
Abstract
Rationale:
Neonates with respiratory issues are frequently treated with aerosolized medications to manage lung disease or facilitate airway clearance. Dynamic tracheal collapse (tracheomalacia [TM]) is a common comorbidity in these patients, but it is unknown whether the presence of TM alters the delivery of aerosolized drugs.
Objectives:
To quantify the effect of neonatal TM on the delivery of aerosolized drugs.
Methods:
Fourteen infant subjects with respiratory abnormalities were recruited; seven with TM and seven without TM. Respiratory-gated 3D ultrashort echo time magnetic resonance imaging (MRI) was acquired covering the central airway and lungs. For each subject, a computational fluid dynamics simulation modeled the airflow and particle transport in the central airway based on patient-specific airway anatomy, motion, and airflow rates derived from MRI.
Results:
Less aerosolized drug reached the distal airways in subjects with TM than in subjects without TM: of the total drug delivered, less particle mass passed through the main bronchi in subjects with TM compared with subjects without TM (33% vs. 47%, p = 0.013). In subjects with TM, more inhaled particles were deposited on the surface of the airway (48% vs. 25%, p = 0.003). This effect becomes greater with larger particle sizes and is significant for particles with a diameter >2 μm (2–5 μm, p ≤ 0.025 and 5–15 μm, p = 0.004).
Conclusions:
Neonatal patients with TM receive less aerosolized drug delivered to the lungs than subjects without TM. Currently, infants with lung disease and TM may not be receiving adequate and/or expected medication. Particles >2 μm in diameter are likely to deposit on the surface of the airway due to anatomical constrictions such as reduced tracheal and glottal cross-sectional area in neonates with TM. This problem could be alleviated by delivering smaller aerosolized particles.
Introduction
The treatment of several diseases that affect neonates, such as chronic lung disease of prematurity (known as bronchopulmonary dysplasia [BPD]), requires the administration of inhaled aerosolized medications including bronchodilators, which reduce small airway obstruction, or corticosteroids, which reduce airway inflammation.1–3 For these inhaled medications to reach the target area of the small airways within the lungs, they must pass through the trachea en route to the lungs. However, many neonates with diseases such as BPD will also have comorbid tracheomalacia (TM), which is the dynamic collapse of the tracheal lumen during respiration.4–7 This study aims to quantify the effect of TM on drug delivery to the lungs.
The size of aerosolized drug particles plays a major role in determining where in the respiratory tract a particle will deposit. For example, Leach et al. 8 showed that 55%–60% of particle size of 1.1 μm deposited in healthy adult lungs compared with 4%–7% of drug with a particle size of 3.5 μm. The optimal particle size range that is delivered to the conducting airways depends on the airway size of the patient, which increases with age, 9 but the particle diameter size of the aerosolized bronchodilators used to treat neonates varies considerably; from <1 μm to >10 μm10–14 and there is no ideal particle diameter size that guaranteed drug delivery to the lungs.
As an example, the mass median aerodynamic diameter of albuterol in a nebulizer is ∼5–6 μm. 15 Optimizing the particle sizes used for drug delivery would ensure sufficient drugs are delivered to the desired region of the lungs while minimizing delivery elsewhere in the respiratory tract. However, the impact of dynamic tracheal collapse on the delivery of inhaled aerosolized particles to the target region in the lungs has not yet been considered.
Previous studies in adults and idealized airway models have shown that airway obstructions and glottis motion can reduce pulmonary drug delivery16–19 because more particles in the diameter range of 6–10 μm are deposited in the obstructed region. In the neonatal population, we have previously demonstrated that neonates with TM have a smaller glottis cross-sectional area than subjects without TM, as they generate auto-positive end expiratory pressure (auto-PEEP). 20
While the tracheal collapse of TM occurs predominately during exhalation, narrowing of the trachea and the glottal opening can be seen during both inhalation and exhalation, and it is possible that this smaller glottal opening during inhalation reduces aerosol delivery to the lungs, assuming the same effect of airway narrowings causing particle deposition occurs in neonates as it does in aforementioned adult studies.
In this study, we use patient-specific computational fluid dynamics (CFD) simulations to model airflow and particle transport within the central airways (upper airway to main bronchi) in subjects with and without TM. Our CFD models incorporate patient-specific airway anatomy, motion, and airflow rates obtained through ultrashort echo time (UTE) magnetic resonance imaging (MRI).20–23
These simulations quantify the particle mass delivered beyond the central airway to more distal airways and deposition percentages in the central airway based on particle diameter range. The objective of this study is to measure the effect of TM on the amount of drug delivered to the lungs during inhalation in neonates and to determine if some particle sizes are more affected than others when traversing an airway with TM.
