
Abstract
Backgroud:
A key attribute in selecting an oral inhaler device for chronic obstructive pulmonary disease (COPD) and asthma is its ability to dispense a high degree of pulmonary deposition of the drug at low inspiratory flows.
Methods:
In this study, the lung deposition of extrafine formulations of beclomethasone dipropionate (BDP) and formoterol fumarate (FF) (pressurized metered-dose inhaler [pMDI] and dry powder inhaler [DPI], NEXThaler) was compared with that of nonextrafine formulations of fluticasone/salmeterol (FP/SAL) Diskus DPI and budesonide/formoterol (BUD/FF) Turbuhaler DPI in 10 patients. Diskus intrathoracic (peripheral and central) lung deposition was estimated at low inhalation flow rates (30 and 40 L/min) via validated functional respiratory imaging (FRI) and computational fluid dynamics (CFD) methods.
Results:
The BDP/FF NEXThaler and BDP/FF pMDI had the highest median percentages of intrathoracic deposition, with consistent mean values of approximately 50% and 40%, respectively. The median percentage of peripheral deposition from extrafine inhalers was above 30% with BDP/FF NEXThaler and pMDI, 5% or less with the FP/SAL Diskus at both flow rates, and ranged between 12% and 22% with the BUD/FF Turbuhaler DPI at flow rates of 30 and 40 L/min, respectively.
Conclusions:
Extrafine BDP/FF using NEXThaler and pMDI resulted in greater peripheral deposition of both the inhaled corticosteroid and long-acting beta-agonists moieties than the nonextrafine FP/SAL Discus and BUD/FF DPIs did.
Introduction
Increasing amounts of data suggest that small airway involvement can contribute to the clinical manifestations of asthma. Inflammation, remodeling, and changes in the surrounding tissue can impact small airways, thereby contributing to their malfunction. 1 Device-dependent inhalation technique training may be ineffective in everyday clinical practice; 2 this ineffectiveness, along with less-than-ideal therapy adherence, 3 may impact the daily efficacy of therapy.
The importance of peripheral lung deposition of inhaled medication in asthma treatment is becoming more widely acknowledged because of the critical role that small airway dysfunction (SAD) plays in this disease. 4 Multiple function tests are needed for the appropriate diagnosis of SAD in patients with asthma, as verified by the cross-sectional phase of the ongoing Assessment of Small Airways Involvement in Asthma (ATLANTIS) cohort study. 5 Furthermore, ATLANTIS revealed that SAD is present at all asthma severity levels, emphasizing the importance of focusing on the peripheral lung to achieve the best possible asthma control.6,7 To achieve effective lung penetration for asthma treatments, we need to consider many factors, such as an individual approach for each patient and a wide variety of inhaler features. 8 These factors determine the quality of aerosol clouds. 9 Deposition (the amount of medicine that reaches and deposits in the airways) is determined by the particle size, shape, and density, as well as the structure of the lungs and respiratory characteristics (e.g., flow and inhaled volume).10,11
SAD plays a significant role in asthma; thus, peripheral deposition of inhaled medication is critical. 9 The Global Initiative for Asthma (GINA) 2023 recommendations regarding low, medium or high inhaled corticosteroid (ICS) doses indicate differences in doses for fine (mass median aerodynamic diameter; [MMAD], 2–5 µm) and extrafine (MMAD <2 µm) ICS particles. 3
Extrafine inhaled medicines have an MMAD <2 µm. Inhaled medications penetrate the peripheral airways because of their particle size; there is more deposition of smaller, extrafine particles than of nonextrafine particles. 12
Drug deposition in peripheral (P) airways reportedly differs between pressurized metered-dose inhalers (pMDIs) and dry powder inhalers (DPIs). 13 The efficiency of drug delivery is highly dependent on the inhalation flow rate. 14 For example, when inhalation is performed at 30 L/min, only approximately 15% of the delivered dose (DD) may reach the lungs, whereas greater quantities of the drug can be effectively deposited at higher rates. Thus, improving the deposition at low flow rates can enhance therapeutic outcomes for asthma patients.
