
Abstract
The negotiations required in managing the adolescent–parent–oncologist relationship while making health decisions are complex. While the capacity to make competent decisions emerges between the ages of 11 and 14, 6 young people can have a reduced sense of responsibility and risk awareness, difficulty regulating emotions, and may be more impulsive than adults.7–9 They also have limited useful experience to draw upon in their attempts to manage decision-making independently.4,10 Research suggests that while involvement of adolescents as collaborators in decision-making is beneficial,11–13 many young people do not want sole responsibility for medical decisions 12 and some desire a passive role.2,11,14
Parents of pediatric patients have also described a desire to share decision-making with their child's multidisciplinary team (the specialists most relevant to the current issue of concern, such as an oncologist, fertility specialist, or radiologist),11,15–17 although their preferences may lie on a continuum ranging from maintaining absolute control of decision-making to deferring completely to their child's multidisciplinary team. 18 It is likely that parental satisfaction is determined by the match between their preferred and actual levels of involvement in decision-making. 17 Parents may also be more likely to prefer a passive over an active role as their child's medical situation becomes more threatening.19,20 However, parental role preferences are not clearly understood for adolescent-aged cancer patients. Furthermore, despite the significant impact of pediatric and adolescent cancer on siblings,21,22 little research has investigated these siblings' decision-making experiences, which may include increased autonomy while parents are absent and attending to the needs of the child with cancer.
Further investigation of the myriad choices families face during adolescent cancer is needed to improve the quality of care provided to patients currently on treatment and particularly to survivors post-treatment, when the “crisis” of diagnosis and treatment has been successfully traversed. 17 Families face both major and minor decisions in the off-treatment period. 23 Major decisions can include choices about commencing or continuing treatment, clinical trial participation, and treatment or screening adherence. Examples of minor medical and social or lifestyle choices include the medical management of fever or nausea, adherence to recommended health behaviors (e.g., diet, alcohol, or drug use), and whether one is well enough to attend social functions. In addition, it is also important to note the differences between decisions that involve only one recommended course of action compared to decisions where there is no clear recommendation but rather multiple options with varying risks and benefits associated with the decision. 24
Three areas relevant to decision-making across the adolescent cancer trajectory were explored in this study: (1) appointment participation (as decisions generally can only be made, or contributed to, by those in attendance), (2) family members' perceptions of who the instrumental decision-makers were in regards to major and minor decisions, and (3) sources of family disagreement.
Methods
Participants
Eligible survivors were all those who underwent cancer treatment before 18 years of age, were an adolescent (aged 12–20) at the time of interview at Sydney Children's Hospital (SCH), Australia, between 2007 and 2009, had completed treatment with curative intent, and were less than 5 years post-treatment. Eligible survivors' parents and siblings (aged ≥12 at interview) were also invited. Potential participants were excluded if language restrictions or other circumstances (e.g., psychiatric or neurological conditions) limited their capacity to participate.
Interview development
The semi-structured interview schedule administered to all survivors was prepared by the multidisciplinary team (which included a pediatric oncologist, adolescent oncologist, social worker, and one clinical and three research psychologists). Small changes in phrasing were made to the interview to create versions appropriate to the perspectives of mothers, fathers, and siblings. The interview was then pilot-tested with two consumers (one mother, one survivor), and modified according to their feedback.
As prescribed by Miles and Huberman, 25 results from early interviews were used to suggest additional lines of questioning in subsequent interviews. Data were collected as part of a larger study that also explored adolescents' psychosocial and educational 26 experiences post-cancer treatment. Participant responses related to decision-making and appointment attendance are reported here. An example of the interview content related to decision-making experiences and clinic attendance is provided in Table 1.
As presented to the survivor; parent and sibling interview schedules were modified to be appropriate for their perspective.
