
Abstract
Background:
Aerosol delivery may be enhanced by utilizing an inspiration-synchronized nebulization mode, where nebulization occurs only during inspiration. This study aimed to compare aerosol delivery of albuterol via a prototype of an inspiration-synchronized vibrating mesh nebulizer (VMN) versus continuous VMN during invasive mechanical ventilation.
Methods:
A critical care ventilator equipped with a heated-wire circuit to deliver adult parameters was attached to an endotracheal tube (ETT), a collection filter, and a test lung. The nebulizer was placed at the humidifier’s inlet, inspiratory limb at the Y-piece, and between the Y-piece and ETT. Conventional VMNs producing standard size aerosol particles (Solo; Aerogen Ltd) were compared with prototype small-particle VMNs (Aerogen Pharma) in both inspiration-synchronization and continuous modes. In each run, 1 mL of albuterol (2.5 mg) was used (n = 5). The drug was eluted from the collection filter and assayed with UV spectrophotometry (276 nm).
Results:
The inhaled dose with inspiration-synchronization mode was 1.4 to 3.6 times that with the continuous mode, regardless of nebulizer positions (all p < 0.001). The small-particle VMN delivered an 8%–69% greater inhaled dose than the conventional VMN (Solo), regardless of the nebulizer placement or aerosol generation mode (all p < 0.001). The highest inhaled dose (50%–60%) with the inspiration-synchronized VMN was observed when it was placed at the ETT (all p < 0.001), whereas the continuous VMN performed better when positioned near the humidifier, with an inhaled dose of 21%–37% (p < 0.001).
Conclusion:
The inspiration-synchronized VMN delivered a greater inhaled dose than continuous VMN, irrespective of nebulizer placement. The prototype VMN producing smaller aerosol particles resulted in a greater inhaled dose than the conventional VMN (Solo), regardless of placement or aerosol generation modes. The inspiration-synchronized VMN achieved the highest delivery when placed close to the airway, whereas the continuous VMN delivered the most when positioned near the ventilator.
Introduction
Aerosolized medications are commonly administered to mechanically ventilated patients, but there is still no standardized method to optimize drug delivery during aerosol therapy.1–3 The vibrating mesh nebulizer (VMN) is commonly utilized for aerosol delivery during mechanical ventilation, since it operates without requiring additional gas flow and has little to no residual volume.3,4 However, the commercially available VMN produces aerosol continuously, leading to medication wastage during the patient’s expiratory phase. To mitigate this loss, the VMN is often placed close to the ventilator, using the humidifier chamber and circuit as a reservoir during expiration. 5
An inspiration-synchronized nebulizer, which generates aerosols during the inspiration phase only, might help reduce aerosol waste. This approach has been utilized in clinical practice for over four decades, primarily with jet nebulizers.1,2,6 However, Ehrmann et al. observed a delay of nebulization termination using jet nebulizers, with 5%–80% of nebulization still occurring during the exhalation phase, leading to a significant aerosol loss. 7 An inspiration-synchronized VMN has been developed and evaluated in several in vitro and in vivo studies with adult subjects receiving noninvasive ventilation.8,9 These studies have shown that the inspiration-synchronized VMN delivers a slightly higher inhaled dose compared to the continuous VMN when placed in the same position.8,9 Similarly, in our previous in vitro study with aerosol delivery via high-flow nasal cannula for adults, when VMN was placed close to the nasal cannula, the inhaled dose was greater with the inspiration-synchronized VMN than the continuous VMN at all flow settings, except for 5 L/min. 10 In addition, the inhaled dose with the inspiration-synchronized VMN placed close to the nasal cannula was comparable to that with a continuous VMN placed at the inlet of the humidifier. 10 In contrast, an in vitro study in pediatric subjects undergoing invasive mechanical ventilation reported a lower inhaled dose with the inspiration-synchronized VMN compared to the continuous VMN, 11 indicating that the effectiveness of the inspiration-synchronized VMN remains controversial, particularly in mechanically ventilated adults.