The particle size of an ICS may affect airway drug deposition and effectiveness. A systematic review and meta-analysis of seven observational real-life studies with 33,453 patients revealed that extrafine ICSs have significantly higher probabilities of achieving asthma control with reduced exacerbation rates at significantly lower prescription doses than nonextrafine particle ICSs. 15
Functional respiratory imaging (FRI), which combines high-resolution computed tomography with computational fluid dynamics (CFD) methods, has been validated,16,17 and is now used to estimate airway deposition of inhaled medicines. 18 This imaging technology is used for the analysis of drug deposition without actual drug inhalation on the basis of airway images from computerized tomography (CT) and FRI, and uses factors such as drug particle size and inhalation flow rate.17,19–22 This methodology can assess central (C) and P drug deposition. Notably, the FRI method was identified by the Food and Drug Administration as an “important tool to investigate regional drug deposition of the intrathoracic region, especially to measure the effects of small-airway variability.” 23
The FRI was also used to assess the degree of lung deposition of extrafine triple therapy beclomethasone dipropionate (BDP)/formoterol fumarate (FF)/glycopyronium bromide (GB) and extrafine BDP/FF administered via pressurized metered-dosage inhalers. The results were compared with gamma scintigraphy data. FRI revealed that extrafine BDP/FF/GB and BDP/FF had similar deposition patterns, with both formulations showing substantial lung deposition. 18
Watz and colleagues used the FRI methodology to compare lung deposition at different mean flow rates (30, 40, and 60 L/min) of three inhaled fixed combinations of ICS/long-acting beta-agonists (LABA) delivered by DPI: NEXThaler® and pMDI, (extrafine BDP/FF pMDI), Relvar Ellipta® (FluF/VI), and Symbicort Turbuhaler® (budesonide/formoterol, BUD/FF DPI). Their results showed that NEXThaler® allows for better peripheral deposition and C/P ratios of ICS/LABA than Ellipta®does; furthermore, NEXThaler® demonstrated an inspiratory flow rate that was independent of lung deposition compared with Turbuhaler®, suggesting that the extrafine formulation is superior to large particle formulations in delivering ICS/LABA consistently both to the large and small airways. 9
In this study, we used FRI to evaluate the lung deposition and the C/P distribution pattern in adults with moderate to severe asthma via four fixed-dose combination ICS/LABAs: extrafine [ef BDP/FF pMDI and ef BDP/FF DPI], nonextrafine budesonide/FF via Turbuhaler [BUD/FF DPI] and nonextrafine fluticasone propionate/salmeterol via the DISKUS [FP/SAL DPI] f at two low flow rates (30 and 40 L/min).
Materials and Methods
Patients
Patients were selected from the Fluidda database according to the following inclusion criteria:
presence of asthma , nonsmokers (never smoked or not smoked for >12 months with <1 pack-year history (pack years = (cigarettes per day smoked/20) × number of years smoked), ability to withhold from using short-acting bronchodilators for 6 hours and long-acting bronchodilators for 12 hours before the study assessments; no history of acute respiratory disease within 4 weeks before inclusion; no history of any other inflammatory lung condition or carcinoma of the lung; and no exacerbation of disease requiring hospitalization within the previous 4 weeks.
The exclusion criteria were as follows:
pregnancy; past or present disease that, as judged by the investigator, would affect subject safety or influence the outcome of the study; presence of both asthma and COPD; history of alcohol or drug abuse; history of claustrophobia; and respiratory tract infection within 4 weeks of the start of the study.
All CT scans utilized by FLUIDDA were acquired through Ethics Committee-approved clinical trials. The scans were fully anonymized, disease severity and demographics were recorded, and FRI parameters, such as lung and airway volumes, were extracted to enable 3D lung quantification. These derived, anonymized FRI parameters, essential for performing CFD analyses, are part of FLUIDDA’s IP. Quantification of FRI parameters (e.g., lobar volumes, airway volumes) are prerequisite for conducting CFD studies.
Characteristics of the selected patients
A total of five males and five females with moderate or severe asthma were selected for inclusion in this study on the basis of the Fluidda data. The severity of asthma in these patients was determined by a medical expert based on the BTS guidelines. The patients’ ages ranged from 21 to 64 years, their BMIs ranged from 20.21 to 30.71 kg/cm,2 and their FEV1 percentage values ranged from 66.03% to 126.25% (Table 1).
Demographic and Clinical Characteristics of the Subjects
BMI, body mass index; FEV, forced expiratory volume; FVC, forced vital capacity.
All relevant institutional review boards approved this study. All patients provided signed informed consent to undergo CT for the evaluation of their functional residual capacity and total lung capacity.
Methods
CT data were used for segmentation, and CFD simulations with automatic segmentation were performed up to the point where no distinction was possible between the intraluminal and alveolar air. The segmented airway tree was converted into a 3D model that was smoothed via a volume compensation algorithm. The smoothed model was then trimmed perpendicular to the centerline at each terminal bronchus. The remaining artifacts in this model, due to noise in the CTs, were manually removed (Fig. 1).
