
Abstract
Background:
Extrathoracic deposition is a large source of in vivo variability in dosing for pressurized metered dose inhaler (pMDI) aerosols. A majority of previous studies have focused on only total extrathoracic deposition for pMDIs. The present work evaluates regional deposition within the extrathoracic region to better understand the impact of actuator orifice diameter and inhalation flow rate on extrathoracic deposition of a suspension pMDI formulation of epinephrine.
Methods:
Regional deposition of a commercially available HFA (hydrofluoroalkane) suspension pMDI formulation of epinephrine was evaluated using plastic and metal versions of the newly developed sectioned Alberta Idealized Throat (s-AIT), divided into analogs of the oral cavity, the pharynx/larynx, and the upper trachea. Influences of actuator orifice diameter and inhaler insertion angle on regional extrathoracic deposition were evaluated in the plastic s-AIT at a 30 L/min flow rate, followed by additional testing in the metal s-AIT to evaluate effects across a range of flow rates (from 10 to 100 L/min).
Results:
Actuator orifice was found to strongly influence regional extrathoracic deposition of a commercially available epinephrine HFA suspension pMDI aerosol, with smaller actuator orifices yielding reduced oral cavity deposition and increased distal-filter (in vitro lung) deposition in both the plastic and metal s-AIT. Inhalation flow rate was found to strongly influence deposition in the metal s-AIT, with higher flow rates associated with reduced oral cavity deposition, increased pharynx/larynx deposition, and increased upper trachea deposition. Smaller orifices showed less variability in results as a function of inhaler insertion angle.
Conclusions:
Actuator orifice diameter (spanning 0.22–0.42 mm) can strongly influence regional deposition of an HFA epinephrine suspension pMDI aerosol within the extrathoracic region. Smaller actuator orifices may provide reduced oral cavity deposition and increased delivery to the lungs. Smaller actuator orifices may also reduce variability in extrathoracic deposition that is associated with patient use aspects such as inhaler insertion angle.
Introduction
Pressurized metered dose inhalers (pMDIs) are perhaps the most widely recognized type of inhaler with a history of use spanning back to their invention in the 1950s. 1 The fundamental function of a pMDI is to generate respirable particles from a metered volume of formulation containing therapeutic agent that is suspended or dissolved in propellant. Actuation of the pMDI exposes a metered volume of formulation to ambient pressure, causing flash vaporization of propellant, rapid expansion of the metered volume, and expulsion through the pMDI actuator orifice. 2 Subsequently formed droplets undergo additional evaporative size changes as they mix with ambient air and are inhaled by the patient. 3
Previous works have investigated the influence of pMDI actuator orifice size and design on various aspects of inhaler performance.4–8 Gabrio et al. 4 evaluated spray force, spray temperature, plume duration, and in vitro extrathoracic deposition for a number of commercial and prototype pMDIs using actuators with known orifice diameters. Spray force increased significantly with increasing actuator orifice diameter, while in vitro extrathoracic deposition increased significantly as the orifice diameter increased from their smallest tested size of 0.29–0.40 mm. Smyth et al. 5 evaluated the influence of orifice diameter, jet length, and sump depth on spray pattern and volume median diameters generated from solution pMDIs. Significant differences in spray pattern axis measurements including elliptical ratio and major and minor axis lengths were associated with differences in sump depth and jet length, but generally not with orifice diameter—an exception was observed for inclination angle of the spray pattern. A companion article by the same group using a wider range of orifice diameters, however, found a nonlinear relation between orifice diameter and spray pattern, complicating the development of a predictive correlation applicable across the full range of tested orifice diameters. 6 Lewis et al. 7 in a unique exploratory study on the influence of actuator orifice diameter and geometric design on a solution-based HFA formulation containing ethanol, found that smaller orifice diameters were associated with longer plume durations and higher ex-valve fine particle fractions. More recently, Moraga-Espinoza et al. 8 used a novel sectioned version of the U.S. Pharmacopeia (USP) Induction Portto evaluate deposition in regions of interest of the USP Induction Port for three commercial pMDI products spanning a wide range of orifice diameters, but did not directly analyze the impact of orifice size on their results. Chen et al. 9 explored the influence of nozzle geometry, nozzle material, and formulation on pMDI plume geometry, but used only a single orifice diameter (0.3 mm), such that the influence of this factor was similarly not explored.
The above works broadly suggest that actuator orifice design can influence pMDI spray characteristics, with some authors suggesting that this may influence total extrathoracic deposition in vivo. 4 Extrathoracic deposition is well-recognized as a major cause of variability in pulmonary delivery for inhaled pharmaceutical aerosols. 10 While numerous studies have evaluated total extrathoracic deposition of pMDI aerosols through in vivo imaging studies, in silico computational models, and in vitro experimentation,3,11 considerably less is known about regional deposition behavior of pMDI aerosols within the extrathoracic region itself. Regionality of extrathoracic deposition can conceivably influence the development of deleterious side effects including dysphonia, oral candidiasis, and pharyngitis12–14 as well as more subjective experiences including taste (bitterness) and temperature (“cold freon effect”)15,16 that can influence patient adherence and interfere with correct inhaler use technique. As such, there exists a gap in our understanding of pMDI performance that may have important implications for the next generation of inhaled therapies.
In the present work, we describe a comprehensive in vitro study to explore the hypothesis that pMDI actuator orifice diameter influences regional extrathoracic deposition of a suspension pMDI formulation. We utilized a new sectioned version of the Alberta Idealized Throat (denoted the sectioned Alberta Idealized Throat or s-AIT) to evaluate extrathoracic deposition in terms of dose depositing in analogs of (1) the oral cavity, (2) the oropharynx, hypopharynx and larynx (referred to herein as pharynx/larynx for simplicity), and (3) the upper trachea.
Materials and Methods
Previous works from our group have focused on the influence of factors including environmental conditions (temperature, humidity) and use conditions (insertion angle of the inhaler relative to the mouth opening) on total in vitro extrathoracic deposition from pMDIs in the AIT.17,18 The present work provides an extension to these methods to allow for examinations of regional extrathoracic deposition from pMDIs in vitro, with a primary aim of investigating effects of orifice diameter on deposition of a commercially available suspension formulation of epinephrine.
