
Abstract
Introduction:
Receiving wrong health education from health care professionals (HCPs) might contribute to patients’ poor inhaler technique. We set out to investigate HCPs' knowledge on asthma and metered-dose inhaler technique in selected health facilities in Dar es Salaam, Tanzania.
Methods:
In a cross-sectional study done from August 2020 to February 2021, participant’s demographics were recorded. The inhaler technique was assessed using a 12-step checklist. Participants had correct inhaler technique when all the steps were performed correctly; otherwise, the technique was poor. An 18-question questionnaire for health care professional knowledge was used to assess asthma knowledge. One point was awarded to each correctly answered question, whereas a zero point was given to a wrongly answered or unanswered question. Knowledge was adequate if the score was 13/18 or higher. Chi-square was used to compare categorical data, while analysis of variance was used for comparison of mean scores for asthma knowledge and inhaler technique. A p value ≤0.05 was considered significant.
Results:
A total of 114 participants were enrolled; 57% were medical officers, and 59.6% had work experience of <5 years. The majority (53.5%) had no training on inhaler technique, and 75% had inadequate knowledge on asthma. Good asthma knowledge was associated with age ≥40 years (p = 0.039) and being a medical specialist (p = 0.002). Only 4.4% of the participants did all the steps of inhaler technique correctly.
Conclusion:
Knowledge on asthma and inhaler use technique is generally lacking among health care professionals. In-service training on asthma and inhaler demonstration should be considered for HCPs in asthma clinics.
Introduction
In the year 2019, asthma affected an estimated 262 million people and caused 455,000 deaths globally. 1 The prevalence of asthma ranges from 7% in rural areas to about 10% in urban areas of Africa. 2 In Tanzania, a precise burden of asthma is unknown. However, 12.1% and 23.1% of school-age children in a rural and an urban district, respectively, reported a wheeze in the past 1 year. 3 In 2019, an estimated 96% of asthma deaths and 84% of disability-adjusted life years occurred in low- and middle-income countries. 4 All these are happening in the midst of the presence of effective medications for long-term asthma control. 4
The burden of poor asthma control is large in Tanzania, reported in over 70% of asthma patients in Dar es Salaam, Tanzania. 5 Poor asthma control causes significant asthma morbidity and mortality 6 and is multifaceted. It can be due to poor medication adherence, presence of comorbidities such as gastroesophageal reflux disease, obesity and chronic rhinosinusitis, smoking or environmental exposure to asthma triggers and allergens, regular or overuse of short acting beta agonists,7,8 anxiety, depression,9,10 socioeconomic problems, 11 and incorrect inhaler technique.12,13
A proper inhaler technique is mandatory to ensure that inhaled medications reach the lungs 14 and to minimize side effects of oral candidiasis 15 and dysphonia 16 due to inhaled corticosteroids. Poor inhaler technique is reported in up to 80% of asthma patients. 17 Several factors are attributable to poor inhaler technique. Patient-related factors such as old age, which is accompanied by frailty, and diseases such as osteoarthritis or Parkinsonism cause difficulties in using inhalers. 4 The type of inhalational device used may also cause difficulties in performing correct inhaler technique. Some of the devices involve many steps for the patient to remember. 18 Health care workers (HCWs) who lacked training on inhaler technique during medical training may have challenges instructing their patients on correct inhaler technique. 19
Successful asthma management requires patients’ education on self-management of asthma including inhaler use. 20 Attending physicians, nurses, and pharmacists have been involved in demonstrating inhaler technique to asthma patients. Unfortunately, not all HCWs are knowledgeable of inhaler technique21–23 and thus are unprepared to teach patients. A study in the United Kingdom found only 22% of health care professionals (HCPs) demonstrated device mastery prior to training. 22 Studies from Africa found mastery of inhalational devices in 4.3% and 16% of HCPs in Ethiopia 24 and South Africa, 25 respectively. Rebuck et al. noted that HCPs’ poor knowledge on inhaler use was due to a lack of structured training in medical schools. 19
The present study aimed to investigate both asthma knowledge and inhaler technique among HCPs whose routines are caring for asthma patients in selected health care facilities in Dar es Salaam, Tanzania. It is in the belief of the authors that the findings will inform many stakeholders including academic institutions about the need for structured training on asthma and inhaler technique. We also hope the findings of the present study will emphasize the need for in-service refresher courses on asthma and inhaler technique.