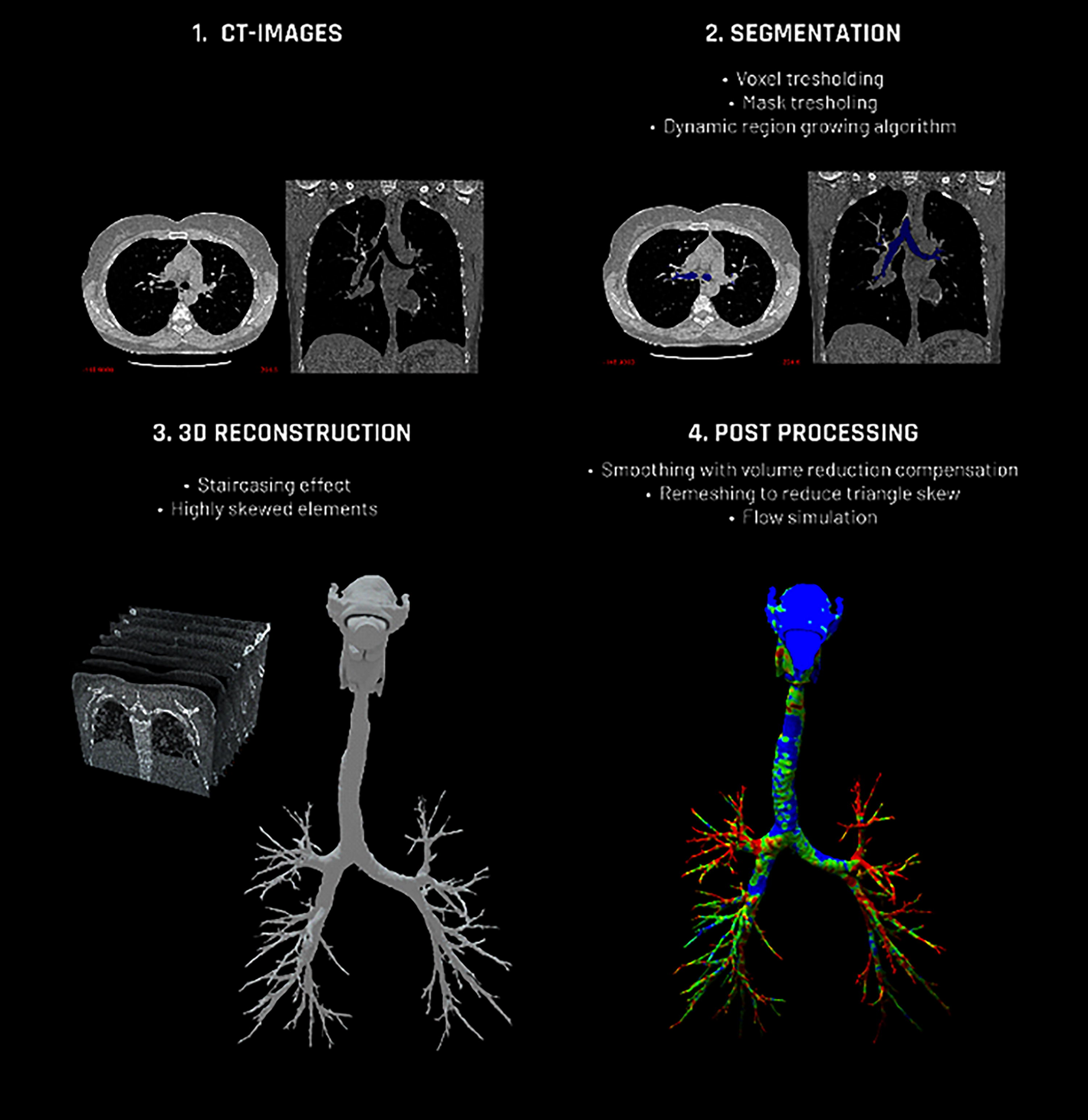
Segmentation workflow. CT, computerized tomography.
The lung deposition of ef BDP/FF delivered through the pMDI and the NEXThaler DPI was then compared with the lung deposition of nonextrafine FP/SAL delivered via the Diskus DPI and nonextrafine BUD/FF delivered via the Turbuhaler DPI.
The behavior of the air and particles passing through the inhaler, mouth, and airways of every patient was simulated via CFD to determine where the particles were deposited in the respiratory system via the Watz method. 9
Deposition calculations
The particle deposition was simulated by injecting solid particles with diameters ranging from 0.9 to 30 µm. The particles were considered inert via one-way coupling between the particles and the air, which allowed only momentum transport from the flow to the particles. The interactions between particles were negligible. Sufficient particles of each diameter were injected to avoid changes in the percentage of deposition. An appropriate mass was then assigned to these particles during post processing. The DD was calculated in the following manner: first, the deposition as a percentage of the DD for each API was calculated, and then the average value for the APIs was obtained.
Different inhalation rates of 30 L/min and 40 L/min were used for the MDIs and DPIs (Table 2).
Inhalation Profiles
DPIs, dry powder inhalers; MDIs, metered-dose inhalers.
CFD simulations were performed through the following strategy:
Inert particles represented the discrete phase. The percentage of flow exiting the model toward a lobe equaled the relative lobar expansion obtained from the patient-specific inspiratory and expiratory CT scans. Transient boundary conditions (inhalation profile). No-slip conditions were applied to the airway walls. Particles were trapped when hitting the wall.
As there was no flow at time zero, the domain was initialized at atmospheric pressure and zero velocity.
Using the MMAD, geometric standard deviation (GSD), and fine particle dose value, a lognormal distribution was fitted for each dataset. The MMAD divided by the GSD and the MMAD multiplied by the GSD represent the 16th and 84th percentiles of the cumulative distribution.
The airflow distribution has been assumed to be constant throughout the breathing cycle because the percentage of flow exiting the model toward a lobe has been considered the relative lobar expansion obtained from patient-specific inspiratory and expiratory scans.
Statistics
All the statistical analyses were conducted via RStudio (The R Foundation for Statistical Computing, Vienna, Austria) version 3.2.5 or higher. In the boxplots, the extremes of the box represent the quartiles, and the black line represents the median. The whiskers extend to the most extreme data point, which is no more than 1.5 times the interquartile range from the box. All the data points outside this range (outliers) are visualized as individual points. Continuous variables are presented as the means ± standard deviations.