Methods
Subjects
This study included 14 neonatal intensive care unit subjects with written parental consent and the approval of the Institutional Review Board (IRB) of Cincinnati Children's Hospital Medical Center. All subjects were using clinically assigned respiratory support at the time of UTE magnetic resonance imaging (MRI) and no sedation was used for the purposes of imaging (Table 1); none of the subjects were intubated. Out of 14 subjects, 7 subjects were diagnosed with TM and 7 did not have TM.
Subject Demographics
BPD,bronchopulmonary dysplasia; CPAP,continuous positive airway pressure; MRI, magnetic resonance imaging; PMA, post-menstrual age; TEF/EA, tracheoesophageal fistula/esophageal atresia; TM, tracheomalacia.
Airway imaging and image reconstruction
To create the subject-specific virtual airway models, subjects were imaged using a neonatal-sized MRI scanner with a field strength of 1.5 T and captured the airway anatomy, motion, and airflow parameters.22,24–27 Each subject was imaged for 16 minutes. The initial point of the free induction decay waveform of the MRI was recorded. This waveform was modulated due to the breathing and bulk motion of the subject. 28 The image acquisition and reconstruction used in this study have been published previously.22,23,29
To capture the movement of the airway and lungs during the breathing cycle, four respiratory-gated UTE MR images at different points in the respiratory cycle were reconstructed retrospectively using the initial point of the free induction decay waveform of the MRI, after removing the bulk motion of the subject, as previously described.22,28,30,31 The four gated images represent end exhalation, peak inhalation, end inhalation, and peak exhalation time points.22,23
Airway dynamics and airflow conditions
Three-dimensional airway surfaces were segmented from the four gated MR images at each time point using the active contour segmentation technique.23,32 The segmented airway surfaces extended from pharynx to main bronchi. 33 The airway surfaces were smoothed using Taubin smoothing filter.34,35 After smoothing the airway surfaces, surface registration was performed through Medical Image Registration ToolKit (version 1.1) software to obtain the motion and position of the airway at any given time during the respiratory cycle.21–23
Each neonate's airflow rates through the main bronchi were obtained using lung tidal volume measurements and the respiratory waveform.22,23,36 The end exhalation and end inhalation MR images were used to calculate each lung tidal volume. The respiratory waveform was derived from the MRI free induction decay signal, and it was scaled based on each lung tidal volume. More details on airway segmentation, registration, airway motion, and airflow rates can be found in previously published research.22,23
Particle modeling and simulation
STAR-CCM +14.04.011-R8 (Siemens PLM Software), a commercial CFD software package, was used to simulate airflow and particle transport in the airway. Each patient's airway anatomy, motion, and airflow rates were used as inputs to perform CFD simulations as described in previous studies.20,22,23 In brief, the airway was discretized using polyhedral cells in the interior and prism layers on the wall. The airway mesh consisted of ∼5 million cells and a temporal resolution of 0.8 ms.22,23
A convergence study was performed to check the independence of the particle deposition map to the mesh size and time step duration. Time steps varied between 0.08 and 1.6 ms and mesh sizes varied between 0.5 million and 10 million cells. Simulations using a mesh of 5 million cells and a time step of 0.8 ms provided the best compromise between solver time and accuracy. The difference in particle delivery to the distal airways between the finest mesh and 5 million cells simulations was 1.3% and between the finest time step and 0.8 ms was 1.9%.
The inlet of the airway was set at ambient pressure while the airflow rates were applied at the main bronchi. Throughout the respiratory cycle, the airflow was assumed to be incompressible and isothermal at body temperature. The large-eddy simulation (LES) mathematical model was used to model turbulence, and a no-slip condition was applied at the airway walls. We have previously validated CFD findings using this approach against in vivo airway measurements using phase-contrast hyperpolarized Xe MRI. 37
At the inlet plane of the airway, a particle injector grid was created that emitted particles throughout inspiration. Each point in the grid randomly releases monodisperse particles with aerodynamic diameters ranging from 0.5 to 15 μm for every time step. 38 The particles' diameter distribution is uniform and continuous. This study models one inhalation of drug delivery, quantifying the proportion of drug particles that enter the lungs out of those that enter the pharynx. In a clinical setting, the drug is given until all the particle mass has been inhaled, which takes roughly 10 minutes.
