
Abstract
Experiments designed to image in vivo deposition of radiolabel-drug mixtures are useful for estimating inhaled drug delivery and for assessing bioequivalence of delivery devices. Validation of the radiolabel-drug mixture is vital to ensure that subsequent imaging is reflective of drug deposition. Application of gamma attenuation corrections allows both total and regional lung deposition of drug to be estimated by two-dimensional (2D) imaging. Imaging methods are also useful for measuring in vivo mucociliary clearance (MC) function. Such measures allow assessment of the efficacy of drugs designed to improve clearance of airway secretions in airway disease. MC rates can be measured by controlled inhalation and gamma camera monitoring of radiolabeled aerosols containing non-permeating tracers. While in vivo MC rates reflect the function of the mucociliary apparatus, they are also dependent on regional deposition patterns of the inhaled aerosol.
Introduction
This section of the chapter on imaging aerosol deposition and mucociliary clearance briefly describes strategies required for assessing in vivo particle deposition and clearance. The details associated with the specific imaging technologies are described in other sections of this chapter, and more complete details of how to best use these technologies with suggestions for standardization have recently been published in the Journal of Aerosol Medicine and Pulmonary Drug Delivery (JAMPDD).(1–4)
In vivo Deposition Studies
Use of imaging technologies to assess deposition of inhaled drugs (or their surrogates) has been important for estimating the amount of medication delivered to the lung for various drug delivery devices. Furthermore, these imaging methods allow for assessment of bioequivalence by comparing total and regional lung deposition associated with multiple aerosol devices/products. To standardize the techniques for in vivo aerosol deposition assessment of orally inhaled products, the International Society for Aerosols in Medicine (ISAM) Regulatory Affairs Networking Group convened the Sub-committee for the Standardization of Lung Imaging Techniques in 2010. As a result of these efforts a supplement to JAMPDD(1–3) was published that provides practical guidance on the methods and techniques for standardizing radiolabel validation and image acquisition/analysis using planar (two-dimensional [2D]), single photon emission computed tomography (SPECT) and positron emission tomography (PET) imaging modalities.
For the purposes of this review, the design and methods described are for 2D planar imaging of particle deposition,(3) but similar procedures can be used for three-dimensional (3D) methods of SPECT and PET with associated differences in image analysis and tracers. Again, these latter techniques are described in other sections of this chapter and the JAMPDD supplement on “Standards for Lung Imaging.”(1)