The deposition of particles (percentage of the DD) was investigated for the intrathoracic, C, and P regions and the C/P ratio. The analysis of the deposition parameter [%] of DD in relation to the administered drug, the site of drug deposition in the lungs, the flow rate, and the type of inhalation device. Two three-factor analyses of variance (ANOVA) with repeated measures were conducted, where the patient ID was included as a random factor, separately for each drug. Except three independent variables, the interactions between the mentioned variables were used as well. The ANOVA results were supplemented with post hoc tests, conducted using paired t-tests with Bonferroni correction for multiple comparisons. The analyses included the comparisons of flow rates of 30 L/min and 40 L/min (separately and combined) and the comparisons of inhalation devices within each flow rate group.
Results
Particle characteristics
During the postprocessing of raw results obtained from the simulation, it was possible to assign certain characteristics (MMAD, GSD, fine particle fraction [FPF], and DD) to the particles that had been injected in the simulation, both at 30 and 40 L/min, to evaluate the mass corresponding to each particle size (Table 3).
Particle Characteristics
BDP/FF pMDI, beclomethasone dipropionate/formoterol fumarate pressurized metered-dose inhaler; BUD/FF, budesonide/formoterol fumarate; DD, delivered dose; DPI, dry powder inhaler; FP/SAL, fluticasone/salmeterol; FPF, fine particle fraction; GSD, geometric standard deviation; ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; MMAD, mass median aerodynamic diameter.
Deposition (% of delivered dose)
The mean percentage of intrathoracic deposition of the DD was consistently approximately 50% with NEXThaler and approximately 40% with pMDI. The intrathoracic depositions of Turbuhaler were lower at 30 L/min than at 40 L/min, and those with Diskus never exceeded 11 (Fig. 2).
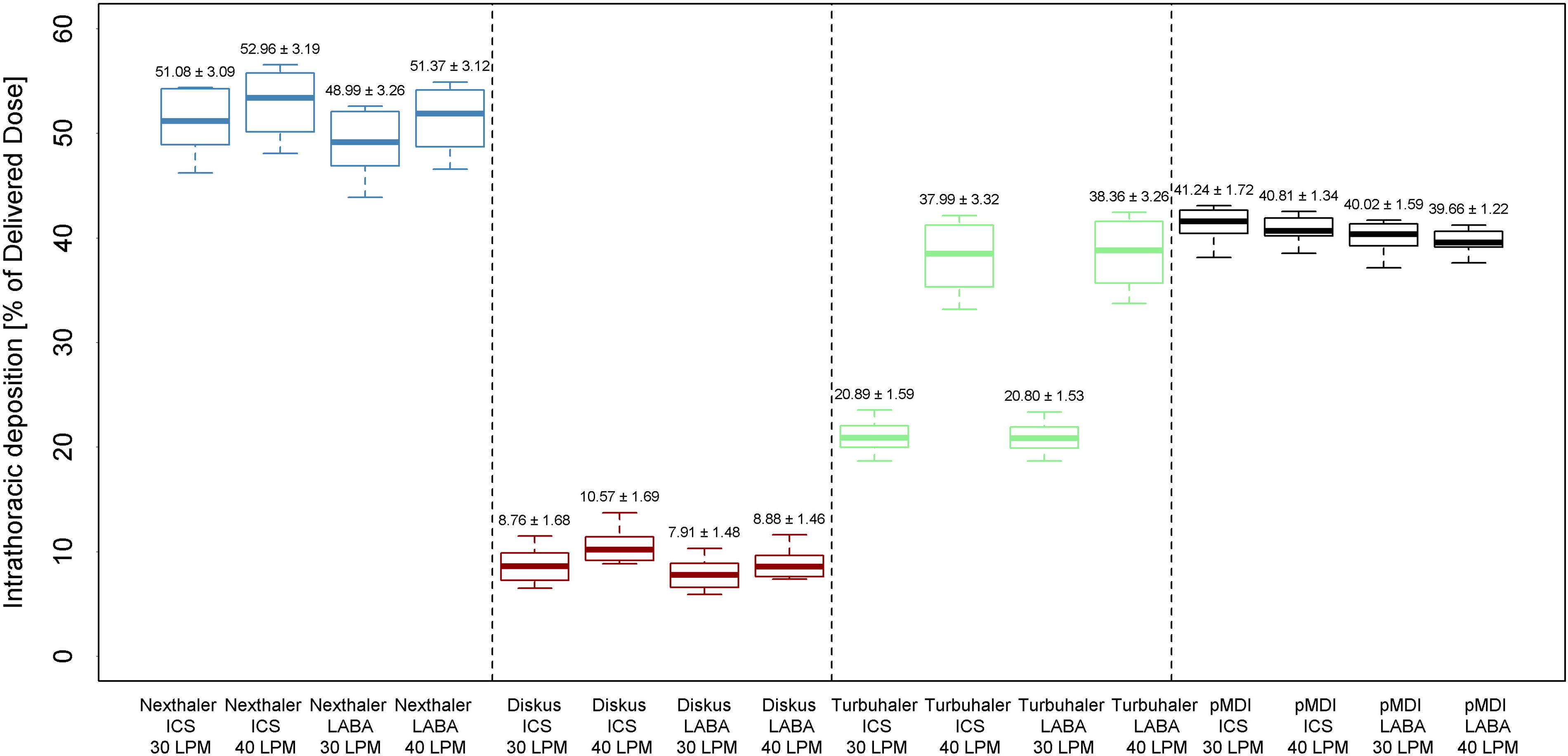
Intrathoracic deposition (percentage of deliveres dose). ICS, inhaled corticosteroids; LABA, long-acting beta-agonists.