Recently, DiBlasi et al. used a VMN prototype that produced smaller aerosol particles with a mass median aerosol diameter (MMAD) of 2.8 µm, 12 and incorporated an inspiration-synchronized mode to deliver surfactant to intubated, surfactant-deficient rabbits and pigs.12,13 They observed improved oxygenation responses compared to a control group (nebulized saline) 12 and responses comparable to direct surfactant installation. 13 It remains unclear to what extent inspiration synchronization and smaller particles contributed to the success of their surfactant delivery. In contrast, Dushianthan et al. conducted a randomized controlled trial to evaluate the efficacy of inhaled surfactants in mechanically ventilated adult patients with COVID-19 using the same VMN prototype but did not find significant differences in oxygenation improvement. 14 Therefore, it is important to explore the factors influencing aerosol delivery efficiency. This study aimed to compare aerosol delivery effectiveness using the prototype VMN that generates small aerosol particles with VMNs generating standard size aerosols, with both compared in continuous and inspiration-synchronized modes. We hypothesized that the inspiration-synchronized mode generated higher inhaled doses than the continuous mode and the small-particle VMN generated higher inhaled doses than the conventional VMN.
Methods
Experiment setup
A critical care ventilator (PB980, Medtronic, Minneapolis, MN) equipped with a heated humidifier and a 22-mm inner diameter heated wire circuit (Fisher & Paykel, Auckland, New Zealand) was connected to a lung model (Training Test Lung, Michigan Instruments, Grand Rapids, MI) via an 8.0-mm inner diameter endotracheal tube (ETT) (Shiley, Medtronic) (Fig. 1). A collection filter (Respirgard 303, CareFusion, San Diego, CA) was placed between the ETT and the lung model to capture aerosols deposited at the end of ETT. The ventilator was set to deliver parameters representing a 70-kg adult, with a tidal volume of 420 mL, breathing frequency of 16 breaths/min, positive end-expiratory pressure of 8 cm H2O, inspiratory time of 1 second, flow trigger of 2.0 L/min, an inspiratory flow of 25 L/min using a constant flow waveform.
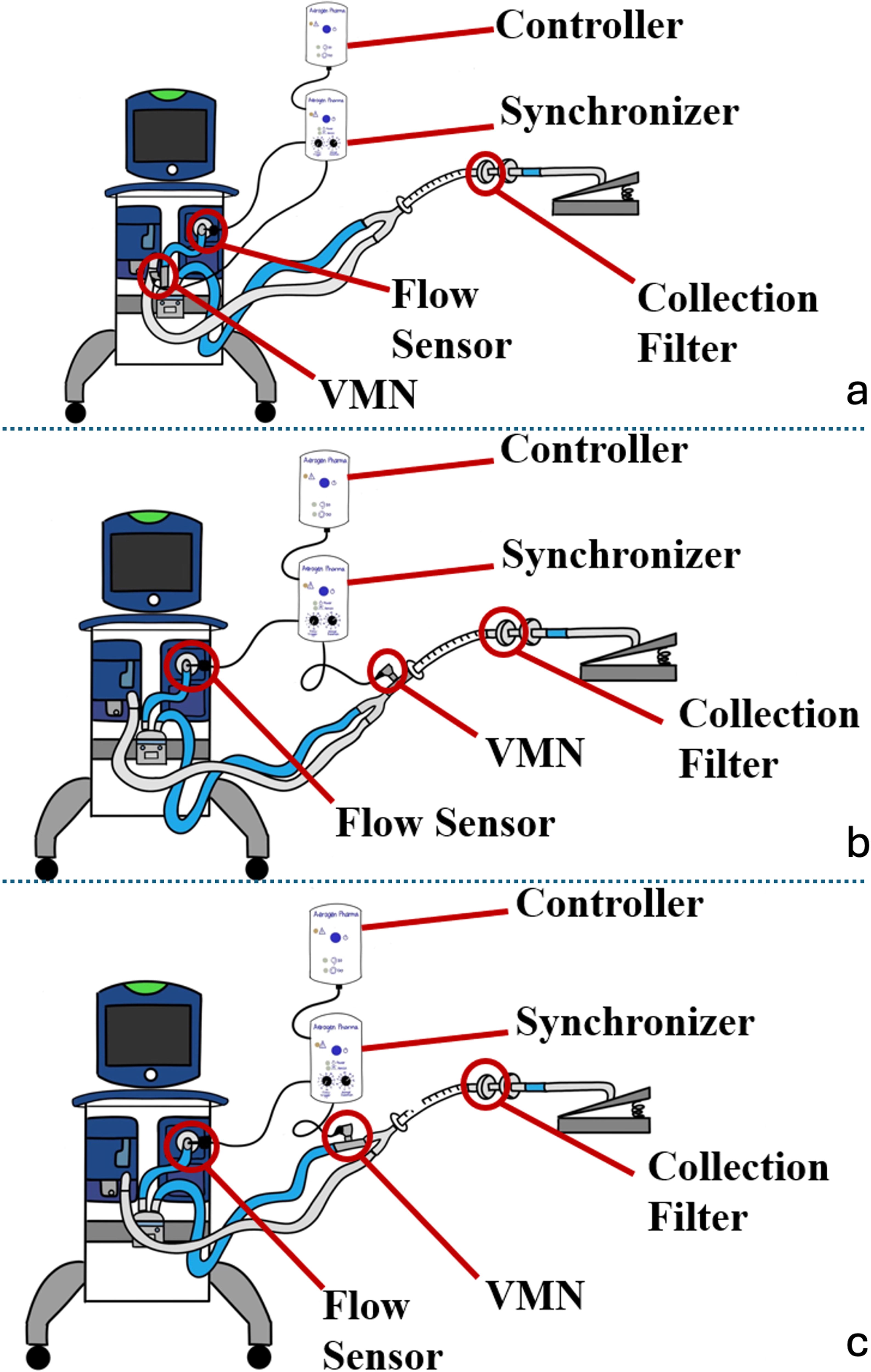
Experiment setup. An 8.0-mm inner diameter endotracheal tube was connected to the Y-piece of a heated wire circuit, which was attached to a critical care ventilator. A collection filter was positioned between the end of the endotracheal tube and the lung model. The flow sensor from the controller of the inspiration-synchronized VMN was located at the ventilator outlet. The VMN was evaluated at three different positions:
Comparisons
Aerosol delivery modes
