
Abstract
Patients and Setting
Qualitative data were gathered in interactive workshops with TYAs and professionals. Three workshops were held in England: one TYA workshop and two professional workshops. Additional quantitative data were collected from a survey with TYAs.
Young people aged 13–24 years at the time of diagnosis, aged 16–29 years at the time of study, and within five years of treatment being complete were recruited through the Internet (www.facebook.com/TeenageCancerTrust). Some members of the National Cancer Research Institute's Teenage and Young Adult Core Consumer Group (NCRI TYA CCG), an experienced service user group, played a dual role of participant and researcher. Eleven TYAs participated, including four CCG members (Table 1). The survey was conducted at “Find Your Sense of Tumour” (FYSOT) 2010, a conference for TYAs with cancer (www.JimmyTeensTV.com). Sixty-four completed surveys were returned, out of approximately 270 (24%; Table 1).
CNS, central nervous system; TYA, teenage and young adult.
Data for participants and Core Consumer Group (CCG) presented together to protect anonymity.
Limited demographic information collected to ensure anonymity.
Professionals were recruited through the Teenagers and Young Adults with Cancer (TYAC) organization's website, which is a professional body for those involved in the research and care of TYAs (www.tyac.org.uk). Twenty-six professionals responded and 22 attended. Participants included doctors (n=4); nurses (n=10, including nurse consultants, nurse specialists, staff nurses, and research nurses); and other professionals (n=8, including social workers, youth workers, and academics).* All but six worked in a principal treatment center.
Institutional approval was granted through a hospital research and development department. Ethical conduct was maintained in line with national guidelines. 9
Methods
The workshops consisted of numerous activities:
1. “Pyramid of Importance”: Fifteen key components of specialist TYA units were identified from published literature and transferred onto cards. Working in groups, participants were asked to rank cards in order of importance on a pyramid. This activity was developed based on the principles of participatory evaluation.10,11 Blank cards were provided so other components could be added and substituted for one of the preprinted options. Additional components suggested by participants were added to the core cards for the next workshop, with the pyramid continuing to have 15 slots so that groups had to prioritize their key 15 components. During the activity, an observer made notes of the group discussions about card selection and placement. 2. Presentation to a “board of hospital governors”: Professional workshops concluded with a mock presentation to a board of hospital governors. These were to explore in more depth the professionals' decisions in defining their key components of a specialist TYA cancer unit. Participants developed a business case and presented this to the board of hospital governors, which was comprised of a CCG member, a professor of TYA cancer care, and a senior researcher in TYA cancer. One professional in each group was nominated by their colleagues to present the case and board members posed questions to gain a deeper understanding of decisions. Presentations were digitally recorded and transcribed verbatim.
The methods were identical in all three workshops; one of the health professional workshops had a greater number of participants so they were divided into two groups, as was the young person workshop for this activity.
FYSOT young person survey
A modified Pyramid of Importance was administered at FYSOT as a self-report survey. Thirteen of the 15 key components were randomly selected to allow two blank spaces for young people to add additional components. Key components were numbered so the number from the list could be inserted in the pyramid in order of importance, that is, the most important in the top box, and so on, until the pyramid was full (Fig. 1). The survey was placed on delegate seats and its purpose explained by the CCG during their presentation (http://jimmyteens.tv/2010/04/fysot-10-research-for-you-ncri-group/). Participants returned completed surveys to a sealed box. The survey contained no identifying information.