Similarly, NEXThaler had the highest mean percentage of C deposition, with mean values consistently above 17%, and extrafine pMDI had a deposition rate of approximately 10% at all flow rates and with all products. The C deposition of Turbuhaler depended on the flow rate: for the ICS, it was 8.4% at 30 L/min and 15.9% at 40 L/min. Similar flow dependencies at low flow rates through the Turbuhaler device were observed for LABA (8,3% for 30L/min and 15.9% for 40L/min). Additionally, the percentage of DDs of both ICS and LABA was consistently less than 5% with Diskus, regardless of the flow rate (Fig. 3). Both intrathoracic and C depositions with NEXThaler DPI were significantly higher at both flow rates than with Turbuhaler DPI, Diskus DPI and Foster MDI for both ICS and LABA (Supplementary Appendix).
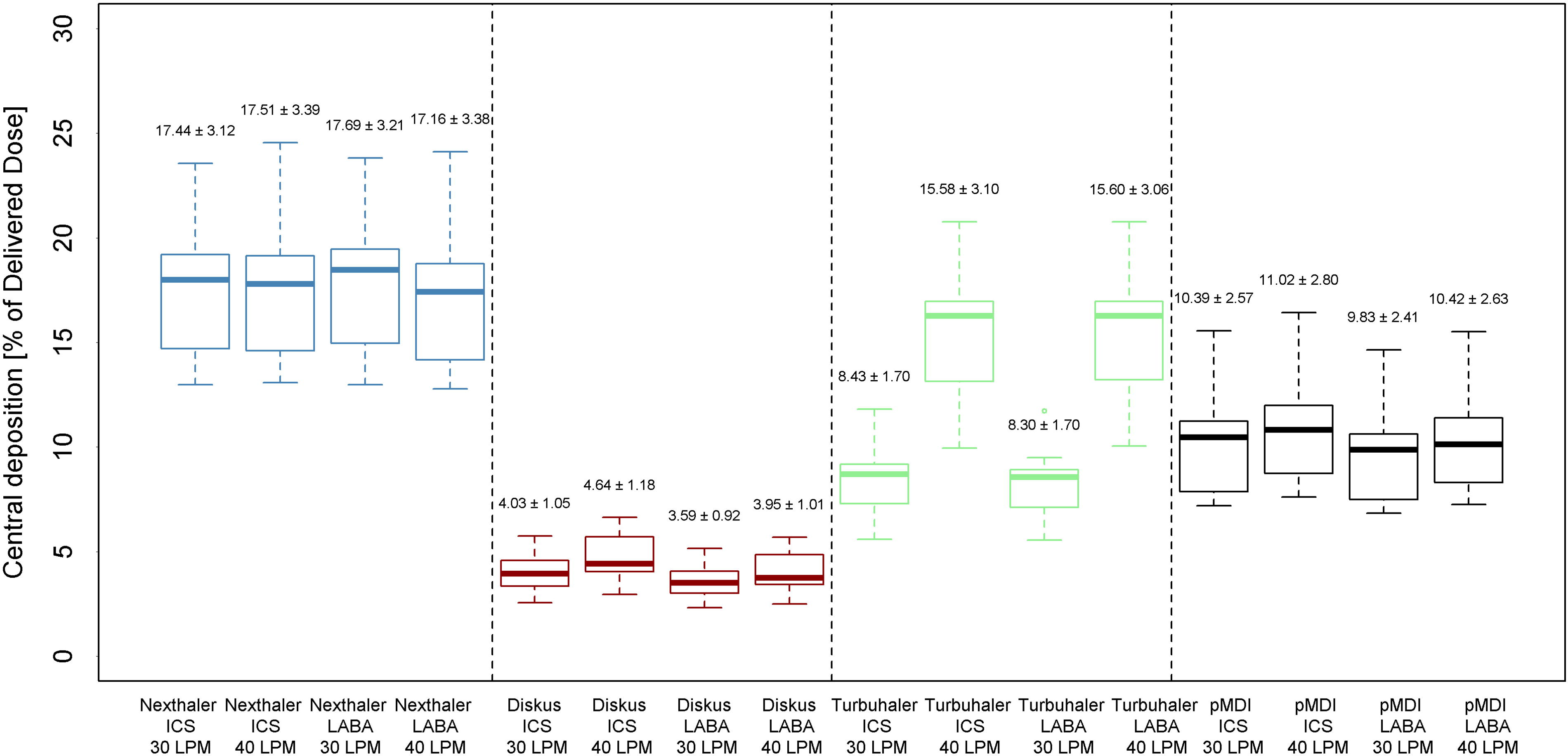
Central deposition (percentage of delivered dose). *p < 0.001 versus all other devices. ICS, inhaled corticosteroids; LABA, long-acting beta-agonists.