Methodology
Study design, setting, and population
In a cross-sectional study, HCPs in three government-owned regional referral hospitals (Amana, Mwananyamala, and Temeke) and two health care centers (Sinza Palestina and Kigamboni) in Dar es Salaam were interviewed. In this regard, the participants of this study were HCPs in the cadres of medical specialists, medical doctors, nurses, clinical officers, intern doctors, pharmacists, and pharmacy assistants.
In the health referral system of Tanzania, the primary health care facilities are the community health services, dispensaries, and health centers, with hierarchy ascending to health centers. Patients from health centers are referred to district hospitals, which, in turn, refer patients to regional referral hospitals. Regional referral hospitals refer patients to zonal and national hospitals. 26
Sample selection and inclusion and exclusion criteria
All 3 government-owned regional referral hospitals and 2 out of 24 government-owned health centers in Dar es Salaam city 27 were conveniently selected. The convenience was derived from budgetary constraints that limited recruitment of many facilities and the intention to recruit primary HCPs from the lowest possible qualification to specialist level who were involved in asthma care.
The sample size of participants was calculated using a 16% prevalence of correct metered-dose inhaler (MDI) technique among healthcare professionals and medical students in South Africa,25 with a power of 80% at a 1.96 significant level and a standard error of 0.05. The minimum sample size calculated was 206, and it was rounded to 250. Basing on the total number of HCPs in each facility, HCPs recruited were 70, 70, 70, 20, and 20 from Mwananyamala, Amana, Temeke, Sinza, and Kigamboni, respectively.
We included HCPs working in the departments of internal medicine, pediatrics and child health, emergency medicine and facility pharmacy, and the departments dealing with asthma patients. There were no exclusion criteria.
Study procedures
Participants underwent interviews, recording demographic characteristics, years of work experience, history of having received education or training on inhaler technique, time since last training on inhaler technique, and health care cadre (physician, medical officer, clinical officer, pharmacist, pharmacy assistant, or nurse).
Participants filled in a self-administered HCPs asthma knowledge questionnaire (HQ). 28 The HQ is an 18-item questionnaire comprised of true and false questions on asthma and its treatment. The questions were universal and applicable to all HCPs and parallel global initiative for asthma guidelines. Each correctly answered question earned one point. Questions not attempted or wrongly answered earned a zero point. HQ score is therefore presented as the score of correctly answered questions out of 18. We used a score of 13 (equivalent to 72%) or higher to indicate adequate knowledge and a score of 12 or lower to indicate inadequate knowledge on asthma. Knowledge mean scores for each HCP cadre were calculated and compared across cadres.
Inhaler technique was assessed using placebo inhalers. A 12-step checklist was used to assess participants’ inhaler technique. These steps were derived from those listed from by Sanchis et al. 29 and Bartolo et al. 30 A modification on the steps was done on numbering and order to arrive at 12 steps. The steps were as follows: Step 1: shake the content well; Step 2: remove the cap, Step 3: hold inhaler upright, Step 4: tilt the head back slightly, Step 5: breath out slowly, Step 6: put the inhaler in mouth with lips tightly sealed around it, Step 7: breath in slowly and deeply through the mouth while actuating the canister once, Step 8: hold breath for 5–10 seconds, Step 9: exhale and wait for 1 minute before the next dose, Step 10: breath in slowly and deeply through the mouth and actuate the canister once, Step 11: shake the contents before the second dose, and Step 12: recap the inhaler. 30 The total score was 12, corresponding to the number of steps to be completed. A step performed correctly earned one point while incorrectly performed step or steps not performed earned a zero point. The technique was correct if all steps were correctly done and was poor if any step was done wrongly.
Data analysis
Data were analyzed using SPSS software version 23. Continuous variables were presented as means and standard deviations or medians with interquartile ranges, whereas categorical variables were presented as percentages. ANOVA was used to compare means, whereas the Mann–Whitney U test was used to compare medians. Comparison of categorical variables was performed using Chi-square tests. Statistical significance was set at p value ≤0.05.