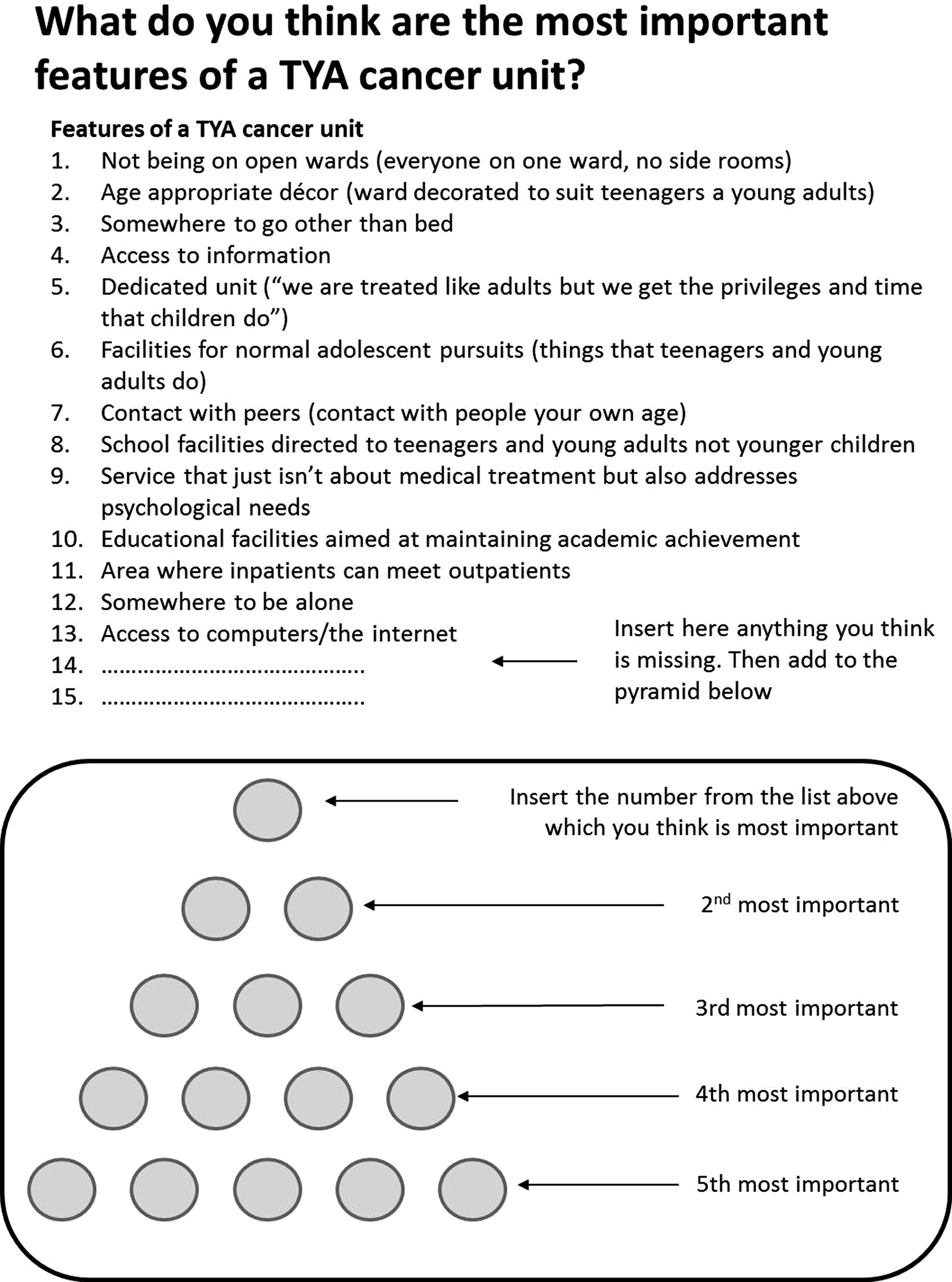
Pyramid of Importance, survey version.
Analysis
Data were analyzed through ranking the cards within the pyramid. The pyramid contained five levels; the cards were scored from 5 to 1 based on their position in the pyramid (e.g., 5 points for items at the top and 1 for those at the bottom). This enabled a rank score for each item to be calculated. 12 To account for variation in card selection, the rank score was standardized by dividing by the sample size (i.e., number of pyramids in each workshop and number of participants in the survey). Data from the professionals and young person workshops and survey were analyzed separately so similarities and disparities in priorities could be explored. Content analysis of transcripts from the governor board presentations and the notes taken by the observer during each activity were undertaken to provide further depth and explanation for ranking decisions.
Following analysis, participants in the young people's workshop, including the CCG, were invited to a “debrief day.” Six young people participated and examined the health professionals' and young people's pyramids. Notes were taken of their comments and discussion, which were integrated into the findings.
Findings
Findings are presented as a description of the ranking of components in the pyramids, interspersed with supporting dialogue taken from notes and governor board transcripts.
The workshops generated two pyramids by young people and three by professionals. Participants agreed that none of the key components, either pre-stated or added during the exercise, were superfluous; the difficulty lay in selecting 15. This was reflected in the final pyramids, for which participants disregarded instructions and inserted multiple cards onto boxes (Fig. 2). The top six priorities identified in the workshop are shown in Table 2. Disparities existed in the ranked order of importance between young people and professionals. Only one item ranked similarly—“access to information”—which was ranked seventh, with young people making additions to the card to specify the type of information they needed: “teenager friendly, info for family/friends, your cancer, facilities available, all aspects of treatment/side effects.” Young people felt current information was generic, inappropriately delivered, and given at irrelevant times. They wanted succinct information that was easily accessible: what they wanted, when they needed it.
