
Abstract
Inhalation of liposomes formulated with phospholipids similar to endogenous lung surfactants and lipids offers biocompatibility and versatility within the pulmonary medicine field to treat a range of diseases such as lung cancer, cystic fibrosis and lung infections. Manipulation of the physicochemical properties of liposomes enables innovative design of the carrier to meet specific delivery, release and targeting requirements. This delivery system offers several benefits: improved pharmacokinetics with reduced toxicity, enhanced therapeutic efficacy, increased delivery of poorly soluble drugs, taste masking, biopharmaceutics degradation protection and targeted cellular therapy. This section provides an overview of liposomal formulation and delivery, together with their applications for different disease states in the lung.
Liposomes for Inhalation
Liposomes are small spherical vesicles produced from a variety of phospholipids and cholesterol components that are similar to the lipids naturally present in the human lung. The highly organized structures of liposomes consisting of one or multi-concentric lipid bilayers with an inner aqueous compartment to enable the incorporation of hydrophobic, hydrophilic or amphiphilic substances. 1 Due to their versatility and biocompatibility, they are commonly used as universal drug carrier systems in the cosmetic and pharmaceutical industry.
Inhalation drug delivery is a well-established means of drug administration for both localized treatment of lung diseases and systemic delivery of therapeutics. The therapeutic efficacies of inhaled therapies are determined by the deposited dose, regional deposition and absorption across the lung epithelial barrier. Locally acting drugs should ideally be maintained within the lungs for a sustained period of time, as absorption into the circulation may reduce efficacy. Generally, drugs for local delivery aimed to treat respiratory diseases such as asthma, cystic fibrosis and chronic obstructive pulmonary disease (COPD) are delivered to the tracheobronchiolar region of the lung. Since they are delivered at a much lower dose compared to systemic therapy, aerosol therapy results in reduced systemic side effects and rapid clinical response locally that have either similar or superior therapeutic effects. 2 Conversely, the rate of absorption into the systemic circulation will dictate the onset of action and efficacy of the drugs targeted for systemic delivery. Rapid absorption could be achieved through delivery of the drug to the alveolar region, where there is a larger surface area and a thin layer of epithelial cells. 3 This could be particularly beneficial for drugs with poor oral bioavailability, high first pass metabolism or large macromolecules.
Recently, interest has increased in liposomes as an inhaled drug carrier system for both local treatments of respiratory diseases and systemic delivery due to their many benefits. Different inhaled therapeutics, including antimicrobial agents, cytotoxic drugs, asthma drugs, anesthetics, proteins and recombinant genes, have been reported to use liposomes as pulmonary drug carriers.
1
The potential benefits of combining liposomes with inhalation therapy include:
Solubilization of poorly soluble drugs; Modification of the release profiles of drugs to increase residence time within the lungs; Improved safety profiles by preventing local irritation to lung tissues or facilitation of drug solubility without the need for toxic solubilizing excipients; Protecting drugs from enzymatic or chemical degradation; Improved efficacy through enhanced activity against intra- and extracellular pathogens; Targeting selectivity to specific cell populations using surface bound antibodies or ligands; The use of biodegradable and biocompatible components.
Despite their advantages, there are several limitations of liposomal delivery systems. The major limitation is the short shelf life of lipid vesicles that limits the overall drug stability with leakage half-lives within hours of manufacture. 4 Instabilities of these liposomes mainly occur by chemical and physical processes. Physical instability of liposomes causes drug leakage from the lipid vesicles, and this problem mainly occurs in in vivo administration. 5 Stability of the liposomes is generally lower under physiological conditions due to the many interactions that can occur between the liposomes and body fluids. 5 This is particularly important for inhalation delivery, as liposomes must be delivered to the lung predominantly intact and must not rapidly release the drug once on the lung epithelia to protect the drug from degradation. Other aspects of physical instability are the aggregation and fusion of the liposomal vesicles leading to changes in size and subsequent therapeutic efficacy. 6 Conversely, chemical instability could occur through the hydrolysis of ester bonds or the oxidation of unsaturated acyl chains of the lipid components of the liposomes. 7 This type of instability mainly occurs in vitro and is dependent upon the lipid composition and storage conditions. To overcome some of these problems, low storage temperatures can help prevent hydrolysis as well as freeze-drying with cryoprotectant or addition of an antioxidant. 8 However, these stability enhancing methods in themselves cause inherent technical challenges such as cold chain storage or reconstitution reproducibility.
