
Abstract
An 18-year-old presented with a large, high-grade osteosarcoma of the proximal femur and multiple primary pulmonary metastases. The tumor responded poorly to preoperative chemotherapy. Four thoracotomies to remove 24 metastases were necessary to achieve a first complete remission. An early pulmonary recurrence was again treated by thoracotomy and systemic therapy. The patient remained in second complete remission at the last follow-up, 76 months after post-diagnosis and 53 months after pulmonary recurrence. This case illustrates that some patients with osteosarcoma and extremely doubtful prognosis may be cured, provided the treatment concept includes aggressive surgery for both the primary tumor and metastatic disease.
Case Report
After a history of several weeks of increasing pain and later swelling of the thigh, an 18-year-old male presented to our pediatric and adolescent oncology unit with a large tumor of the left proximal femur. Conventional X-rays and magnetic resonance imaging (MRI) were suggestive of osteosarcoma (Fig. 1); the initial tumor volume estimated by MRI was 1800 cm3. Multiple bilateral partially ossifying pulmonary metastases with a diameter of up to 1.5 cm were evident on plain X-rays and computed tomography (CT) of the chest (Fig. 2); the 99mTc bone scan was without evidence of bone metastases. Two biopsies of the primary tumor were performed, and it was finally classified as a predominantly chondroblastic, high-grade osteosarcoma with some osteoblastic areas. Prior to initiation of therapy, the serum alkaline phosphatase was markedly increased at 2110 U/L (upper limit of normal [ULN]: 130 U/L).
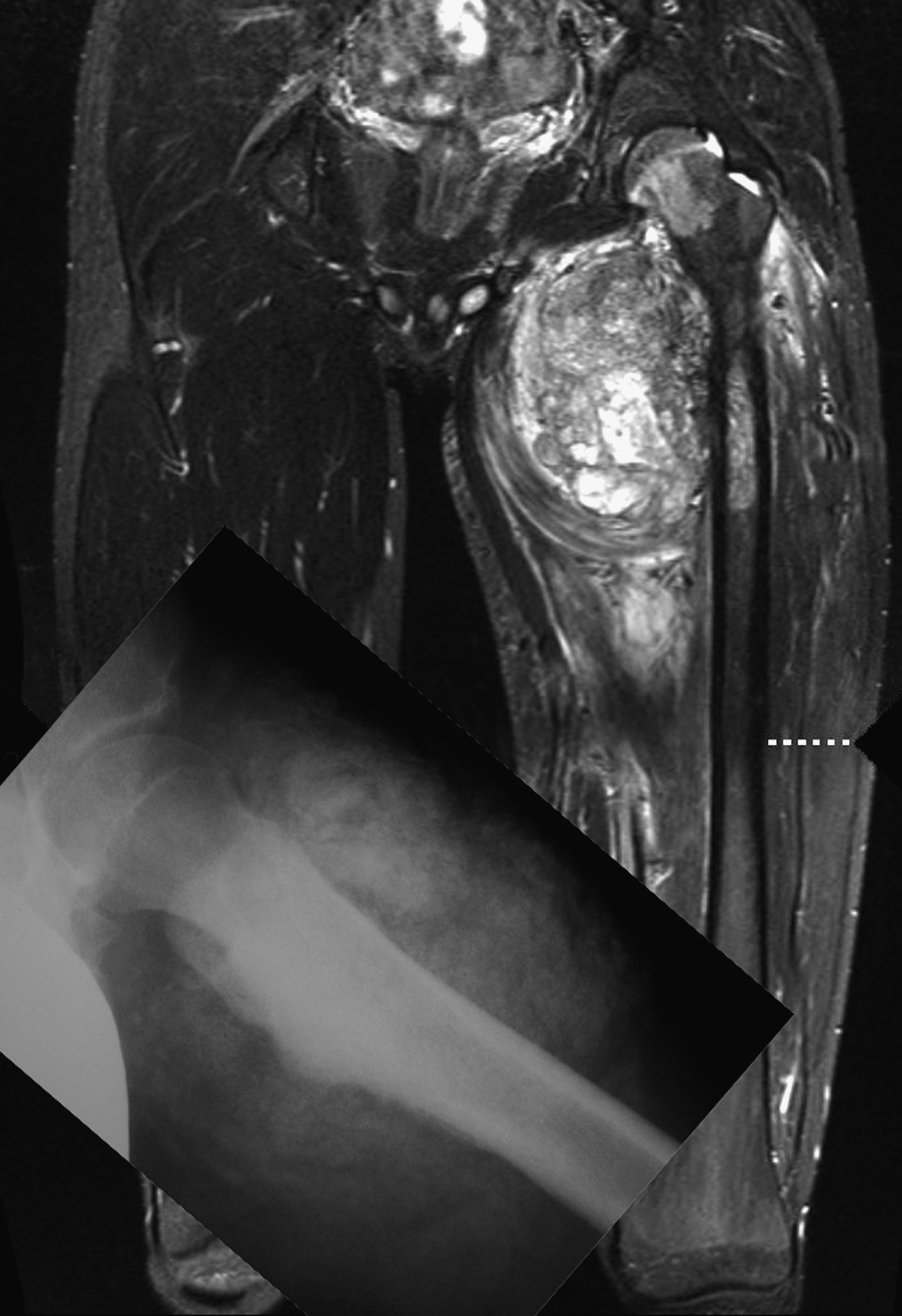
Primary tumor: magnetic resonance imaging (MRI) of both hips and thighs at presentation. Coronal short T1 inversion recovery (STIR), 4 mm. Large soft tissue mass medial in the left thigh involving the proximal femur and the hip joint. The inserted lateral (Lauenstein) view of the left hip shows amorphous sclerosis and indistinct margins of the proximal femur and cloud-like calcifications in the surrounding soft tissue.

