nebulizers; the greater the Ti/Ttotal, the greater the delivered dose. The delivered dose was significantly higher for PocketAir, Mobi, and DELBio (Fig. 3A, p < 0.001), as Mobi had a significantly higher residual dose (Fig. 3B, p < 0.001). The Ti/Ttotal had no impact on the residual dose (p = 0.37). The drug dose on the accessory was significantly greater with the DELBio (p < 0.001).
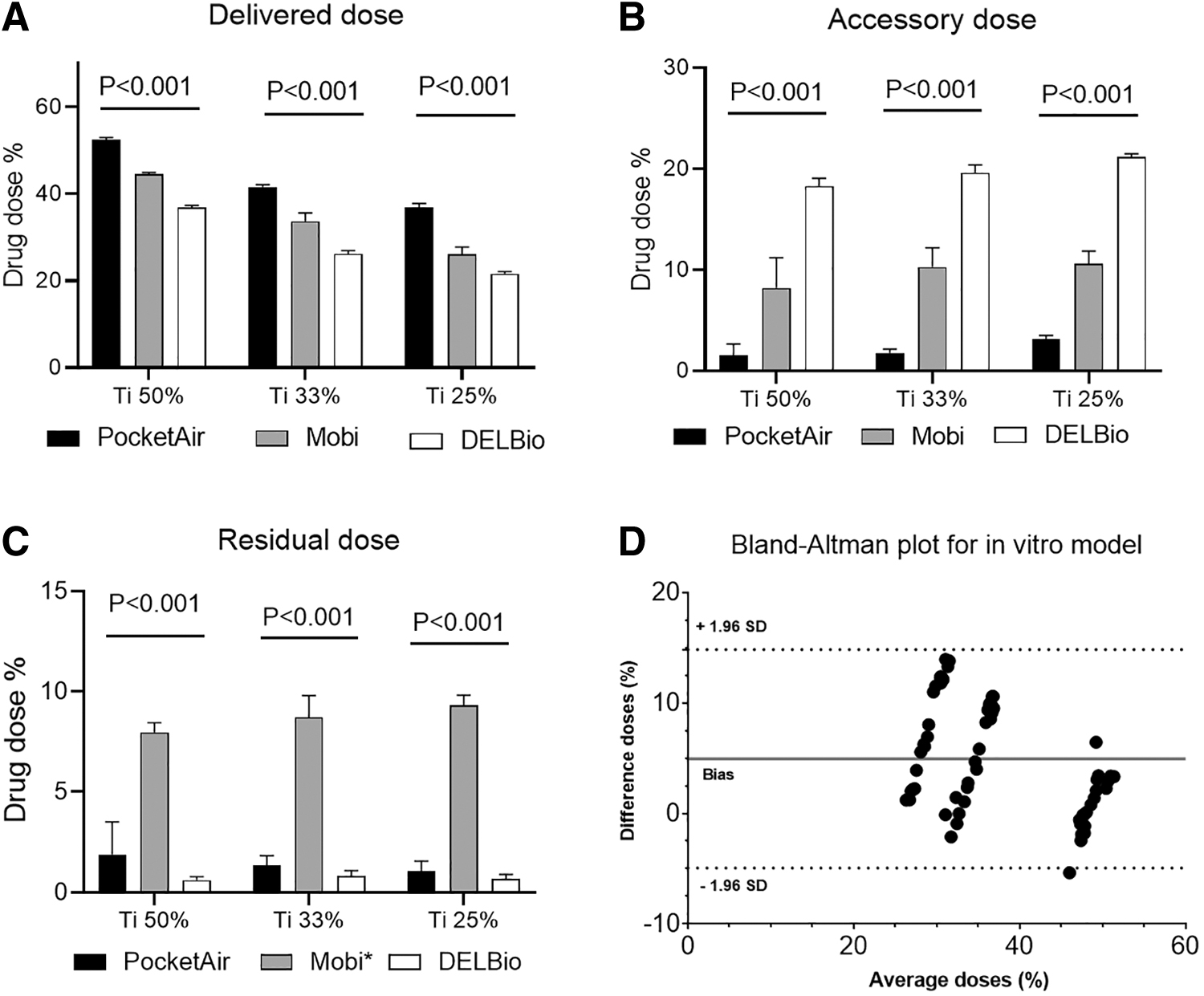
Comparisons of inhaled dose
According to data from the in vitro study and the sensing module, a strong correlation was found between the retained dose and pause time (r
2
= 0.824, p < 0.001). Linear regression equations were established for each nebulizer based on the delivered dose. The equations were simplified, and then an algorithm was rewritten as follows:
In the aforementioned equation, k is a constant that represents the retained dose in a unit of time.