Structure and Properties of Liposomes
Structure
Liposomes are self-assembling structures that spontaneously form when lipids are suspended in excess of water, due to intrinsic interfacial chemistry forming one or more phospholipid bilayers surrounding a water space as colloidal dispersions. The vesicles are generally made up of natural or synthetic phospholipids, which could also have lipoproteins and range from 0.05–5.0 μm in size. Numerous techniques could be used for liposomal preparations that result in vesicles that are large unilamellar vesicles (LUVs, >100 nm), small unilamellar vesicles (SUVs, 25–100 nm) and multilamellar vesicles (MLVs) (Fig. 1). 9

Schematic of the different types of liposomes and a simple liposome vesicle that has a shell consisting of a lipid bilayer. A liposome can trap hydrophobic drugs ( × ) within the hydrophobic bilayer or amphiphilic drug (■) closer to the polar head-groups within the hydrophobic bilayer and hydrophilic drugs (0) in its larger interior.
There are other variations of liposomes that include targeted liposomes with monoclonal antibodies or lectins attached to the surface for specific receptor or cell interactions, stealth liposomes for engulfment avoidance and reactive liposomes that react to a specific environment or interaction encounter, such as change of pH. 2 Modification of the physicochemical properties of liposomes can be performed by changing several parameters that include 7 :
Types of lipids;
Composition and proportions of lipids;
Size of liposomes;
Charges on the liposomal surface;
Fluidity in the liposomal membrane, which can be controlled via addition of cholesterol or other additives;
Temperature and pH sensitivity.
The different composition of liposomes and their subsequent properties allow the encapsulation and delivery of a range of hydrophilic, hydrophobic and amphiphilic drugs, including nucleotides and peptides. The interior of the vesicles can be actively or passively loaded with hydrophilic drugs, while lipophilic drugs can be dissolved within the lipid bilayer or bound by ionic interactions to acidic or basic groups of the lipid component. 2
Size and lipid components of liposomes
The two important properties that could affect the stability of the liposomes are lipid composition and vesicle mean size. A series of studies have been performed to investigate the parameters that could affect the release of carboxyfluorescein from liposomes following nebulization.10–12 It has been demonstrated that a decrease in mean liposomal size results in a lower release rate of drugs. 13 However, the decrease in size of the liposome results in a reduction in entrapment efficacy. 12 Hence, the ratio of lipid to drug will be increased to deliver sufficient concentrations to the lungs for therapeutic efficacy, which could go beyond the patient's tolerability and may compromise the pharmacokinetics of a drug. 6 To add to the clinical constraints, the formulation would need to deliver an efficacious dose in a reasonable amount of time for patients to be compliant with their treatment regimen.
On the other hand, the lipid composition affects the fluidity/rigidity of liposomal membranes, surface charges and steric hindrance, which govern the stability of liposomes during nebulization and determine the liposomal interaction with biological components. 6 Hence, the nature of the liposomal-cell interaction determines the mode of intracellular delivery of liposomal drugs, as shown in Figure 2.
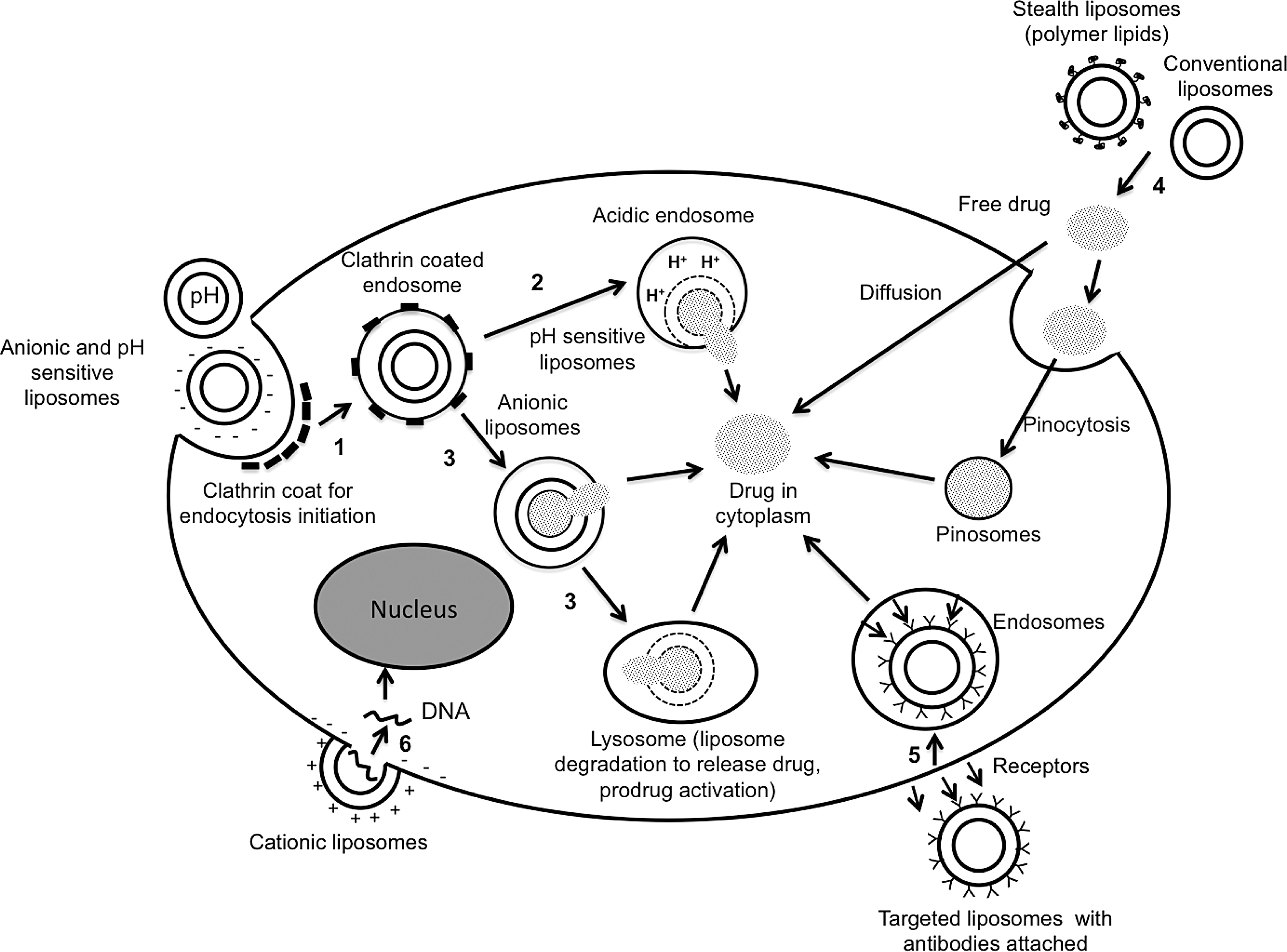
