
Abstract
Background:
To evaluate the safety and efficacy of 2.5 and 1.25 mg nebulized salbutamol on Transient Tachypnea of the Newborn (TTN) compared with placebo.
Methods:
We conducted a triple-blind, phase II/III parallel randomized controlled trial in two university-affiliated hospitals with neonatal intensive care units. Newborns with a confirmed diagnosis of TTN, with gestational age >35 weeks and gestational weight >2 kg were included. Cases of asphyxia, meconium aspiration syndrome, and persistent pulmonary hypertension were excluded. Ninety eligible patients were randomly allocated in three intervention groups (2.5 mg salbutamol, 1.25 mg salbutamol, and placebo), and a single-dose nebulized product was prescribed 6 hours after the birth. Safety outcomes included postintervention tachycardia, hyperglycemia, hypokalemia, and changes in blood pressure. To evaluate the efficacy, the duration of postintervention tachypnea, TTN clinical score, and clinical and paraclinical respiratory indices were assessed. Parents, Outcome assessors, and data analyzer were blind to the intervention.
Results:
There was no adverse reaction, including tachycardia, hypokalemia, and jitteriness. Both groups of salbutamol recipients showed significant improvement regarding respiratory rate, TTN clinical score, and oxygenation indices compared with the placebo (p-values <0.001). Nonstatistically significant higher hospital stay was observed in the placebo group. Single 2.5 mg salbutamol nebulization showed a little better outcome than the dose of 1.25 mg, although we could not find statistical superiority.
Conclusion:
The newly applied single high dose of 2.5 mg nebulized salbutamol is safe in treating TTN and leads to notable faster improvement of respiratory status without any considerable adverse reaction.
Registry code:
IRCT20190328043133N1.
Introduction
Transient T
TTN is usually self-limited, although it postpones breastfeeding and lengthens the hospital stay. Respiratory support can prevent potential complications, reduce hospitalization time, and assure parents.8,9 The basis of TTN Management includes: precisely monitoring newborns' oxygenation using pulse oximetry and repeated arterial blood gas (ABG) following appropriate oxygen support, adequate nutritional support, and ruling out infectious diseases and medications.1,2 There is no high-level evidence for the beneficial effects of furosemide or epinephrine on TTN regarding tachypnea and length of hospital stay.3,10 It is hypothesized that beta-adrenergic agonists enhance alveolar epithelial sodium (Na+) transport at the plasma membrane through magnifying activity of epithelial Na+ -channels, Na+ -K+ -ATPase, and protein abundance. 11 These activities are associated with the increase in fetal catecholamine release, which exert their effects through b-adrenergic receptors found within alveolar type II cells and lead to lung liquid absorption. 12
Many clinical trials reported that salbutamol prescription is going to be promising in reducing the time of hospitalization9,13 although the last updated meta-analysis showed some levels of uncertainty about the success of salbutamol administration in the respiratory improvement of newborns with TTN. 14 In these trials, salbutamol is usually prescribed in a dosage of 0.15 mg/kg through a nebulizer. Since its tolerability in neonates at the dose of 2.5 mg/kg was frequently reported,15–17 it seems reasonable to consider the early administration of a single high dose of salbutamol in infants with TTN to expedite their recovery time and facilitate the initiation of breastfeeding. This phase II/III triple-blind randomized trial study aimed to investigate the safety and efficacy of nebulized salbutamol in doses of 2.5 and 1.25 mg in TTN management compared with the placebo.
Methods
Study design
The current study is a triple-blind three-arm, parallel, randomized controlled trial. The study was conducted in two university-affiliated hospitals (Shahid Akbar-Abadi and Firooz-Abadi hospitals) in Tehran, Iran. The study groups include Group A: a single dose of salbutamol with a dose of 2.5 mg; Group B: a single dose of salbutamol with a dose of 1.25 mg; and Groups C: a single dose of normal saline as placebo. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Iran University of Medical Sciences (IUMS) Committee of Ethics in Research coded: IR.IUMS.FMD.REC.1401.413. The study was registered prospectively in the Iranian Registry of Clinical Trials as: IRCT20190328043133N1.