Radiolabeling
The first step in the process of in vivo deposition studies is validation of the radiolabeled drug formulations.(2) In most cases the drug itself is not labeled but rather is mixed in solution or as a dry powder with a short half-life radioisotope such as 99mTc (half-life = 6 hours). Because the radioisotope is not chemically bound to the drug, validation is required to insure that the radiolabeling technique has not altered the aerosol particle size characteristics of the formulation and that the size distribution is similar as determined by activity of the label vs. mass of the drug.
The aerodynamic particle size distribution (APSD) of drug for both the reference formulation and the radiolabel-drug formulation must be characterized using a multistage cascade impactor, such as a multistage liquid impinger, an Andersen Cascade Impactor, or the Next Generation Impactor.(2) An example of such validation data is given in Figure 1 for radiolabeling of extrafine beclomethasone dipropionate (BDP). Such validation data should be repeatable/reproducible for a given device/drug combination. For these sets of data it can clearly be seen that the drug and radiolabel have similar particle size distributions. Devadason and colleagues also provide recommendations for determining the acceptability of the radiolabeling validation.(2)
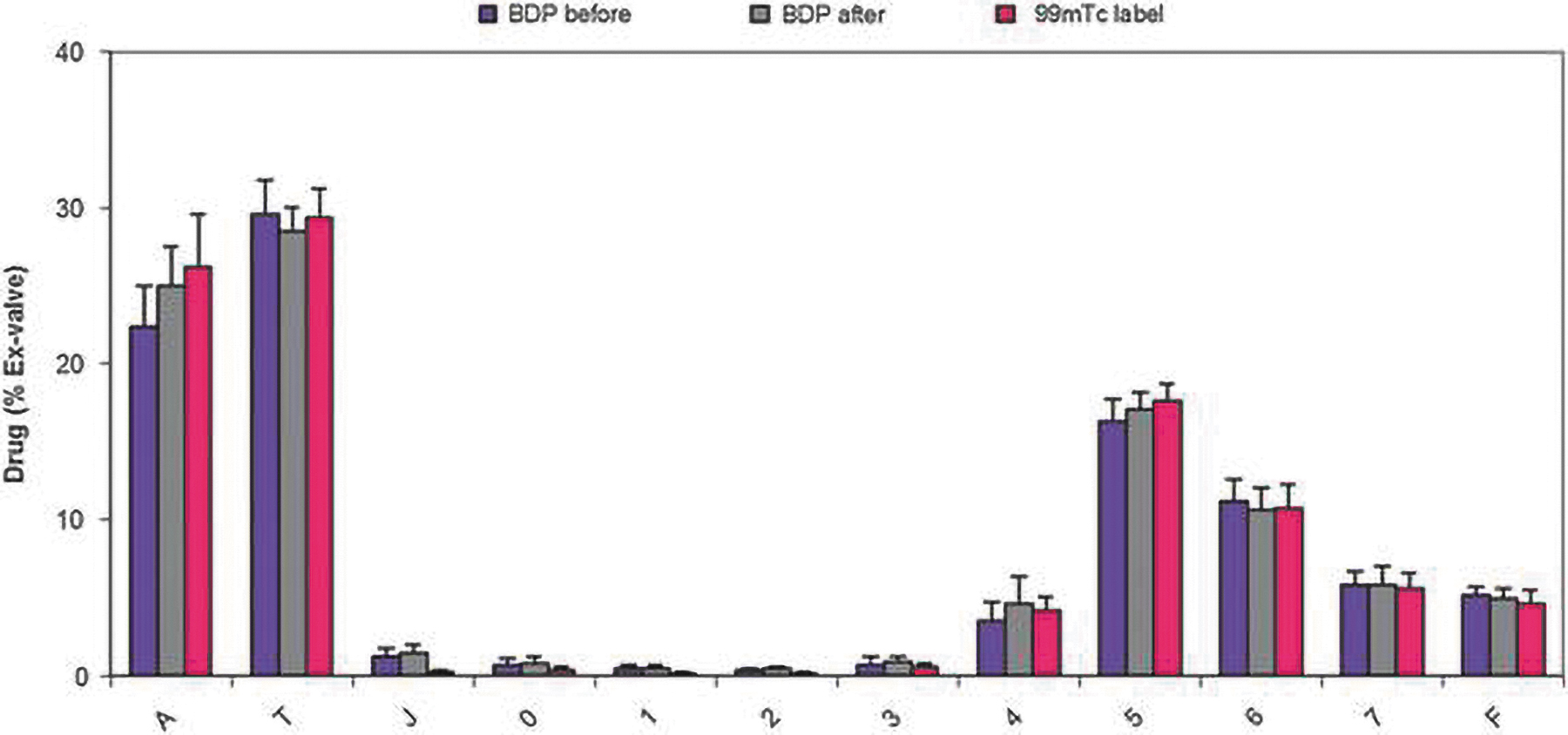
. Radiolabeling of extrafine beclomethasone dipropionate (BDP): Comparison of the APSD of the reference drug (BDP before) with radiolabeled drug (BDP after) and radiotracer (99mTc label) using an Andersen Cascade Impactor. Abscissa represents the stages of the impactor from largest (left) to smallest (right) particle sizes, A = actuator, T = throat, J = jet, and F = filter.(2)
Quantification of deposition
Newman and coworkers(3) describe in great detail the methods for quantifying total and regional deposition in the lungs and extrathoracic airways (mouth, throat, pharynx, and larynx) by planar (two-dimensional [2D]) imaging using a single-headed or dual-headed gamma camera, the most widely used and most straightforward of the radionuclide imaging methods used to assess drug deposition.
Radioaerosol inhalation from the device should be accomplished in the same manner as would occur under realistic drug delivery conditions. Accordingly, subjects should practice the correct inhalation maneuver before the radioaerosol inhalation and the key inhalation parameters (e.g., inhalation flow rate, inhaled volume, and breath-hold pause) should be recorded. The radioaerosol inhalation should occur in front of or in close proximity to the camera (with appropriate shielding) to obtain an immediate scan of deposited activity in the respiratory tract.