Development of the s-AIT
The AIT has been previously described in the literature. 19 This geometry was purposefully designed as an idealized geometrical model of the oral extrathoracic airways using a combination of medical scan data, observation of living subjects, and archival information. Containing analogs of the oral cavity (including teeth, tongue, and hard palette), pharynx, larynx (including epiglottis and glottis), and upper trachea, the AIT has been shown to replicate average extrathoracic deposition from various pharmaceutical inhalers in adults.20–22
The s-AIT was designed using the AIT as a template. Inner surfaces of the AIT were delineated into sections corresponding to (1) oral cavity, (2) pharynx/larynx, and (3) the upper trachea in a manner consistent with previous works.23,24 The boundary between the oral cavity and the pharynx/larynx was selected as an approximation of the location of the oropharyngeal isthmus, while the boundary between the pharynx/larynx and the upper trachea was placed 20 mm below the idealized analogue of the glottis. External surfaces of the AIT were modified as necessary to facilitate ease of manufacturing and assembly/disassembly during use.
A prototype of the s-AIT was 3D-printed out of a rigid plastic (PolyJet VeroGrey photopolymer, using an Objet Eden 350V printer). Rapid prototyping using polymers provides an inexpensive means for developing complex three-dimensional geometries, but perceived drawbacks of plastic geometries for inhaled pharmaceutical aerosols testing include solvent compatibility, durability, and concerns related to the use of electrically insulating materials in mouth-throat models. 25 After performing initial tests in the plastic s-AIT, we opted to construct a metal version of the s-AIT to align with recommendations that components used for in vitro characterization of pharmaceutical aerosols be manufactured from electrically conductive materials. 25 A metal version of the s-AIT was prototyped in stainless steel via laser powder bed fusion (Linear AMS, Livonia, MI) with postprototyping machining and finishing performed by the University of Alberta Mechanical Engineering Machine Shop. Slight modifications of the initial plastic s-AIT design were incorporated into the metal version to facilitate manufacturability and ease of assembly/disassembly—namely, the delineation between the oral cavity and pharynx/larynx was shifted to accommodate feasibility in machining of the mating surface between these sections. Schematics of the plastic s-AIT and metal s-AIT are shown in Figure 1, with relative proportions (volume and surface area percentages of the total values of approximately 75 mL and 16,000 mm2, respectively) of each section identified. Further description and details of the AIT can be found in the literature.19,26
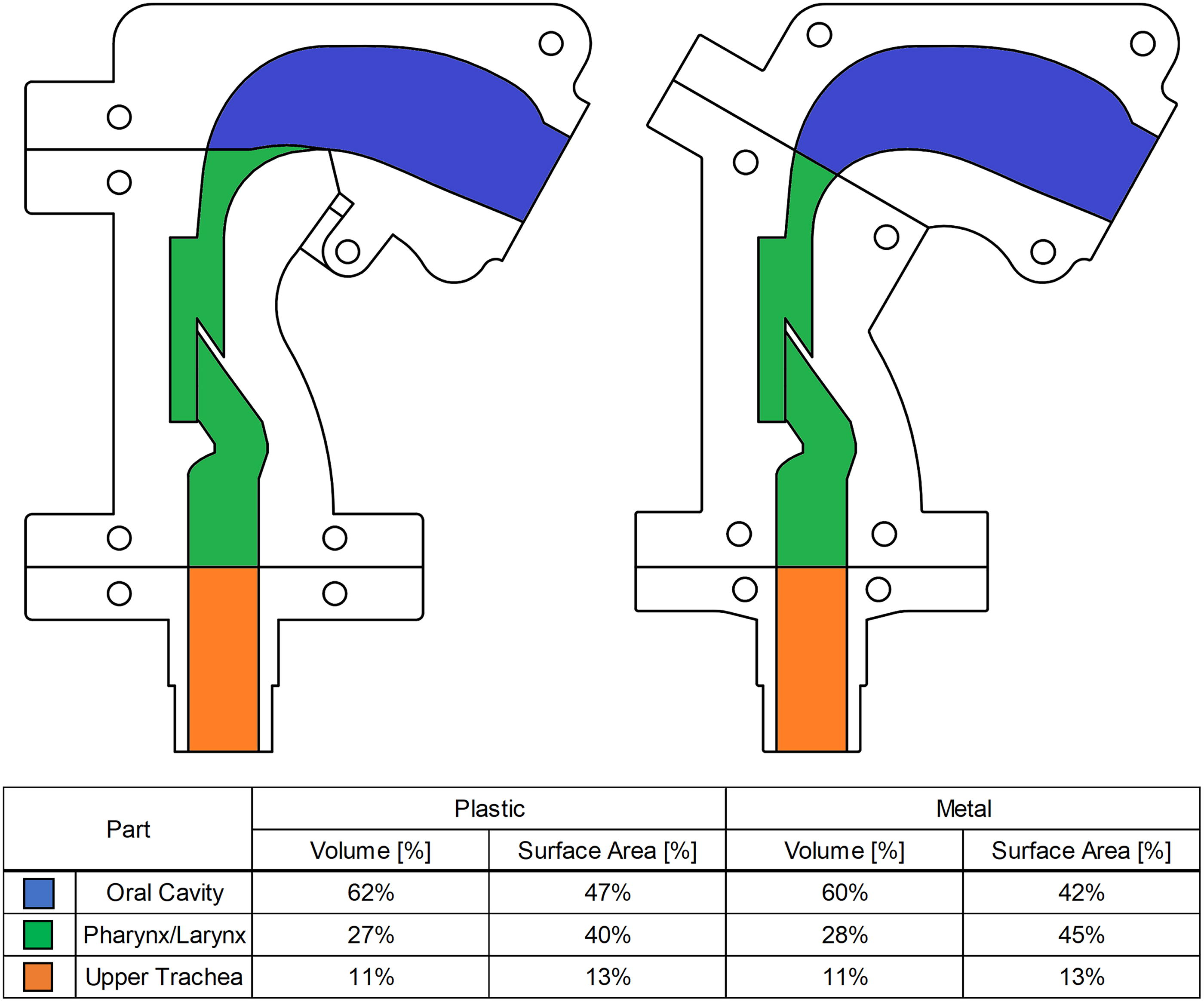
Schematics of the plastic (left) and metal (right) s-AIT prototypes, with analogs of anatomical regions identified. Relative proportions of the volume and surface area of each section are included. s-AIT, sectioned Alberta Idealized Throat.
Experimental design
Investigational inhalers
Canisters containing suspension formulation of epinephrine in HFA-134a (Primatene MIST™; Amphastar Pharmaceuticals Inc, Rancho Cucamonga, CA) were purchased for testing. pMDI actuators manufactured by Bespak (Consort Medical, now Recipharm) with various orifice diameters were used for experiments. Three actuator orifice diameters, nominally 0.42 mm, 0.33 mm, and 0.22 mm, were selected for testing. Primatene Mist canisters were purchased over the counter, with canisters from lot numbers PR302D8, PR303E8, PR306B1, PR328H1, and PR309B3 used during testing.