According the ISO standard testing with Ti/Ttotal 50%, the residual doses in the drug-holding chamber were 1.43% ± 0.93% for the PocketAir, 1.28 ± 0.45 for the Mobi, and 1.11% ± 0.72% for the DELBio. In addition, the dose deposited on mouthpiece and aerosol exit (accessory) were 1.47% ± 0.85% for the PocketAir, 2.18 ± 0.71 for the Mobi, and 3.13% ± 0.72% for the DELBio. Those results were in cooperated to the prediction formula for each nebulizer are written as follows:
For a PocketAir nebulizer:
For an Apex nebulizer:
For a Philips nebulizer:
The agreement between the delivered dose from the in vitro model and the predicted dose according to the equations aforementioned was tested with the Bland–Altman analysis. The results showed a bias, referring to the mean differences, 4.94% and all data were fitted in the 95% confidence intervals (Fig. 3D). The Bland–Altman analysis appeared in three groups. The group on the left, presenting dose differences of Ti 25%, showed a trend that the differences tended to get larger with higher doses; on the contrary, the group on the right for the dose differences of Ti 50% tended to be larger with lower doses.
Ex vivo study
Ten participants were recruited with a mean age of 24.8 ± 2.86 years, height of 169.2 ± 6.8 cm, tidal volume of 993.8 ± 524.8 mL, and respiratory rate 13.4 ± 6.48 breaths/min. Table 3 shows the demographics of the participants and the parameters of breath patterns between men and women. Although the participants were coached with normal breaths and provided entertainment on a cellphone, the results showed large tidal volumes with high minute ventilation. The Ti/Ttotal was 37% with a 9%–10% breath hold time, which accounted for ∼47%–48% of the inspiration time.
Demographic of Participants
Data analyzed using ANOVA.
Aerosol delivery and correlations to respiratory parameters
Table 4 shows that the inhaled dose from the collecting filters was significantly greater with the PocketAir than with the other two nebulizers (p < 0.001). The DELBio had a significantly greater dose deposited on the accessories (p < 0.001) but with the lowest residual dose (p < 0.001). The differences between predicted dose and delivered dose were 3.0%–4.65%.
Percentage of Breath Cycles and Delivered Dose and Deposited Dose on Accessories and Residual Dose
Data analyzed with ANOVA; *p < 0.05; **p < 0.001.
Correlations between inhaled dose, respiratory parameters, and nebulizer performance ex vivo were tested. The percentage of inspiratory time to total respiratory cycle time was significantly correlated with the delivered dose among the respiratory factors (r 2 = 0.367, p = 0.046), in addition to strong correlations with nebulization time (r 2 = 0.613, p < 0.001) and the dose deposited on the accessory (r 2 = −0.732, p < 0.001). The nebulizer brand was moderately correlated with the drug delivery dose (r 2 = −0.372, p = 0.01). Other factors, including tidal volume, respiratory rate, minute ventilation, expiration time, and residual dose, were not correlated for inhaled doses.
Agreement between delivered and predicted doses
The agreement between the delivered and predicted doses was tested with the Bland–Altman plot within a 95% confidence interval. Figure 4A–C shows the individual delivered doses for each nebulizer. Great intrapersonal differences were found; for example, the largest differences in inhaled dose among the subjects were 21.68% for PocketAir, 18.22% for DELBio, and 12.86% for Mobi. The Bland–Altman plot for the ex vivo model shows a bias 0.65% with differences between −7.6% and 9.2% (Fig. 4D). There are strong correlations, ranging from 0.88 to 0.967 among the three nebulizers (Fig. 4E; all p < 0.001).
