
Abstract
Background:
It remains challenging to quantify lung pharmacokinetics (PK) of a drug administered and targeted to act in the lung. Exhaled breath particles (PEx), which are generated when collapsed distal airways reopen during inhalation, offer a noninvasive way to access undiluted epithelial lining fluid (ELF). Therefore, it was the aim of this study to investigate whether PK data can be derived from PEx.
Methods:
Six healthy volunteers received either an inhaled dose (400 µg) or an oral dose (8 mg) of salbutamol in a randomized, crossover design with 7-day washout between treatments. PEx were collected before and at nine time points after dosing (0–315 minutes [min]). Following each 15 min PEx sampling period, nasosorption and plasma samples were collected. Salbutamol was quantified by liquid chromatography-mass spectrometry.
Results:
After oral delivery and inhalation, salbutamol PK profiles could be obtained for plasma and nasal samples. In PEx samples, a PK profile could be obtained in 5 of 6 participants after inhalation, but the salbutamol concentration was often at or below detection limit after oral intake. After inhaled administration we found higher salbutamol concentrations in PEx as compared with nasal and plasma samples.
Conclusion:
This study provides proof of principle that PEx samples can be used to quantify drug levels in ELF.
Introduction
It remains challenging to quantify lung pharmacokinetics (PK) for drugs targeted to act in the lung, as PK data in clinical trials are generally limited to plasma analysis. We have shown recently that lung spatial PK studies are feasible with invasive collection methods, when PK profiles are derived by combining the data of several individuals. 1 While this is an important step forward, there remains a need to find novel methods that could help to avoid invasive procedures and have the feasibility to be used in early-phase clinical trials during clinical drug development.
There appears to be a broad consensus in the research community that exhaled breath particles (PEx) are generated when collapsed small airways (∼14th–17th generation, ∼0.5 mm diameter) reopen during inhalation.2–4 PEx therefore most likely represent epithelial lining fluid (ELF) from the very peripheral lung. Furthermore, their mode of generation makes contamination of sampled material with secretions from larger airways unlikely. Compared with bronchoalveolar lavage (BAL), which collects ELF down from the wedge position in the 4th–5th generation of airways, 5 PEx therefore could be a unique way to specifically investigate the peripheral lung. However, the major advantage of PEx analysis is its noninvasive nature as method of collection, which allows to assess lung PK in individuals at repeated short interval time points. Although only very small amounts of PEx are emitted during each exhalation, specific breathing maneuvers generally allow to collect sufficient amounts of material during a sampling period of 15 minutes (min). 6 It is also important to note, that in opposite to BAL, there is no unknown and variable dilution factor as PEx is considered to represent undiluted ELF.
The aim of this clinical study was to investigate the hypothesis that exhaled breath particle analysis can serve as the novel noninvasive tool for pulmonary PK analysis. In this pilot study, we included a small number of healthy volunteers and used salbutamol as a model for lung-targeted drugs. To create PK profiles after administration through two different routes, the drug was administered both orally and by inhalation in a randomized cross-over design and PEx data were compared with standard plasma. In addition, we also collected nasosorption samples to serve as control from the upper respiratory tract.
Methods
Materials
Salbutamol metered-dose inhaler (Sultanol® Dosier-Aerosol 100 µg/dose) was purchased from Glaxo Smith Kline GmbH & Co. KG (München, Germany) and salbutamol for oral intake (Volmac® 8 mg retard) from Dexcel® Pharma GmbH (Alzenau, Germany). For the collection of breath particles, we used the PExA® instrument (PExA AB, Gothenburg, Sweden). PEx were collected on Teflon membranes (0.45 μm poplytetrafluorethylene membranes 25mm, Merck, Germany). For the nasosorption, we used the nasal sampling device NasosorptionTM FX·i (Hunt Developments, Midhurst, United Kingdom). Blood samples were collected in 2,6 mL S-Monovette® EDTA K3E tubes (Sarstedt AG & Co. KG, Nümbrecht, Germany).
Study design
Six healthy volunteers were included into the study to assess eligibility. At screening (up to 28 days prior to the first visit), medical history and basic demographics were assessed, and a physical examination was performed, including spirometry. Then a baseline PEx sample was collected. Participants were enrolled if they were able to emit at least 200 ng PEx during a 15 min time interval.
Enrolled participants underwent two further visits separated by a minimum of 7 (+14) days. After collecting a pre-dose sample of plasma, PEx and nasosorption, each participant was dosed with salbutamol (time point 0). Each participant was randomized to receive salbutamol either orally (8 mg) or via inhalation (400 µg) on the respective two dosing visits.