Participants
All newborns with gestational age >35 weeks and gestational weight >2 kg diagnosed for TTN in the study hospitals, and their parents who signed the informed consent were included in the study. The following criteria were used for diagnosis of TTN: respiratory distress (respiratory rate >60/min, grunting, nasal flaring/intercostal retraction, cyanosis) during the first 6 hours after birth and radiologic-specific findings, including the presence of fluid in the minor fissures, overinflation, prominent central vascular marking, a flattened diaphragm, increased anteroposterior diameter, and bilateral perihilar congestion. Exclusion criteria were: meconium aspiration syndrome, other known causes of newborns' tachypnea (such as respiratory distress syndrome [RDS], PPHN, pneumonia, early-onset neonatal sepsis, polycythemia, hypocalcemia, hyperglycemia, cardiac murmur in physical examination, tachycardia >180/min, arrhythmia, asphyxia).
Randomization and masking
After evaluating eligibility criteria, newborns' parents were informed about the study process, and informed consent was obtained to participate in the study. Patients were randomly allocated between three study groups. A blocked randomization method with a fixed size of six was used in the study. The random sequence was generated by the study epidemiologist utilizing the web-based software of the site: www.sealedenvelope.com. For concealment of the sequence, it was given to an independent third person and revealed individually throughout the study.
The study was triple-blind, whereas none of the newborns' parents, outcome assessors, and the data analyzer were unaware of the type of intervention received by the patients. To achieve this goal, the intervention products, two different doses of salbutamol and the placebo product, were prefilled and labeled in three 2.5-ml vials with three different cap colors, as follows: blue (2.5 mg), purple (1.25 mg), and red (placebo). This color-based pattern was used similarly to blind the data analyzer.
Procedures
All newborns with gestational age (GA) >35 weeks and weight >2 kg who suffered from tachypnea were evaluated for the presence of TTN and other possible diagnosis to assess eligibility criteria. Meconium aspiration syndrome was ruled out based on the absence of coarse reticulonodular opacities and irregular densities in chest X-ray (CXR). RDS was ruled out based on the absence of fine reticulonodular opacities and reduced inflation in (CXR) and no need for surfactant therapy. Leukocytosis >5000/mm3 and immature/mature neutrophil count <0.25, negative CRP test, and focal lesions in (CXR) were considered indicative markers for early sepsis diagnosis before the availability of blood culture results A difference between pre/post ductal O2 saturation of less than 5% rejects the presence of PPHN.
The randomization and consequence intervention was performed 6 hours postpartum after the primary workup and ensuring from eligibility criteria attainment. A baseline laboratory assessment was done to evaluate complete blood count; ABG; and serum levels of sodium, potassium, and calcium. Participants underwent cardiorespiratory monitoring all throughout the study period.
The salbutamol nebulizer solution (Cipla EU LTD, India) was prefilled in 2.5-mL vials with corresponding doses by a pharmaceutical company in a sterile situation as well as a 2.5 mL normal saline solution as the placebo. Following randomization, the content within the corresponding vial was diluted with 3.5 mL of normal saline. Subsequently, the mixture was applied into the ultrasonic nebulizer (Medineb300; Media Kavosh Company, Iran) utilizing a plastic cup. A single dose of the solutions was then nebulized at an intensity of 0.8 mL/min, with a free-flow oxygen rate of 5 L/min, beneath the cylindrical infanthood with a capacity of 13.8 L (Model 360; Arj Company, Iran) for a duration of 10 minutes. A few minutes after the end of nebulization process, ∼0.5 mL of the solution remained within the cup, which was the result of condensation (Fig. 1).