Schematic diagram of the predominant mechanisms of intracellular delivery of liposomal drug formulations. The different pathways include: 1) coated pit endocytosis of anionic and pH sensitive liposomes, 2) release of drug from pH sensitive liposomes within the acidic endosomes, 3) drug release from anionic liposomes through leakage into the endosome lumen or fusion with endosome membrane, 4) extracellular drug release from circulating liposomes, 5) receptor mediated endocytosis, and 6) fusion of cationic liposomes with cell plasma membrane (Modified from Sharma and Sharma 6 ).
It has been shown that neutral liposomes have reduced physical stability due to aggregation of the vesicles. 14 Furthermore, neutral liposomes do not interact well with cells, and as such, drugs mainly enter the cells after they are released from the liposomes into the extracellular environment. 15 Conversely, charged liposomes enhance intracellular uptake of drugs by target cells possibly through endocytosis (mainly negatively charged liposomes) or fusion with cell membranes (cationic liposomes).6,16–18
Cholesterol and other more rigid phospholipids, such as dipalmitoyl-phosphatidylcholine (DPPC) or distearoylphosphatidylcholine (DSPC), have been known to stabilize liposomes by increasing the rigidity of the liposomes thus enhancing their resistance to the sheer forces of nebulization. 19 However, the composition of lipids needs to be carefully considered as it also influences the phase transition temperature (Tc) of the lipid mixture.1,6 Increasing the Tc of the lipid mixture will result in higher drug stability during nebulization and also in vivo, as temperatures tend to be higher in these instances. On the other hand, lipid concentrations in the dispersion do not have an effect on the rate of drug release from the liposomes, up to a concentration of 50 mg/mL but affect the aerosol generated from the nebulizers.11,19 Hence, successful generation of liposomal formulations for inhalation will require the tailoring of liposome characteristics to the specific drug to be retained within the liposomes.
Liposomal preparation
Liposomal drug formulations will be useful only if sufficient therapeutic amounts of drugs together with reasonable amounts of lipids are delivered to the lungs. Hence, the encapsulation process of the drug into the liposomes has a very important influence on the therapeutic utility of liposomes. The choice of liposomal preparation method depends on the physicochemical characteristics of the selected drug and the lipid composition, the nature of the dispersion medium, the effective concentration of the drugs and its potential toxicity, optimum size, intended shelf life and reproducibility. In general, methods of liposome preparation involve four basic stages: 1) the lipid soluble components are solubilized in organic solvent to ensure a homogenous mixture of lipids followed by evaporation of solvent, 2) dispersing the lipid into aqueous media, 3) purifying the resultant liposomal suspension, and finally, 4) the final product is analyzed for size, encapsulation efficiency and stability.20,21 The drugs to be encapsulated are added to either the aqueous hydration buffer (hydrophilic drugs) or in the lipid film (hydrophobic drugs).20,21
Drug encapsulation can be achieved either passively or actively (Fig. 3). Passive loading techniques involve the loading of drugs before or during the manufacturing process. For example, hydrophobic drugs, such as amphotericin B or annamycin, can be combined with the liposomes during the vesicle formation.