Directly after dosing, a plasma sample was taken and then the first PEx sampling started. Samples were then taken at pre-defined time points after dosing: 20 min, 40 min, 60 min, 120 min, 180 min, 240 min, 270 min, and 300 min. PEx samples were collected first, each over a time period of 15 min, followed by blood sampling and the nasosorption procedure.
The investigator and study-participant were both unblinded because PK drug levels as the primary endpoint are robust to bias. The study was completed after a follow-up phone call.
The study was approved by the local ethics committee (Hannover Medical School), and all participants gave their written informed consent after being fully informed about the study and prior to study procedures. The study was registered with clinicaltrials.gov (NCT04914273) and conducted in accordance with the Declaration of Helsinki and the International Council for Harmonisation Harmonised Tripartite Guideline for Good Clinical Practice (CPMP/ICH/135/95).
Procedures and Analysis
Participants were asked to perform repetitive breathing maneuvers, 7 such as deep exhalations and breath hold, which generally allow to collect sufficient amounts of PEx during a sampling period of 15 min. Nasal lining fluid samples were taken using nasosorption devices, which consist of an absorptive surface placed in direct contact with nasal lining fluid for 30 seconds. Nasosorption is considered minimally invasive sampling method.8,9 Sample handling of PEx samples have been described in detail previously. 6 Plasma, nasal lining fluid, and PEx samples were first extracted using a methanol/acetic acid (0.2%) solution including a stable-isotope labelled internal salbutamol standard. Following evaporation samples were redissolved in 50% methanol containing 0.2% acetic acid. Salbutamol was quantified by liquid chromatography-mass spectrometry as recently reported. 1 The detection limit of salbutamol in plasma samples was 0.041 nM and 0.004 nM in nasal lining fluid samples. In PEx samples, the detection limit was 0.002 nM. Each sample was corrected for the mass of nasosorption and PEx samples. Estimations of the PEx mass are based on the data of the optical particle counter (Grimm Aerosol, Germany), which is part of the PExA instrument.
Results
The study was conducted from June to July 2021 at Fraunhofer ITEM, Hannover, Germany. Six healthy, nonsmoking (<1 pack year, nonsmoker at least 1 year) volunteers were enrolled for this study (table 1). Participants had to be able to emit >200 ng of particles within 15 min of sampling in the screening visit. The median (interquartile range, IQR) emission of all participants in the measurements prior to treatment was 205.9 (15.9) ng.
Demographics
BMI, body mass index; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
The median (IQR) amount of PEx in all collected samples was 202.8 (149.5; 211.0) ng. Some volunteer participants were not able to maintain the 200 ng throughout the study (Supplementary table S1 and Supplementary figure S4, online supplement). High-emitting subjects needed fewer breathing maneuvers to accumulate the desired sampling weight of 200 ng. The total expiratory volume during sampling was positively correlated with the number of breathing maneuvers, and the number of breathing maneuvers was negatively correlated with sampling weight. As shown by figure S4 (online supplement), the profiles for the collected PEx amount and the required breathing maneuvers show some inter- and intraindividual variation. The median nasal sample weight (range) was 0.043 (0.032; 0.059) mg, individual data is provided in Supplementary table S2 in the online supplement.
The PK profiles were measurable in plasma samples both after inhaled and oral administration of salbutamol (Fig. 1). Oral intake of salbutamol showed a delayed increase in plasma concentrations compared with salbutamol inhalation but reached overall higher plasma levels. Interindividual differences appeared to be smaller after inhalation of the drug. The PK profiles in nasosorption samples were similar to those in plasma (Fig. 1). The concentrations were corrected with the respective sample weight. The profiles and concentration ranges (in nM) of plasma and nasal samples were comparable. Participant 114 showed a delayed increase after oral intake both in plasma and in nasal secretions. Individual data is provided in the online supplement (Supplementary figure S1, figure S2).