Primary lung metastases: computed tomography (CT) of the chest at presentation. The section above the level of the diaphragm shows four of multiple metastases (arrows) on both sides. (Image courtesy of GM Richter, Department of Radiology, Klinikum Stuttgart—Katharinenhospital, Germany).
In May 2006, the patient was started on neoadjuvant induction chemotherapy with high-dose methotrexate, doxorubicin (adriamycin), and cisplatin (MAP), following the regimen used in the current EURAMOS-1/AOST0331 trial. 1 He was not included in the trial itself because several entry criteria were not met: a differential diagnosis of a periosteal variant of osteosarcoma was considered (later definitively refuted by reference pathology of the resected specimen), and it was unclear whether the widespread pulmonary metastases would become resectable.
During preoperative therapy, pain related to the primary tumor improved, and there was a slight reduction of the observed swelling. The size and number of pulmonary metastases, however, remained unaltered upon imaging. A wide resection of the primary tumor was performed at week 16 of treatment, with reconstruction by rotationplasty type IIb, as described by Winkelmann. 2 Multiple postoperative complications necessitated three revision operations in the first 2 weeks after tumor surgery, and finally resulted in severe atrophy, complete loss of function, and loss of almost all sensation of the left lower extremity. Histopathology of the resected tumor specimen revealed wide resection margins, but response to preoperative chemotherapy was poor, with 10%–20% viable tumor cells remaining, corresponding to regression grade 4 according to the six-grade scale of Salzer-Kuntschik or grade 3 according to the four-grade Huvos classification.3,4 Postoperatively, adjuvant chemotherapy was continued until week 57. We intended to use MAP, but multiple delays and modifications of the treatment plan became necessary because of surgical complications and chemotherapy toxicity.
At weeks 29 and week 34, respectively, left- and right-sided thoracotomies were performed. Twenty-one histologically proven, mostly viable primary metastases were removed; 12 from the left lung and 9 from the right. Unfortunately, postoperative CT scans suggested that residual metastases remained. A complete remission upon imaging was only achieved after two additional right-sided thoracotomies (week 52: nine resections, two of these with viable metastases; week 63: seven resections, one histologically proven metastasis). Afterwards, the chest CT was without evidence of residual metastases. Therefore a total of 24 histologically proven metastases were removed during four thoracotomies (one left, three right) before a first complete surgical remission was achieved.
Twenty-two months after initial diagnosis, 8 months after the fourth thoracotomy, and 10 months after the end of adjuvant chemotherapy, the patient developed a recurrence in the form of bilateral pulmonary metastases (Fig. 3). Complete restaging was without evidence of local recurrence or extrathoracic metastases. Both lungs were again operated upon by open thoracotomy. Two viable metastases were removed from the left lung by wedge resection. A metastasis measuring 4.5 cm in diameter with vascular invasion was removed by total resection of the right lower lobe, and histological evaluation also identified an involved lymph node adjacent to and removed with the resection specimen. Postoperative CT imaging of the thorax suggested that a second complete surgical remission had been achieved.

Lung metastases at first recurrence: anterior radiograph of the chest 10 months after neoadjuvant chemotherapy showing large round metastases (arrows) in the lower parts of the right lung, which were partly hidden by linear densities caused by scars after thoracotomy for the primary pulmonary metastases.