Experimental methods
Experiments were performed following methods for in vitro testing of extrathoracic deposition from pMDIs as described in previous work.18,20,27 In brief, pMDIs were actuated into the s-AIT at known flow rates and insertion angles, with a filter positioned downstream of the s-AIT to capture the dose of epinephrine exiting the s-AIT. A schematic of the apparatus is provided in Figure 2. Inner surfaces of the s-AIT (both the metal and plastic versions) were coated with silicone grease (Molykote 316; Dow Corning) prior to testing. Flow rates were generated via vacuum pump, monitored via flowmeter (Model 4043; TSI), and set to the desired value prior to actuation of the pMDI into the s-AIT. Prior to each test, the pMDI canister was inserted into the actuator of interest, shaken vigorously for 3–5 seconds, and then fired once to waste within a fume hood. The pMDI was then re-shaken, placed in the mouthpiece adapter connected to the s-AIT, and actuated into the s-AIT with attached downstream filter. After 5 seconds, the pMDI was removed from the mouthpiece adapter, and the process was repeated until three total actuations were delivered into the throat and filter.
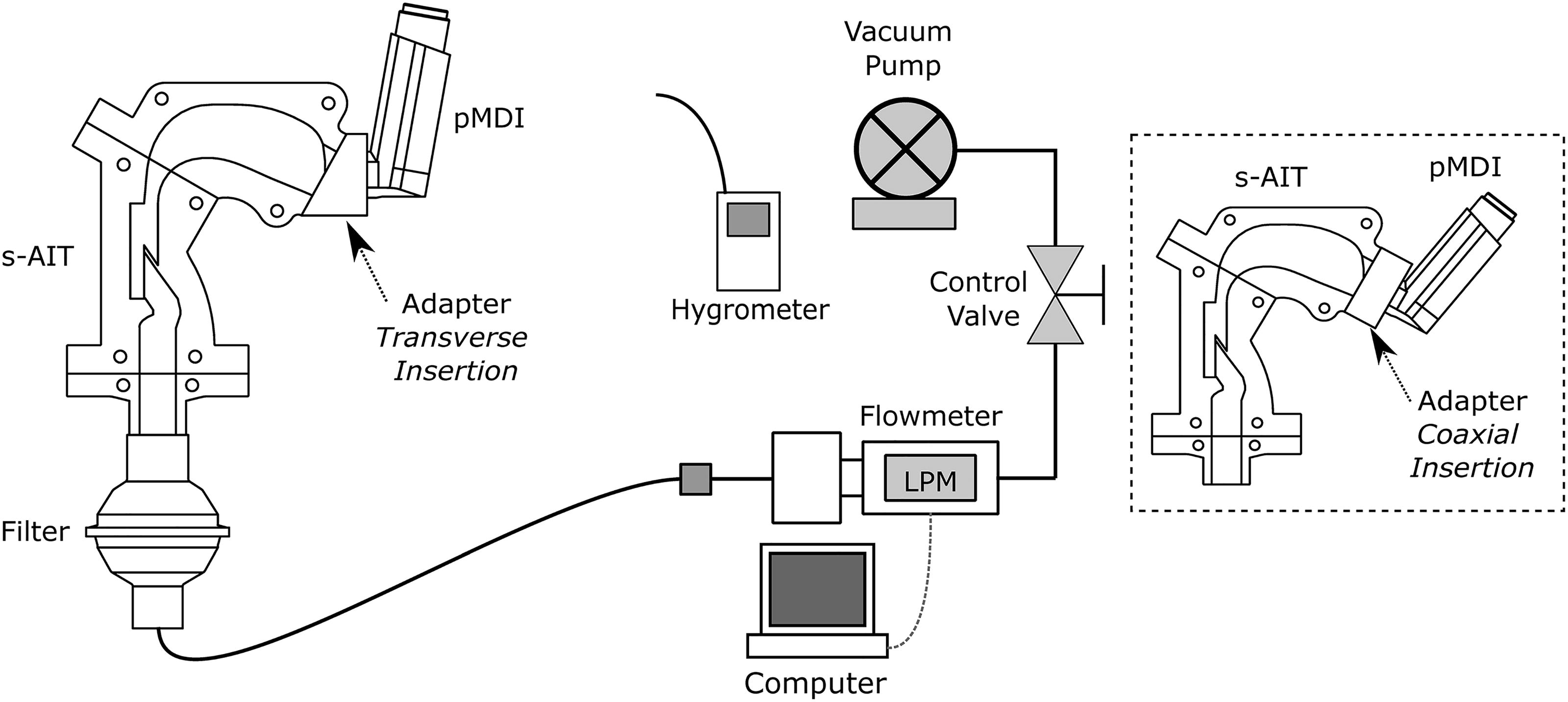
The experimental setup used to investigate deposition of Primatene Mist HFA in the s-AIT and filter, where the inhaler is inserted in the transverse insertion angle (i.e., directed toward the tongue). The dotted box shows the s-AIT with the inhaler oriented in the coaxial insertion angle (i.e., directed toward the back of the throat, at a 29° inclination from horizontal 18 ).
Experiments were first performed in the plastic s-AIT. These experiments evaluated the effects of actuator orifice diameter (0.42 mm, 0.33 mm, and 0.22 mm) and insertion angle (coaxial—directed toward the back of the throat; transverse—directed toward the tongue 18 ) on deposition at a flow rate of 30 L/min (typical of standard pMDI testing). Five repeated measures (n = 5) were performed for each factor combination using a single actuator for each actuator orifice of interest. Prior to each day of testing, the pMDI canister was primed by firing two shots to waste. The testing order for the three actuator orifice diameters was randomized. The block of tests utilizing the coaxial insertion angle were performed first using a canister from Lot PR302D8, followed by the block of tests utilizing the transverse insertion angle using a canister from Lot PR303E8. After each day of testing, actuators were cleaned with warm soapy tap water, then rinsed with deionized ultra-filtered (DIUF) water and dried with compressed building air. Environmental conditions in the laboratory were monitored with a digital hygrometer/thermometer (MI70 Measurement Indicator with HMP75B Humidity and Temperature Probe; Vaisala); temperatures ranged from 22°C to 25°C, while relative humidity ranged from 4% to 20%.