Results
Participants’ characteristics
A total of 114 participants were enrolled in the study, 18 (15.8%) from health centers and 96 (84.2%) from regional referral hospitals. The participants were predominantly male, 63/114 (55.3%), medical doctors, 65/114 (57%), and in the age group 21–30 years, 61/114 (53.5%). About 60% of the participants (59.6%) had work experience of <5 years. The majority of the participants, 61/114 (53.5%), received no training on asthma or inhaler technique. Of those who received inhaler technique training, 53/114 (46.5%), the majority, 30/53 (60.4%), had their training more than 12 months prior to the study commencement. Just over a half of the participants, 66 (57.9%), reported to routinely demonstrate inhaler use to patients (Table 1).
Participants Characteristics (n = 114)

Asthma knowledge among HCPs
The asthma knowledge scores are shown in Figure 1. Among 114 HCPs, 28 (24.6%) participants had adequate knowledge on asthma. There was a statistically significant difference in mean scores for asthma knowledge among the health care cadres, p < 0.001. In the post hoc analysis, using medical specialists as the comparator, the mean score for asthma knowledge for medical specialists (14.5) was significantly higher than that of the medical doctors (11.31) p < 0.001, the nurses (10.36) p < 0.001, pharmacy technicians (8.4) p < 0.001, and clinical officers (10.33) p < 0.001 (Fig. 1).

Asthma knowledge scores among health care professionals. Note: Box and whisker for clinical officers is invisible because out of the six clinical officers, five had similar scores.
HCWs’ skills on inhaler use