Previous studies demonstrated that most of the respirable particle diameter range is 1–5 μm and the majority of larger particles deposit in the upper airway.39–41 The particles were simulated using the Lagrangian phase model in STAR-CCM+, which included drag force, Saffman shear lift force, and pressure gradient force. To test if Brownian motion had a significant effect on the delivery of small particles (<1 μm), simulations were performed with Brownian motion in one patient without and one patient with TM.
The difference in particle mass delivered to lower airways due to Brownian motion was 1.3% and 1.6%, respectively. As this difference is small, Brownian motion was not included in subsequent simulations. The particles were assumed to be fully deposited on the airway wall when they reached the airway surface as the mucus layer of the airway mucosa is 97% liquid and readily absorbsfluid particles. 42
Data analysis
Particles were categorized by three separate outcomes by the end of one modeled inhalation: delivery to more distal airways, deposition in the central airway, and suspension in the air within the central airway. All particle mass that reached the main bronchi at the end of one modeled inhalation was calculated as a percentage compared with the total mass inhaled (released from the injector grid). All particle mass deposited in the airway at the end of inhalation was calculated as a percentage compared with the particle mass inhaled.
These percentages were calculated separately for each particle diameter range to identify which particle size range(s) were more effective for drug delivery beyond the central airway in neonates with TM. Shapiro–Wilk test was performed on the data set to verify that the data are normally distributed. A two-tailed unpaired and unequal variance t-test was used to compare the findings between TM and non-TM groups.
To quantify the airway dynamics of the two subject groups, the maximum cross-sectional area and minimum of the minor-to-major diameter ratio were calculated (Table 1). The change in maximum cross-sectional area from end expiration to end inspiration was expressed as a percentage relative to the end inspiration airway, following the methodology demonstrated in previous work. 43 To determine the minimum of the minor-to-major diameter ratio, minor and major diameters were obtained for each airway as described previously.43,44