Imaging should allow for inclusion of the mouth, lungs, and stomach to obtain accurate measurements of total and regional intra- vs. extrathoracic deposition. A reference image of the lung obtained by transmission (e.g., 57Co) or gas equilibrium (e.g., 133Xe) should be obtained to outline the edges of the lung. An example of such scans is shown in Figure 2. In this example, it is clear that the lung borders are not delineated accurately in the aerosol scan, because the aerosol has penetrated poorly to peripheral lung regions. Corrections to observed counts should also be made to allow for radioactive background and decay and gamma ray attenuation by body tissues. To quantify deposition from inhaler devices accurately, correction for gamma ray attenuation is essential in 2D imaging studies. Further details on determination of total deposition in the respiratory tract (as well as mouth vs. lung) may be found in Newman and colleagues.(3)

Transmission (from a Tc99m flood source), Xenon-133 equilibrium, and deposition image (aerosol of Tc99m-sulfur colloid) in the same healthy, nonsmoking adult.(4) Reproduced with permission from Mary Ann Liebert publications.
According to the ISAM recommendations for regional lung deposition analysis,(3) the lungs should be divided into inner (I) and outer (O) rectangular regions as defined and illustrated in Figure 3. The O/I deposition ratio should be calculated and normalized by dividing by either the corresponding ratio for a radioactive gas scan or by that for a transmission scan (sample images in Fig. 2). Regional lung analysis should normally be confined to the right lung to avoid problems of stomach/left lung overlap, but in patients with severe lung disease, consideration should be given to analyzing data from both lungs.
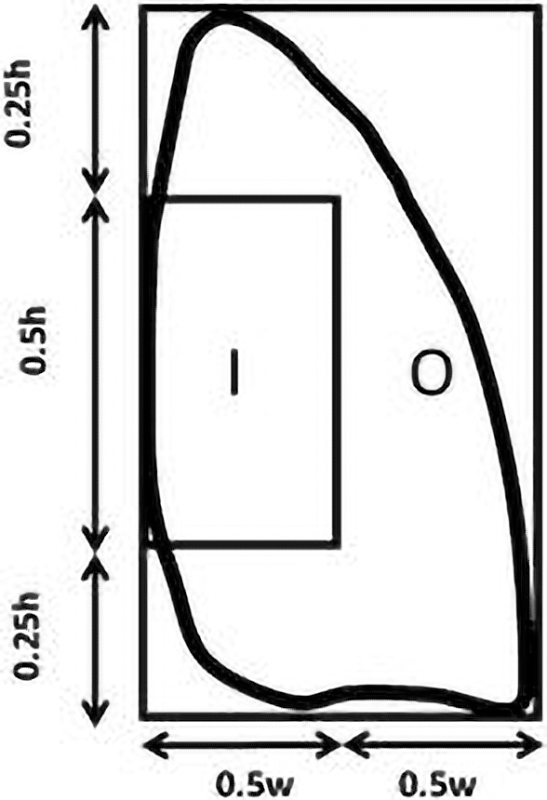
Recommended method for dividing the right lung into inner (I) and outer (O) zones. An inner region with dimensions equal to half of the width (w) of a whole-lung rectangle and one-half of its height (h) is positioned on the interior boundary of the lung, centered by height. The I and O regions represent 25% and 75%, respectively, of the area of the whole-lung rectangle.(3)
In Vivo Mucociliary Clearance Studies
As with the above description on in vivo deposition, the following description of methods and design of in vivo mucociliary clearance studies is limited to those in humans, and greater detail is provided in two recent reviews.(4,5) Mucociliary clearance (MC) rates can be measured in humans by assuming that a non-permeating, inhaled marker depositing on the airway surface moves out of the lung at the same rate as the airway secretions in which it is immersed.(6) The most common technique is to use inhaled, radiolabeled (99mTc) particles, aqueous or dry, that upon deposition in the lung can be followed by a 2D gamma camera to determine their rate of egress from the lung. After controlled inhalation of these markers, retention of activity in the lung (as a percent or fraction of initial deposition) is monitored by gamma camera as a function of time (decay and background corrected) over a period of up to 24 hours to determine clearance rates (Fig. 4).