A separate full-factorial study was then performed using the metal s-AIT to investigate the effects of actuator orifice diameter (0.42, 0.33, and 0.22 mm), insertion angles (coaxial—directed toward the back of the throat; transverse—directed toward the tongue), and inhalation flow rates (10, 30, 60, and 100 L/min) on regional extrathoracic deposition. This wider range of flow rates was chosen to reflect the surprisingly large variation in flow rates that have been observed in real-world patient use of pMDIs. 28 Three repeated measures were obtained for each factor combination using a different specific actuator for each test (n = 3 at each experimental condition, for a total n = 72 across all runs and repeats). Testing order of the 72 runs was randomized. Prior to each day of testing, the pMDI canister was primed by firing two shots to waste. After each individual test, actuators were cleaned with warm tap water, rinsed with DIUF water, and dried with compressed building air. Environmental conditions in the laboratory were monitored with a digital hygrometer/thermometer (MI70 Measurement Indicator with HMP75B Humidity and Temperature Probe; Vaisala); temperatures ranged from 21.1°C to 21.6°C, while relative humidity ranged from 5% to 23%, reflective of the relatively dry indoor air conditions experienced in Edmonton, Alberta, Canada during winter, when these experiments were performed.
For tests using the plastic s-AIT, drug depositing in the plastic s-AIT and downstream filter was assayed via UV spectroscopy using 0.1 N hydrochloric acid as solvent. Absorbance relative to standard was quantified at a maximum wavelength of 279 nm using a diode array UV-vis spectrophotometer (Cary 8454; Agilent). For the study using the metal s-AIT, the assay was optimized to reduce the need for repeated washings while also examining the dose remaining in the actuator: drug depositing in the metal s-AIT, in the downstream filter, and remaining in the actuator (including in the sump and orifice) was assayed via UV spectroscopy using 1:1 (volumetric) 0.1 N hydrochloric acid and methanol as the solvent. Absorbance relative to standard was quantified at a maximum wavelength of 280 nm using the same diode array UV-vis spectrophotometer. In all cases, appropriate blanks were used to account for potential interference of silicone grease on samples recovered from sections of the s-AIT. The label claim of Primatene Mist is 125 µg of epinephrine per dose, with the nominal total label claim for each test being 375 µg (3 × 125 µg).
Residual particle size
A limited batch of testing was performed to investigate the influence of orifice size on residual particle size distributions measured downstream of the AIT, following previously described methods from our group based on compendial approaches. 29 Here, a standard AIT was used in conjunction with a Next Generation Impactor (NGI) without pre-separator operated at 30 L/min using the largest (0.42 mm) and smallest (0.22 mm) actuator orifice diameters, with inhalers oriented in the coaxial configuration. For each test, three actuations from the inhaler were collected in the AIT and NGI, with deposition assayed via UV spectroscopy as described previously, using a canister from lot PR309B3. Mass median aerodynamic diameter (MMAD) and geometric standard deviation (GSD) were calculated via linear interpolation on measured particle size distributions following standard approaches. MMAD and GSD were compared via student’s t-test for three repeated measurements.
Data analysis
For tests conducted using the plastic s-AIT, the drug was recovered from each section of the s-AIT as well as the downstream filter. Deposition in each portion of the plastic s-AIT was normalized by the ex-actuator dose, with the ex-actuator dose calculated as the sum of drug mass recovered from each section of the s-AIT and the filter. The ex-actuator doses for each actuator orifice (collated across insertion angle) were compared with one-way ANOVA. Two-way ANOVA was used to evaluate the effects of actuator orifice diameter and inhaler insertion angle on deposition in each portion of the plastic s-AIT and downstream filter, with post-hoc multiple comparisons via Tukey’s method to evaluate main effects of actuator orifice.
For tests conducted using the metal s-AIT, the sum of drug masses recovered from each section of the metal s-AIT, the downstream filter, and the actuator was taken as the total recovered dose for each test. The ex-actuator dose was calculated as the sum of deposition in components of the metal s-AIT and the downstream filter. The total measured dose, ex-actuator dose, and dose recovered from the actuator itself were compared across each actuator orifice via one-way ANOVA with post-hoc multiple comparisons (via Tukey’s method), with data collated across flow rates and insertion angles. For each experimental run, deposition in each portion of the metal s-AIT and the downstream filter was normalized by the ex-actuator dose. Actuator orifice diameter and flow rate were considered the main variables of interest, with two-way ANOVA used to identify differences in deposition as a percent of ex-actuator dose. Post-hoc multiple comparisons, performed using Tukey’s method, were performed to evaluate simple effects of actuator orifice diameter at each flow rate (comparisons of results across flow rates were not considered), with p values for multiple comparisons being multiplicity-adjusted. This analysis was applied to data taken with each inhaler insertion angle separately, and statistical comparisons were performed in GraphPad Prism (v 9.5.1) using an α level of 0.05.
Additional analysis was performed to explicitly compare deposition between the coaxial and transverse insertion angles at each particular flow rate and actuator orifice diameter for tests in the metal s-AIT. The difference in deposition (
Results
Plastic s-AIT
Ex-actuator dose, measured for each actuator orifice size in the plastic s-AIT and collated across insertion angle, ranked in order with actuator orifice: 361.1 (standard deviation [SD] 53.0) µg with the 0.42 mm actuator, 331.3 (SD 32.5) µg with the 0.33 mm actuator, and 320.1 (SD 32.9) µg with the 0.22 mm actuator, although the differences were not statistically significant (p = 0.293 via one-way ANOVA). Deposition in each region of interest in the plastic s-AIT at a 30 L/min flow rate is shown in Figure 3. Two-way ANOVA yielded significant effects of actuator orifice in all regions (p < 0.001 in the oral cavity and filter, p < 0.010 in the pharynx/larynx, p = 0.016 in the upper trachea). Significant effects of inhaler insertion angle were found in the oral cavity (p = 0.043) and the pharynx/larynx (p < 0.001). A significant interaction effect between actuator orifice and insertion angle was observed only in the pharynx/larynx (p = 0.003).

Deposition in each region of interest in the plastic s-AIT for both coaxial and transverse insertion angles at a 30L/min flow rate. Top left = oral cavity, top right = pharynx/larynx, bottom left = upper trachea, and bottom right = filter. Error bars denote SD. Asterisks (
The 0.22 mm actuator gave lower oral cavity deposition (∼27% of ex-actuator dose) compared with 0.33 mm and 0.42 mm actuators (∼44% and ∼48%, respectively, averaged across insertion angle). Oral cavity deposition with the 0.42 mm actuator also showed sensitivity to insertion angle, increasing from ∼42% with a coaxial insertion angle to ∼54% with a transverse insertion angle. In the pharynx/larynx, deposition (averaged across insertion angle) was significantly greater with the 0.22 mm actuator (∼25%) than was observed with the 0.42 mm actuator (∼21%). The 0.42 mm actuator also showed high sensitivity to insertion angle with regards to deposition in the pharynx/larynx, with the coaxial insertion angle yielding much greater deposition than the transverse insertion angle (∼26% versus ∼16%, respectively). The 0.22 mm actuator yielded much greater deposition in the filter (∼43%) compared with either the 0.33 and 0.42 mm actuators (∼28% in both cases, averaged across insertion angle).