The mean P deposition showed similar trends to those observed for C and thoracic depositions, with higher and consistent percentages of depositions with extrafine NEXThaler and Foster MDI, inconsistent depositions with Turbuhaler, and lower deposition rates with Diskus (Fig. 4). P deposition with NEXThaler DPI were significantly higher at both flow rates than with Turbuhaler DPI, Diskus DPI while they were similar to the ones observed with Foster MDI for both ICS and LABA (Supplementary Appendix).
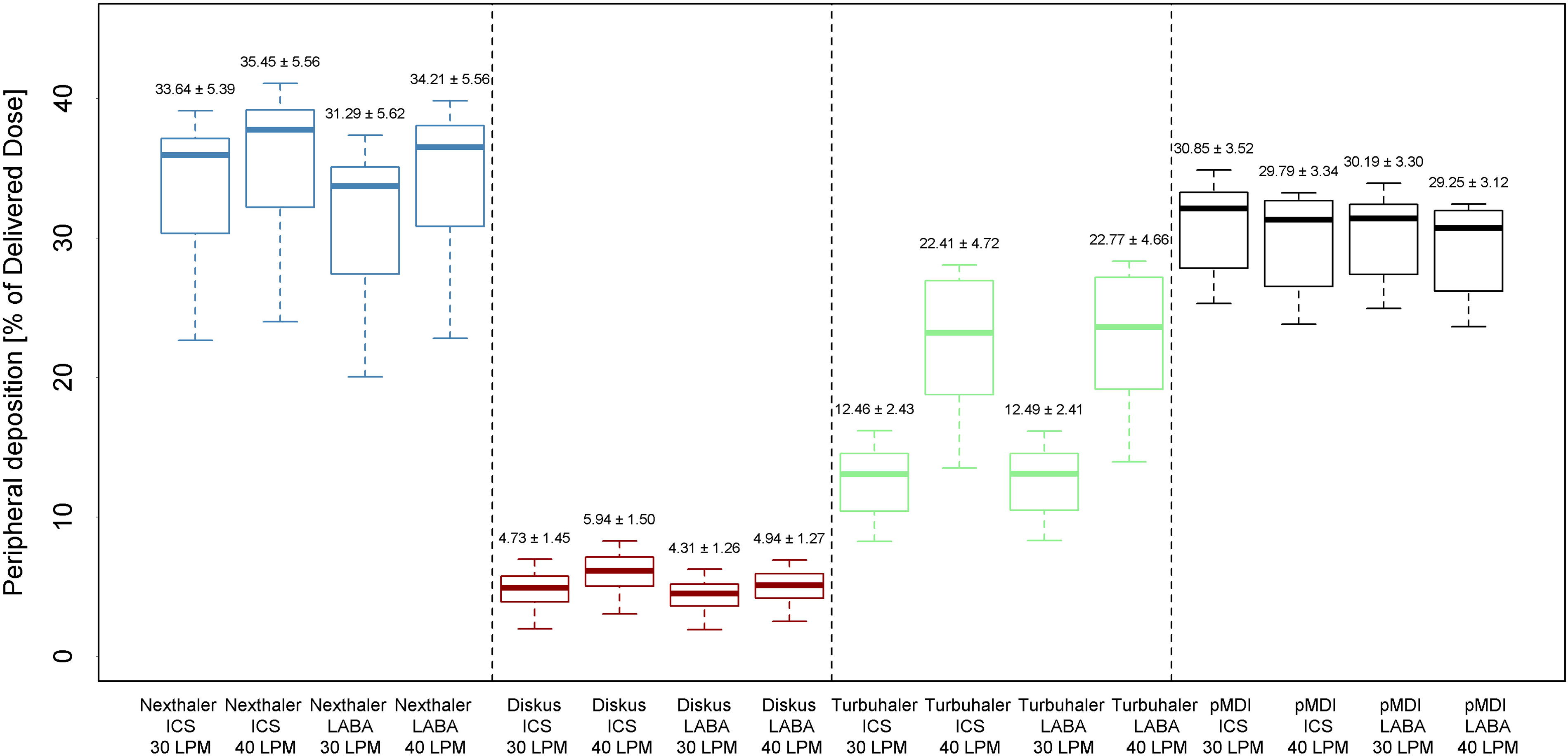
Peripheral deposition ratio (considering both ICS and LABA). ICS, inhaled corticosteroids; LABA, long-acting beta-agonists.
The mean C/P deposition ratio ranged from 0.383 ± 0.146 when the administration was performed at 40 L/min flow with extrafine pMDI to 0.971 ± 0.540 when the administration was performed at 30 L/min flow with Diskus (Figs. 5 and 6). None of these values resulted statistically different between the different inhalers at any flow rate both for ICS and LABA.