For each particle diameter range, Stokes number was calculated using the following equation:
9
where
This study assumed that the particles have density of water. The mean inhalation velocity was calculated by using the mean inhalation airflow divided by the average glottis cross-sectional area for each subject. This value was used as the characteristic velocity
Results
Particle mass delivered to more distal airways
Figure 1 demonstrates the percentage of particle mass delivered to the distal airways in neonatal subjects diagnosed without TM and with TM, for all particle diameters included (0.5–15 μm). On average, the percentage of inhaled particle mass delivered to the distal airways was 47% ± 4% and 33% ± 10% in subjects without TM and with TM, respectively (p = 0.013). It is noted that the eight of the subjects in the cohort with BPD, the percentage of inhaled particle mass delivered to the more distal airways was reduced from 48% ± 12% to 36% ± 6% due to the presence of TM.
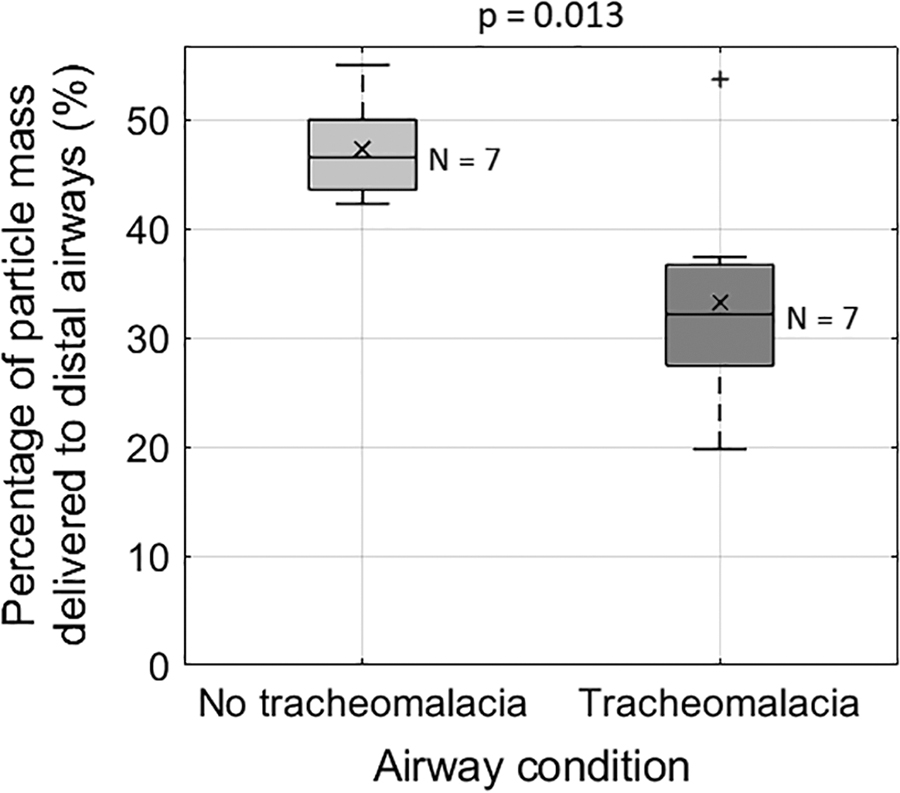
The percentage of inhaled particle mass delivered to the distal airways in subjects without TM and subjects with TM. The average percentage of particle mass delivered to the distal airways in subjects without TM was 47% ± 4% and in subjects with TM was 33% ± 10% (p = 0.013). Plot elements: average = cross; median = middle line; IQR = box; data within 1.5 times the IQR <25% or >75% = whiskers; outliers = plus sign. IQR, interquartile range; TM, tracheomalacia.
To identify the effect of particle diameter on drug delivery to the distal airways, various particle diameter ranges were investigated (0.5–1, 1–2, 2–3, 3–4, 4–5, and 5–15 μm), as shown in Figure 2A.The larger particle's diameter range (5–15 μm) was further divided into small ranges in Figure 2B. When the particle diameter range was >3 μm, a significantly lower percentage of particle mass was delivered to distal airways in subjects with TM than in subjects without TM (p = 0.02 for 3–4 μm; p = 0.005 for 4–5 μm; p = 0.005 for 5–15 μm). However, there was no significant difference between the study groups when the particle diameter range was between 1 and 3 μm (p = 0.095 for 1–2 μm; p = 0.182 for 2–3 μm), and 14–15 μm (p = 0.077).