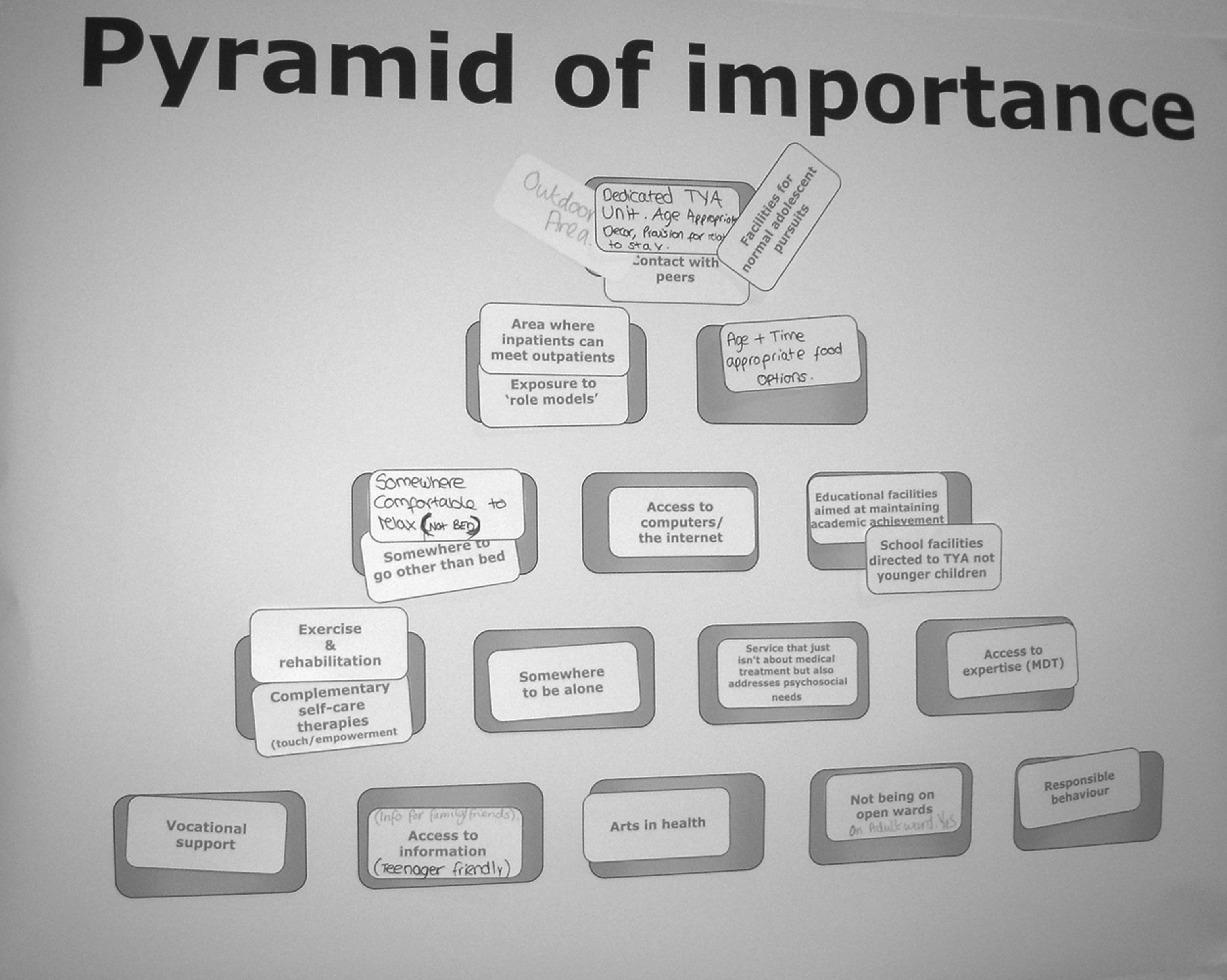
An example of one of the pyramids generated during the workshop.
MDT, multidisciplinary team; QOL, quality of life.
Using arts as a distraction.
Note: Multiple entries per rank denotes equal score in the analysis.