Procedure
Eligible participant families were sent a letter from the Head of the Centre for Children's Cancer and Blood Disorders at SCH inviting them to participate in the study, with interviews conducted from February 2009 to February 2010. Families were asked to return an opt-in card using a reply-paid envelope should they be interested, and were subsequently contacted by a member of the research team to arrange an interview. Individual interviews were conducted by telephone (n=66). However, one mother–father pair and one father–son pair chose to be interviewed together in person. These pairs requested their interviews take place while attending their next scheduled clinical appointment, as this time had already been allocated to cancer-related appointments and would not interfere with their work or school commitments. All interviews were conducted by a post-doctoral level researcher (JKM). The study received Institutional Review Board approval, and informed consent was obtained from all participants.
Data analysis
We took an inductive approach to analysis, though guided by the Parental Treatment Decision Making (PTDM) model as a conceptual framework. 18 The PTDM model outlines contextual factors that can influence parental involvement in decision-making (including illness-specific factors, individual parent characteristics, and the relationship with clinicians). Participant responses were recorded and transcribed verbatim. Transcripts were coded line-by-line, and analysis was facilitated by QSR NVivo8 software, which allows the researcher to store, code, and retrieve raw data and collate researcher observations and ideas. Fifteen percent of interviews were coded independently by two investigators, who met to review the coding and address any disagreements. If the coding pair did not agree on how to code a passage, the issue was referred to the team. This multilevel consensus coding method meets accepted standards in qualitative research. 27 Emergent themes were cross-tabulated with participant characteristics and counts of the numbers of participants who endorsed particular beliefs were used to moderate potential researcher bias.25,28 We used recurring patterns and multiple comparisons to provide additional support for each theme that was identified, and used divergent views and negative cases to challenge generalizations. Participant responses for each question were compared with those of their participating family members to gauge intra-family agreement on key issues. As concordance between family member reports was generally high, results presented are grouped by family. Disagreements between family member reports are highlighted in the analysis and discussed separately. Participants' responses were spontaneous in nature, and therefore not every participant discussed every issue. As such, all counts of the number of families who reported experiencing a particular issue are conservative estimates.
Results
Interviews were conducted with 70 individuals from 22 families (family response rate=34%) and included 19 survivors, 21 mothers, 15 fathers, and 15 siblings (Table 2). The number of participants per family ranged from one to five (mean cluster size=3.2), with two families including two participating siblings. Survivors from three families chose not to be interviewed. Seven sets of parents (32%) were divorced or separated.
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; CML, chronic myeloid leukemia; SD, standard deviation.
Appointment participation
During treatment, the most commonly described appointment arrangement (10/22 families) was for both parents to attend critical appointments, while mothers alone accompanied patients to non-critical appointments (Fig. 1): “It's only been those important doctor's appointments where we've both gone to find out whatever the news was on that particular day” (Mother [female, 15]). 1 Siblings rarely attended appointments, except out of necessity (e.g., lack of childcare), and reported satisfaction with this arrangement. Post-treatment, 8 of these 10 families reported that mothers began accompanying their child alone because consultations had become less critical.