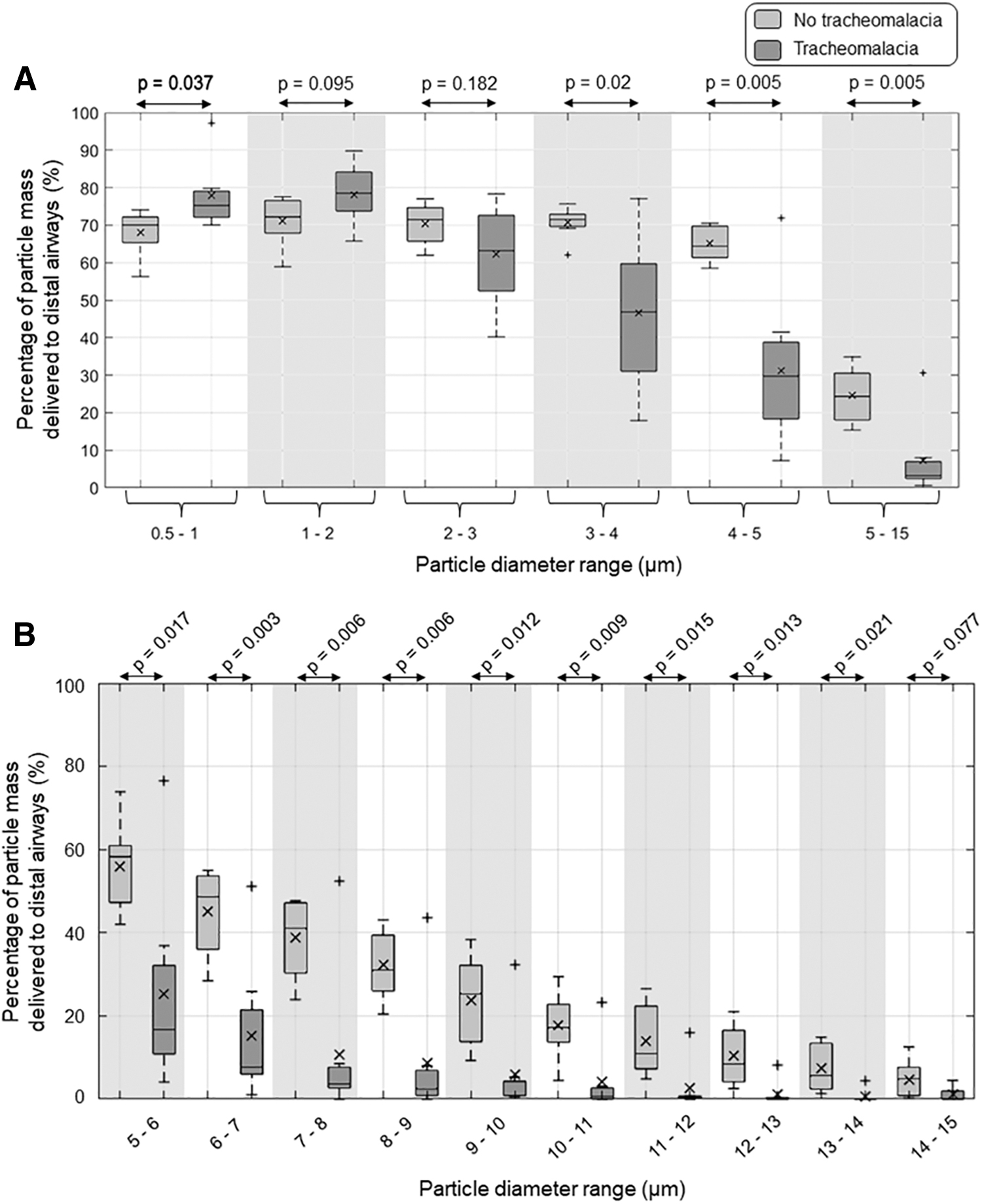
The percentage of particle mass delivered to distal airways compared with particle mass inhaled was based on the particle diameter range separated into small subgroups for smaller particles 0.5–5 μm
Particle deposition on the central airway wall
The particles that did not reach the main bronchi could either have been deposited on the central airway wall or remain suspended in the air within the central airway; these suspended particles are likely to be exhaled during the next exhalation, rather than re-inhaled for delivery to the more distal airways. The percentage of particle mass deposited on the central airway wall (upper airway to main bronchi) in subjects without TM and subjects with TM is shown in Figure 3. On average, a higher percentage of particle mass was deposited on the central airway wall in subjects with TM than in subjects without TM compared with the total mass (particle diameter range 0.5–15 μm) inhaled (48% ± 13% vs. 25% ± 7%, respectively; p = 0.003).

The percentage of particle mass deposited on the airway wall (upper airway to main bronchi) in subjects without TM and subjects with TM. The average percentage of particle mass deposited in the airway in subjects without TM and subjects with TM was 25% ± 7% and 48% ± 13%, respectively (p = 0.003). Plot elements: average = cross; median = middle line; IQR = box; data within 1.5 times the IQR <25% or >75% = whiskers; outliers = plus sign.
Figure 4 represents the effect of particle diameter on particle mass deposited on the airway wall. When the particle diameter was >2 μm, a significantly higher percentage of particles was deposited in the central airway in subjects with TM than in subjects without TM (p = 0.025 for 2–3 μm; p = 0.008 for 3–4 μm; p = 0.003 for 4–5 μm; p = 0.004 for 5–15 μm), Fig. 4A). However, there was no significant difference between the study groups when the particle diameter range was between 0.5 and 2 μm (p = 0.1 for 0.5–1 μm; p = 0.069 for 1–2 μm), and 14–15 μm (p = 0.083).

