
Abstract
This paper, summarizing the March 2012 presentation at the second international workshop of the Canadian Task Force on Adolescents and Young Adults with Cancer, describes the situation in Italy concerning the inadequate access to optimal cancer services for adolescents, and the need to improve the quality of care for these patients while investing in more research on the diseases that afflict them. National actions to bridge the gap in care and implement specific programs tailored to these patients arose from the pediatric oncology community. These actions include creation of the national Committee on Adolescents of the Associazione Italiana Ematologia Oncologia Pediatrica (AIEOP), founded with the mission of ensuring that Italian adolescents with cancer have prompt, adequate, and equitable access to the best care to optimize their treatment outcome and quality of life. Also developed was the Youth Project of the pediatric oncology unit at the Istituto Nazionale Tumori in Milan, which is currently dedicated to adolescents aged 15–19 years old and may eventually serve young adults up to the age of 25 that are affected by pediatric-type tumors.
The adequate management of adolescents with cancer—such as coping with their complex psychological and social needs, providing age-appropriate facilities, and their inclusion in clinical trials—remains a challenge that requires broad-based schemes involving not only healthcare providers, public awareness, or the cooperative groups running clinical trials but also national and local governments. The most relevant international programs dedicated to AYAs were begun some years ago, largely starting in the United Kingdom and United States and then later in Australia and Canada.9–15 In 2006, our group became formally involved in the International Working Group on Adolescent/Teenage and Young Adult Oncology, developed under the auspices of the International Society of Paediatric Oncology (SIOP). 16 The following year, a project dedicated to adolescents was launched by the Associazione Italiana Ematologia Oncologia Pediatrica (AIEOP; www.aieop.org), the national pediatric oncology association founded in the late 1970s that involves all 49 pediatric oncology centers in Italy and promotes multicenter clinical trials and other research. A formal AIEOP Committee on Adolescents was officially established in 2010.
The Italian AIEOP Committee on Adolescents
In light of previous research indicating adolescents' limited access to dedicated cancer centers and under-accrual into clinical trials,2–6 the AIEOP Committee on Adolescents' first objective was to investigate whether this was true also in our country. With this aim, we compared the number of 15–19-year-old cancer patients treated at AIEOP-affiliated pediatric oncology centers (as recorded in their hospital-based registries, the so-called “model 1.01”) to the number of cases expected to occur in Italy based on incidence rates obtained from population-based cancer registries (Associazione Italiana dei Registri Tumori [AIRTUM]). 17 The ratio of observed to expected (O/E) adolescents was compared to that in children aged 0–14 years old. The study included more than 22,000 cases registered in the model 1.01, of whom 1743 were adolescents. It found the O/E ratio was only 0.10 for adolescents, as opposed to 0.77 for children (Fig. 1). 17 This ratio increased gradually from 0.05 to 0.18 over the years (three successive 6-year study periods, from 1989 to 2006, were considered for the analysis), and was higher for certain tumor types (e.g., sarcomas). This study focused only on adolescents treated within pediatric oncology centers, representing only the view of the Italian pediatric oncology world on the problem of access to optimal care. No data on where and how patients not seen in AIEOP centers had been treated were available, and it is possible, in principle, that some of them were enrolled in clinical trials for adults. Nevertheless, this report emphasized that the AIEOP network was far less effective in serving adolescents than children.