Metal s-AIT
Total measured dose, ex-actuator dose, and the dose recovered from the actuator for three actuations into the metal s-AIT with each actuator used are presented in Table 1, where results have been collated across flow rates and insertion angles. Because the canister was primed to waste in the actuator once immediately prior to each test, the dose recovered from the actuator reported here is actually for four actuations; the total measured dose (the sum of the ex-actuator dose and the dose recovered from the actuator) should be interpreted accordingly. Total measured dose in the metal s-AIT study averaged 537.8 µg (SD = 63.7 µg; n = 72). No differences were observed in the total measured dose as a function of actuator orifice (p = 0.216). Significant differences were observed in the ex-actuator dose as a function of actuator orifice (p = 0.001): the 0.22 mm actuator yielded significantly lower ex-actuator doses than the 0.42 mm actuator (p < 0.001), with other differences being statistically insignificant (0.22 mm vs. 0.33 mm, p = 0.139; 0.33 mm vs. 0.42 mm, p = 0.151). Differences were also observed in the dose recovered from the actuator itself (p < 0.001), with the 0.22 mm actuator having a higher amount of drug remaining in the actuator than the 0.33 mm (p = 0.033) and 0.42 mm (p < 0.001) actuators.
Total Measured Dose, Ex-Actuator Dose, and Dose Remaining in the Actuator with Each Actuator for Tests in the Metal Sectioned Alberta Idealized Throat, Collated Across Flow Rates and Insertion Angles
Presented as average with standard deviation in parenthesis. After a single priming shot to waste, three actuations were delivered into the sectioned Alberta Idealized Throat for each test.
Dose remaining in the actuator corresponds to four actuations—see text in Results: Metal s-AIT.
Deposition in regions of interest of the metal s-AIT: Coaxial insertion angle
The distribution of deposition obtained with each actuator as a function of flow rate, delineated by region of interest, is presented in Figure 4 for data obtained with the coaxial insertion angle in the metal s-AIT.

Comparison of deposition obtained with each actuator for the coaxial inhaler insertion angle at each flow rate in the metal s-AIT, delineated by region of interest: top left = oral cavity, top right = pharynx/larynx, bottom left = upper trachea, and bottom right = filter. Error bars denote SD. Asterisks (
Significant differences in deposition obtained with different actuators were consistently evident in the oral cavity and filter. For oral cavity deposition, two-way ANOVA suggests that main effects of flow rate and actuator were significant, in addition to a significant interaction effect between these variables (all p’s < 0.001). The 0.22 mm actuator with the coaxial insertion angle yielded significantly lower oral cavity deposition than the other actuators at each flow rate, showing a maximum of 18.3% of the ex-actuator dose at 10 L/min that decreased to a relatively stable value near 11% for flow rates of 30, 60, and 100 L/min. The greatest oral cavity deposition was observed for the 0.42 mm actuator, with a maximum of roughly 36% at 10 L/min that decreased steadily to a minimum of approximately 20% at 100 L/min. The 0.33 mm actuator gave middle-ground values between these cases. Differences in oral cavity deposition across actuators were lowest at 100 L/min.
For deposition in the pharynx/larynx, a significant main effect of flow rate was observed (p < 0.001), but not of actuator (p = 0.641) nor interaction effects (p = 0.793). Deposition in the pharynx/larynx, increased from a minimum of approximately 1.3% of the ex-actuator dose at 10 L/min to a maximum of approximately 13% at 100 L/min, and was generally consistent across actuators.
For deposition in the upper trachea, significant main effects of flow rate (p < 0.001) and actuator (p = 0.010) were observed, with no interaction effect (p = 0.190). The only significant difference in deposition caused by actuator occurred at 10 L/min, where the 0.42 mm actuator had lower deposition than the others. Overall deposition in the upper trachea was low, ranging from roughly 0.5%–3% of the ex-actuator dose.
For deposition in the filter, significant main effects were found for flow rate and actuator (p’s < 0.001), in addition to a significant interaction effect (p = 0.004). The 0.22 mm orifice had significantly greater filter deposition than all other actuators at 10, 30, and 60 L/min flow rates, as well as significantly greater deposition at 100 L/min compared with the 0.42 mm actuator. Filter deposition for the 0.22 mm orifice ranged from a minimum of 71.9% at 100 L/min to a maximum of 84.8% at 30 L/min. The 0.33 mm actuator also had significantly greater filter deposition than the 0.42 mm actuator for the 10, 30, and 60 L/min flow rates but not at 100 L/min. Filter deposition for the 0.42 mm actuator ranged from a minimum of roughly 62% at 10 L/min to a maximum of approximately 68% at 60 L/min. Overall differences in filter deposition across actuators was lowest at 100 L/min.
Deposition in regions of interest of the metal s-AIT: Transverse insertion angle
Results obtained with the transverse insertion angle are presented in Figure 5. Trends were consistent with those observed with the coaxial insertion angle, that is, considerable differences in deposition were observed in oral cavity and filter deposition across actuators, while deposition in the pharynx/larynx and the upper trachea were more similar. An exception occurred in the upper trachea, where a significant interaction effect was observed (p = 0.029) unlike what was found for the coaxial orientation. This manifested in a few minor differences in deposition in this region, but overall deposition remained low (i.e., <4% in all cases).