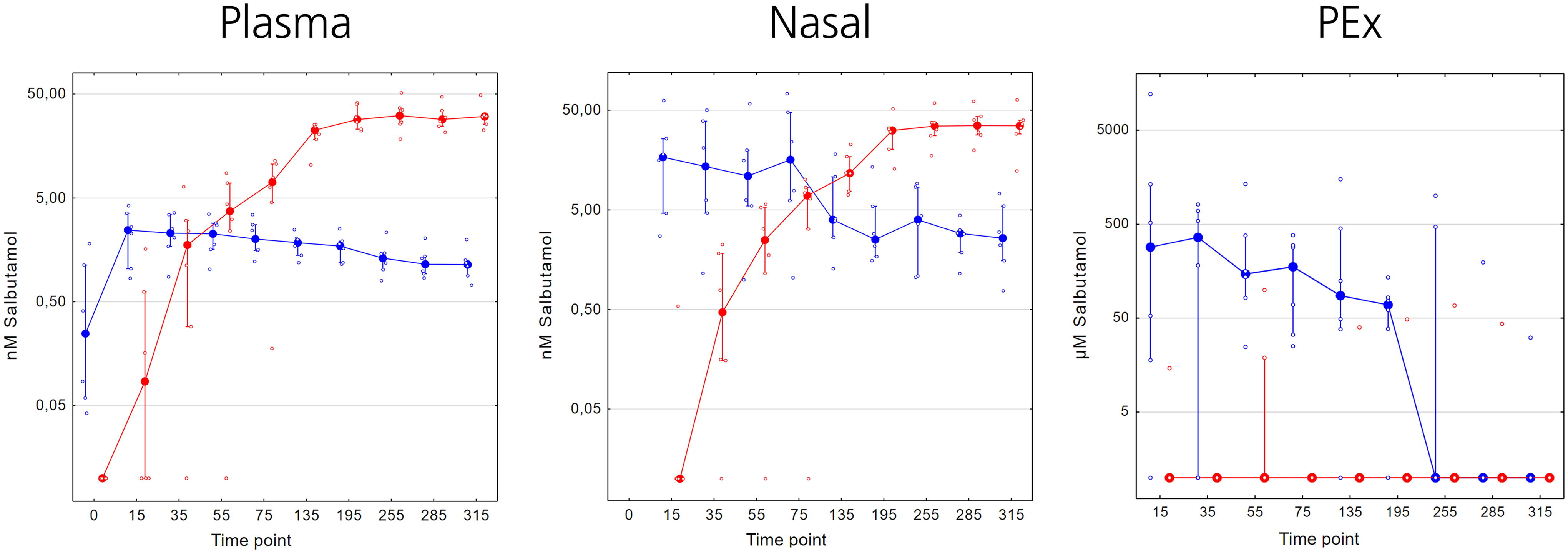
Pharmacokinetics of inhaled (blue) and orally (red) administered salbutamol in plasma (left), nasal lining fluid (middle), and in exhaled breath particles (PEx, right). The samples were collected over a time period of 315 minutes. Median (IQR) molar concentrations are displayed on a log scale axis. The respective individual data is shown as dots. PK, Pharmacokinetics.
In PEx samples, a PK profile could be obtained in five of six participants after inhalation of salbutamol. After oral intake, the PEx salbutamol concentration was generally at or below detection limit (Fig. 1). Interestingly and as shown in Fig.1, the concentrations of salbutamol in PEx were much higher (IQR of the samples: 46–381 µM) as compared with the concentration detected in plasma (1–19 nM) and nasal secretions (2–23 nM), respectively. Individual data is provided in Supplementary figure S3 (online supplement).
Discussion
This study provides proof of principle that PEx samples can be used to quantify drug levels in ELF, in particular after inhaled administration of a model drug like salbutamol. To achieve this goal, the availability of highly sensitive detection methods for the respective drugs is a prerequisite, and it is important to include participants with a sufficiently high PEx emission.
Systemic PK of salbutamol in our study was very well in line with published data.10,11 Compared to our previous study, the administered dose of inhaled salbutamol was doubled from 200 µg to 400 µg to increase the chance of detecting drug levels in PEx. While the PK profile was comparable, the mean peak plasma level (Cmax) was only slightly higher at 35 min as compared with our previous study. 1 In addition, we included treatment with oral salbutamol (8 mg) as a control. The profiles were nearly identical with previous work, and the mean peak plasma concentration of 32 nM at 255 min after dosing was very similar to our previously reported peak concentration of 29.5 nM at 240 min. 1
As expected, nasal concentrations were in the same nanomolar concentration range as the plasma samples. Both nasal and plasma samples showed the increasing concentration profile over time after oral intake and the decline over time after salbutamol inhalation. In line with this expected close relationship, we observed the same delayed increase in nasal and plasma sample concentrations after oral intake for participant 114.
In contrast to our previous study, we were able to detect salbutamol in most PEx samples after inhaled administration. We consider the fact that we only included participants known to be “high emitters” of PEx to be one of the reasons. A “high emitter” was defined as a person able to emit more than 200 ng of PEx within the 15 min collection interval in the screening visit. It is known from previous studies 6 that this characteristic is fairly reproducible over time, therefore it could be expected that a person that shows a high emission during screening will also do so during the study. Although not all participants were able to maintain this high level throughout all collections (Supplementary table S1 and Supplementary figure S4 in the online supplement), we were able to achieve a much higher overall level of emission compared to our previous study. 1 As all salbutamol levels were adjusted according to the respective weight of the PEx sample, we consider an influence of varying samples weights on the results as neglectable.