Of 114 participants, only 5 (4.39%) performed all the steps of inhaler technique correctly. These five consisted of two medical specialists, two medical officers, and one clinical officer. No nurse or pharmacist/pharmacy technologist was able to perform all the steps correctly.
No single step of inhaler technique was correctly performed by all the participants. Additionally, some participants could not perform some steps of inhaler technique including the critical steps. Only 81/114 (71.1%) of HCPs remembered to remove the cap of the canister, 88/114 (77.2%) held the canister upright, 19/114 (16.7%) breathed out completely before taking the first puff, 9/114 (7.9%) breathed in slowly during canister actuation, and 43/114 (37.7%) held their breath for 6–10 seconds after drug inhalation (Fig. 2).

Percentage of health care workers who performed correctly the steps of inhaler use technique. Key to Figure 2: Step 1: shake the content well, Step 2: remove the cap, Step 3: hold inhaler upright, Step 4: tilt the head back slightly, Step 5: breath out slowly, Step 6: put the inhaler in mouth with lips tightly sealed around it, Step 7: breath in slowly and deeply through the mouth while actuating the canister once, Step 8: hold breath for 6–10 seconds, Step 9: exhale and wait for 1 minute before the next dose, Step 10: shake the contents before the second dose, Step 11: breath in slowly and deeply through the mouth and actuate the canister once, and Step12: recap the inhaler.
Relationship between knowledge on asthma and inhaler technique scores