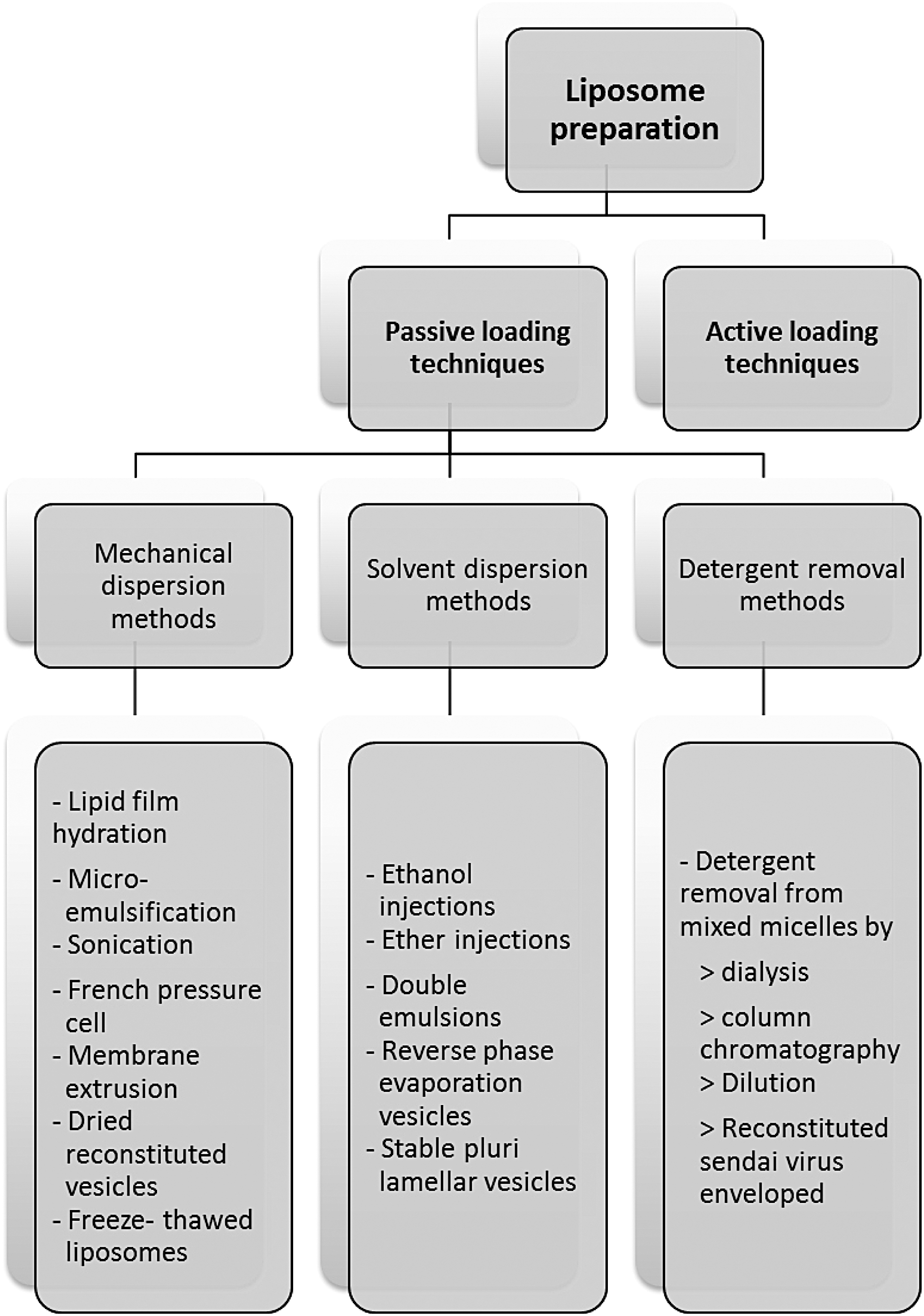
Summary of the different methods for liposomes preparations (Adapted from Dua and colleagues, 201221).