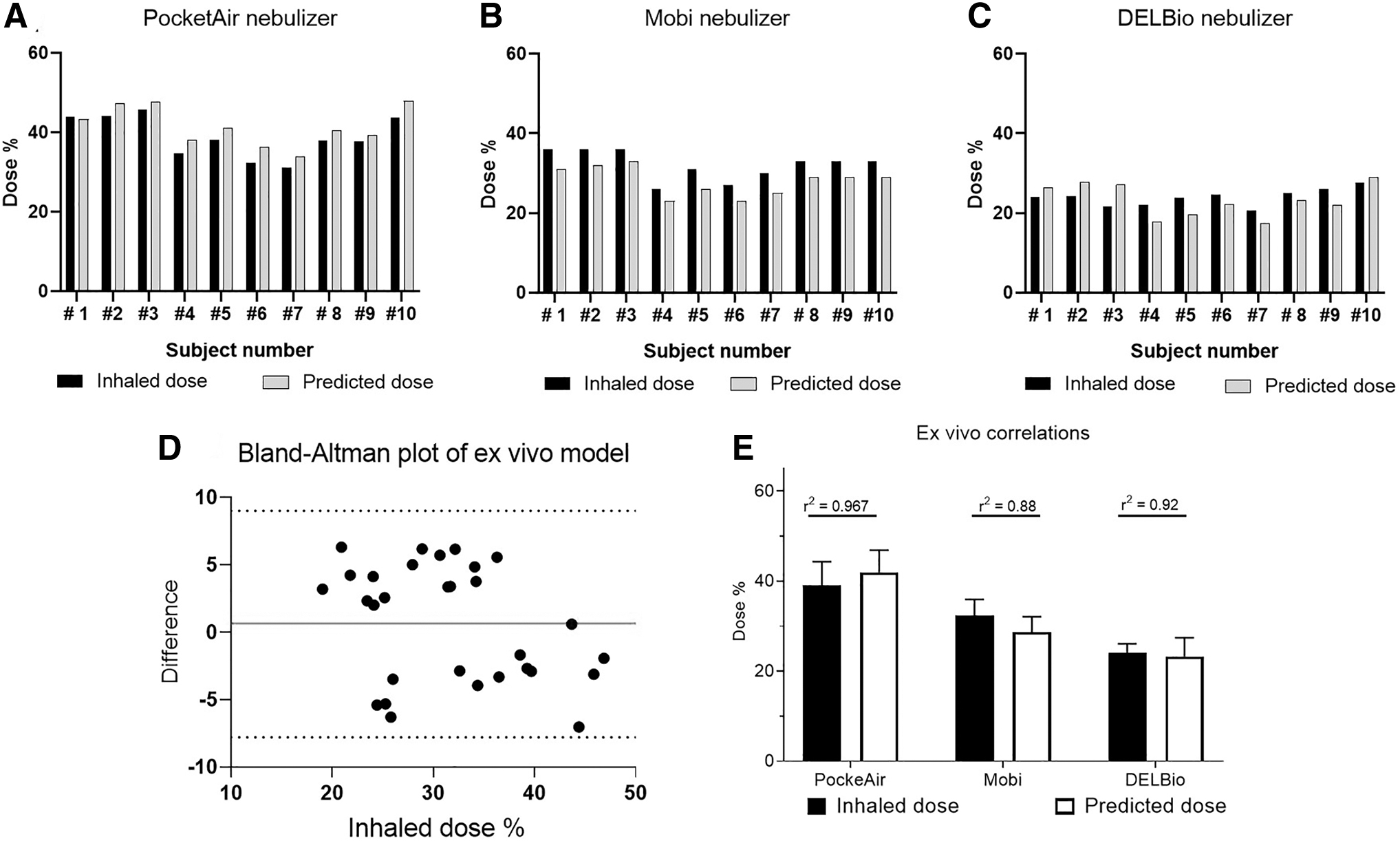
Comparisons of inhaled dose of each participant between the inhaled and predictive doses among the three nebulizers. The Bland–Altman plot shows mean of the predicted and inhaled doses (%) and difference between the predicted and inhaled doses (%).