Each nebulizer was tested in both continuous and inspiration-synchronized modes. Continuous delivery was powered by a standard control module (Aerogen, Gateway, and Ireland), while the inspiration-synchronized delivery was powered by a prototype control module (Aerogen Pharma Corp., San Mateo, CA), which consisted of a flow sensor placed at the ventilator outport to detect the inspiratory flow (Fig. 1). Nebulization was initiated when the inspiratory flow exceeded the baseline and continued for the first 50% of the inspiratory time, meaning aerosol delivery time was 0.5 seconds of the 1.0 seconds inspiratory time.
Nebulizer type
Two types of nebulizers were compared: a conventional VMN (Aerogen Solo, Aerogen, Gateway, Ireland) generating MMAD of 4.8 µm, 15 with geometric standard deviation (GSD) of 2.2 µm and a prototype small-particle VMN (Aerogen Pharma Corp., San Mateo, CA) generating 2.8 µm MMAD and 1.6 µm GSD. 12
Nebulizer placement
Experiments were conducted with the nebulizer placed at three different locations (Fig. 1): (1) at the inlet of the humidifier, (2) at the Y-piece in the inspiratory limb, and 3) between the Y-piece and the ETT.
Each condition was repeated five times (n = 5), for a total of 60 experiments. Three nebulizers of each type (small-particle and conventional VMNs) were used in rotation.
Drug formulation and sample measurement
Albuterol powder (1.0 g, Sigma-Aldrich, St. Louis, MO) was reconstituted with 400 mL sterile water to prepare a concentration of 2.5 mg/mL. For each condition, a fill volume of 1 mL was used. The collection filter was removed 1 minute after the nebulization ended and eluted with a 10-mL solution of 0.1 M HCL mixed with 20% ethanol. The elution was assayed with ultraviolet spectrophotometry at 276 nm.
Statistical analysis
The inhaled dose was calculated as a percentage of the amount of the nominal dose of albuterol (2.5 mg) captured by the collection filter and expressed as mean ± standard deviation for each experiment setting with different nebulizer placement, nebulizer type, and aerosol delivery modes. The Mann–Whitney test was used to compare differences in the inhaled doses between the nebulizer types (conventional VMN vs. small-particle VMN) and aerosol delivery modes (continuous vs. inspiration-synchronized). The Kruskal–Wallis test was used to compare differences in inhaled doses across different nebulizer placements. The linear regression analysis was conducted to identify the significant factors influencing the inhaled dose. The factors examined included aerosol delivery modes, nebulizer type, and nebulizer placement. A p-value of ≤0.05 was considered statistically significant. Data analysis was conducted with SPSS statistical software (SPSS 26.0 for Windows; SPSS; Chicago, IL).