Young people selected a dedicated unit as the most important component of specialist TYA care as it facilitated peer contact. Interestingly, in contrast to the priority given by young people, professionals discussed that “peers were important but not the top three.” Professionals argued it was the philosophy of care that was more important, not just the physical unit. Considerable debate ensued about the service versus the unit and whether it was possible to have one without the other; it was concluded that both were needed as the unit provided a building block in which to build expertise. Professionals noted the age range of young people accessing specialist TYA care in England was broad (13–24 years) and would be difficult to provide for in a single unit. Concern arose that complex issues experienced by older adolescents and young adults may not be appropriate for younger adolescents to be exposed to (no examples were given in the discussion of what was a “complex issue”).
Professionals ranked “best chance of survival and best quality of life” as the top priority:
[The young person] walks into a service that's going to give [them] the best chance of a healthy survival. And is going to provide the best quality of life…it's about making that survival a healthy survival…not about taking the cancer, treating, curing it and leaving it and just assume that everything is going to work out. It's about the whole person and ensuring a healthy long-term life.
This was unranked by young people, as it was an additional component by participants at a later workshop. Young people ranked allowing “partners/parents to live in the unit with them” highly. One young person who had received care on an adult unit recalled what it was like not being allowed to have parents stay: “sometimes I would cry if mum wasn't there.” Young people agreed they wanted access to expertise, although they required an explanation of what “MDT” (multidisciplinary team) stood for. Further, not all young people were aware of the existence of MDTs, which initiated a heated discussion about not being informed of what was discussed about them at MDT meetings.
Professionals concluded the top two components were “best chance of survival…” and “access to expertise,” but these were underpinned by components in subsequent layers that reflected elements that provided hope to young people and optimism about the future (e.g., “facilities for normal adolescent pursuits”). Interestingly, young people commented they did not think professionals recognized the importance of education, which was reflected in the low ranking of this component by professionals. Young people also ranked this low, and in their discussion one young person stated: “If I'd had cancer when I was at school then I would have used it as an excuse not to go.” Similarly, young people noted rehabilitation was ranked low by professionals, and they felt this needed to be accorded higher ranking, especially as it was an aspect of care young people knew was important but did not want to do: “everyone hates the physio!”
Young people and professionals added an additional 22 TYA cancer unit components they felt were not covered by those originally provided (Table 3). Young people who had access to outdoor space during treatment found this to be a pleasant escape: “fresh air does the world of good.” However, they noted the only outdoor space provided by most hospitals was “where old people congregate to smoke!” Young people also included food and mealtimes, wanting the ability to choose what food to eat and when. Worryingly, young people attending the “debrief day,” when asked why they had not considered “privacy and dignity,” stated that they had resigned themselves to not having any from the point of diagnosis.
QOL, quality of life; MDT, multidisciplinary team; TYA, teenage and young adult.
Note: Text added in italics at the end of some entries indicates comments added by young people.
Using arts as a distraction; †complementary therapies used to promote self-care, and art and music therapy.
Analysis of the FYSOT survey data showed wide variations in preferences, ranked across 12 levels. The 13 components used in the survey from the workshop pyramids were analyzed separately to enable comparison across the three datasets. Similarities existed between the rankings of components by young people, but it was clear that professionals had different perceptions of what the key components of a TYA cancer unit were. Young people felt professionals' pyramids were very clinical, reflecting the friction between what tasks professionals wanted to complete and what patients felt they needed.
Finally, in one of the board of hospital governors' presentations, the presenting professional was asked why young people and not older adults with cancer should get specialist services. The response:
Without these key services these young people are going to present back into the services later on in life, be it through psychological medicine…perhaps be unemployed, they're not going to go back into education, they're not going to be productive for society, but they're also going to…create the healthcare burden…so by putting these services in place, we're reducing that.
Discussion
Our study identified the key components of a specialist TYA cancer unit from the perspective of both young people and health professionals. We found there were considerable differences in opinion. Professionals' views tended to be service-orientated, while young people viewed care as a personal experience. This may be partially explained by age and developmental stage because young people tend to live for the “here-and-now.” 13 Young people have said during treatment they focus on “getting through it.” 14 As such, the environment facilitating them to do this with the least disruption to “normality” may take priority. Professionals are more likely to take a long-term view, ensuring immediate survival but also enabling young people to reintegrate back into “normal” life when treatment ends. 15
Differences in perception also existed within the two professional groups, as the composition of participants was different. Participants in one were from established principal treatment centers compared to the other where professionals were from either new principal treatment centers or pediatric/adult environments. Similarly, variation in young people's results reflected their range of experiences of care. Satisfaction with care is reported as being higher by young people who attend dedicated TYA units. 6 However, participants in our workshop who received care in specialist TYA units were the harshest critics. This may be due to raised expectations as to what a dedicated unit can provide. 14 There is pressure on health professionals to constantly deliver higher standards of care in such a setting and any lapse in care delivery may become a significant memory in young people's experience.