High encapsulation efficiency is often achievable but is dependent on the solubility of the drug in the lipid mixture used to form the vesicles. 7 On the other hand, passive encapsulation of water-soluble drugs such as amikacin and tobramycin depends on the ability of the liposomes to entrap the aqueous drug solution during the liposome formation. The efficiency of encapsulation in this case is usually relatively low and is limited by the concentrations of drug at the time of liposome preparation and the trapped volume within the liposomes. 22 Passive loading techniques include three different methods, namely mechanical dispersion, solvent dispersion and detergent removal methods. Furthermore, each of these methods has different subtype manufacturing processes to achieve its optimum liposomal formulation. For further detailed review of liposome preparation, see Dua and colleagues 21 and Akbarzadeh and coworkers. 20
In comparison to passive loading techniques, compounds with ionizable groups, such as weak acids and bases that are soluble in both lipid and water, can be introduced into fully-formed liposomes through active loading techniques. The general encapsulation mechanism involves a transmembrane ion gradient where the neutral drug diffuses across the membrane bilayer, followed by accumulation within the aqueous interior of the liposomes after ionization into its weak acid or base counterparts. This technique yields higher encapsulation efficiency (as much as 85–99%) and a higher drug/lipid ratio compared to passive encapsulation.21–23
Aerosolization of liposomal formulations
Liposomal formulations can be delivered to the lungs by dry powder inhalers (DPIs), pressurized metered-dose inhalers (pMDIs) and more commonly by using nebulizers. Several types of nebulizers, including air-jet, ultrasonic and vibrating mesh have been trialed to aerosolize the liposomal suspension into inhalable droplets. The different technology used in the nebulizers will affect liposomal stability to different degrees.
Nebulizers
Air jet nebulizers expose the formulation to shear at the air-liquid interface. Additionally this nebulizer exposes liposomes to repeated nebulization, as 98% of the droplets are re-deposited into the reservoir after each passes through the jets. 11 This exposure could affect the vesicle size of the liposomes and drug encapsulation. The shearing stress could cause a disruption to the liposomal bilayer, resulting in fusion of vesicles with a corresponding increase in vesicle size or fragmentation and hence a reduction in vesicle size. During fusion, and more so in liposomal fragmentation, encapsulated drugs could be prematurely released into its dispersing medium, rendering the liposomal formulation ineffective. 2 Incorporation of more rigid phospholipids and reducing the size of the liposomes could help make the formulation more robust to the nebulization process. 24 However, the increase in liposomal robustness to nebulization is often accompanied by a reduction in the release rate of drugs in vivo. Hence, alteration to the liposomal composition will be required to achieve a balance of these competing requirements.
An important factor that needs to be taken into consideration when subjecting the liposomal formulation to jet nebulization is the lipid concentration. A study by Bridges and Taylor 19 reported that there was a direct correlation between lipid concentration and aerosol droplet size, but this correlation was independent of liposomal size and vesicle composition. It was found that the increase in phospholipid concentration was associated with an increase in median nebulized droplet size with the extent of this effect being dependent on the design of the nebulizer. Although the increase in lipid concentration leads to an increase in aerosol droplet size, it also leads to a corresponding decrease in aerosol output. This was attributed to the increase in viscosity or vesicle aggregation of these liposomal formulations at higher lipid concentrations forming larger liposomes. 19 As such, a reduced number of liposomes could be incorporated into the aerosolized droplets and a higher fraction of the liposomes will be retained within the nebulizer with an increase in mean liposome size. Furthermore, larger liposomes are considered more unstable during the nebulization process.12,13
When considering ultrasonic nebulizers, limited studies on the effects of liposomal formulations have been performed, as the generation of aerosols using high frequency ultrasound waves generates heat within the nebulization chamber.25,26 This could affect the stability of the encapsulated drug within the liposomes, especially when less rigid or low Tc phospholipid mixtures are used for vesicle formation. Generally, the lipid composition of liposomal formulation has little influence on the median aerosol size generated from jet nebulizers as long as the lipid concentration remains constant, but a study by Leung and colleagues 26 obtained different results when using the ultrasonic nebulizers. It was found that more fluid liposomes, that is, egg phosphatidylcholine (EPC) liposomes, generated a relatively constant median aerosol size of 5 μm across lipid concentration of 2–40 mg/mL, while more rigid liposomes with cholesterol incorporated into the EPC saw a decrease in median aerosol size from 4.8 to 4.3 μm over the same concentration. Furthermore, the size of the liposomes remaining in the reservoir after nebulization decreased in both formulations but was much more significant in the EPC liposomes, which is indicative of vesicle breakup and drug release. In another study that compared both a jet and ultrasonic nebulizer using dilauroylphosphatidylcholine (DLPC) liposomes containing budesonide, it was found that jet nebulizers have a superior performance and hence efficacy compared to the ultrasonic nebulizers due to their higher aerosol output. 27
More recently developed vibrating mesh nebulizers have certain appealing properties that enable the delivery of higher density aerosols with greater efficiency, while reducing the potential for liposome disruption.2,28 This is because the formulation is only exposed once to the aerosol generation process when the liposomes pass through the mesh to generate aerosol droplets. However, there is a potential for the mesh to become clogged and hence require thorough cleaning after each use to ensure consistent performance. 28 While some studies29–31 have demonstrated that vibrating mesh nebulizers cause less liposomal disruption and loss of encapsulated drug compared to jet nebulizers, there is still significant loss of encapsulated drug collected after nebulization and also in the remaining reservoir that has not passed through the mesh.29,32,33 It was suggested that the energies required to produce aerosol droplets through the vibrating mesh affect the liposomes upstream of the mesh. In terms of effects of mesh nebulization on vesicle size, there is no consistent trend between different studies. 2
Kleemann and colleagues 31 then compared the stability of two iloprost liposomal formulations with lipid mixtures of either DPPC/cholesterol and DPPC/cholesterol/polyethyleneglycol- dipalmitoylphosphatidylethanolamine (DPPE-PEG) when nebulized using the air-jet, ultrasonic and vibrating mesh nebulizer. They concluded that a vibrating mesh and ultrasonic nebulizer showed improved liposomal stability, high mass output and small aerosol droplets compared to the air-jet nebulizer. However, it needs to be noted that the more rigid liposomes with higher Tc, DPPC/cholesterol were used, and these were more resistant to nebulization.