Results
Inhaled dose of inspiration-synchronized vs. continuous aerosol delivery
The inhaled dose was greater with the inspiration-synchronization mode compared to the continuous mode, regardless of nebulizer positions or nebulizer types (all p < 0.001) (Table 1). When the nebulizer was placed close to the ETT, the inhaled dose with inspiration-synchronized VMN was 2.4 to 3.6 times that of the continuous VMN. In contrast, when placed at the inlet of the humidifier, the inhaled dose with inspiration-synchronized VMN was 1.4 to 2.1 times that of the continuous VMN.
Comparison in the Inhaled Doses with Inspiration-Synchronized Versus Continuous VMN
ETT, endotracheal tube; VMN, vibrating mesh nebulizer.
Inhaled dose of small-particle vs. standard size aerosols
The inhaled dose was greater with small-particle VMN than with conventional VMN (Solo) that generates standard size aerosols, regardless of nebulizer placement and aerosol delivery modes (all p < 0.05) (Fig. 2). With the use of inspiration-synchronized VMN, the inhaled dose increased slightly with small-particle aerosols compared to standard size aerosols (VMN Solo), with increments ranging 8% to 24%. In contrast, with continuous VMN, the increments in the inhaled dose with small-particle aerosols compared to standard size aerosols (VMN Solo) were greater, ranging from 49% to 69%.
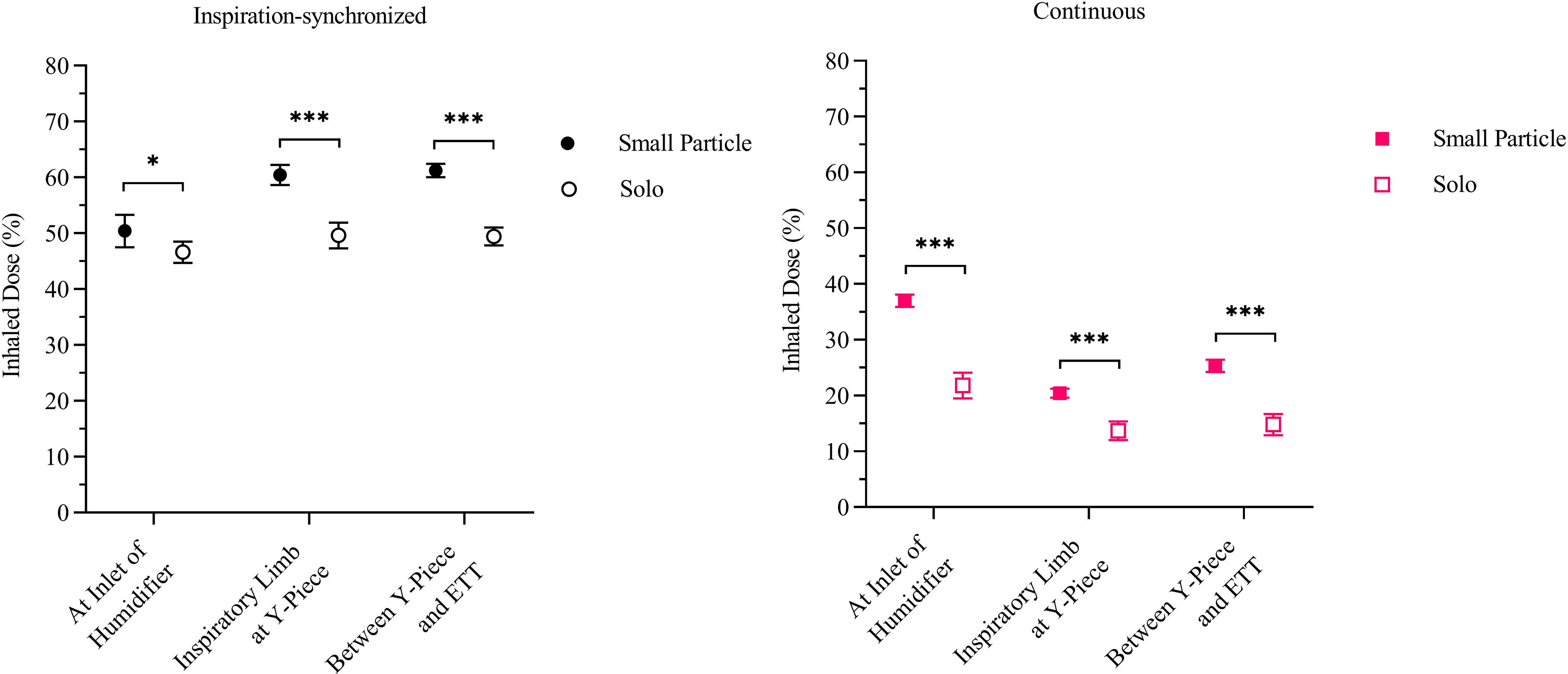
Inhaled dose of small-particle VMN vs. conventional VMN (Solo). Regardless of the aerosol delivery mode (inspiratory-synchronized or continuous) and the nebulizer placement, the small-particle VMN consistently resulted in a higher inhaled dose compared to the conventional VMN (Solo). *p < 0.05, ***p < 0.001. VMN, vibrating mesh nebulizer.