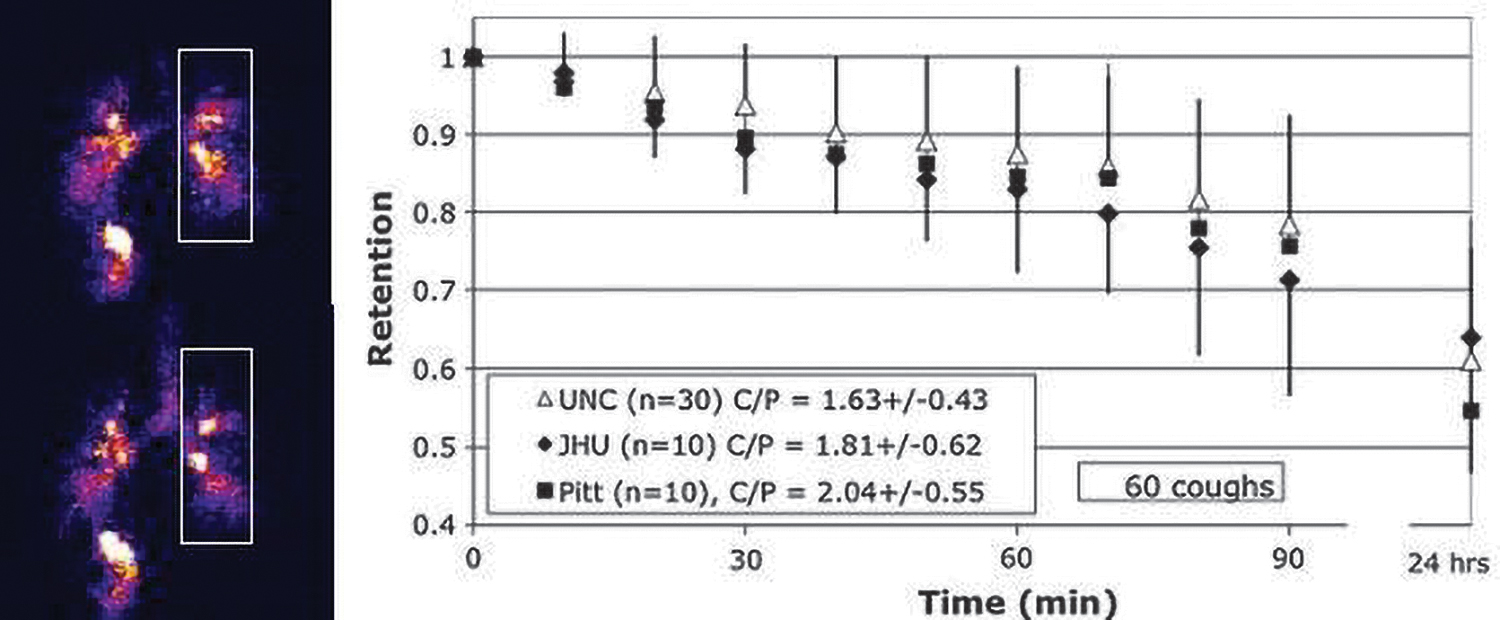
Left. Deposition image (top) and 20 minutes post deposition (bottom). Activity seen moving up the trachea. Right. Comparison of average retention at each time point for each of the three sites using standardized MC methods. UNC – University of North Carolina; JHU – Johns Hopkins University; Pitt – University of Pittsburgh.(7) Reproduced with permission from Mary Ann Liebert publishers.