Pressurized metered-dose inhalers
pMDIs are widely used for the administration of anti-asthmatic drugs, and there has been some reported success in formulating liposomes. An early study by Farr and co-investigators 34 proposed the in situ formation of liposomes, which spontaneously form upon hydration in the aqueous environment in the airways. EPC lipids were dissolved in chlorofluorocarbon propellant, and upon deposition to a multistage liquid impinger, liposomes were formed as assessed by electron microscopy. Subsequently, it was demonstrated that the respirable fraction of emitted aerosols were directly related to the phospholipid concentrations while drug entrapment within the liposomes from pMDIs is dependent on the physicochemical characteristics of the drug molecule. 35 Entrapment of ionized, hydrophilic drug salbutamol was found to be negligible while hydrophobic compounds such as hydrocortisone octanoate were highly efficient. Hence, this approach to formulate and deliver liposomal formulations is largely restricted to hydrophobic drugs. More recently, Vyas and colleagues36,37 have attempted to formulate pMDI of antibiotic liposomes. They evaluated the encapsulation of rifampicin and amphotericin B in EPC and cholesterol based liposomes in addition to alveolar macrophage-specific ligands with the aim to improve treatment of tuberculosis. However, the dose of antibiotic delivered by pMDIs may not be sufficient to treat infection.
Dry powder inhalers
Liposomal suspensions are often associated with stability problems. Dry powder formulations have been developed to avoid the requirement for a large number of additional excipients and for their ability to deliver larger doses per puff. DPIs can be stored at room temperature whereas liposomal suspensions require refrigeration and cold chain storage. Dry powder liposomal formulations can be created directly by spray drying, spray freeze-drying or by freeze-drying of a liposomal suspension with the possible subsequent milling to reduce the particle size into a respirable size for inhalation. 2 However, liposomal stability to ensure that they do not agglomerate or rupture and release the encapsulated drug during its manufacturing is a challenge for these processes. Furthermore, it is important that this structure is retained upon hydration in the airways.1,38 The stabilization of the vesicles in these processes during exposure to hydrophobic surfaces (i.e., air) may cause the phospholipid bilayers to deform and uncover the hydrophobic lipids.1,2 Hence, excipients to replace water near the bilayer help retain the hydrophilic nature during processing, and sugars were found to be a superior stabilizer. Crowe and colleagues 39 found that trehalose and maltose, and to a lesser extent sucrose, were effective for stabilizing the liposomal bilayer during freeze-drying; while another study found mannitol superior to trehalose and lactose. 40 The stability mechanism that helps prevent vesicle fusion is the immobilization of the vesicles in a rigid glass at the lipid-solvent interface by sugar bound to the lipids in the bilayer, preventing the impact and or formation of ice crystals that damage the liposomes during freezing/drying. The most stable liposomes during the drying process were found to be smaller in size, ∼100 nm and to also have sugars present on both sides of the bilayer. 41
However, a study by Desai and colleagues 38 demonstrated that although the use of lactose cryoprotectant was able to retain the encapsulated drug in reconstituted liposomes after lyophilization, subsequent jet milling processes demonstrated a much lower drug retention of only 40%. This team went on to develop a unique approach, termed pro-liposomes, to create the liposomes in situ once deposited in the aqueous fluids of the airways from the individual dried components, a similar concept used in pMDIs. The individual components of the formulations, that is, phospholipids, drug and cryoprotectant, are blended and jet milled to form respirable size in its solid state. This method has successfully encapsulated 100% and 96% of cationic CM3 peptide and ciprofloxacin, respectively, but only 45% of salbutamol sulfate.
The encapsulation efficacy of this strategy is dependent on the nature of the drugs and the lipid composition and hence may not be feasible for all drug molecules. More recently, several studies42–44 have successfully formulated proliposome DPI formulations of isoniazid, rifampicin and pyrazinamide using a one-step spray drying of all lipid components and drugs together dissolved in ethanol and water solution. Although, the formulations showed improved efficacy against infected alveolar macrophages43,44 and increased residence time in the lungs compared to free drug, 42 the encapsulation efficiency of these formulations can vary from 20–70% and may require further investigation before developing into a commercial product.