Inhaled doses of different nebulizer placement
With inspiration-synchronized VMN, the inhaled dose was 6%–21% greater when the nebulizer was placed at the Y-piece in the inspiratory limb or between the Y-piece and the ETT compared to placement at the inlet of the humidifier. There were no significant differences in the inhaled doses between placement at the Y-piece in the inspiratory limb and between the Y-piece and the ETT (Fig. 3). With continuous VMN, the inhaled dose was greater when the nebulizer was positioned at the inlet of the humidifier than close to the ETT. Even at the optimal placement for each type of nebulizer, the inhaled dose with inspiration-synchronized VMN placed close to the ETT was still 1.7 to 2.3 times that of the continuous VMN placed at the inlet of the humidifier.
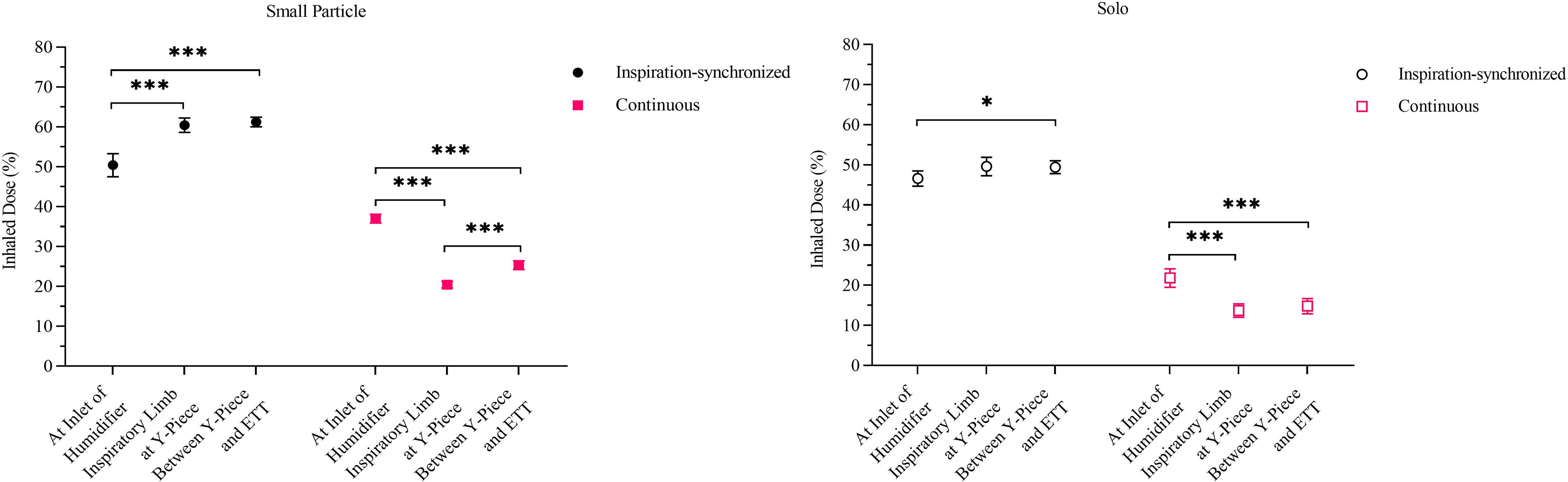
Inhaled dose with different nebulizer placements. Regardless of the aerosol particle sizes (small-particle VMN or conventional VMN [Solo]), for the inspiration-synchronized VMN, placing the nebulizer between the Y-piece and endotracheal tube resulted in a greater inhaled dose compared to placement at the inlet of the humidifier. Conversely, for the continuous VMN, positioning the nebulizer at the inlet of the humidifier generated a higher inhaled dose than positioning it at the Y-piece in the inspiratory limb. *p < 0.05, ***p < 0.001. VMN, vibrating mesh nebulizer.