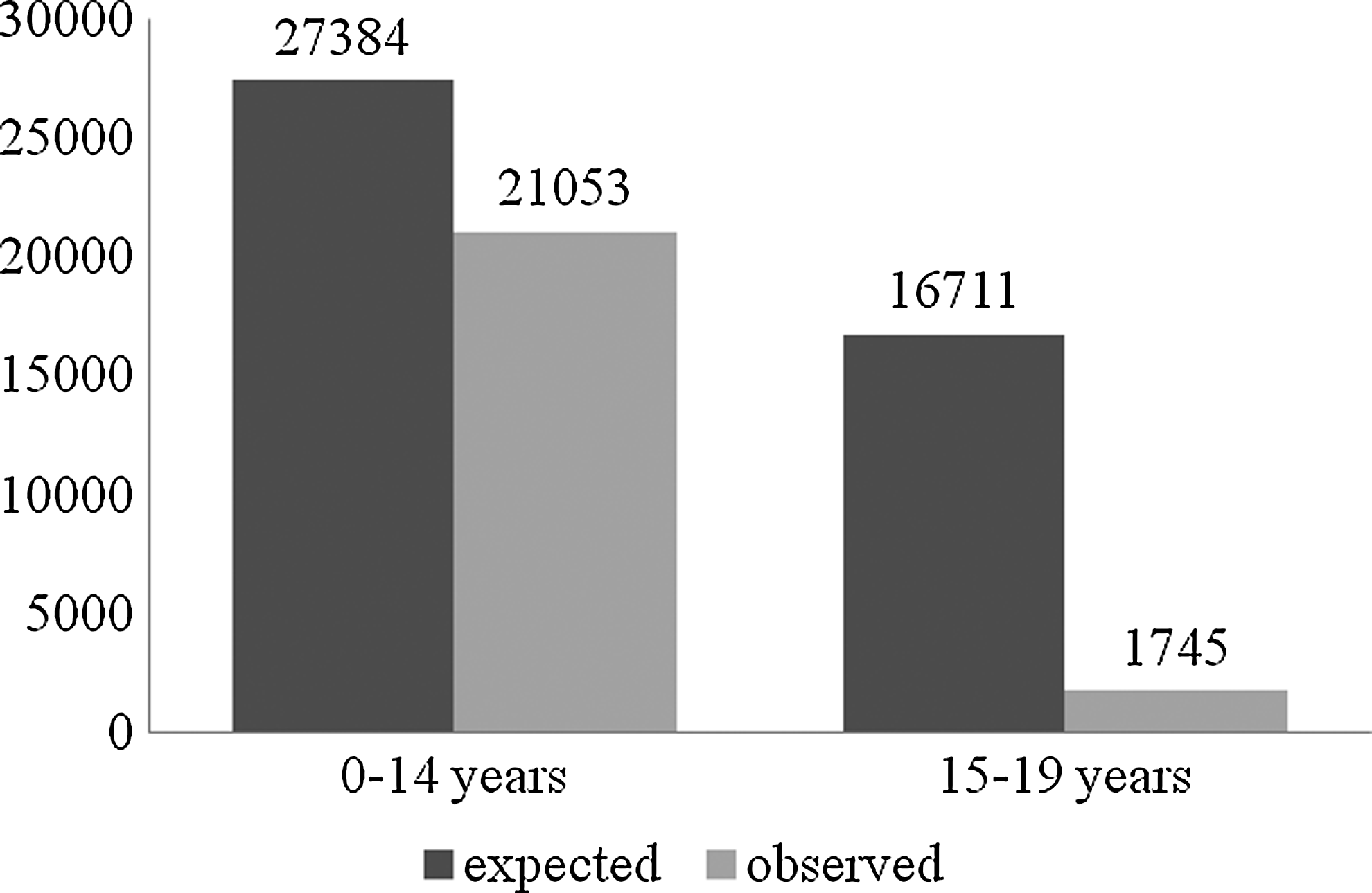
Comparison of the number of observed (treated in AIEOP-affiliated pediatric oncology centers) and expected (based on epidemiological data) cancer cases in children aged 0–14 and adolescents aged 15–19, Italy, 1989–2006. AIEOP, Associazione Italiana Ematologia Oncologia Pediatrica.