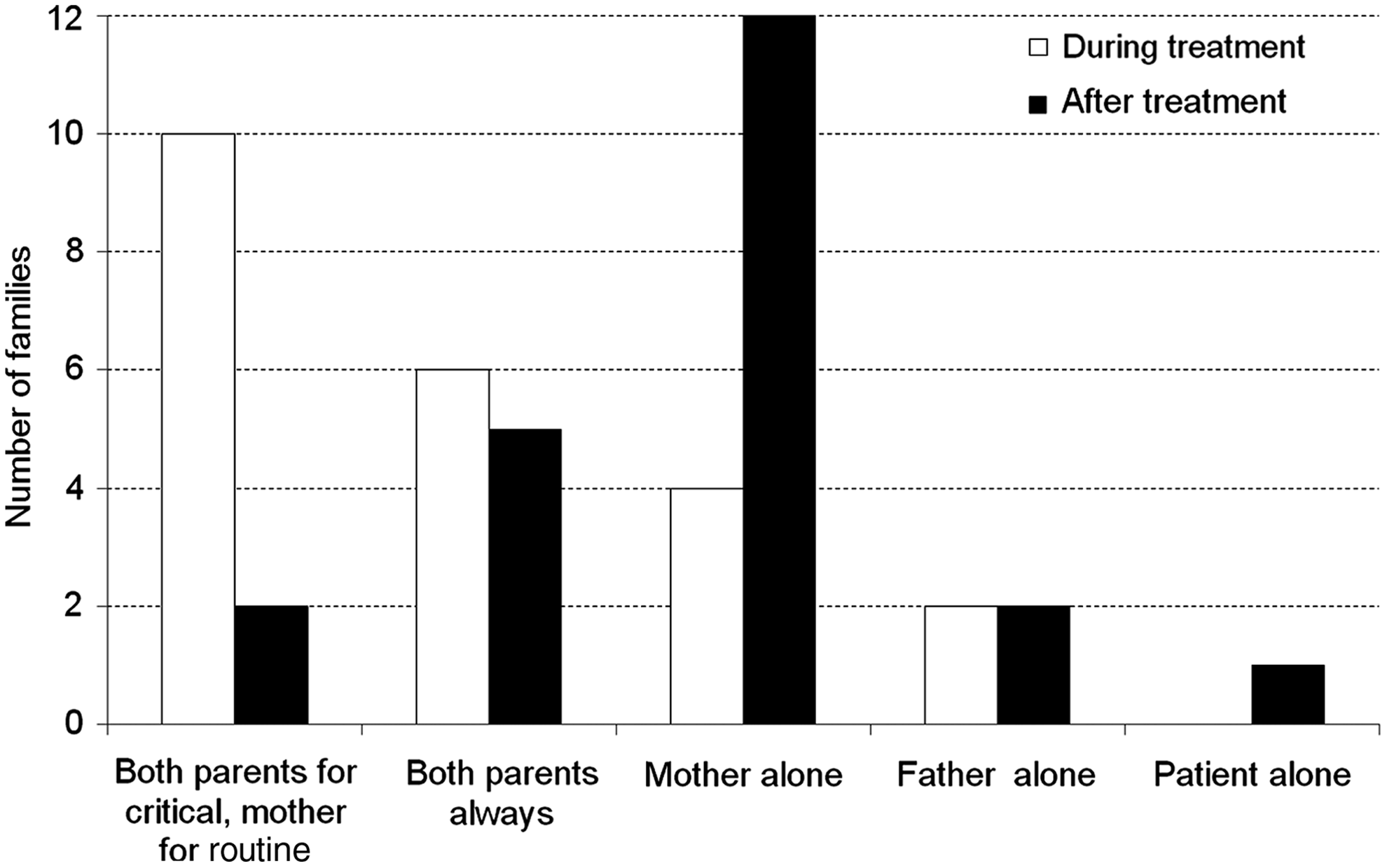
Reported appointment attendance during and after treatment, by family (n=22). Note: The patient/survivor attended every appointment, with both parents, one parent, or alone.
In six families, both parents attended every appointment together. While many parents were aware of the increasing maturity of their child, they continued to accompany their child because of the possibility of receiving unexpected news: “No, we take that responsibility, his dad and I. I'd still personally rather be there, for anything, just in case” (Mother [male, 17]). In four families, mothers attended all appointments without paternal involvement (in three cases due to divorce), while in two families fathers were primarily responsible. Several fathers reported that they would have preferred to attend more often, but were restricted by work, cost or distance of travel, or the needs of their other children. There were no disagreements between family members regarding appointment participation.