As we considered the patient to be at very high risk for a second relapse, options for adjuvant treatment were discussed. The patient went on to receive pegylated interferon alpha-2b (PegIntron®, 1×70 μg subcutaneously once weekly) for 1.5 years, when it was discontinued because of recurrent liver enzyme elevations. Afterwards, regular follow-up by imaging was continued starting every 2 months and subsequently decreased to every 3 months. At the last follow-up, 76 months after primary diagnosis and 53 months after diagnosis of pulmonary recurrence, the patient remained in continuous second complete remission. He led an active life, had completed his primary education and was now a university student, and had managed to become a state champion Paralympic swimmer less than a year after his last thoracotomy.
Discussion and Conclusion
Osteosarcoma is the most frequent primary bone sarcoma and one of the most typical cancers of adolescents and young adults. Treatment is by surgical excision and chemotherapy, usually divided into a pre- and postoperative phase. With current multimodal treatment, 5-year survival expectancies up to and above 70% can be achieved in patients with localized, resectable extremity osteosarcomas.5,6 A large primary tumor, proximal site within the affected extremity, and marked increases of serum alkaline phosphatase levels are well-defined adverse prognostic factors.7,8 The extent of chemotherapy-induced tumor response also has major prognostic implications in osteosarcoma, and patients whose primary tumors respond poorly (usually defined as >10% viable tumor in the resected specimen) fare significantly worse than good responders.5,7 The patient described here had all of these unfavorable prognostic factors. In addition, he presented with multiple metastases to both lungs. Our Cooperative Osteosarcoma Study Group (COSS) has observed a 5-year overall survival expectancy of 23% and a 5-year event-free survival probability of only 3% for patients presenting with more than five metastatic lesions. 9 In summary, we may conclude that the young man's chances for cure seemed remote when he first presented.
Regardless of all other prognostic factors, complete surgical removal of the primary and all detectable metastatic lesions must almost be considered a prerequisite for curing osteosarcoma.9–11 Open thoracotomy with manual palpation is required to detect small lesions that might be not be obvious upon imaging and could be missed by less invasive techniques, such as video-assisted thoracoscopic surgery.12,13
The most common site of osteosarcoma recurrence is the lungs.14–17 Prognosis is poor, and considerably fewer than 30% of affected patients will survive beyond 5 years. A short disease-free interval, more than one or two metastases at recurrence, and bilateral pulmonary involvement are associated with particularly unfavorable outcomes.17,18 Again, complete surgical resection of all metastases is largely a prerequisite for cure.17–19 The role of second-line systemic treatment remains ill-defined. While several series suggest that patients with unresectable metastases might survive somewhat longer if treated by second-line chemotherapy, the role of second-line adjuvant treatment remains controversial.17,18
We believe that surgery should be discussed with all osteosarcoma patients whose metastases can be considered resectable—regardless of their number, almost regardless of their site, and regardless of whether it is initial presentation, or first-, second-, or even subsequent relapse. The discussion with patients and their families should, of course, be quite frank. The considerable uncertainties concerning systemic adjuvant therapies for recurrent osteosarcoma must be addressed. The chances aggressive surgery can offer should not be exaggerated, but they should also not be denied. In this context of cure being possible only with complete removal of all lesions, which patients should not proceed to surgery? Pleural or even chest wall involvement by lung metastases heralds a very poor prognosis even with seemingly complete surgery, and this must be taken into account during the decision-making process. However, we would not consider it an absolute contraindication to surgery. Very brief intervals between previous disease episodes might also argue against immediate thoracotomy, as the next recurrence will be looming in the very near future 20 if no additional effective systemic treatments are available to slow down disease progression. In such situations, it is our policy to recommend chemotherapy first and to proceed to surgery only in cases without rapid progression. For all other patients with resectable metastatic osteosarcoma, we offer—and recommend—surgery. Based on our cooperative group's data,17,20 we usually also offer additional systemic treatment, but try to convey a realistic impression of just how limited its potential benefit is likely to be.
In summary, the case described above highlights the fact that aggressive surgery, repeated if necessary, may be curative for some osteosarcoma patients who, by common standards, would be considered as having an extremely poor prognosis. Multidisciplinary teams will often face the challenge of having to determine when cure is no longer a realistic option and when the primary aim of medical care should shift toward palliation. However, a remote chance for cure is not no chance at all, and this fact should not be neglected during the decision-making process.
Footnotes
Acknowledgments
The authors are grateful to the patient for allowing his case to be reported. They wish to thank the teams in Heidelberg, Stuttgart, Muenster, and Gerlingen who helped care for him.
Author Disclosure Statement
No competing financial interests exist.