Participants with adequate knowledge on asthma presented with a significantly higher median score (6) on inhaler technique compared with those with inadequate knowledge on asthma who had a median score of 5, p = 0.02 (Fig. 3).
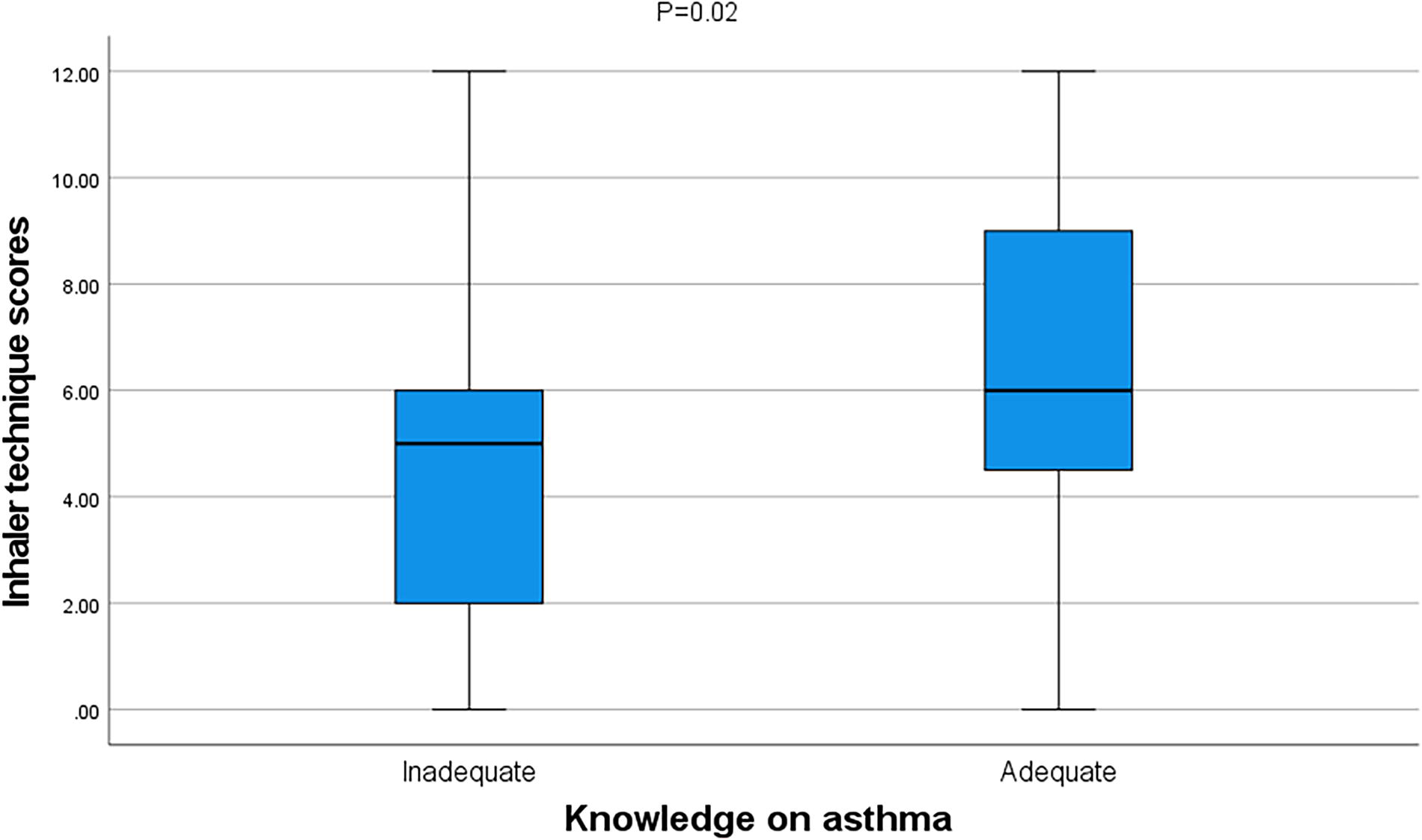
Relationship between asthma knowledge and inhaler technique scores.
Factors associated with asthma knowledge
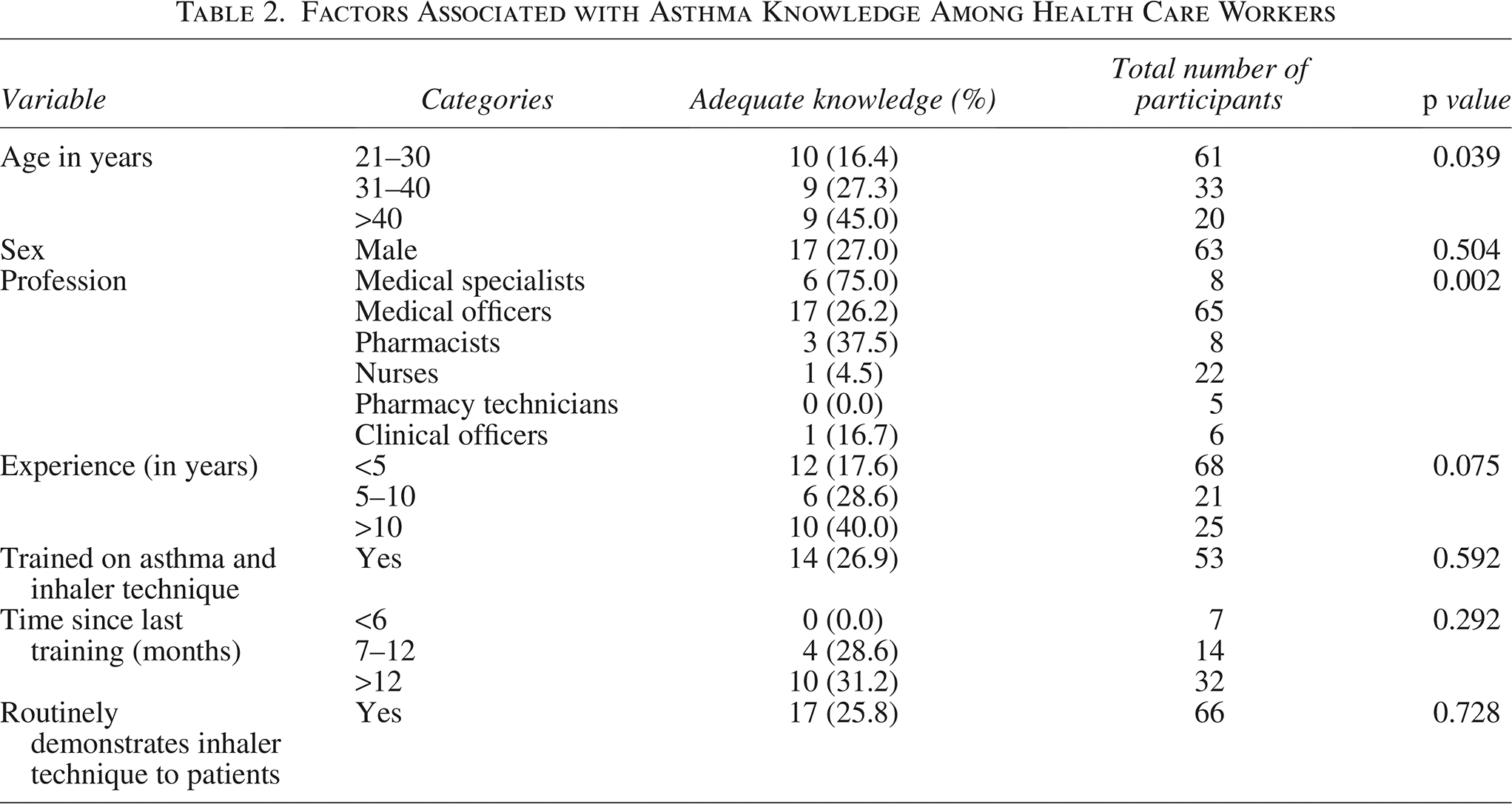
The highest proportion (45%) of HCPs who had knowledge on asthma was found in participants aged more than 40 years than were participants aged 31–40 (27.3%) or 21–30 years (16.4%) p = 0.039. Medical specialists significantly presented with the highest proportion (75%) of knowledgeable people than were pharmacists (37.5%) and nurses (4.5%) p = 0.002. There was no significant difference in asthma knowledge with regard to participants’ sex, years of experience, previous training on inhaler use, or routine demonstration of inhaler use to patients, all with p value >0.05 (Table 2).
Factors Associated with Asthma Knowledge Among Health Care Workers
Inhaler technique mean scores among HCPs
Figure 4 shows scores on inhaler skills among different healthcare professional (HCP) cadres. Medical specialists scored the highest (mean score 10 ± 1.5) followed by pharmacists (mean score 7.4 ± 2.1), whereas the nurses scored the lowest (mean score 3 ± 2.1) (Fig. 4).
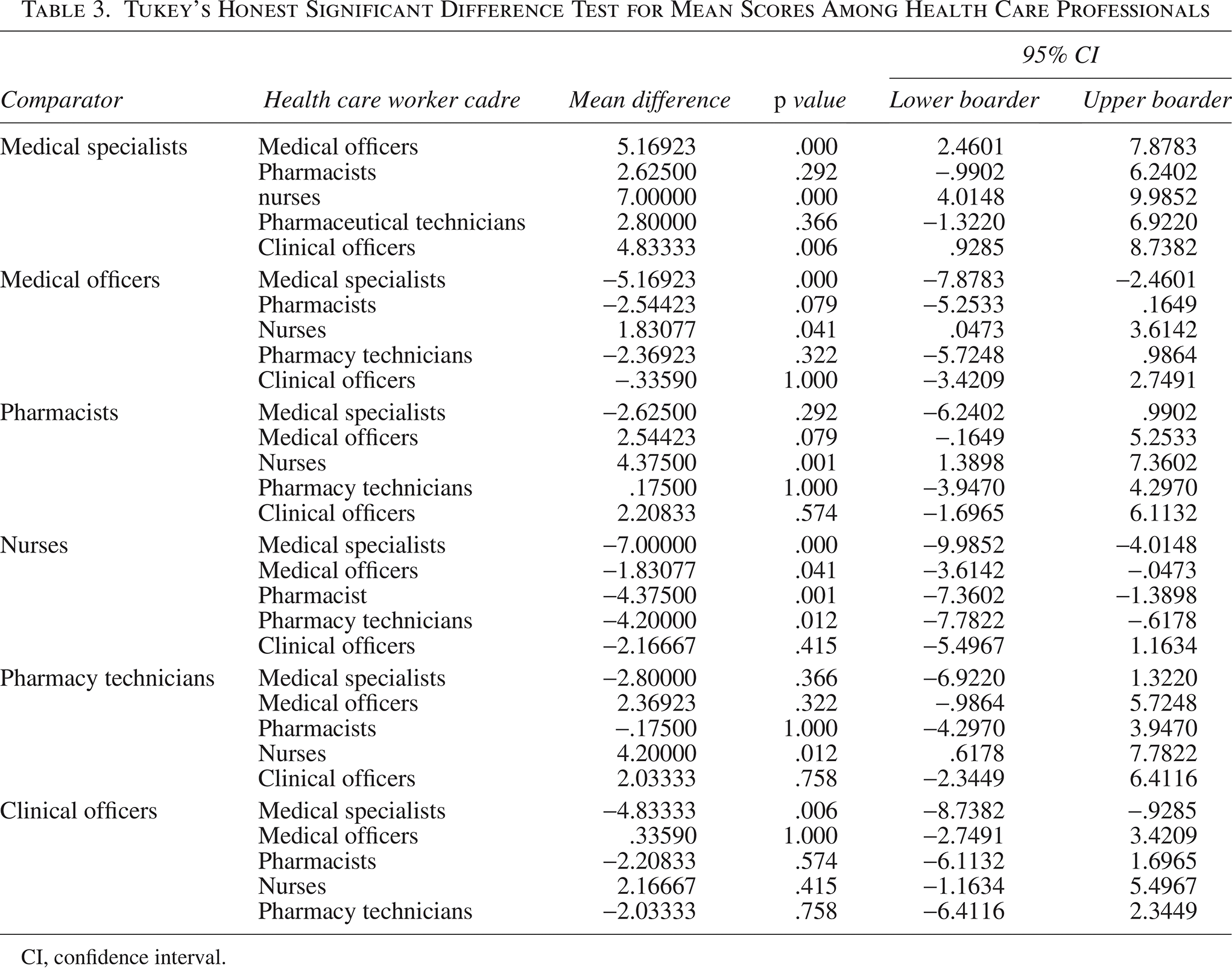
There was a statistically significant difference in mean scores for inhaler technique between HCP cadres, p < 0.001. In the post hoc analysis with medical specialists as the comparator, it was found that medical specialists’ mean scores for inhaler technique were significantly higher than those for medical doctors (p < 0.001) and nurses (p < 0.001). Comparison of medical specialists with other cadres did not show any significant difference (Table 3).