Involvement in decision-making
Medical decisions
During treatment, 9 of 22 families reported that the oncologist made all major decisions (Fig. 2): “I said to my oncologist ‘Look, just do your job.’ My only question during the whole time was when will this be over?” (Survivor [male, 19]). This was in accordance with participants' preferences and often related to the need for critical and complex decisions to be made quickly. Three survivors would have preferred to be more involved in specific decisions (e.g., fertility preservation and gastrostomy feeding). In five families, parents felt they made all medical decisions together during treatment, and in a further five, mothers were named as the primary decision-maker. Only one survivor was named primary decision-maker during treatment. However, five were allowed partial decisional autonomy (e.g., to make minor decisions such as anti-emetics use). Twelve interviewees spontaneously discussed the age at which young people in general were capable of making medical decisions, and their responses ranged from 12 to 18 years (most commonly, ages 14 or 15): “Maybe 14 plus. You would still discuss with your family, but the further you get from 14, the more you should talk to the patient, not the parents” (Survivor [female, 19]). However, age was seen as secondary to the maturity of the adolescent: “It depends on the maturity of the kid..I would regard him as a less mature child than someone else of his age” (Mother [male, 13]).

Perceived primary decision-maker of medical and social or lifestyle decisions, by family (n=22). Note: The term “joint” refers to a decision being made jointly with the patient, parents, and multidisciplinary team.
Post-treatment, two participants remarked that “basically there are no decisions to make. There is only the occasional check-up” (Father [female, 20]). Others felt important decisions remained and these were increasingly made by survivors (n=9): “We've…taught her it's her body. She's old enough and makes the right decisions for her own health now” (Mother [female, 16]). Four families nominated the mother as primary decision-maker. However, in three of these families, survivors would have preferred their mother to be less involved: “She's very over-protective and we'll have arguments, [where I say] ‘I'm not that sick kid anymore’” (Survivor [female, 16]). There were no disagreements between family members regarding nomination of the primary decision-maker responsible for making major decisions.
Social or lifestyle decisions
Given the patient's condition during treatment, 12 of 22 families reported that few social or lifestyle decisions were made (Fig. 2): “She missed a lot of social events because she was just in bed by 7:30” (Mother [female, 16]). Three families reported that parents were primarily responsible for social or lifestyle decisions during treatment, while a further three reported that social decisions were made jointly with the patient. During their brother's or sister's treatment, 7 of 15 siblings reported adopting additional decisional responsibilities, such as making social or extra-curricular decisions or caring for younger children. Other siblings felt they maintained their pre-cancer levels of responsibility: “I already made my own decisions before that. It's not like all of a sudden I didn't have a boss” (Male sibling aged 20 [male, 13]).
After treatment, the majority of survivors (n=14) assumed responsibility for social or lifestyle decisions, determining their consumption of alcohol, smoking, and socialization with peers: “I would like to think it is more me that makes the decisions now. I want to leave mum and dad behind” (Survivor [male, 17]). Parents confirmed they had relinquished this responsibility in each of these cases. There were, however, five mothers (of younger adolescents) who were still considered responsible for their child's social or lifestyle choices, with this manifesting as limiting activities possibly detrimental to the child's health. Fathers rarely took primary responsibility for their child's lifestyle choices, except in the case of a son's re-involvement with sporting activities. Post-treatment, three siblings noted increased levels of parental involvement in their own lives, which was mostly positively received. Three parents noted they allowed the siblings more freedom than their peers because the siblings had proven their capabilities during their siblings' treatment.
Sources of disagreement
Sources of family disagreements included social issues (primarily mothers wanting their child to socialize less frequently), health behaviors (e.g., mothers wanting their child to eat more healthily), and minor medical decisions (e.g., monitoring for fever; summarized in the Supplementary Appendix which can be viewed online at www.liebertpub.com/jayao). However, the majority of families described a harmonious experience during treatment (14/22): “My parents pretty much trust me with anything…because they knew I could make the right decisions” (Survivor [male, 13]). Six families described their experience using more mixed language with times of harmony and conflict, while two survivors reported a predominantly acrimonious experience. In three cases, family members reported disagreeing about a major medical decision (including fertility preservation).