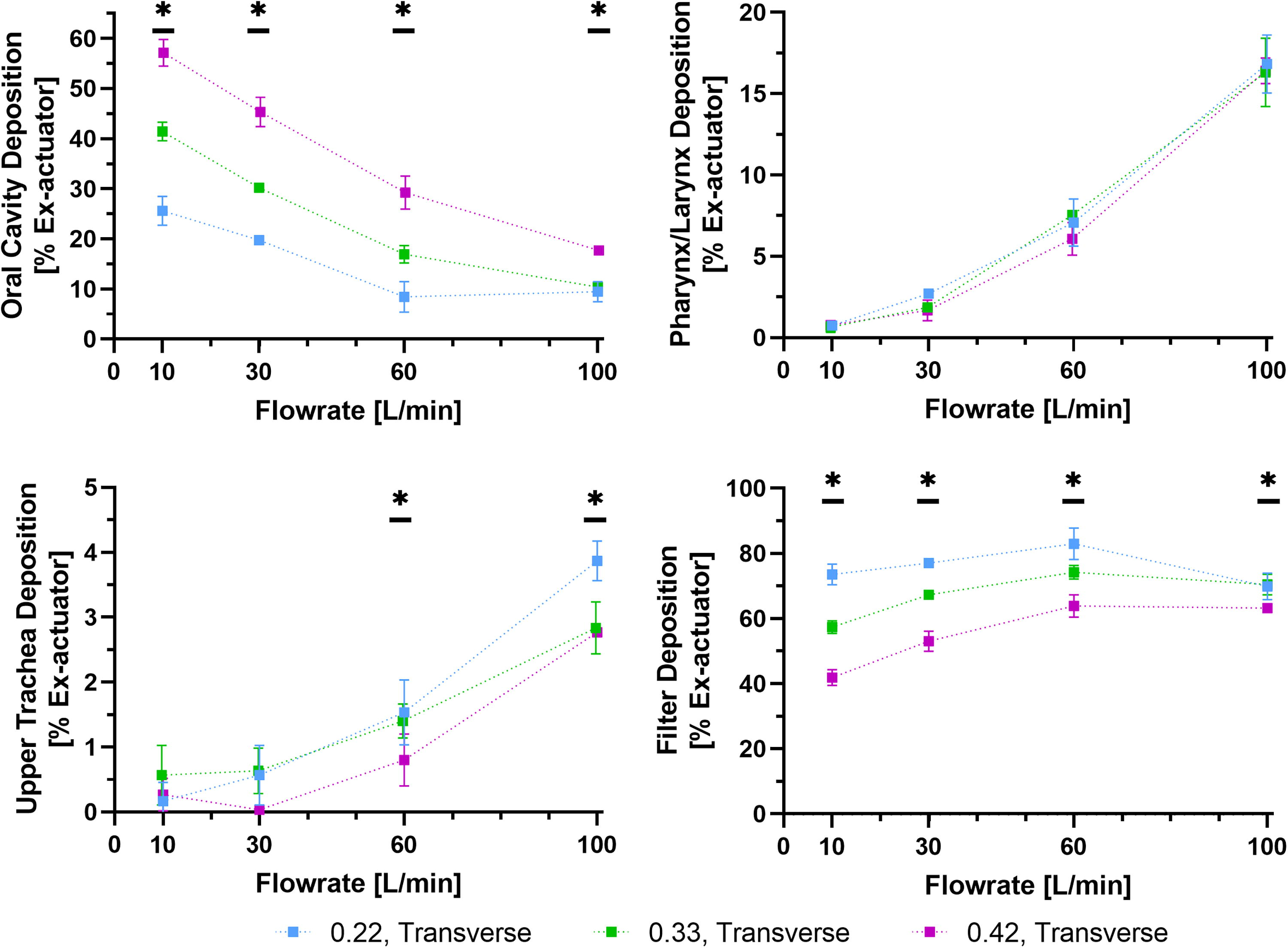
Comparison of deposition obtained with each actuator for the transverse inhaler insertion angle at each flow rate in the metal s-AIT, delineated by region of interest: top left = oral cavity, top right = pharynx/larynx, bottom left = upper trachea, and bottom right = filter. Error bars denote SD. Asterisks (
Effect of inhaler orientation in the metal s-AIT
Figure 6 shows the difference in deposition when changing from a coaxial to a transverse insertion angle in the metal s-AIT, calculated via Equation (1) (where positive values indicate increased deposition when using the transverse orientation). In the oral cavity, two-way ANOVA showed significant main effects of flow rate and actuator on differences with angle, in addition to a significant interaction effect (all p’s < 0.001). Deposition with the transverse angle was generally greater than with the coaxial angle for the lower flow rates of 10 and 30 L/min, becoming more similar at 60 and 100 L/min. The maximum difference in oral cavity deposition with angle was 21.3% (SD 3.9%) of the ex-actuator dose, obtained with the 0.42 mm actuator at 10 L/min. Overall, the 0.22 mm actuator provided the smallest differences with angle in the metal s-AIT oral cavity across all flow rates, ranging from approximately 8% at 10 and 30 L/min to approximately −2% at 60 and 100 L/min (a span of 10% of the ex-actuator dose). The largest differences with angle were observed with the 0.42 mm actuator, ranging from approximately 21% at 10 L/min to −2% at 100 L/min (a span of 23% of the ex-actuator dose).
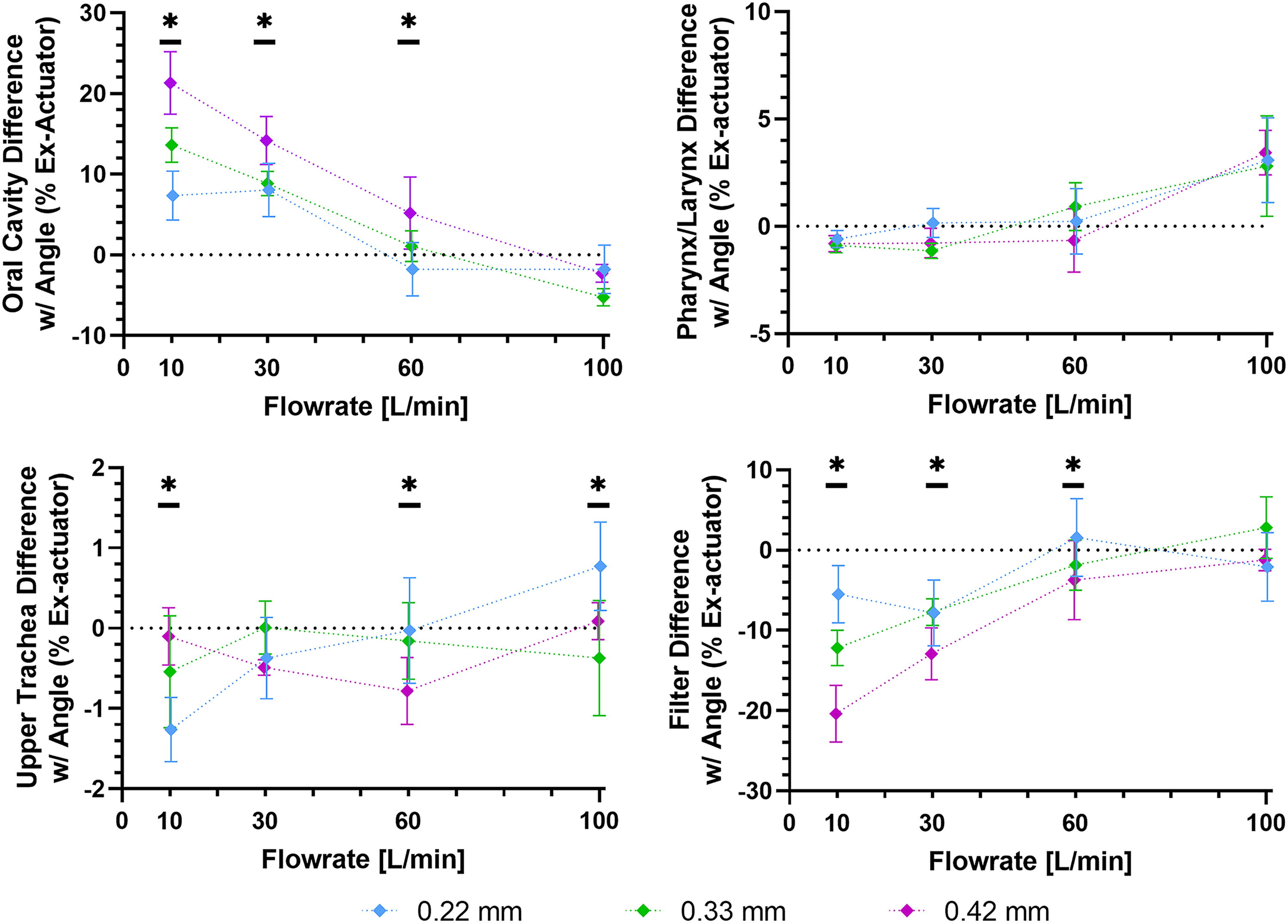
Difference in deposition with a transverse inhaler insertion angle relative to a coaxial insertion angle for each actuator orifice in the metal s-AIT, delineated by region of interest: top left = oral cavity, top right = pharynx/larynx, bottom left = upper trachea, and bottom right = filter. Error bars denote SD. Asterisks (
In the pharynx/larynx, significant main effects of flow rate (p < 0.001) on difference with angle were observed, with no observed effect of actuator size (p = 0.470) and no interaction effects (p = 0.242). Differences with angle were within 1.2% of the ex-actuator dose for the 10, 30, and 60 L/min flow rates for all actuators in the metal s-AIT, and slightly greater at 100 L/min (∼3% of ex-actuator dose). In the upper trachea, significant main effects of flow rate (p < 0.001) and interaction effects were observed (p < 0.001), with no observed effect of actuator (p = 0.788). Regardless of statistical significance, differences with angle here were small for all cases, ranging from a minimum of −1.3% to a maximum of 0.8%.
In the filter, significant main effects of flow rate (p < 0.001) and actuator (p < 0.001) were observed, in addition to a significant interaction effect (p < 0.001). The overall span of difference with angle was lowest for the 0.22 mm actuator (from approximately −8% at 30 L/min to 2% at 60 L/min, a span of 10% of ex-actuator dose that mirrored the changes observed in the oral cavity) and greatest for the 0.42 mm actuator (from approximately −20% at 10 L/min to −1% at 100 L/min, a span of 19% of ex-actuator dose). The greatest differences with angle were observed at the lowest flow rate of 10 L/min, with the largest difference (−20.4% of ex-actuator dose) occurring for the 0.42 mm actuator. Differences between angles as a function of actuator orifice were lower at higher flow rates, and were not significant at 100 L/min.
Residual particle size distributions
Total recovered drug from the AIT and NGI (the ex-actuator dose) were 340.2 ± 26.0 µg and 403.9 ± 32.5 µg for the 0.22 mm and 0.42 mm actuator orifice diameters, respectively. The 0.22 mm actuator yielded a residual MMAD of 1.92 (SD 0.05) µm and GSD of 1.81 (SD 0.04) compared with a residual MMAD of 2.03 (SD 0.04) and GSD of 1.73 (SD 0.03) for the 0.42 mm actuator. No significant differences were observed in MMAD (p = 0.09) or GSD (p = 0.09).
Discussion