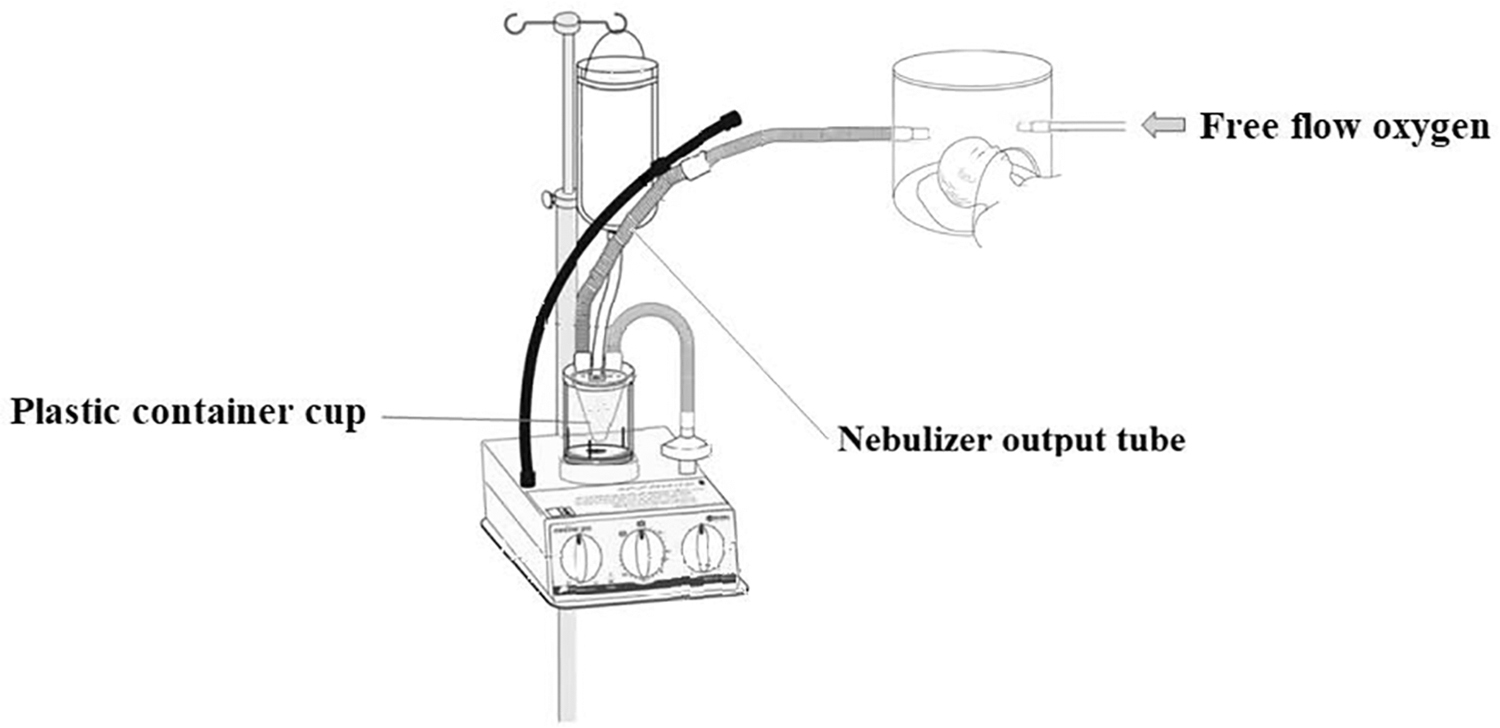
The hood and nebulizer setting.
Newborns of all three groups received routine inward care, including cardiopulmonary monitoring, intravenous dextrose water serum 10% (70 mL/kg), and empiric antibiotics therapy (Ampicillin, Amikacin). The respiratory support for TTN was applied to maintain peripheral oxygen saturation 90–95, using appropriate routs based on O2 concentration they needed. Postrandomization exit criteria were parents' withdrawal or adverse drug reactions, including tremors, hypokalemia, hypertension, tachycardia, or arrhythmia.
Outcomes
Primary safety outcomes were the mean of patients' pulse rate and presence of Jitteriness 30 minutes, 1 hour, and 4 hours after the intervention. Serum blood sugar; serum potassium; and systolic, diastolic, and mean blood pressure of patients were defined as the secondary safety outcomes. The primary efficacy outcome was the duration of tachypnea (respiratory rate >60/min) and the clinical TTN score. This scoring system employs indicators of respiratory distress, including expiratory grunting, supraclavicular retraction, subcostal retraction, cyanosis, and nasal flaring, to quantify the severity of TTN 18 (Supplementary Table S1). Other outcomes include the mean of respiratory rate, FIo2, O2 saturation, Spo2 (all measured 30 minutes, 1 hour, and 4 hours after the intervention), ABG improvement 4 hours after intervention, length of hospital stay, and level and duration of respiratory support needed during hospitalization. All outcomes were assessed by emergency ward and neonatal intensive care unit physicians and nurses who were blind about the intervention received by the patients.