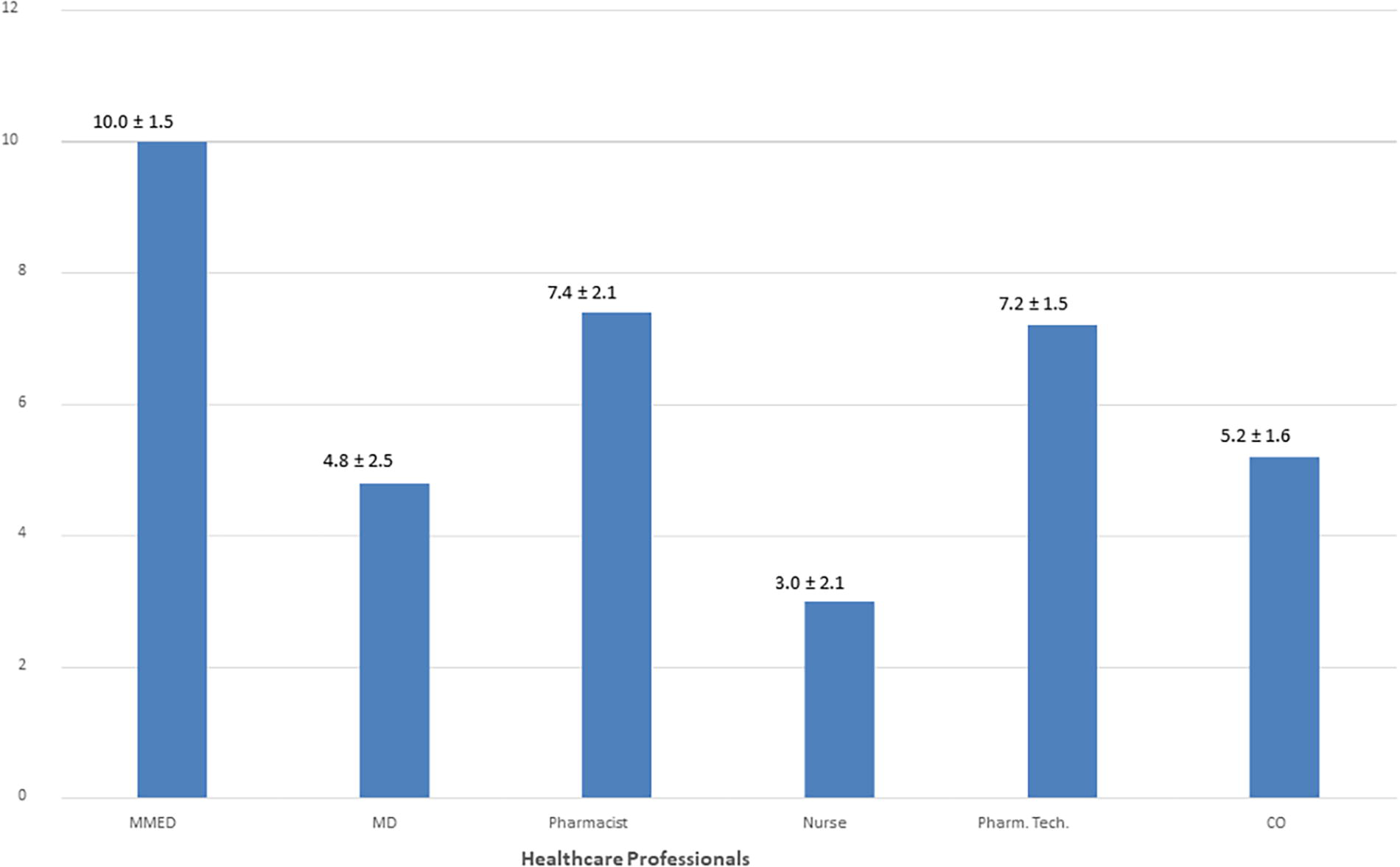
Comparison of inhaler use technique mean scores among health care professionals. Key to Figure 4: MMED, medical specialists; MD, general practitioners (medical officers); Pharm.Tech, pharmacy technicians; CO, clinical officers.
Tukey’s Honest Significant Difference Test for Mean Scores Among Health Care Professionals
CI, confidence interval.
Discussion
The findings of the present study showed that only 25% of HCPs had adequate knowledge on asthma, and about 5% of HCPs demonstrated good inhaler technique. Doctors of all cadres significantly scored the highest mean scores for asthma knowledge. Age 40 years or older and being a medical specialist were associated with adequate asthma knowledge.
Inadequate asthma knowledge among HCPs is partly explained by lack of on-job training on asthma, as was reported by more than half of the participants who never received any training on asthma and/or inhaler technique. In the present study, HCPs in the age group of 21–30, which covers most of the new employees in the health care field, had the least proportion of participants with adequate asthma knowledge, implying a lack of experience and/or inadequate training in medical schools. Poor asthma knowledge was also reported in Ghana among newly qualified doctors. 