Major findings in the present work show that actuator orifice diameter strongly influences deposition of a suspension formulation of epinephrine in regions of interest in a plastic and a metal version of an idealized airway model sectioned into analogs of the oral cavity, the pharynx/larynx, and the upper trachea. The use of smaller actuator orifice diameters was associated with decreased oral cavity deposition and increased deposition in a downstream filter (an in vitro measure of the total lung dose) for deposition reported as a percent of the ex-actuator dose. Smaller actuator orifice diameters were also associated with reduced differences in deposition between coaxial and transverse inhaler orientation in regions of interest. Flow rate was observed to influence the distribution of deposition across regions of interest in the metal s-AIT, with higher flow rates associated with reduced oral cavity deposition, increased pharynx/larynx deposition, and increased upper trachea deposition. Effects of flow rate on filter deposition were somewhat lower, with the filter dose showing more consistency in dosing than other regions of interest for different flow rates. Smaller actuator orifices were associated with slight decreases in the ex-actuator dose, caused by increased amounts of drug remaining in the sump, orifice, or actuator body itself—tuning of, for example, the formulation or metering valve volume may allow for constancy of the ex-actuator dose if desired. These results are the first demonstration of actuator orifice diameter having significant influence on in vitro regional extrathoracic deposition, adding clarity to propositions that actuator orifice diameter influences throat deposition from pMDIs.4,30 Results also suggest that use of smaller actuator orifice diameters may improve consistency of performance with respect to plausible elements of variability in patient use, such as inhaler insertion angle and flow rate.31–33
The reductions in oral cavity deposition that were observed with smaller actuator orifice diameters may be a result of the decreased plume momentum associated with smaller actuator orifices4,30 and related effects on interactions between the spray plume and the sheath of ambient co-flow air inhaled through the pMDI. 18 The lower momentum associated with smaller orifice diameter follows from the choked flow condition that occurs shortly after pMDI actuation, as the metered dose empties through the valve stem, actuator sump, and orifice, exiting at sonic velocity.34,35 If thermo-physical properties of the formulation are similar between different size orifices during the atomization process, the sonic velocity of the two-phase flow occurring within the actuator orifice may be largely independent of orifice size (some differences in the sonic velocity may occur between actuator orifices due to, for example, wall friction effects—see discussion by Myatt et al. 35 —but for present purposes we ignore such effects). Conversely, with velocity and metered volume fixed, the mass flow rate of propellant exiting the orifice decreases with decreasing orifice area, resulting in a longer plume duration and a lower momentum plume. In the present experiments, we suspect that lower momentum plumes were associated with reduced impaction of pMDI droplets on airway surfaces as they transited the oral cavity, during which time droplet velocities rapidly decrease from initially high values at the exit of the orifice 36 to velocities that match the inhaled airstream. A competing hypothesis relates to potential effects of actuator orifice on initial droplet sizes, although earlier works37,38 have shown that orifice diameter has a very minor influence on initial droplet size distributions for pMDI formulations containing low ethanol levels such as the commercial formulation used here. While we did not measure initial droplet sizes in the present work, our measurements of residual particle size distributions suggest no differences in the residual size of aerosol generated for the present formulation with different actuator orifice diameters, as would be expected for the case where initial droplet distributions are likewise similar.