Statistical methods
Sample size of 90 was calculated based on information obtained from Malakian study, considering the type one and two of 0.05 and the effect size of 40%. 19 Data are presented as mean (SD), median (IQR), and frequency (%). One-way ANOVA and repeated measures ANOVA (in the case of serial outcome assessment) were used to compare the quantitative study outcomes between groups before and after the intervention. Data analysis was performed using SPSS software version 18 with a level of statistical significance of 0.05. The intention-to-treat approach was used in the analysis.
Results
Between November 2022 and January 2023, 115 newborns with tachypnea were evaluated for eligibility criteria, and 90 cases were enrolled in the study (Fig. 2) with a mean (SD) of gestational age = 36.41 (1.12), gestational weight = 2921 (550), and 5-minute Apgar score = 8.02 (0.54). There was no withdrawal case during the study, and all cases were followed successfully until hospital discharge. No case of mortality and tracheal intubation was observed.

Study participant's flow diagram.
Assessment of baseline characteristics between three study groups, including Apgar scores, birthweight, gestational age, maternal age, and past medical history, showed no substantial difference between groups indicating that the randomization process is working properly (Table 1).
Baseline Characteristic of Newborns in Three Study Groups
Quantitative data are presented as mean (SD) (range). Categorical data are presented as frequency (%).
NVD, natural vaginal delivery; LGA, large for gestational age; SGA, small for gestational age; AGA, appropriate for gestational age; HTN, hypertension.
Safety outcome evaluation showed no adverse effect of a high single dose of salbutamol, both in 1.5 and 2.5 mg, compared with the placebo. Jitteriness was not observed in the newborns. The serum potassium and blood sugar levels were not statistically different between the three study groups. We did not detect any statistically significant change in systolic, diastolic, and mean blood pressure (Table 2). Repeated measurement of newborns' heart rates showed a significant reduction in all three groups during 4 hours after intervention (p < 0.001), but the trend of decline was not significant between the three groups (Fig. 3 and Table 3).

Repeated measured outcomes of three study groups during 4 hours postintervention.
Comparison of Safety Outcome Assessment in Three Study Groups Evaluated Before and 4 Hours After the Intervention
Quantitative data are presented as mean (SD) (range). Categorical data are presented as frequency (%).
Repeated Measure Assessment of Study Outcomes Compared During the Study and Between Study Groups
Quantitative data are presented as mean (SD) (range). Categorical data are presented as frequency (%).
Significant pairwise differences in LSD post hoc analysis.
LSD, least significant difference (test).
To evaluate the efficacy of interventions, we compared the duration of tachypnea and TTN score as the primary outcome. Both groups of newborns who received salbutamol in doses of 1.5 and 2.5 mg showed significantly lower time of tachypnea with a mean (SD) of 1.45 (1.10), 1.42 (0.93) hours compared with the placebo (mean, SD: 6.37, 4.12), whereas there was no difference between the first two groups. A similar pattern was observed in the TTN score trend during 4 hours postintervention. Seemingly, most of the other clinical and secondary outcomes were improved significantly after intervention in salbutamol groups compared with the placebo (Table 4). The median hospitalization time in the placebo group was 3 days, which was higher than the groups receiving salbutamol (both 2.5), but the difference was insignificant. Comparison between the two salbutamol-receiving groups mostly showed no differences in outcomes (Table 4). As an exception, O2 arterial pressure measured 4 hours after the intervention was significantly higher in groups that received salbutamol in the dose of 2.5 mg (mean, SD: 90.26, 9.01) compared with the intervention with a dose of 1.25 mg (mean, 84.83, 7.13) (Table 5).