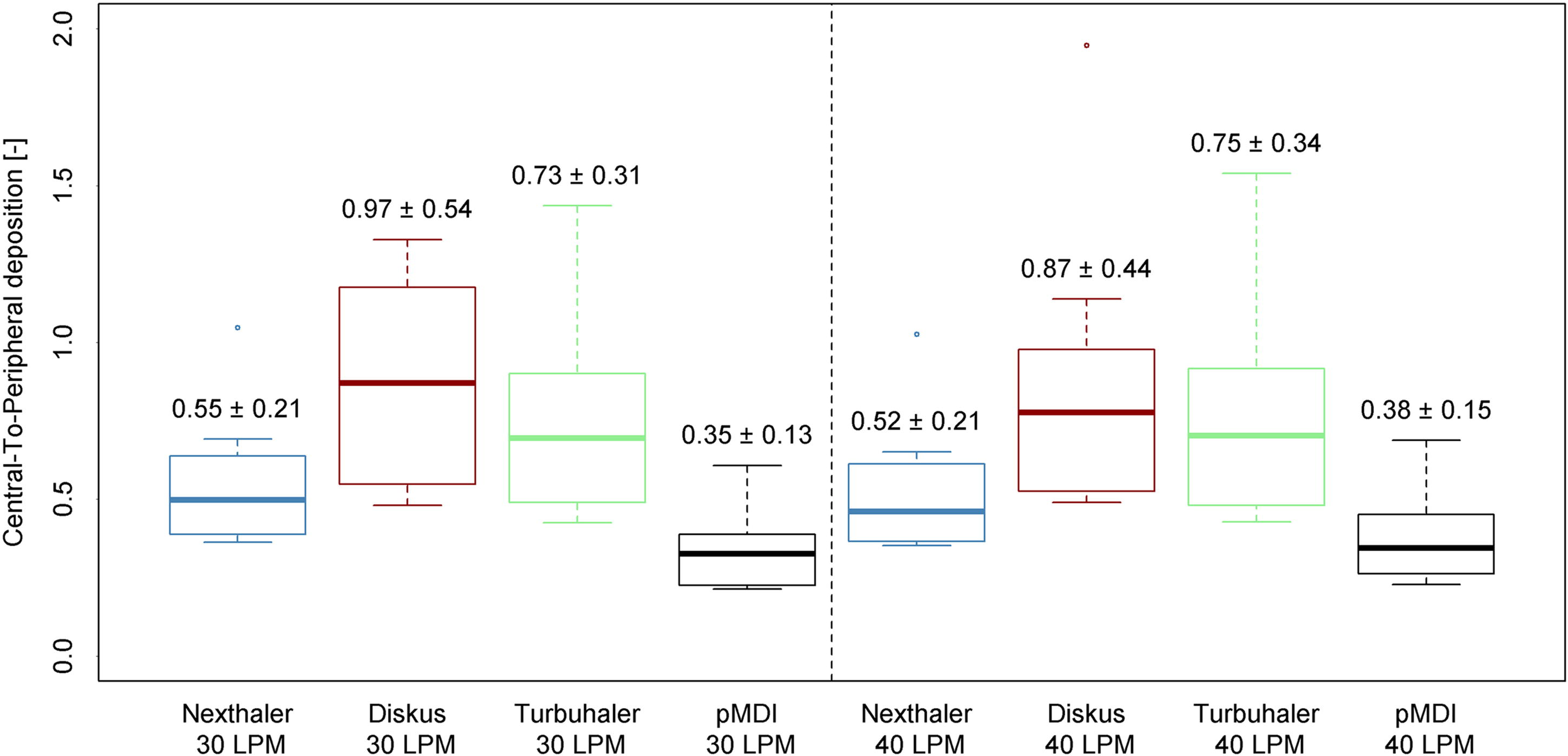
Central to peripherial deposition ratio. BDP, beclomethasone dipropionate; FF, formoterol fumarate; GB, glycopyronium bromide.

Example of deposition.
Conclusions
The results of this work confirm that patient-specific CFD simulations with adequate boundary conditions provide information that is similar to that acquired with functional imaging methods, such as SPECT/CT, 16 without the need to expose patients to any radioactive compounds.
Flow simulations were performed for the ICS and LABA components delivered through one pMDI and three DPIs in patients with moderate and severe asthma. The airway geometries of each patient were coupled to all devices. The simulations were performed with idealized inhalation profiles with mean flow rates of 30 L/min and 40 L/min. In the present study, the deposition pattern in the lungs confirmed drug dispersion throughout the airways, including both large and tiny drugs, as reported in previous similar studies 16 as well as when different inhalation systems were investigated.
Researchers have previously explored the lung deposition and distribution patterns of the fixed combination of BDP and FF (BDP/FF 100/6 µg) delivered as an extrafine dry powder formulation (MMAD [µm] BDP = 1.5; FF = 1.4) through the NEXThaler device in healthy subjects, patients with asthma, and chronic obstrutive pulmonary disease (COPD) patients using FRI. The fixed extrafine dry powder combination BDP/FF (100/6 µg) administered through the DPI NEXThaler achieved similar intrapulmonary deposition in healthy subjects, asthmatic patients, and COPD patients (approximately 55% of the emitted dose), regardless of the underlying lung disease, with a negligible number of exhaled particles. 16
An adequate dosage of ICS can reduce the risk of severe exacerbations, whereas an adequate distribution of ICS/LABA can ensure symptom relief, as suggested by the GINA recommendations.3,24 Brownian diffusion is the primary mode of deposition of aerosols <0.5 µm, while sedimentation is the primary mode of deposition for other small particles. Impaction-induced deposition in extrathoracic airways and at locations of blockage in the asthmatic or COPD lung is thus significantly smaller than that of larger medication particles. 11 Consequently, extrafine formulations ensure a uniform distribution of active medicines throughout the entire bronchial tree, regardless of the pathophysiological condition. 16
These data confirm the previously investigated inspiratory flow rate independence of extrafine NEXThaler lung deposition versus that with Turbuhaler. 9 The results of our study show that the administration of both ICS and LABA with NEXThaler and extrafine pMDI ensured that higher peripheral and central deposition rates would result.