Factors that influence the inhaled dose
The linear regression analysis indicated that an increased inhaled dose was significantly associated with both inspiration-synchronized delivery and small particle aerosols. The adjusted R2 values were 0.835 (p < 0.001) for inspiration-synchronized delivery and 0.919 (p < 0.001) for small particle aerosols, respectively, demonstrating strong predictive power for these variables.
Discussion
In this in vitro study, we found that the inspiration-synchronized VMN had greater aerosol delivery than the continuous VMN but resulted in a longer administration duration. With the inspiration-synchronized VMN, smaller aerosol particles had a significant but relatively minor impact on aerosol delivery. The highest inhaled dose for the inspiration-synchronized VMN was observed when the nebulizer was positioned close to the ETT in either of the positions tested, while for continuous VMN, the highest inhaled dose occurred when the nebulizer was placed at the inlet of the humidifier.
The greater aerosol delivery with the inspiration-synchronized VMN compared to the continuous VMN aligns with previous findings by Michotte et al., who compared inspiration-synchronized versus continuous VMN during single-limb noninvasive ventilation.8,9 However, when the VMN was placed between the mask and exhalation valve, their in vitro study reported a 13%–20% improvement in aerosol delivery with the inspiration-synchronized VMN compared to the continuous VMN. 8 Likewise, their study among healthy volunteers also reported a 10% greater inhaled dose with the inspiration-synchronized VMN. 9 In contrast, using the same type of VMN (conventional VMN [Solo] generating standard particle size aerosols), we found up to 3.6 fold improvement in aerosol delivery with the inspiration-synchronized VMN. The discrepancy might be explained by the large leak during noninvasive ventilation, which causes significant aerosol loss.
Unlike the in vitro study conducted by Sidler-Moix et al. during pediatric mechanical ventilation, which reported a lower inhaled dose with the inspiration-synchronized VMN compared to both continuous VMN and expiration-synchronized VMN, 11 our study found different results. It should be noted that the inspiration-synchronized VMN in their study was positioned 10 cm away from the Y-piece in the inspiratory limb. 11 Although the bias flow was not reported, given that the 10 cm section of 22 mm inner diameter ventilator tubing contains ∼100 mL volume was similar to the tidal volume used in their study, 11 most aerosols generated during inspiration could not reach the patient airway, leading to substantial waste of aerosols. This might explain the very low (∼5%) inhaled dose with inspiration-synchronized VMN in their study, 11 emphasizing the importance of closer nebulizer placement to the airway when using an inspiration-synchronized VMN, especially for patients with small tidal volumes.
In contrast, when we placed the inspiration-synchronized VMN at the inlet of the humidifier in our study, we found that the inhaled dose was comparable to when the nebulizer was placed near the ETT. This is likely due to the large storage volume (∼1 L) of the inspiratory limb circuit and the humidifier chamber, which allows the aerosols generated during the inspiration phase to be stored and delivered during the subsequent inspiration. Similarly, placing the continuous VMN near the ventilator is beneficial, as the circuit and the humidifier chamber act as reservoirs to store aerosols generated during the exhalation phase. 5 Conversely, placing the continuous VMN close to the airway results in aerosol wastage, as aerosols generated during exhalation migrate to the expiratory limb due to trigger or bias flow. This rationale may explain the greater differences in inhaled doses observed with continuous VMN placements compared to inspiration-synchronized VMN placements. Further studies are needed to investigate whether other ventilator settings (e.g., tidal volume, inspiratory flow, and bias flow) would generate such small differences in inhaled doses with different nebulizer placements when using inspiration-synchronized VMNs.
We observed a significant, though relatively minor, increase in the inhaled dose with the small-particle VMN compared to the conventional VMN, particularly when the inspiration-synchronized mode was used. This finding suggests that the difference in the inhaled dose due to smaller aerosol particles is less influential than the effect of inspiration-synchronization in this adult model. These results imply that other factors besides impactive losses may play a role, warranting further research.