The post-treatment period emerged as a time of escalating conflict, with seven families reporting family turmoil caused by parental protectiveness: “She went to her first disco the other night and I lived on edge. If anything happens I will never forgive myself for letting her go” (Mother [female, 15]). In two cases, conflicts resulted in the survivor moving out of the family home. While family conflict was a cause for concern, no parent reported any formal support or coping strategies used to manage the anxiety this elicited. Rather, this was viewed as a common occurrence and many parents acknowledged that their child's peers whom did not have cancer were also in conflict with their parents: “I think it's just normal teenager stuff” (Mother [male, 15]).
Discussion
This is the first study, to our knowledge, to explore decision-making in families of adolescent cancer survivors from the viewpoint of each family member, including siblings. This multi-perspective approach allowed for the investigation of complex relationships, with both complementary and contradictory perspectives.17,29 There are three principle findings from this study.
First, despite all participants feeling that young people were entitled to involvement in health-related decision-making, there was uncertainty about the age at which adolescents were capable of making sound decisions. This supports findings that age is a poor proxy for maturity and developmental capacity.10,14 Additionally, role preferences were individual, situation-specific, and changed over time, which is in line with the PTDM model 18 and mirrors previous research.9,14 During treatment, families were more likely to prefer the multidisciplinary team to make important medical decisions, with few social or lifestyle decisions to be made themselves (although as expected, there were large variations in preferences across families). Post-treatment, however, the preference was for the survivor to be the primary decision-maker for both medical and social decisions, due in part to the increased maturity of the survivor, their more advanced understanding of their disease, and the reduction in the number of urgent or life-threatening decisions to be made.
Similar to other clinical settings, 30 there was a still a clear role for parental support, with a parent in attendance for almost every appointment during treatment. This is in accordance with reported adolescent and parent preferences and theoretical expectations, 18 in which the multidisciplinary team makes many key treatment decisions while families take responsibility for less critical decisions. Thus adolescents coping with a cancer diagnosis have different decisional-support needs over the cancer trajectory, which should be considered unique to the individual and determined in consultation with the adolescent themselves.
In line with the PTDM model, 18 preferences for involvement in decision-making varied significantly between and within families, and were associated with individual and situation-specific factors. However, young people (both survivors and siblings) were generally satisfied with their level of involvement. This is in contrast to previous research suggesting that clinicians and/or parents had a paternalistic attitude toward,31,32 and marginalized, adolescents14,33 and that this difference may be cultural,34,35 site-specific (this study was limited by recruiting participants from one site), or may be a result of changing or improving clinical practice. Families were keen to learn their clinician's recommendations and eagerly followed them. In certain circumstances (e.g., for choices potentially affecting prognosis), the evidence suggests that this is the preferred course of action and can lead to positive outcomes in the short term.12,24,34
What is not known is the impact that decision-making involvement has on longer-term psychological outcomes. It is possible that decisions made by clinicians may be resented as the adolescent matures (fertility-related decisions may be particularly prone to this). Conversely, it is possible that regrets may be heightened when negative outcomes emerge from a decision made by an adolescent and/or parent.18,36 Interestingly, early evidence suggests that there may be no relationship between patient decisional involvement and subsequent guilt experiences. 34 While assuming decisional responsibility may not always be the preference, clear clinician–family communication remains vital to ensuring families remain engaged with treatment 37 and to facilitate young people in taking responsibility for their own healthcare as they mature.
Lastly, conflict occurred where there was a mismatch between adolescents' desire for involvement in making decisions and parental desire for control, which aligns with the patterns of conflict hypothesized by the PTDM model. 18 It was the less critical decisions that were a potential source of conflict in families, particularly post-treatment. Some familial disagreements were similar to those described by non-cancer-affected families. 38 However, other sources of parental concern and conflict were cancer-specific (e.g., parental reluctance for adolescents to catch public transport to and from school). The match between adolescents' and parents' involvement preferences change over time. 14 In this study, it lessened post-treatment. If the key issue is the congruence (or lack thereof ) with decision-making preferences, it is critical to respect the involvement preferences of each stakeholder and to check regularly that these have not changed. The PTDM model is useful in identifying potential mismatches between preferred and actual roles in decision-making, 18 and may be useful for clinicians to develop strategies to reduce current or future family distress.