The percentage of deposition observed after Diskus inhalation was consistently the lowest across the entire respiratory tract compared to other devices for all the investigated products. The C/P deposition was similar at the different flow rates with all the investigated devices, both for ICS and LABA. Compared with Turbuhaler, extrafine NEXThaler and extrafine pMDI demonstrated inspiratory flow rates that were independent of the low PIF range of lung deposition. NEXThaler and extrafine pMDI, in contrast with Turbuhaler, yielded markedly higher deposition at lower flow rates, allowing more efficient DPI administration of an extrafine formulation than nonextrafine formulations in delivering ICS and LABA consistently not only to the central airways but also to the peripheral airways.
The present findings are very important because this study is the first to compare extrafine BDP/FF pMDI and DPI versus nonextrafine FP/SAL Diskus DPI and nonextrafine BUD/FF Turbuhaler DPI.
Limitations
The results of this study should be interpreted with caution because the data on the particle size distribution of each drug were generated from imaging data in the FRI model, which were expressed numerically as the number of monodispersed particle sizes and the flow rate. Furthermore, this approach offers poor spatial resolution of the lung, and static volume distribution is a limitation of FRI technology. 19 Another limitation is that the study modeled the airways of patients with moderate and severe asthma and not patients with very severe asthma, in which low PIF is commonly observed.
Finally, our findings confirm the greater peripheral lung deposition of ICS and LABA with the extrafine BDP/FF NEXThaler DPI and pMDI, even at the low end of inspiratory flow rates of 30 and 40 L/min., It is consistent with previous observations showing that the NEXThaler breath-actuated mechanism can also be activated by patients with severe asthma, 9 resulting in increased peripheral lung deposition of both ICS and LABA. Furthermore, these results confirm that FRI-based evaluation is a reliable method for modeling particle distributions, as both components are deposited throughout the thoracic and peripheral airways, which increases the possibility for synergistic interactions.
Footnotes
Acknowledgments
Fluidda (FLUIDDA NV, Groeningenlei 132, 2550 Kontich, Belgium) was responsible for including the patients, data collection, and statistical analyses. The authors thank Andrea Rossi for the medical writing support and the Chiesi and Fluidda study team for managing the study.
Authors’ Contributions
M.K. contributed to the conceptualization, methodology, investigation, and writing—review and editing. M.P. contributed to the conceptualization, methodology, investigation, and writing—review and editing. W.D.B. contributed to the conceptualization, methodology, investigation, and writing review—editing. H.S. contributed to the conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing—review and editing, and visualization. M.W. contributed to the conceptualization, resources, project administration, and funding acquisition. T.D. contributed to the conceptualization, resources, writing—original draft, project administration, writing—review and editing, supervision, and funding acquisition. All the authors have full access to all of the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Ethics Approval and Consent to Participate
All CT scans utilized by FLUIDDA were acquired through Ethics Committee-approved clinical trials (Institutional Review Board at University Hospital Antwerp, Drie Eikenstraat 655, 2650 Edegem).
All patients provided their informed consent to collect their respiratory tract characteristics used to perform this study.
Data Availability Statement
The data that support the findings of this study are available from Hosein Sadafi (Fluidda), but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available. Data are not available without the permission of
Author Disclosure Statement
M.K. received speaker fees from AbbVie, Adamed, AstraZeneca, Berlin Chemie, Chiesi, EMMA, GSK, Hal Allergy, HVD, Lek-Am, Polpharma, Teva, Sanofi, Zentiva, participates on advisory boards for AbbVie, AstraZeneca, Chiesi, GSK, Pfizer, and Sanofi, and is a president of the Polish Society of Allergology. M.K. is also an employee of Chiesi Poland Sp. z o.o. M.P. received payment or honoraria for lectures, presentations, speakers bureaus, article writing or educational events from Astra-Zeneca, Boehringer Ingelheim, Chiesi, GSK, Elpen, Guidotti, Menarini, Specialty Therapeutics. Support for attending meetings and/or travel from Astra-Zeneca, Sanofi, Chiesi, GSK, Novartis, Zentiva, Boehringer Ingelheim. H.S. is an employee of Fluidda. W.D.B. has received grants from AstraZeneca, Chiesi, and GlaxoSmithKline. T.D. is an employee of Chiesi Poland Sp. z o.o.
Funding Information
All the activities were funded by Chiesi Poland Sp. z o.o., Warszawa (Poland). Grant number CHI-PL-FOS-02.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.