Age limits and issues of referral and delays in diagnosis in Italy
Given these results, the AIEOP Committee on Adolescents launched a survey to investigate whether a possible reason adolescents were not accessing AIEOP units was the existence of rigid upper age limits for admission to pediatric cancer units and pediatric hospitals. This study showed great variability in the age limits adopted at AIEOP centers, finding that among the 36 pediatric oncology centers participating in the survey (73% of all AIEOP centers), 46% used upper limits as low as 16, 15, or even 14 years old, while 39% placed a limit of 18 years of age. 18 Only a minority of centers reported having no upper age limit. In principle, AIEOP units with such age cut-offs should reject patients over the upper age limit even if they suffer from tumors typical of childhood, such as rhabdomyosarcoma or acute lymphoblastic leukemia, though 10 centers reported that their age limit was not necessarily binding. 18 A correlation existed between the presence of an upper age limit at an AIEOP center and the overall number of adolescents they treated, that is, centers with age limits fixed at 18 saw a limited number of not only 18-year-old patients but also those aged 15–17. As a further finding, the analysis reported that one-third of the centers did not continue treating their patients if a patient suffered a relapse past the age of 18, even if the patient had a pediatric-type neoplasm. 18
A further study on rhabdomyosarcoma confirmed the problem of referral to pediatric oncology centers for adolescents affected by this typical pediatric malignancy: adolescent patients were usually not referred to pediatric oncology units (O/E ratio of 0.27, compared to 0.9 in children), and even when they were, they often arrived after a considerable delay (the median latency period for adolescents was twice as long as for children, 8 vs. 4 weeks, p<0.0001), 19 which likely affected their chances of cure. 20 Again, no data existed on where and how adolescents not managed at AIEOP centers were treated, but some reports give reasons to worry about the quality of care for adolescents in Italy with rhabdomyosarcoma who are treated outside pediatric oncology centers. 21
A further prospective study of 425 patients (28% of them adolescents) with all types of solid tumor confirmed that adolescents are often diagnosed with longer delays as compared to children: the median symptom interval was 47 days for patients aged 0–14 years, and 137 days for those ≥15 years old. 22 The analysis also showed that both components of symptom interval—patient delay (time from symptom onset to first contact with a doctor) and referral delay (time from first doctor visit to assessment by an oncologist)—were significantly longer for adolescents than for younger patients. 22 This finding is probably influenced by teenagers' (and their families') limited awareness that the AYA might have cancer, but also by the inadequate awareness of medical providers, 22 suggesting that corrective actions would be necessary at multiple levels (e.g., educational measures for teenagers and their families or designed for school staff, training programs for healthcare operators, university courses, or refresher courses for general practitioners).
Other analyses focusing on pediatric soft-tissue sarcomas—tumors that may occur in young children as well as in older adolescents—confirmed the finding that the AIEOP network has been more effective in serving children than adolescents. The pattern of cases registered in the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG) database, in fact, changed according to the “type” of center: at pediatric oncology units that are part of children's hospitals (the most common arrangement in Italy), the median age of patients they treated was 4 years old, and they rarely treated adolescents. The median age in years of registered cases was 10 for the pediatric oncology unit at Padova University Hospital (a large comprehensive general hospital) and 14 for the pediatric oncology unit at the Istituto Nazionale Tumori in Milan (INT, the only Italian pediatric oncology unit forming part of a large cancer hospital). 23
Mission of the AIEOP Committee on Adolescents
With these findings in mind, the AIEOP Committee on Adolescents defined its strategy, with a mission to ensure that Italian adolescents with cancer have prompt, adequate, and equitable access to the best care in order to optimize their treatment outcomes and quality of life. Increasing the number of adolescents referred to pediatric oncology units was declared as the first objective. However, it was clear that for this to occur, pediatric centers must demonstrate commitment, such as having the adequate infrastructure for clinical trials access, age-appropriate psychosocial teams, supportive care projects, fertility programs, and plans for transitions in care. An official document has been prepared by the Committee on Adolescents for submission to the AIEOP centers' administrations and boards, with the hope of removing administrative barriers and raising the institutions' upper age limits for patient admission.
Given the major aim of the Committee, for practical purposes, we have decided to focus on an age range that can be managed in the pediatric setting: adolescents (15–19 years old) and young adults (20–24 years old) with pediatric-type tumors.
Three further aims have been identified as priorities of the Committee:
1. Improving awareness: A communication strategy has been defined for different target groups (general community, family physicians, oncologists, and medical institutions). Different formal press releases were launched, and various conferences and media interviews have been organized. A document has also been prepared to send to the Ministry of Health, universities, and hospitals. A brief documentary video on the issue of access to care for AYAs was created and uploaded on YouTube (http://youtu.be/5WO26cV1qPc), followed by other informative videos on the different tumor types occurring in this age group (www.infoadolescentietumori.it). 24 Partnerships with charities and testimonials are also planned.