Downstream of the oral cavity, the similarity in deposition fraction in the pharynx/larynx across actuators for the metal s-AIT suggests that plume dispersion may be largely complete after transit through the oral cavity, such that subsequent deposition behavior may be well-described as that for fully entrained aerosol particles. 39 Fittingly, deposition in the pharynx/larynx increased with flow rate, as is expected for entrained aerosols based on consideration of the impaction parameter, or particle Stokes number, 40 and as has been previously demonstrated in vitro with the AIT. 24 Our results show that some differences in deposition may occur between plastic and metal geometries on a regional basis, adding to existing literature that has demonstrated dissimilarities in total deposition from suspension pMDIs between plastic and metal in vitro extrathoracic geometries. 41 Here, deposition in the plastic s-AIT trended toward higher amounts in the regions representing the pharynx/larynx and upper trachea and lower amounts in the filter when compared with the metal s-AIT at a 30 L/min flow rate. Differences in deposition between the plastic and metal geometries were considerable in some cases. For example, filter deposition with the 0.42 mm actuator orifice diameter at 30 L/min was ∼25% of the ex-actuator dose in the plastic s-AIT, versus ∼60% in the metal s-AIT, a consequence of lower total deposition in the metal s-AIT relative to the plastic s-AIT. While slight differences exist in the delineation between regions of interest in the plastic versus metal s-AIT (see the relative surface areas and volumes summarized in Fig. 1), the magnitude of differences in total deposition in the s-AIT as a proportion of the ex-actuator dose cannot be explained by these differences in internal delineations between regions. An alternative explanation may relate to differences in electrostatic effects on particles during transit of the mouth-throat, resulting from dissimilar electrostatic properties of plastic versus metal materials. Kwok, Glover, and Chan 42 have shown that suspension pMDIs can generate particles with high levels of charging, up to a degree that deposition behavior during transit of the upper airways may be influenced. 43 Differing electrostatic forces acting on particles near airway surfaces as a result of differing material properties between the metal and plastic geometries may therefore play a role in the current findings, particularly as we did not implement measures to influence or mitigate potential electrostatic effects (e.g., triboelectric charging) in the present work. At present, no study has systematically investigated the role of electrostatics on in vitro extrathoracic deposition of pMDI aerosols. Importantly however, the overall trends in deposition related to actuator orifice (namely, that smaller actuator orifices were associated with reduced oral cavity deposition, increased filter deposition, and more consistency in dosing across varying inhaler insertion angles) were consistent between the plastic and metal s-AITs. In vivo deposition data would be valuable in evaluating whether the plastic or metal data is more predictive of mouth-throat deposition for the pMDIs tested, and the lack of such information is a limitation of the current work.
An additional limitation of the present work relates to the lack of validation for regional deposition in the three subregions of the s-AIT. The AIT was itself developed as an idealized model of adult oral extrathoracic airways by incorporating simplified analogs of important anatomical features and dimensions 19 to replicate extrathoracic deposition behavior of inhaled aerosols that occurs on average in adults. While the AIT has been shown to provide accurate estimates of total extrathoracic deposition measured in vivo for numerous pharmaceutical aerosols,20–22 this does not necessitate that regional extrathoracic deposition is accurately replicated by the s-AIT. A validation of regional deposition measurements with the s-AIT is complicated by an absence of readily-available in vivo regional extrathoracic deposition information for pMDI aerosols in the literature. In vivo imaging studies typically report total extrathoracic deposition (including swallowed dose via the stomach) and are not focused on regional deposition within the upper airways.44–46 Absent of a full validation, there is a risk that our regional deposition measurements are not fully representative of what may be observed in a real adult patient population. This is further complicated by the quantitative differences in deposition observed in different regions between the plastic and metal s-AIT geometries, for which there is a lack of suitable in vivo data to interpret. Nevertheless, we suspect that our major findings (that actuator orifice diameter influences the relative proportions of deposition in sections of the extrathoracic region, as well as the dose reaching the lungs) are robust, given the consistency of the trends we have observed here across inhalation flow rates and inhaler insertion angles, for both plastic and metal geometries.
Our results suggest that the use of smaller pMDI actuator orifice diameters can significantly reduce the dose depositing in the oral cavity, significantly increase the dose reaching the lungs, and reduce the sensitivity of deposition to elements of variability in patient use like inhalation flow rate and inhaler insertion angle.
Conclusions
Actuator orifice diameter (spanning 0.22–0.42 mm) was found to influence deposition within the extrathoracic region for a commercially available HFA suspension epinephrine pMDI formulation in plastic and metal sectioned AITs. Smaller orifices were associated with reduced oral cavity deposition, increased filter deposition, and reduced variability in dosing with changing inhaler insertion angles. Flow rate (ranging from 10 to 100 L/min) was also observed to influence regional deposition, with higher flow rates associated with reduced oral cavity deposition, increased pharynx/larynx deposition, and increased upper trachea deposition in tests with the metal s-AIT. The present work suggests that optimization of actuator orifice diameter can reduce deposition of an HFA suspension epinephrine formulation in the oral cavity, while simultaneously increasing the dose delivered to the lungs.
Footnotes
Acknowledgments
PMDI actuators were supplied by Bespak. The authors gratefully acknowledge late H. Orszanksa for support in early phases of this work.
Authors’ Contributions
C.A.R. was involved in the study design, performed experiments, conducted data and statistical analysis, and wrote the article. S.T. was involved in the study design, performed experiments, and reviewed and edited the article. G.L., K.S., and W.H.F. were involved in the conception and study design, and reviewed and edited the article. A.R.M. was involved in the conception and study design, supervised the study, and reviewed and edited the article.
Author Disclosure Statement
C.A.R. is currently employed at a contract research organization that receives commercial and noncommercial funding for preclinical drug development programs. S.T. and A.R.M. have received consulting fees from Kokua Pharma Inc. A.R.M. has received research support from Kokua Pharma Inc.
Funding Information
The study was funded by Kokua Pharma Inc.