31 Best scores among medical specialists can be attributed to additional training in their postgraduate training. In the present study, nurses presented with poor asthma knowledge and inhaler technique. This poor performance among nurses is alarming, as most doctors rely on nurses for inhaler technique demonstration to patients. We understand that nurses do not receive extensive training on asthma management while in nursing colleges; however, it is the expectation of everyone that a nurse caring for asthma patients on a daily basis be well informed of asthma and its management. It has been reported that understaffing might lead to the involvement of nurses in many other tasks that are not directly based on patient management, 32 a situation that might lead to a lack of knowledge and skills on patient care. Similar findings were reported in Jordan, whereby medical specialists had the best scores for inhaler technique, whereas the nurses recorded poor performance. 23
In the present study, the proportion of HCPs with correct inhaler technique was alarmingly low, with only 5% of HCPs performing inhaler technique correctly. This finding is comparable to findings in Jordan 23 and Nepal, 33 whereby inhaler technique scores were very low among HCPs. In Nepal, none of the HCPs could perform all the steps correctly. 33 In the present study, the medical specialists had the best scores for inhaler technique. This is partly explained by years of experience and having received extra education during postgraduate training. Nurses’ poor scores have been reported elsewhere despite the presence of high confidence with inhaler device education. 34 Nurses should be equipped with correct inhaler techniques, as they routinely demonstrate the technique to patients.