2. Cooperation with adult medical oncologists: When an adolescent with a pediatric-type tumor is not directly treated in an AIEOP pediatric oncology center (and therefore is treated in an adult oncology setting), there should be an effort to treat the patient through close cooperation between the pediatric and the adult oncologists, adopting a pediatric protocol or a pediatric-like approach. A structured program aiming to implement the cooperation of AIEOP with adult oncology groups has been started. As a first step, the AIEOP Committee has focused on soft-tissue sarcomas. 25 The goal of developing a prospective observational study for adult rhabdomyosarcoma was achieved through a collaboration with the Italian Sarcoma Group and the Rete Tumori Rari (Italian Rare Tumor Network).
3. Addressing other specific issues: Links have been established with other AIEOP disease-specific working groups to define adolescent-specific aims in their protocols. Adolescent-focused biological studies have been planned, and a comprehensive project on fertility preservation has been started. Furthermore, the AIEOP Committee has started to involve various stakeholders to foster the implementation of its activities, including organizations for nursesand family physicians, survivor groups, advocacy organizations, cancer agencies, and universities. In particular, cooperation has been improved with the confederation of organizations for parents of pediatric and adolescent cancer patients (Federazione Italiana Associazioni Genitori Oncoematologia Pediatrica [FIAGOP]; www.fiagop.it).
Local Projects
Youth Area Project of the Centro di Riferimento Oncologico in Aviano
Until recently, few centers in continental Europe had attempted to start programs specifically tailored to AYAs with cancer. In Italy, the Youth Area Project of the Centro di Riferimento Oncologico in Aviano was a pioneering experience (www.areagiovanicro.it). Started in January 2007 and dedicated to 14–24 year olds, this project developed within an adult medical oncologist setting and was devised with a trans-departmental dimension, rather than as the “property” of a single department with different specialists retaining their own roles and specialties. 8
Youth Project at the Istituto Nazionale Tumori in Milan
A further initiative is the Youth Project developed by the Pediatric Oncology Unit at INT. 26 Founded in 1925, INT is the largest cancer hospital in Italy. Its pediatric oncology unit has beds for 23 inpatients and 12 outpatients, and treats more than 250 new solid-tumor patients a year. Being part of a large cancer hospital has facilitated the development of close cooperation with the hospital divisions dedicated to cancers in adults, enabling the pediatric unit to gain particular experience in certain tumor types (e.g., bone and soft-tissue sarcomas) across the pediatric and adult age groups,27,28 in adult-type tumors occurring in children,29–31 and in pediatric tumors occurring in young adults.32–34 Some years ago, it was decided not to consider any upper age limit for admitting patients with pediatric cancers to the pediatric unit, and this has meant that a large number of adolescents, as well as patients up to 25 or even 30 years old with pediatric-type tumors, have been referred to INT's pediatric unit. For example, among 4110 newly diagnosed patients treated between 1985 and 2010, 880 were 15–19 years old and 206 were older than 20 (26% of all cases were over 15 years of age). 26 Among all Italian pediatric centers, 40% of solid-tumor patients registered in the AIEOP database from 1989 to 2006 who were more than 15 years old were treated at INT (nearly one in two cases of brain tumors as well as soft-tissue and bone sarcomas). 26 In other words, a particular focus on adolescents has been a feature of the pediatric oncology unit at INT for many years, long before any formal youth project was developed.
In such a period of worldwide economic crisis, an initial proposal to create a new unit at INT tailored specifically for AYAs was considered infeasible for administrative, logistic, and—moreover—economic reasons. Therefore, a dedicated program within the pediatric oncology unit was developed as an offshoot of our existing activities, without requiring major changes to the hospital's organizational structure, hiring new professional staff, or new demands on the institution's administration and board. In November 2011, the Youth Project officially launched with a conference entitled “Sex, Chemo and Rock ’n’ Roll” and a focus on AYAs aged 15–24 years old with pediatric-type solid tumors (www.ilprogettogiovani.it). The project requires that patients in this age range are admitted to the pediatric oncology inpatient and outpatient wards, and managed by the same multidisciplinary staff as children, but dedicated access to particular services is available.