Efficacy
The variety of liposomal formulations allows the design of effective treatments for a range of diseases and subsequent therapeutic success. Although liposomal formulations are a well-established formulation technology, it is yet to be approved for treatment via inhalation in humans. Liposomal formulations that have been evaluated in in vivo preclinical or clinical settings are summarized in Table 1.
Overview of Liposomal Formulations Evaluated in Vivo Preclinical and Clinical Settings
DPPC, dipalmitoylphosphatidylcholine; DSPG, distearoyl phosphatidylglycerol; EPC, egg phosphatidylcholine; HPC, hydrogenated egg yolk phosphatidylcholine; HSPC, hydrogenated soy phosphatidylcholine; Man, 4-aminophenyl-α-D-mannopyranoside; MBSA, maleylated bovine serum albumin; O-SAP, O-steroyl amylopectin; PEG-DPPE, N-methoxypolyethyleneglycol succinoyl-2-N-dipalmitoylphosphatidylethanolamine; pMDI, pressurized metered-dose inhaler; chol, cholesterol; DC-Chol, 3β (N-N’,N’-dimethyl amino ethane-carbomoyl cholesterol; DCP, dicetyl phosphate; DLPC, dilauroyl phosphatidylcholine; DOPE, dioleoyl phosphatidylethanolamine; DMPC,1,2-dimyristoyl-sn-glycero-3-phosphocholine; DMPE-PEG5000, 1,2-dimyristoyl-sn-glycero-3-phosphoethanolamine-polyethylene glycol.
Respiratory infections
Respiratory tract infections (RTIs), including bacteria and fungi, are a major cause of morbidity and mortality in patients with chronic lungs diseases, such as cystic fibrosis and COPD. Inhalation of antibiotics to treat these RTIs, such as TOBI® and Cayston®, provide high local drug concentrations, while minimizing the overall body exposure to the drug and subsequent occurrence of side effects. However, these treatments are often accompanied by rapid clearance of antibiotics from the lungs, resulting in frequent dosing. The development of liposomal formulations for inhalation is particularly attractive for treatment of RTIs since they provide gradual and sustained release of drugs. This allows the maintenance of high drug concentrations for an extended period of time with decreased toxicity. Liposomal ciprofloxacin (CFI, Aradigm) and amikacin (Arikace®, Insmed, Inc.) have been successfully developed and are currently undergoing Phase 3 clinical trials. Previous studies have demonstrated that these liposomal formulations showed a sustained drug release profile allowing for once daily dosing and superior efficacy with significant reductions in Pseudomonas aeruginosa in sputum against baseline and with improvement in lung functions.45–47 In addition to the increased lung retention from liposomes, the enhanced antibacterial efficacy could also be attributed to the intracellular delivery of the antibiotics into the Pseudomonas aeruginosa through fusional interactions of the liposomes with the bacterial membrane or intracellular metabolism releasing the drug into the cytoplasm.16,48–50 Similarly, inhaled liposomal amphotericin B (AmBisome® or Albelcet®), was developed for the treatment of fungal lung infections and as prophylaxis in lung transplant patients. The aim of this treatment is not only to achieve higher dose at the infection site and reduce systemic toxicity but also to reduce the irritation caused by inhalation of the free drug.51–55 These studies also demonstrated that the substantial lung concentration of amphotericin led to superior efficacy of liposomal formulations in treating or preventing invasive pulmonary aspergillosis in immune-compromised patients.
Intracellular microorganisms such as Mycobacterium tuberculosis and Chlamydia pneumonia are able to survive and proliferate within alveolar macrophages (AM) after being phagocytosed. Leemans and coworkers 56 demonstrated that depletion of AM in mice infected with M. tuberculosis had improved outcomes when they were administered liposomal dichloromethylene. Hence, a possible solution to treat these paracellular parasites is to formulate inhaled liposomal antibiotics that target macrophages using specific ligands. Formulations with ciprofloxacin encapsulated into mannosylated liposomes and rifampicin 57 into liposomes coated with maleylated bovine serum albumin (MBSA) or O-stearoyl amylopectin (O-SAP) 36 have been evaluated for their efficacy following pulmonary administration into rats. In addition to sustained high drug concentrations in the lung, the ligand-anchored liposomal formulation demonstrated significantly higher efficiency in targeting AMs compared to drugs incorporated into unmodified liposomes.