The study was limited by its reliance on retrospective experiential accounts. Participants may have endorsed a more participatory role when describing their involvement retrospectively, as once treatment outcomes are known (and in these cases were successful), survivors tend to report that they were more responsible for decisions. 18 The low response rate is in line with other adolescent cancer research, 39 but does limit generalizability and increase the chance of sampling bias. Family members' reasons for refusal remain unknown. However, it is possible that the response would have been greater had we approached them while the patient was on active treatment, at which time they may have been more invested in cancer-related research. 40 It is also possible that inviting fathers affected the response, given that males are less likely to participate in research, regardless of the data collection strategy adopted. 41
Given the small sample size, it was not possible to delineate the experiences of families affected by different cancers. It is likely that experiences will differ by diagnosis, and this may be particularly relevant for survivors whose cancer and cancer treatment may have affected their cognitive ability. Participants' responses may have been inhibited by the use of the telephone. 42 However, there is little difference in the quality of data collected face-to-face when compared with telephone interviews. 43 Telephone interviews also yield more in-depth responses when discussing sensitive issues and increase the rate of response from individuals who would not otherwise have their views represented (e.g., those living rurally).43,44
In conclusion, due to the lack of critical mass of adolescents with cancer, health professionals are often poorly equipped to deal with their needs. This is a unique situation that differs from an adult or pediatric consultation. Despite being generally satisfied, there will always remain a power imbalance between adolescents, their parents, and their oncologist, 14 and this must be managed sensitively. While patients or parents may not always want sole responsibility for critical decisions, they should have the opportunity to decide the level of involvement they wish to have, and their preferences should be respected.17,45 This way, the benefits espoused by family-centered care 45 can be achieved without putting unnecessary pressure on patients or parents. This strategy should allow families to feel included and that their views are valued, and this is likely to increase trust in the adolescent–parent–oncologist relationship. 17 This approach also aligns well with modern and more nuanced shared decision-making models that promote collaboration without the expectation that all patients or parents take full responsibility for all decisions during their medical care.46–48 Instead, these models allow flexibility in recognizing that patients and families can make an informed choice to allow experts to make some decisions on their behalf.46–48
Future directions
Best practice models14,45 are yet to incorporate fully the evolving nature of the family decision-making experience during and after adolescent cancer. To capture this evolution more fully, further longitudinal research, whereby the same stakeholders are interviewed several times over the course of the cancer trajectory, would be a valuable addition to the literature. Additional research on decision-making regarding clinical trial participation and sibling experiences (given our small sibling sample and their wide age range) is also warranted. Further in-depth exploration is also needed to describe any potential differences in survivor–parent and sibling–parent conflicts, as well as the conflict resolution strategies families adopt in this setting. Research also needs to move beyond documenting preferences to the next stage of testing interventions to support family decision-making.17,18 The Negotiated Care Tool, designed to formalize parent preferences for involvement in the care of their hospitalized child, shows promise in this regard. 49 This tool has been successful in increasing parental inclusion in decision-making, encouraging parents to ask questions during their child's hospital stay, and expanding the participation of extended family members (with parental permission). The tool also aims to raise the awareness of hospital staff about the importance of effective communication and negotiation of care with parents. 49
Footnotes
Acknowledgments
We thank Sarah Ellis (research officer) and Kate Lenthen (senior social worker) at Sydney Children's Hospital, and Dr. Kelly Mok (medical oncologist) at Prince of Wales Hospital for their contributions to this study. The study was supported by the Leukaemia Foundation of Australia and the Sydney Children's Hospital Foundation. Dr. Wakefield is supported by the National Health and Medical Research Council of Australia (ID 510421) and the Cancer Institute NSW.
Disclosure Statement
No competing financial interests exist.
1
Participant details indicated as: (relationship to survivor [survivor gender, survivor age at interview]).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.