In particular, new customized arrangements have been implemented concerning:
a. Psychological support: Three clinical psychology specialists are permanent staff members, available on a daily basis in the pediatric oncology unit, two of whom are dedicated specifically to AYA patients and to research areas such as informed consent for minors (particularly regarding phase I–II clinical trials), quality of life, personality, diagnostic delay, and spiritual needs of AYAs.35–37 A large project focusing on returning to school after a cancer diagnosis and treatment led to the production of a professional movie about teenagers with cancer, “I Like that Tall Guy with the Crutches.”
b. School and job support: The hospital-based school and home schooling programs provide four teachers (three for high school) and five educators as part of the pediatric oncology unit's team; a social worker is dedicated to addressing problems related to young adults' jobs.
c. Fertility preserving facilities: A new oocyte cryopreservation program has been started.
d. Access to care after cancer therapy: Long-term survivors continue to be managed by the unit, and two permanent staff members are dedicated especially to this service. Patients have different follow-up programs according to their risk of late effects, irrespective of their age. Special programs include neurological rehabilitation for brain tumor survivors, 38 cardiologic monitoring, endocrine functional surveillance, and early breast cancer screening after radiotherapy to the chest wall.
Since the pediatric oncology unit was originally designed for children, the Youth Project has provided suitably equipped, multifunctional dedicated rooms where AYAs can socialize and occupy their time in recreational activities, including a gym, or study. The rooms contain computers; internet connections; musical instruments; a library with books, magazines, and DVDs; a radio station for a broadcasting channel managed by patients; and a corner for face makeup. These new spaces have been developed by converting three rooms previously used for other purposes. “Magic Time” is the format that includes activities, events, and courses (e.g., arts, photography, music, and new technologies), with special attention paid to sports. A current activity involves various professionals working with the patients to develop a stylist collection made by the patients, which has its own brand (B.LIVE), a planned fashion parade, and a book.
Notably, these two local projects developed in Italy—the Youth Area Project in Aviano and the Youth Project in Milan—have many similarities, but arose in completely different local settings (from the medical oncology and pediatric oncology sides). The effort to establish a fruitful cooperation between pediatric and adult medical oncologists is a common denominator of the two projects, regardless of their origins, and a key element for achieving a successful program. The hope is that these two examples may influence other Italian oncology centers to dedicate attention and resources to AYA patients, regardless of whether they are in a pediatric or adult unit.
Conclusion
The necessity to bridge the gap in the quality of professional care for adolescents with cancer is currently a major challenge and a primary objective for the Italian pediatric oncology world. Various steps have already been taken, but it is clear that a more ambitious and forward-thinking vision is necessary to establish a large, effective, and comprehensive national program.
Three further actions are needed and are currently ongoing:
1. Fully involve adult medical oncology groups in the national task force: The aim is to evolve from a pediatric oncology-based committee on adolescents to a national broad-based task force dedicated to adolescents and young adults, forming an official structure which can be accessed by public authorities.
2. Achieve the Ministry of Health's formal support: While the most relevant international programs dedicated to AYAs are supported by national organizations and governments,9–14 Italy is rather far from this. The national task force is currently working on a document highlighting the specific needs of AYAs, their required special attention, and the need for collaboration between adult and pediatric oncologists and to increase the quality of care and level of research promotion. It is hoped that this document will be included in the next National Oncologic Plan (Piano Oncologico Nazionale). We hope to clearly define the specific criteria and required facilites to allow centers—whether they are pediatric or adult units—to treat adolescents with cancer. These include: no restrictive age cut-offs, multidisciplinary teams, active cooperation between pediatric and adult oncologists, clinical trial availability, adequate settings (dedicated spaces with privacy), adequate staff (coordinating nurses, social workers, psychologists, teachers, activity organizers), fertility preservation programs, and transition programs.
3. Establish cooperation and network with other international groups involved in the field of adolescent and young adult oncology.
Footnotes
Acknowledgments
The author is grateful to the Associazione Bianca Garavaglia and the Near/Magica Cleme Foundation for supporting the Youth Project at the Pediatric Oncology Unit of the Istituto Nazionale Tumori of Milan. Thanks are also due to Maura Massimino, Director of the Pediatric Oncology Unit of the Istituto Nazionale Tumori of Milan, for her strong support of the Youth Project, and to all the colleagues and other stakeholders working in Milan and as part of the Committee on Adolescents of the Associazione Italiana Ematologia Oncologia Pediatrica. Finally, the author thanks Drs. Archie Bleyer, Ronnie Barr, and Karen Albritton, sources of precious advice and continuous inspiration for our activities in adolescent and young adult oncology.
Author Disclosure Statement
No competing financial interests exist.