The percentage of particle mass deposited on the airway wall compared with particle mass inhaled based on particle diameter range separated into small subgroups for smaller particles 0.5–5 μm
Figure 5 demonstrates the airflow pattern at peak inhalation (Panel A) and the particle deposition at the end of inhalation in the central airway for the respirable particle range (0.5–5 μm, Panel B) and the remainder of the delivered range (5–15 μm, Panel C); two example subjects without TM and with TM are shown. In neonates without TM, the glottis expands during inhalation and narrows during exhalation. However, we have previously shown that the glottis is much narrower in neonates with TM compared with neonates without TM at all breathing phases. 20
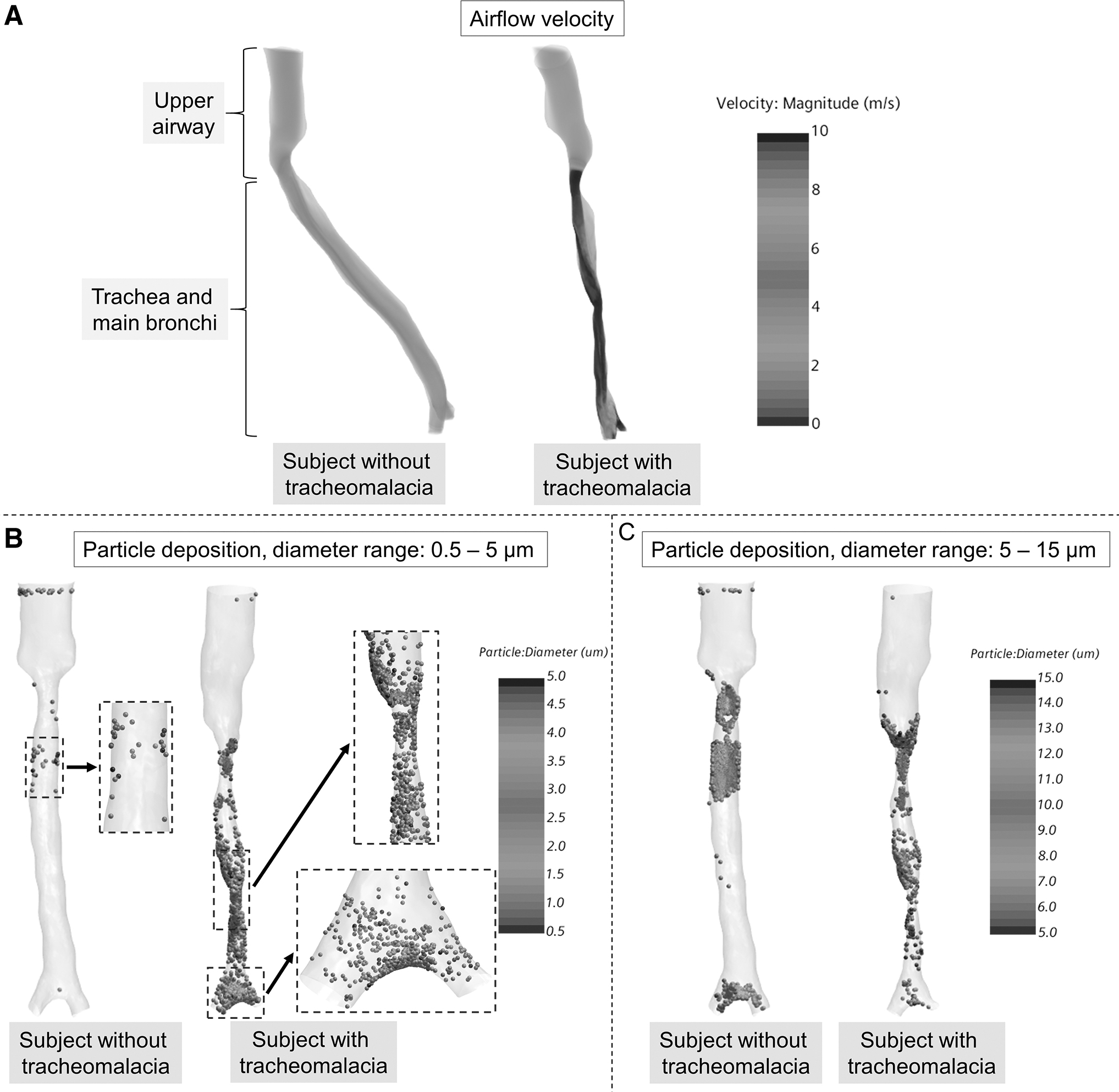
Airflow velocity distribution
In the subject with TM, many particles were deposited in the middle of the trachea, where there is reduced cross-sectional area due to airway collapse, and in the main bronchi (Panel B). However, fewer particles were deposited in the central airway of the subject without TM. In both example subjects, the larger particles (>5 μm) have been deposited near the carina due to higher momentum (Panel C), although this can be observed to a stronger degree in the subject with TM.
To understand the particle deposition in the neonatal airway as a function of the Stokes number, the deposition percentage was plotted against the Stokes number for all 14 subjects (Fig. 6). The deposition percentage of the airway in subjects with TM has shifted to lower values of Stokes number compared with the deposition percentage of the subjects without TM.