Comparison of Clinical Study Outcomes Between Two Groups of Study
Quantitative data are presented as mean (SD) (range). Categorical data are presented as frequency (%). For more details about respiratory support levels please see Supplementary Table S2.
Significant pairwise differences in LSD post hoc analysis.
Comparison of Arterial Blood Gas Outcomes: Between Two Groups of Study in Baseline and 4 Hours After the Intervention
Quantitative data are presented as mean (SD) (range). Categorical data are presented as frequency (%).
significant pairwise differences in LSD post hoc analysis.
We did an additional analysis for PAo2 to adjust its baseline difference; a comparison of the amount of PaO2 difference before and after intervention showed a significant improvement in PaO2 in those who received 2.5 mg salbutamol (Mean, SD: 19.60, 8.19) compared with the 1.25 mg salbutamol and placebo recipient (Mean, SD: 16.83, 6.31) and (9.27, 5.14).
Three infants of the salbutamol-receiving groups experienced a relapse of TTN 4–6 hours after the treatments with lower severity. The TTN scores were 7–8. The first was a 39-week gestational-aged newborn, a recipient in the 1.25 mg salbutamol-receiving group, with a maternal history of diabetes and hypothyroidism, who was delivered by elective cesarean section with a gestational weight of 4.4 kg and Apgar score of 8/10. The second infant was a 35-week gestational-aged newborn with a gestational weight of 2.9 kg and urgent C/S delivery (Apgar 8/10) without reported maternal risk factor in the 2.5 mg salbutamol-receiving group. The third was a 35-week gestational-aged newborn with a gestational weight of 2.6 kg and urgent C/S delivery (Apgar 9/10) with a maternal history of diabetes in the 2.5 mg salbutamol-receiving group. In all three cases, tachypnea was resolved after receiving an additional dose of salbutamol.
Discussion
In this study, we assessed the effect of nebulized salbutamol in two high doses of 2.5 and 1.25 mg compared with the placebo on TTN treatment, which has not been done so far. The results showed that most of the clinical and paraclinical outcomes 4 hours after the treatment, including TTN clinical score, duration of tachypnea, respiratory rate, duration of oxygen therapy, the fraction of inspired oxygen, time to start breastfeeding, and time of transition to noninvasive positive pressure oxygenation are significantly improved in salbutamol groups compared with the placebo. Nevertheless, we found no statistical difference in hospitalization time between the three study groups. Although we detected better results in salbutamol with a dose of 2.5 mg regarding TTN score, improvement of tachypnea, respiratory rate, time to start breastfeeding, and time of oxygenation compared with the group treated with the 1.25 mg, the comparison was not statistically significant. A statistically significant better outcome was achieved in arterial blood O2 pressure in the recipients of 2.5 mg compared with 1.25 mg of salbutamol.
Moreover, we did not observe any adverse reaction to the study interventions in neither 2.5 mg nor 1.25 mg of salbutamol. There was no report of hypokalemia, hyperglycemia, or tachycardia regarding high dose of salbutamol.
Whereas some references suggest a 1.25–2.5 mg/2–6-hour dose of salbutamol,17,20–22 almost all studies on the effect of salbutamol on TTN management applied a nebulized dose of 0.1–0.15 m/kg.9,13,19,23,24 Ballard et al. in a survey on usage of salbutamol in practice reported that 1.25–2.5 mg nebulized salbutamol is used in 74% of university-affiliated hospitals in the United States. 20 Rocha suggests a 1.25–2.5 mg salbutamol/2–8 hours for treatment of neonatal bronchospasm and hyperkalemia. 17 The safety profile of newborns with TTN in our study is compatible with mentioned statements. No case of hypokalemia, serious tachycardia, or jitteriness was observed and a single high dose of salbutamol was well tolerated by newborns.