We also improved the salbutamol extraction process of the PEx samples by reducing the dilution factor. This resulted in more samples to exceed the detection limit of the analysis method. Here, it is important to consider the fact that the extremely small amount of total material of PEx available, still requires a larger dilution for the sample to be analyzed as compared with nasal and plasma samples. This results in much more PEx samples being below the limit of detection, despite the fact that the overall concentration of salbutamol in PEx was much higher as compared with nasal and plasma samples.
Finally, the higher administered dose of inhaled salbutamol as compared to the previous study 1 is likely to have contributed to the increased number of PEx samples with levels above the detection limit. Especially after inhalation, it appears plausible that PEx samples from the lung are more affected by the dose increase as compared with plasma samples which, as outlined above, showed only slightly increased peak plasma concentrations compared to our previous study.
We would like to emphasize that all salbutamol concentrations were converted to provide the actual concentration in the respective matrix. By this way, the concentrations between plasma, nasal, and PEx samples are comparable. As nasal secretions are in close exchange with plasma concentrations and resemble an aqueous matrix rich in proteins, it was expected to find a similar concentration range in these two sample types.
PEx are considered as undiluted ELF and are therefore rich in phospholipids and most likely without substantial contamination of secretions from larger airways.12,13 Two major observations were made in this study. First, the concentration of salbutamol in PEx after inhalation was found much higher (in the µM range) as compared with plasma and nasal samples. Second, most samples after oral administration were below the limit of detection. The fact that the few samples with detectable drug levels were found in later collections after oral intake is in line with the increasing concentrations found in nasal and plasma samples.
While the overall decline in salbutamol concentration after inhaled intake appears to be comparable to nasal and plasma samples, it also showed a larger variability in PEx. We assume that the more complicated collection and analysis process for PEx is responsible for this observation. With respect to the much higher concentration as compared with plasma and nasal samples, we can only speculate about potential reasons. As PEx are thought to be solely generated in the distal airways, the salbutamol aerosol particles might have preferentially reached these small airways.
This study provides first evidence that the PEx methodology is suited to be used as noninvasive tool to study PK levels in ELF. However, we acknowledge that our study has some limitations. The sample size was small; however, comparable to group size in other PK studies. We only used one drug candidate, which we thought to be sufficient for hypothesis testing, but it does not allow to draw general conclusions with respect to the suitability of PEx analysis for other drugs, in particular non-small molecules such as biologics. It is also important to consider the fact that high PEx emitters are needed to assure sufficient amounts of PEx for quantification. For future studies with novel compounds, it will also be of great importance to have very sensitive analysis methods available to be able to analyse the low amount of PEx samples. Finally, this was a single center study. Therefore, it is difficult to conclude that the method can be used in multicenter settings because expert know-how and standardization will be required prior to bringing such a study into the general early-phase drug development environment.
Conclusion
This study has provided the proof that repetitive PEx sampling is feasible to assess pharmacokinetics of drugs aimed to target the lung.
Footnotes
Acknowledgments
The authors thank all volunteers for their study participation and the site staff for their diligent study conduct. This investigator-driven study was supported by Fraunhofer internal grants and the German Center for Lung Research. The manuscript is based upon a previously published ERS International Congress abstract (Holz O, Sadiq MW, Nehrig J, et al. Assessing human lung pharmacokinetics using exhaled breath particles [PEx]. ERJ 2022; 60: 2960. DOI: 10.1183/13993003.congress-2022.2960).
Authors’ Contributions
O.H., M.W.S., and J.M.H. designed the study. C.G., N.S., S.S., and A.L. contributed to data acquisition. O.H., M.W.S., S.S., and A.L. contributed to data analysis. All authors contributed to interpretation of results. O.H. drafted the manuscript. All authors critically reviewed the manuscript and gave their final approval for submission.
Author Disclosure Statement
O.H., C.G., N.S. have no conflicts of interest to declare. M.W.S., S.S., and A.L. are employees of AstraZeneca, Sweden. J.M.H. reports grants to his institution for early-phase clinical study conduct from AltamiraPharma GmbH, Astellas Pharma GmbH, AstraZeneca AB, Bayer AG, Beiersdorf AG, Boehringer Ingelheim Pharma GmbH & Co. KG, CSL Behring GmbH, Desitin Arzneimittel GmbH, EpiEndo Pharmaceuticals, F. Hoffmann-La Roche AG, Genentech, Inc., GlaxoSmithKline GmbH & Co. KG, Janssen Pharmaceutical NV, M&P Pharma AG, Novartis AG, ReAlta Life Sciences, Sanofi-Aventis Deutschland GmbH, and UCB Pharma GmbH as well as personal grants for consultancy and board activities from Boehringer Ingelheim Pharma GmbH & Co. KG, CSL Behring GmbH, Cureteq AG, Merck & Co, Inc., Nocion, and Roche.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.