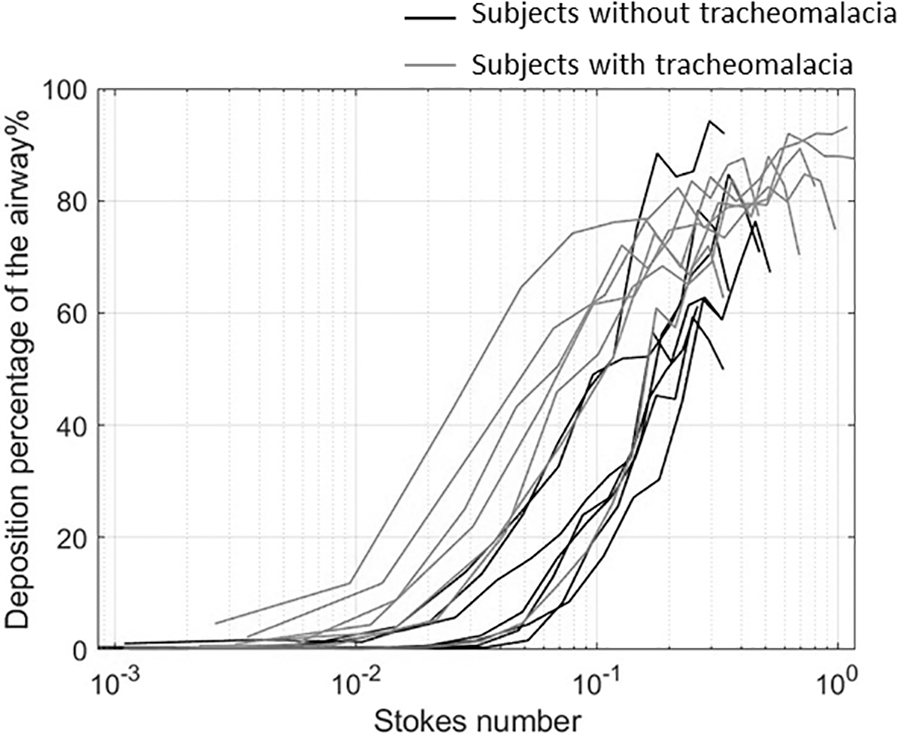
Deposition percentage of the airway vs. Stokes number. The deposition percentage of the airway in subjects with TM has shifted to lower values of Stokes number compared with the deposition percentage of the subjects without TM.
Discussion
This study suggests that TM significantly affects the distribution of inhaled drug deposition in neonates. Major findings of this study include that less mass of aerosolized drug reaches beyond the main bronchi in neonates with TM than in neonates without TM and that a larger amount deposits on the central airway wall in neonates with TM, although the deposition in neonates with and without TM is similar if particles are between 1 and 2 μm.
These results raise several questions that may impact the clinical care of neonates with TM:
In subjects with TM and comorbid lung disease, is a sufficient volume of aerosolized bronchodilators reaching the lungs, as currently implemented in clinical settings? Is the increased quantity of bronchodilator particles deposited on the tracheal wall in subjects with TM exacerbating the tracheal collapse by relaxing the trachealis? Could bronchodilators be delivered at smaller particle sizes (e.g., ∼1 μm at the lower end of the respirable range), at which size more particles reach the lungs in neonates with TM and without TM and potentially not impact the trachea?
Currently, the aerosolized drug doses for neonates are determined based on body weight, but the particle size delivered is not altered to account for patient size. Several studies have raised the importance of using smaller particles in children as smaller particles have a lower probability of depositing in the upper airway.9,45–48 Our results highlight that when the particle diameter was >2 μm, there was a dramatic increase in particle deposition in the trachea in neonates with TM compared with neonates without TM (Fig. 5). Less than 5% of particles >5 μm can reach the smaller airways in neonatal subjects with TM. This could have significant implications for inhaled therapies administered in neonates.
The impact of the dynamic collapse of the trachea on the path of inhaled aerosolized particles to the target region in the lungs has not yet been considered. The findings of this study suggest that TM could affect the response to inhaled therapies. The nebulized bronchodilators such as albuterol primarily deposit in the central airway, this will serve to relax tracheal smooth muscle, increase airway collapse, and worsen respiratory mechanics. 49 Furthermore, by depositing on airways proximal to the carina, the peripheral airways would be less likely to receive the benefit of bronchodilation for those patients with concurrent reversible airway obstruction.