For proper delivery of the medication to the lower respiratory systems, all the steps have to be performed correctly. However, Step 2 (removal of canister cap) is a very critical step, as failure to do so leads to no drug delivery at all. In the present study, about 29% of HCPs omitted Step 2, making the rest of the steps useless. Steps 6–8 need hand–mouth coordination to ensure maximal drug delivery to the lungs, thus considering critical steps. In the present study, only about 8% of the participants could perform Step 7 correctly, i.e., they did breathe in slowly while actuating the canister. Likewise, only over a third of HCWs performed Step 8 (holding breath for 5–10 seconds after canister delivering the drug). Omitting or wrongly performing Steps 2 or 6–8 leads to no drug delivery or suboptimal dosage, respectively, even when all other steps were correctly performed. Errors in performing Steps 6–8 have been reported in other studies too.23,25,33 A study among patients with chronic obstructive pulmonary disease reported severe exacerbation in patients who poorly performed these critical steps using a dry powder inhaler. 35
In the present study, more than half of the participants reported not having ever received any training on asthma despite caring for asthma patients daily. As knowledge mean scores were higher among those who received training, it is prudent that all staff caring for asthma receive an on-job training on asthma and asthma care. The benefit of training is witnessed in the study in Jordan where posttraining assessment and 4 months posttraining follow-up noted that those who attended a training workshop (n = 48) scored significantly higher mean scores for all devices (score = 7.64) than nonattendees (n = 81, score = 5.99, p < 0.001).
Study limitations
This study was conducted in public health facilities only, thus limiting its generalizability to HCWs in the private facilities.
Only pMDI technique was assessed, as this is the most available device in the country; thus, the study is not generalizable to other inhalational devices.
The present study used a 12-step checklist to assess inhaler technique. It is important to note that there are also 8- and 10-step checklists; thus, some participants’ knowledgeable of these other checklists might have been wrongly labeled not as knowledgeable of the technique, as they might have performed steps short of 12. However, the differences in the checklists were not critical, as all the steps necessary to ensure medication delivery and adequacy are included in these other checklists.
Different training packages and durations of training might have contributed to the differences observed in asthma knowledge and inhaler technique among doctors, nurses, and pharmacists.
Conclusion
Knowledge on asthma is generally poor among HCPs in Dar es Salaam. HCPs' advanced age and postgraduate training were positively associated with adequate asthma knowledge. In the absence of the placebo inhalers for patients’ training on inhaler technique, only about five (mostly being doctors) out of a hundred health professionals could perform all the steps of inhaler technique correctly. In-service training of HCPs and making placebo inhalers available in asthma clinics might improve asthma knowledge and inhaler technique among HCPs. For sustainable knowledge, medical schools should consider the need for structured training on asthma and inhaler technique for the students.
Authors’ Contributions
G.A.S. and A.W. conceived the study. A.W. and M.K. supervised data collection. G.A.S. and A.W. analyzed the data. G.A.S. wrote the first draft of the article. All authors read and approved the final draft of the article.
Footnotes
Acknowledgments
The authors would like to thank the facilities and health care professionals who consented to this study. This publication originates from a dissertation work by A.A., which was submitted in the year 2021 as a partial fulfillment for her residence in Internal Medicine at the Muhimbili University of Health and Allied Sciences in Dar es Salaam, Tanzania.
Author Disclosure Statement
The authors declare no competing interest.
Funding Information
This study received no funding.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Issues
Approval to conduct the study was obtained from MUHAS Ethical Review Board (IRB no. MUHAS-REC-07-2020). Permission to conduct the study in the selected health facilities was obtained from district medical officers in the districts the health facilities were located. Each participant signed and provided a written informed consent before they were enrolled in the study. The study was anonymous. Health care professionals with incorrect technique were instructed on correct MDI technique.