Discussion
The estimation of delivered inhaled drugs provides clinicians with a better evaluation of drug responses and symptoms for disease management. We developed a prediction formula for the delivered aerosol dose that accounts for the breath pattern of the user and performance of the nebulizer. The prediction formula was validated using real breath patterns from ex vivo testing. Our results demonstrate great intrapersonal differences in delivered drug doses; however, small differences with strong correlations between the predicted and actual inhaled doses may indicate the accuracy of the predicted algorithm. Lung deposition of inhaled drugs is essential for achieving therapeutic effects and is a focus in aerosol medicine.
An inadequate dose deposited in the lungs may compromise the physiological effect of the drug, and an overdose may lead to adverse effects. The inhaled drug varies by drug formulation, device design, and patient characteristics, and most studies have focused on inhalers for which the lung dose is technique dependent. 21 In addition, in vivo–in vitro correlations have been considered for predicting pulmonary drug deposition using physical airway models and computational fluid dynamics models for inhalers.12,22,23 However, steady features of breathing patterns generated by a simulator may underestimate drug delivery. 19
Although most studies on inhaled drug doses often report a central tendency by their mean or median, it is possible that the delivered drug may underestimate the differences between subjects. Previous studies have shown great intra-subject variability, with two- to sixfold differences in lung dose compared with five metered-dose inhalers. 24 This is the first study to report intrapersonal variability in aerosolized drug delivery generated by mesh nebulizers. The inhaled dose by participants was 31.2%–45.9% for PocketAir, 24.5%–27.7% for Mobi, and 26.5%–36.4% for DELBio nebulizer.
Our prediction formula accounts for both patient breath characteristics and nebulizer factors. The sensing module used a flow sensor to measure inspiratory flow and time, as well as the average percentage of inspiration, expiration, and pause times with respect to the total cycle time during the measurement. The breath cycle time of each phase was integrated into the prediction formula alone, with a predetermined residual dose and accessory dose. The predicted dose was computed simultaneously at the end of the nebulization. During the development of the formula, the predicted doses tended to be overestimated for Ti/Ttotal of 25% and underestimated for Ti/Ttotal of 50% (Fig. 3D).
The formula was adjusted, and the results of the collected and predicted inhaled doses showed differences within 7% randomly (Fig. 4D). We observed that the Mobi nebulizer was intermittently interrupted during nebulization, while a low drug solution volume was detected. The results showed a lower correlation than that of the other two nebulizers, indicating the influence of nebulizer performance on the accuracy of dose prediction. Previous studies have demonstrated that adding accessory devices, such as a holding chamber or a reservoir bag, for nebulizers significantly improves the inhaled dose. The design of a nebulizer and its accessory affects the inhaled dose; thus, the predicted algorithm requires reformulation for the individual nebulizer.5,20
The ISO standard for a nebulizer requires a breathing simulation with a set I:E ratio of 1:1, as a Ti/Ttotal 50%. 7 Similarly, our results from the ex vivo model showed a Ti/Ttotal 47%–48%. Hence, our sensing module, measured with healthy participants, confirmed the requirement for breath simulation according to the ISO standard. In our study, the Ti/Ttotal for delivering a higher drug dose was ∼50%. This was inconsistent with Ti/Ttotal of 46%–58% from previous studies because of the inspiratory time set.4,11 We found a stronger correlation (r 2 = 0.888) with the Ti/Ttotal than what had been reported in a study by Bauer et al.
Whereas the ISO 27427:2013 requires a test with a breathing simulator to generate a respiratory rate of 15 breaths/min, Ti/Ttotal 50%, and a tidal volume of 500 mL, previous studies have shown the alteration of inhaled dose with different I:E and respiratory rates.4,12,13 We compared the breathing rates independently, whereas the tidal volumes and Ti/Ttotal remained constant in a well-controlled in vitro study, the results indicated a moderate correlation with respiratory rate. The tidal volume was not associated with the deposition dose across different Ti/Ttotal and respiratory rates. The results conflicted with several existing studies due to small discrepancies, such as a tidal volume of 500 mL versus 700 mL for adult simulations in our model. Remarkably, the tidal volume had the highest effect in the child and infant breathing models, caused by the greater influence on dead space 23 ; however, it was not the case in the adult model.