While inspiration-synchronized VMN has been available with limited ventilator options (Galileo ventilator, Hamilton Medical, Bonaduz, Switzerland), 11 the parameters tested (aerosol delivery during first 50% of inspiration and small particle VMN) are not commercially available, they have been actively used in drug/device investigations with adults.8,9,14 Our findings show promise for improving aerosol delivery during adult mechanical ventilation. Typically, the conventional jet nebulizer used during mechanical ventilation delivers an inhaled dose of 5%–12%, while conventional VMN delivers 22%–27%.15,16 In contrast, we found significant improvement in aerosol delivery efficiency, achieving an inhaled dose of up to approximately 60%. This high inhaled dose might increase the applications for aerosol therapy with other medications, providing possible advantages for local pulmonary targeting over systemic routes, such as direct delivery, shorter onset time, and lower doses. This is particularly crucial for drugs that demonstrate ototoxicity or nephrotoxicity when delivered systemically, such as Tobramycin and Amikacin, or drugs that require high concentration in the lung, such as Colistin. 17 However, it is important to note that the nebulization duration is nearly three times longer when using the inspiration-synchronized VMN compared to the continuous VMN. 18 Although VMN does not require additional external gas to drive aerosols, and its use does not directly affect ventilation, the longer administration time might not be beneficial for drugs that are concentration-dependent with a short duration of action, due to a longer time to reach maximum concentration in the airways. 17 However, it might be advantageous for time-dependent drugs or those requiring prolonged use, such as inhaled pulmonary vasodilators. 19 Future in vivo studies are needed to validate these effects. While the administration duration could potentially be shortened by increasing the aerosol delivery time, however, this reduction could impact the aerosol deposition, and the optimal aerosol delivery time requires further investigation.
Our study has several limitations. We used only one ventilator setting with one patient condition in our study, and results might vary with other settings, breathing patterns, and respiratory mechanics such as obstructed or restricted patterns.20,21 In addition, we did not evaluate scenarios involving spontaneous breathing effort, which could affect aerosol distribution in the lungs. As such, our findings may not be fully applicable to clinical cases with spontaneous breathing. Incorporating models that simulate spontaneous breathing efforts or varying lung compliance, along with a broader range of ventilator settings and humidification levels, would make the findings more generalizable. Further studies are needed to investigate aerosol delivery in these scenarios. We directly connected the ETT to the Y-piece without an in-line suction catheter, which is commonly used in clinical practice and has been shown to reduce aerosol deposition by 5%–6%. 21 The impact of an in-line suction catheter when using an inspiration-synchronized VMN is still unknown. Lastly, Kadrichu et al. reported a reduction in the inhaled dose with the use of active exhalation humidification in their in vitro study investigating inspiration-synchronized VMN during mechanical ventilation. 20 This suggests that our results with our model without active exhaled humidification might overestimate the actual inhaled dose to the lungs. Future clinical studies, particularly those focusing on drug absorption, therapeutic effectiveness, time to clinical response, and clinical outcomes such as improved oxygenation or reduced duration of ventilation, are needed to confirm the benefits of using inspiration-synchronized VMNs.
Conclusion
During aerosol delivery via VMN in mechanically ventilated adults, the inspiration-synchronized VMN generated 1.4 to 3.6 times higher inhaled doses compared to the continuous VMN. VMNs that produce smaller aerosol particles delivered 8%–69% higher inhaled doses than conventional VMNs (Solo), especially during continuous aerosol delivery. The inspiration-synchronized VMN achieved the highest delivery when placed close to the airway, whereas the continuous VMN delivered the most when positioned near the ventilator.
Footnotes
Acknowledgment
The authors wish to thank Aerogen Pharma for generously donating the prototype vibrating mesh nebulizers used in this study.
Authors’ Contributions
J.L.: Conceived the study and designed the research, analyzed and interpreted the data. S.A.S. and O.A.: Conducted the experiments under J.L. supervision. J.B.F.: Provided technical support for nebulizer use. J.L. and C.A.S.: Drafted the article, with revisions from O.A., and J.B.F. All authors reviewed and approved the final version of the article.
Author Disclosure Statement
J.L. discloses research funding from MEKICS Co. Ltd, Vincent Ltd, COPD Foundation, and American Association for Respiratory Care, and speaker fees from American Association for Respiratory Care, Aerogen Ltd, Heyer Ltd, Vincent Ltd, and Fisher & Paykel Healthcare Ltd. J.L. is also the section editor of RESPIRATORY CARE. J.B.F. is the Chief Science Officer for Aerogen Pharma Corp. Other authors have no conflict to disclose.
Funding Information
No funding was received for this article.