Therapy lung cancer
Lung cancer has poor survival rates due to late diagnosis, and treatment options are generally reduced to surgical procedures due to limited success of systemic chemotherapies. Inhalation therapies have become an attractive alternative to reduce systemic toxicity while delivering high drug concentration to the tumor sites. Similarly to systemic administration of cytotoxic drugs, toxicity and tolerability issues in the lung could be an issue and may be addressed by encapsulation of the drug in liposomes. Cytotoxic drugs such as cisplatin, 58 paclitaxel, 59 and 9-nitrocamptothecin60,61 encapsulated into liposomes have been studied for their antineoplastic effects in animal models and early phases of clinical trials. Animal studies demonstrated high local drug concentrations, slow clearance from the lung and at the same time showed drug accumulation in tumors with prolonged survival rates compared to control. Clinical trials have also been performed in patients with primary or metastatic lung cancer who did not respond well to conventional treatments. Overall, the trials demonstrated good response in all patients involved in the Phase 1 trial, with good safety and feasibility profiles of aerosolized liposomal anti-cancer treatments. Another strategy used to treat lung cancer is the aerosolization of immunostimulatory cytokines, which are known to have limited solubility and short half-lives. As a result, liposomal interleukin-2 (IL-2) has been designed to protect the hydrophobic peptide from enzymatic degradation. An early clinical study showed that the liposomal IL-2 formulation was well tolerated, with increased IL-2 receptors in serum in most of their patients and a further two patients (out of 7) experienced antitumor effects. 62 Following from this, Ten and colleagues 63 investigated the potential of liposomal IL-2 for primary immune deficiency and showed that the liposomes were able to preserve the biological activity of the cytokines that subsequently resulted in lymphatic absorption and activation of the immune system.
Gene therapy
Gene delivery by inhalation holds many promises for a variety of diseases such as lung cancer and cystic fibrosis. However, the delivery of such long and fragile DNA molecules would require complexation and encapsulation into liposomes to protect it from destruction or degradation. Initial study in animal models to assess gene expression following administration of liposomal encapsulated gene, showed encouraging results with restoration of ∼50% of the ion transport abnormalities. 64 Furthermore, it is suggested that the nonviral nature of liposomes as gene carriers compared to adenoviral therapies carries lower risk of immunogenicity. In a Phase 1 clinical trial, liposome-mediated gene transfer was assessed in cystic fibrosis patients, in terms of safety and efficacy of nebulizing cationic liposomes containing the cystic fibrosis transmembrane conductance regulator (CFTR) gene into the lungs. A significant degree of recovery of the chloride abnormalities was found in patients receiving active treatment, and bacterial adherence was also reduced. However, most patients also reported mild influenza-like symptoms—myalgia, headache and fever that resolved within 36 hours in the same group. Similar side effects were observed in a second trial by Ruiz and coworkers with no apparent long-term effects. 65 These studies suggest that the toxicities observed with cationic liposomes encapsulating DNA are associated with immunostimulation, and hence better understanding of the formulations and DNA vectors will be required before further advancement in this area can progress.
Conclusion
The formulation of inhaled liposomes has allowed the delivery of various compounds with different solubilities, DNAs, peptides and cytotoxic drugs. The possibility and ease of modifying the vesicles enables them to have widespread applications for different disease states. There is no one size fits all formula for inhaled liposomal formulations. Manipulation of the different physicochemical properties such as size, lipid composition and type, fluidity and surface charge enables the formulation of a desired carrier with specific pharmacokinetic and pharmacodynamic properties, reduced toxicity and simultaneously enhanced efficacy for the targeted disease states and specific drug. Promising data over the past 20 years on inhaled liposomal formulations in vitro and successful translation into animal models and clinical trials will eventually lead to breakthroughs and clinical success. The ultimate success will depend on innovative liposome design with high stability and integrity coupled with efficient and predictable drug release at specific target sites or cells.
SUMMARY
Although liposomal formulations are well established, none are yet marketed for treatment via inhalation in humans.
Manipulation of the physicochemical properties of liposomes enables innovative design of the carrier to meet specific pharmacokinetic and pharmacodynamic properties, reduced toxicity and simultaneously enhanced efficacy.
Liposomal formulations can be delivered to the lungs by dry powder formulations (DPIs), pressurized metered-dose inhalers (pMDIs) and more commonly by using nebulizers.
Liposomes containing small amounts of cholesterol to enhance the rigidity of the bilayer are generally more resistant to the nebulization process.
Successful translation of inhaled liposomal formulations in vitro into animal models and clinical trials will eventually lead to breakthroughs and clinical success.
Footnotes
Acknowledgments
Dr. Hui Xin Ong is the recipient of a European Respiratory Society Fellowship (LTRF 2013–1730). Associate Prof. Traini is the recipient of an Australian Research Council Future Fellowship (Project no. FT12010063). Prof. Young is the recipient of an Australian Research Council Future Fellowship (Project no. FT110100996).
Author Disclosure Statement
The authors declare they have no conflicting financial interests.