Inspiratory flow is a primary factor influencing lung deposition in various inhalation devices.25,26 Pressurized metered dose inhalers require a low inspiratory flow of 20 L/min, whereas dry powder inhalers require a flow ranged 30–60 L/min. Lung depositions are correlated with inspiratory flows, as the higher the flow rate, the greater the inhaled drug dose for dry powder inhalers.27,28 In contrast, for nebulizer use, inhaled drug dose is associated with slow inspiratory flow. Our results showed an inverse correlation between the delivered dose and inspiratory flow (Fig. 2D). A fast inspiratory flow increases inertial impaction, which would have increased deposited drugs in this in vitro model. However, the different results might be due to the effect of inspiration time. A longer inspiratory time or a larger Ti/Ttotal % increases the inhaled drug dose per unit of time with a constant output nebulizer.
Known respiratory or device factors can influence the lung deposition of inhaled drugs, thus further affecting their therapeutic effects. Intrapersonal differences may lead to inconsistent treatment outcomes and difficult disease control. Predictions have been developed for metered-dose inhalers and dry powder inhalers for a technique-dependent device. This prediction formula for nebulizers provides a real-time method for measuring inhaled drug dose in proportion to the total dose. The estimated inhaled drug doses during the preclinical phase of drug development allow researchers to develop a dose–response chart and lead to effective drug titration.
Smart nebulizers, such as the Akita jet nebulizer, utilize breath-control mechanism to deliver a regulated flow to the patient, resulting in slow deep inhalation.29,30 Otherwise, some smart nebulizers operate with breath-actuation during inspiration to prevent drug waste during expiration for maximized delivered drug dose. Whereas innovated nebulizers adopt breath control for optimal aerosol delivery, our prediction formula measures patient's breath pattern and proves an estimated delivered dose for existing nebulizers.
Our study has several limitations. To develop the prediction algorithm, the drug dose deposited on the accessories and reservoirs of each brand required predetermination. As each nebulizer composite has its own unique design, the dose deposited on the accessories and in the reservoir of each brand must be determined before the implementation of this prediction formula. Extensive experimental tests are needed before they can be widely adapted.
In addition, the predicted algorithm was tested with an ex vivo study that measured the delivered dose at the mouth rather than in the lower airway. The dose to the lower airway was expected to be lower due to oropharyngeal impaction. Future correlations with in vivo data would be required to develop a truly useful model, as well as to establish a reliable correlation between the predicted drug dose and therapeutic efficacy. In addition, for consistent nebulizer performance, experiments were conducted with one nebulizer from each brand. However, the accuracy of prediction formula may be altered with the variation of each nebulizer.
Conclusions
Aerosolized drug delivery was influenced by both patient factors and device characteristics, with variations in the doses delivered to individuals. The prediction formula developed in the study demonstrated a good prediction for three brands of mesh nebulizers, achieving strong correlations. Nevertheless, the development of prediction formula required predetermination; thus, the prediction formula in our study may be solely applied to the tested devices.
Footnotes
Authors' Contributions
Conceptualization by Y.-C.H. and H.-L.L. Data curation by H.-H.L., W.-C.C., and H.-L.L. Formal analysis, resources, supervision, and writing—review and editing by H.-L.L. Investigation by W.-C.C. and H.-L.L. Methodology, validation, visualization, and writing—original draft by H.-H.L. and H.-L.L. Project administration by H.-L.L., T.P.F., and Y.-C.H.
Author Disclosure Statement
H.-L.L. received research grants from the Microbase Technology Corp., National Science and Technology Council, and Chang Gung Memorial Foundation. Y.-C.H. and W.-C.C. were employees of Microbase Technology Corp. during research period. The other authors have disclosed no conflict of interest.
Funding Information
This study was partially funded by the Microbase Technology Corp. and National Science and Technology Council (Most-2314-B182-067), grant SCRPD1K0561. The funders had no role in data collection, analyses, or interpretation in the writing of the article or in the decision to publish the results.
Reviewed by:
Stephan Erhmann
Ariel Berlinski