However, metered-dose inhalers which are typically preferred to deliver smaller particles than nebulizers could minimize this impact.10,14 As with bronchodilators, the impact of TM could help explain some of the disparate outcomes with inhaled steroids in neonates who are born extremely premature. Infants randomized to receive nebulized inhaled steroids show a reduction in the development of BPD, but there is a concern for increased mortality; however, the increased risk of mortality is less clear in studies that relied on metered-dose inhalers for steroid treatment. 2
Several mechanisms contribute to the difference between particle mass delivered to the lungs in neonates without TM and with TM. In neonates with TM, the glottis cross-sectional area and tracheal cross-sectional area are smaller compared with neonates without TM.20,44 The narrower cross-sectional area leads to a higher airflow velocity for the same airflow rate, resulting in particles with more momentum that are more likely to hit the central airway walls.
Our previous work suggests that neonates with TM have a higher minute volume compared with neonates without TM, perhaps due to their elevated work of breathing. 22 However, the difference was not statistically significant. The airway motion associated with TM changes the shape of the tracheal cross-section to be less round, which may lead to increased particle deposition on the tracheal walls.43,44 The relative contribution of each of these mechanisms to increased particle deposition is not known but may be the focus of future studies.
We have shown previously that the airflow inside the airway can be turbulent and may need to account for turbulence in the CFD simulation. 23 This study used the LES turbulence model to account for the effect of turbulence in the airway. Previous studies have demonstrated the sensitivity of deposition results depends on the mesh size and turbulence model.50,51For example, Koullapis et al. 51 demonstrated that LES simulations capture more of the turbulent flow features across a range of length scales than Reynolds Averaged Navier–Stokes simulations.
These flow features will affect the deposition of particles, which was one of the reasons for selecting the LES model in this study. In this work, a convergence study was performed using meshes with up to 10 million cells, in line with the mesh sizes used in the aforementioned studies (although the neonatal geometries used in this study are much smaller than the previous studies), and a mesh with 5 million cells was chosen as it resulted in only a 1.3% difference in the percentage of particles reaching the distal airways.
The main limitation of this study was that the airway geometry only included a subsection of the respiratory tract; the MRI field of view only included a portion of the more proximal upper airway, and the image voxel size (∼0.7 mm) was too large to capture more distal airways beyond approximately the main stem bronchi. A portion of the upper airway was included to provide the inflow conditions for the trachea, but the effects of nasal and bronchial anatomy and the particle size distribution of various drugs were not included in this study.
Releasing equal numbers of particles of different sizes into the pharynx differs from the in vivo case, where drugs have particular size distribution functions and are inhaled at the nose, which may filter out some particles before they reach the pharynx. However, in this study, we did not investigate the efficacy of a particular drug and reported only the percentage of particles that are deposited between the pharynx and bronchi, at each particle size.
Therefore, the inlet distribution function does not affect these results. A larger cohort is needed to compare which mechanical therapy is most effective in enhancing delivery to the distal airway is beyond the scope of this article. All outcomes of this study were based on inhalation-phase CFD simulation and did not take into account the exhalation phase for particle deposition. Future studies may include more complete airway anatomy and investigate which drug delivery method would be beneficial to neonates with TM (i.e., nebulizer vs. inhaler vs. spacer).
Conclusion
This study suggests that TM reduces the percentage of drug particle mass delivered beyond the central airway to the more distal airways in neonates. Particles of >2 μm diameter will primarily deposit on the airway wall in neonates with TM due to reduced tracheal and glottal cross-sectional area.To maintain treatment efficacy, neonates with TM may require a different nebulized medication with a smaller particle diameter size and/or a different medication delivery mechanism.
Footnotes
Authors' Contributions
Conceptualization by C.C.G., C.M., E.B.H., J.C.W., and A.J.B.; data collection by C.C.G., C.M., and N.S.H.; data analysis and interpretation by C.C.G., C.M., Q.X., E.B.H., J.C.W., and A.J.B.; article writing and editing by all authors.
Author Disclosure Statement
J.C.W. has a research agreement with Philips and A.J.B. has research agreements with Philips and Siemens PLM Software.
Funding Information
This study was supported by the Trustee grant award at Cincinnati Children's Hospital and the National Institutes of Health (NIH) grants R00 HL144822 and R01 HL146689.
Reviewed by:
Josue Sznitman
Tim Corcoran