The current study showed an immediate effect of a single high dose of salbutamol on improving respiratory status, oxygenation indices, and breastfeeding time of newborns with TTN. This instant response to the drug was against the results of the previous studies with lower doses, which reported at least four hours' delayed success of salbutamol in control of the TTN. Kim et al. reported a reduction in respiratory rate during the hospitalization following salbutamol nebulization without any significant change in other clinical and paraclinical outcomes, including ABG or oxygenation indices. 13 The result of Babaei et al. study suggested that salbutamol can improve tachypnea and oxygenation status and anticipate the time of oral intake of newborns with TTN 4 hours after the treatment. 23 The observed effect might refer to the single high dose of the drug delivered to the patients.
The relapse of symptoms in three patients of salbutamol groups suggests a need for repeated administration of the drug. A study represented by Malakian et al. showed a significant respiratory recovery, lower hospitalization time, and faster breastfeeding after treatment with 0.1 mg/kg nebulized salbutamol in multiple doses compared with the placebo. The result showed an immediate improvement. 19 According to their result and the relapse of three patients in our study, the safety of multiple dosing of 2.5 mg salbutamol should be evaluated.
Our results did not detect a difference in hospitalization time in opposition to the result of the previous meta-analysis, 14 but this might be due to some methodical differences in conservative medical policies in the discharge of patients in our center. The other obstacle to finding the expected difference was the low precision of the study in hospitalization time assessment based on days instead of hours. It seems related to the official limitation in scheduling medical visits and laboratory reporting during admission and after complete recovery.
The current study was conducted in a triple-blind setting, which made the results highly reliable, especially regarding the subjective clinical outcomes or those that might be sensitive to surveillance bias. To the best of the authors' knowledge, high doses of salbutamol used in the study have not been used previously in the management of TTN, and the study is the pioneer. We tried to study the safety and efficacy of the drug in both clinical and paraclinical aspects and make a comprehensive conclusion. However, the study suffers from two limitations. Since we had no information about the safety of high-dose salbutamol, multiple drug dosing on newborns was against the ethical code. Considering the result of the current study, a new design for the safety evaluation of repetitive high-dose salbutamol administration can be conducted. The second limitation refers to the limited power of the study to precise measurement of hospitalization time. It was calculated by the days that patients were admitted to the hospital (and might be biased with medical visit schedules and the time needed for the official admission and discharge process). Its low variance within three groups leads to nonstatistical significance.
In third, the results can be generalized to some specific type of nebulizers and hoods, whereas there is a wide variation regarding the aerosol delivery systems. 25
In summary, our study highlights the considerable efficacy and safety of a single-dose administration of nebulized salbutamol (2.5 or 1.25 mg) for newborns with TTN in a closely monitored setting. The 100% success rate in treatment, combined with a mere 5% relapse, indicates that the majority of infants may benefit from just a single-dose treatment. Any additional interventions should be strictly administered as needed following relapse. Furthermore, upcoming clinical trials should investigate diverse dosage regimens and explore alternative nebulizer types to refine and optimize treatment approaches.
Footnotes
Acknowledgments
The authors express their gratitude to the Aliasghar Clinical Research Development Center (AACRDC) in Tehran, Iran, for their valuable assistance. Additionally, they extend sincere appreciation to NanoAlvand Company at Avicenna Tech. Park, Tehran University of Medical Sciences, Tehran, Iran, for their support in repacking the investigational medicinal product. Their thanks to Mediakaosh Co. (Knowledge based company), which has been leading in the Medication Delivery Solutions (MDS) since 2008 and is a manufacturer of smart injection pumps and nebulizers. The administration of salbutamol in this study was done through nebulizers manufactured by this company and their technical support was so useful in the trial conduct.
Authors' Contributions
F.A.C.: Conceptualization, study design, supervision, funding acquisition, and article preparation and revision. Z.V.: Clinical investigator, conceptualization, study design, study implementation, data gathering, article preparation, and documentation. Al.M.: Conceptualization, study design, study implementation, and article revision. M.T.: Study implementation, data gathering, documentation, and article revision. N.Kh.: Conceptualization and article revision. Z.S.: Documentation and article revision. Ar.M.: Study design, data management, data analysis, and article preparation. R.A.: Clinical investigator, conceptualization, study design, study implementation, data gathering, article preparation, and documentation.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
The trial is financially supported by the Iran University of Medical Sciences.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.