Controlled inhalation of the radiolabeled aerosols is important for targeting the bronchial airways and improving intrasubject repeatability of MC measures. The breathing patterns employed by different laboratories are quite variable,(4) but each strives to produce sufficient airway versus alveolar deposition to provide for measure of MC over a 24-hour period. Recently, three study sites (University of North Carolina, Johns Hopkins University, and University of Pittsburgh) performed MC measures in healthy, nonsmoking adult subjects using a standard methodology for inhalation of the radioaerosol and analysis of images.(7) The subjects in this study inhaled an aerosol (mass median aerodynamic diameter of 5.4 um, geometric standard deviation = 2.0) of sulfur colloid labeled with99mTc from a DeVilbiss 646 nebulizer. While breathing the radiolabeled aerosol, the subject targeted his/her tidal flow and breathing rate at 500 mL/s and 30/min, respectively, by following a visual flow signal while breathing in time to a metronome. The resulting retention vs. time data is illustrated in Figure 4, showing similar results between the three sites. By comparison, Mortensen and coworkers(8) achieved greater clearance over the first 1–2 hours, but they did not control inhalation flow rates or tidal volumes per se. Rather they had subjects perform slow inhalations of radiaoaerosol followed by a forced exhalation, the latter providing efficient large airway deposition. However, the repeatability of their measures within an individual, which is important for crossover studies of therapeutic effects on MC, is not known. More recently, it was shown that the MC signal could also be enhanced (i.e., more clearance through 24 hours) by use of larger aerosol particles (9.5 um) and controlled very slow inhalation flow (0.08 L/s).(9)
The rate of particle clearance from the lung is highly dependent on regional deposition in the lung, that is, the more proximal the deposition of particles occurs in the bronchial airways the more rapidly particles will leave the lungs. Controlling particle size characteristics and inhalation patterns in patients, as described above, is an attempt to minimize intrasubject variability in regional particle deposition. But intersubject variability in regional deposition is also affected by variation in airway and lung sizes between individuals. For either case, intra- or intersubject comparisons, an index of initial, regional deposition (e.g., central/peripheral [C/P] or O/I ratio as illustrated in Fig. 3) are needed to include as a covariate in analyses of particle clearance from the lungs. To accomplish this, a clear definition of the lung provided by a transmission or gas equilibrium scan is required to prepare regions of interest (ROIs) (Figs. 2 and 3) that can be overlayed on the deposition image to calculate regional deposition.
For some patient groups and therapies, the primary airway clearance mechanism of interest may be that of coughing. Because some patients may not be able to avoid coughing during clearance measurements, the number and timing of spontaneous coughs should be recorded. Then in the study design, the number of spontaneous coughs might be considered as a covariate in the analysis to ensure that frequency of these coughs does not overly influence any differences due to therapy effects. Some investigators have included a separate study arm with voluntary coughs equal to the number of spontaneous coughs in the treatment arm as a “cough” control measurement,(10) that is then compared to the other arms to correct for spontaneous cough effects. While uncontrolled coughing may confound measures of MC, measuring cough clearance by incorporating controlled, voluntary coughs during the measures of particle clearance may provide a more sensitive indicator of rheological changes in airway secretions (e.g., in the 60–90 minute period of retention measurements in Fig. 4).(7)
The MC methodology has been valuable for assessing acute enhancement of mucus clearance in patients with airways disease (e.g.,(6,8,10–12). The most recent example of this success has been with the application of inhaled, hyperosmotic agents (hypertonic saline and mannitol) to improve clearance of secretions and lung function in cystic fibrosis (CF) patients.(11,12) The MC biomarker may also become an important tool for assessing new therapies for other airway diseases, for example, chronic obstructive pulmonary disease (COPD) and asthma, as there becomes increasing awareness of the role that insufficient MC plays in these diseases.
SUMMARY
Imaging of in vivo deposition is useful for estimating inhaled drug delivery and for assessing bioequivalence of delivery devices.
Supplement to JAMPDD, “Standardization of Lung Imaging Techniques,” provides practical guidance on these in vivo methodologies.
Validation of the radiolabel-drug mixture is vital to ensure that subsequent imaging is reflective of drug deposition.
With attenuation corrections, both total and regional lung deposition of drug may be estimated by 2D imaging.
In vivo MC rates can be measured by controlled inhalation and gamma camera monitoring of radiolabeled aerosols containing non-permeating tracers.
While in vivo MC rates reflect the function of the mucociliary apparatus, they are also dependent on regional deposition patterns of the inhaled aerosol.
In vivo measures of MC are useful for assessing the efficacy of drugs designed to improve clearance of airway secretions in airways disease.
Footnotes
Author Disclosure Statement
The author declares there are no conflicting financial interests.
Funding Information
No funding was received for this work.