Young people identified a “dedicated unit” as being central to specialist TYA cancer care. This reflects the preference reported by young people in other studies.4,7 But the question remains, what are the key components of dedicated units? While this has been reported as “not being particularly difficult to define,” 7 there is no empirical evidence of what is essential and what is the “icing on the cake.” The available evidence suggests that young people cared for in dedicated units are better able to regain control, 5 which is important for emotional well-being. 16 A recent report suggests that dedicated units provide the staff and equipment, which promotes the philosophy of specialist TYA cancer care. 5 Importantly, it has been argued that dedicated units should become a vessel in which expertise is nurtured and enables “a sustainable critical mass for practice development and research.” 8
Similar to other reports,17,18 young people rated the need for information very high. Effective provision of information is an essential aspect of specialist care. 19 Information underpins empowerment, which promotes self-care and the ability to participate in decisions, as well as improving emotional well-being. 20 Provision of information in TYA care is a skill in which both the timing and level of information are influenced by the age of the person receiving it. Information needs to be imparted at different and often critical time points to both young people and their families. Young people need to be in the “foreground of communication,” 21 with information provided in an age-appropriate way and without alienating parents (i.e., providing information to the young person and respecting their instructions on what can and cannot be divulged to parents).
Our study included self-selected groups of young people and professionals with a particular interest in TYA cancer care. This may have biased selection of key components. Despite this limitation, the method of data collection allowed group interaction, which facilitated discussion. However, one challenge encountered was managing those with strong opinions. Skillful facilitation was required to ensure all participants had the opportunity to express their opinion. Flexibility was also required to allow participants to make their own interpretation of the instructions. All but one team inserted multiple cards rather than one per box. Stricter facilitation could have potentially curtailed discussion.
NICE guidance drives the development of services for young people with cancer in England and Wales, including provision of age-appropriate facilities. 1 Providing such services is truly challenging for professionals, and young people's perceptions of “age appropriate” varies according to life-stage commitments. Caution needs to be taken not to raise young people's expectations of what TYA cancer units can deliver. As the United Kingdom is at the forefront of TYA cancer care with specialist units being provided for through charitable funds, 5 we have a responsibility to evaluate these services systematically. In turn, such evaluation will provide the evidence for service development in other countries. In a cost-conscious era, identifying the essential components to optimize outcome is paramount. Our study has highlighted key components of specialist cancer units as identified by users and providers of TYA cancers services in England.
This description is important for a number of reasons. It adds to the emerging evidence about what young people and professionals consider important features of a TYA cancer unit. Such descriptions can inform quality checklists that professionals can use to evaluate their service. Young people can use them when deciding on their satisfaction with care. In countries where TYA cancer care is beginning to emerge as a distinct specialty and where decisions need to be made in relation to the environment, the make-up of the core multi-professional team, and approaches to care, it can help inform and prioritize choices. Based on the findings of this study, a definition of specialist TYA cancer units is proposed:
…a philosophy of expert cancer care which addresses the physical and psychosocial needs of young people with cancer. This is delivered in a dedicated unit, providing age-appropriate holistic care with access to a range of experts and peer support. As a consequence, the potential for young people to have a healthy physical and psychological survival will be maximized.
Footnotes
Acknowledgments
This study was funded by Teenage Cancer Trust and was undertaken at UCLH/UCL, who received a proportion of funding from the Department of Health's NIHR Biomedical Research Centre's funding scheme. Teenage Cancer Trust had no involvement in the design, conduct, or reporting of the study.
The authors would like to thank Professor Tim Eden, the young people, and the TYA community who participated wholeheartedly in the workshops. We would also like to thank the Steering Committee and participants of the “Find Your Sense of Tumour” 2010 patient conference.
This study was presented as an oral presentation at the 2010 Teenagers and Young Adults with Cancer (TYAC) Winter Education Day in Bristol, United Kingdom.
Author Disclosure Statement
Lorna Fern and Rachel Taylor are funded through grants from Teenage Cancer Trust; otherwise no competing financial interests exist.
*
Precise details of professionals are not provided to maintain anonymity.