
Abstract

AYA “Adherence” in the Literature
Others have reviewed and noted the limitations of the literature describing adherence among AYA oncology patients.4,5 Due to significant heterogeneity with respect to both the age of patient groups and definitions of adherence, published rates of non-adherence range from 1% to 100%.4,5 Most studies have focused solely on measures of pharmacoadherence (the extent to which a patient follows a prescribed medication regimen),6–12 with few investigating health-related behaviors or psychosocial components of adherence among AYAs.13–16 Much of the literature is decades old; authors have speculated that there is no incentive to perform new investigations because adherence rates in other AYA populations (e.g., patients with cystic fibrosis, 17 asthma, 18 diabetes, 19 or inflammatory bowel disease 20 ) are comparable to those in cancer patients. 4 Divergent methodologies further preclude a complete understanding of how to appropriately identify and intervene with non-adherent patients across the cancer continuum. 5 Indeed, providers have difficulty recognizing non-adherence or initiating appropriate interventions for non-adherent patients. 21
These challenges underscore the need for further rigorous research and also raise new questions. For example, there are no clear guidelines regarding what constitutes adequate adherence or how to reduce non-adherence. Meaningful classifications of adherence may require a spectrum that incorporates pharmacoadherence as well as other health behaviors. Additionally, we question the appropriateness of comparing oncology patients to those with other chronic diseases. A diagnosis of cancer not only carries a particular social stigma, but it also requires new life changes, challenges, and perspectives. Whereas many patients with the aforementioned chronic diseases may have had a lifetime to adapt, oncology patients must make dramatic life changes quite quickly. This adaptation is particularly challenging for AYAs, who have variable levels of active participation in the treatment process and who may more poignantly struggle with psychosocial and developmental processes than older or younger patients with cancer.
AYA Developmental Challenges
The inferior outcomes observed in AYA patients have been attributed to a variety of factors, including delays in diagnosis, 22 biological factors, 23 and poor accrual of AYA oncology patients in clinical trials. 24 These disparities may also be due to the fact that AYA patients have unique developmental needs that go unmet during their cancer experience. 25 Adolescence and young adulthood is normally characterized by distinctive challenges, transitions, choices, and milestones related to education, employment, identity, relationships, and family. 26 AYA cancer patients may miss or delay the achievement of these milestones while they are undergoing therapy. They may need to withdraw from school or work, become increasingly reliant again on parents or others for help with daily living, and move back into their childhood home. Side effects from cancer therapy may affect body image and sense of self. AYAs may feel removed or absent from life experiences that define career goals, social networks, sexuality, and self-identity. In addition, some may lack the maturity or insight to grasp the short- and long-term consequences of their illness.27,28
Patients vary in their individual responses to challenges to their autonomy during cancer therapy, but the nature of such struggles may color the relationship between AYAs, caregivers, and healthcare providers. AYAs also have distinctive styles of learning and communication that are vastly different from younger or older patients with cancer,29,30 necessitating novel approaches to the provision of optimal healthcare delivery.
Collectively, the unique developmental characteristics of the AYA period have the potential to affect adherence negatively, in turn affecting medical and psychosocial outcomes. Indeed, although the relationship between non-adherence and outcomes has never been formally described among AYA cancer patients, non-adherence among younger pediatric oncology patients is known to increase the likelihood of relapse and decrease overall survival.31,32
Improving AYA Adherence
A recent qualitative investigation among AYA oncology patients described a “process of adherence” consisting of three distinct steps. 33 To adhere to a treatment regimen, patients must: (1) recognize the threat to long-term health and well-being posed by their cancer diagnosis, (2) take control of their treatment, and (3) manage it for the duration of therapy and survivorship. Less adherent behaviors may manifest if any or all of these steps are bypassed. Contextual factors such as sociodemographics, personality, social support, and provider interactions may all contribute to ultimate adherence. Others have suggested specific strategies to promote adherence among AYAs, including individualized anticipatory guidance (e.g., individualized psychologic preparation to help relieve patients' anxiety of expected stress), ongoing monitoring, and more vigilant management when/if non-adherence is identified.4,5
While these suggestions are helpful, they fail to address the unique developmental needs and challenges of AYA patients previously mentioned.27,28 Additionally, the term “adherence” suggests collaboration between patients and providers, but the variable maturity levels and capacities for self-care among AYA patients can dramatically affect their roles as functioning members of their treatment team. Some AYAs with cancer, particularly adolescents, may feel disempowered and have a sense that treatment decisions are being dictated by healthcare providers and/or parents. Young adults attempting to manage their own care may struggle with complex treatment regimens that include frequent clinic visits and multiple medications, offering little flexibility for patient decision making. Patients may be deliberately non-adherent in an effort to exercise control and create a sense of independence.
We propose a flexible algorithm to inform clinicians of the risk of non-adherence and guide corresponding clinical care (Fig. 1). This algorithm is based on clinical observations, an understanding of AYA development, and questions raised in the existing literature. We include consideration of the patient's maturity and independence and his or her psychosocial challenges and unmet needs. This algorithm has yet to be tested in clinical research; rather, it provides a possible platform for clinicians to support patient adherence better and, in turn, improve patient outcomes. To our knowledge, no formal assessment tool of this type currently exists.
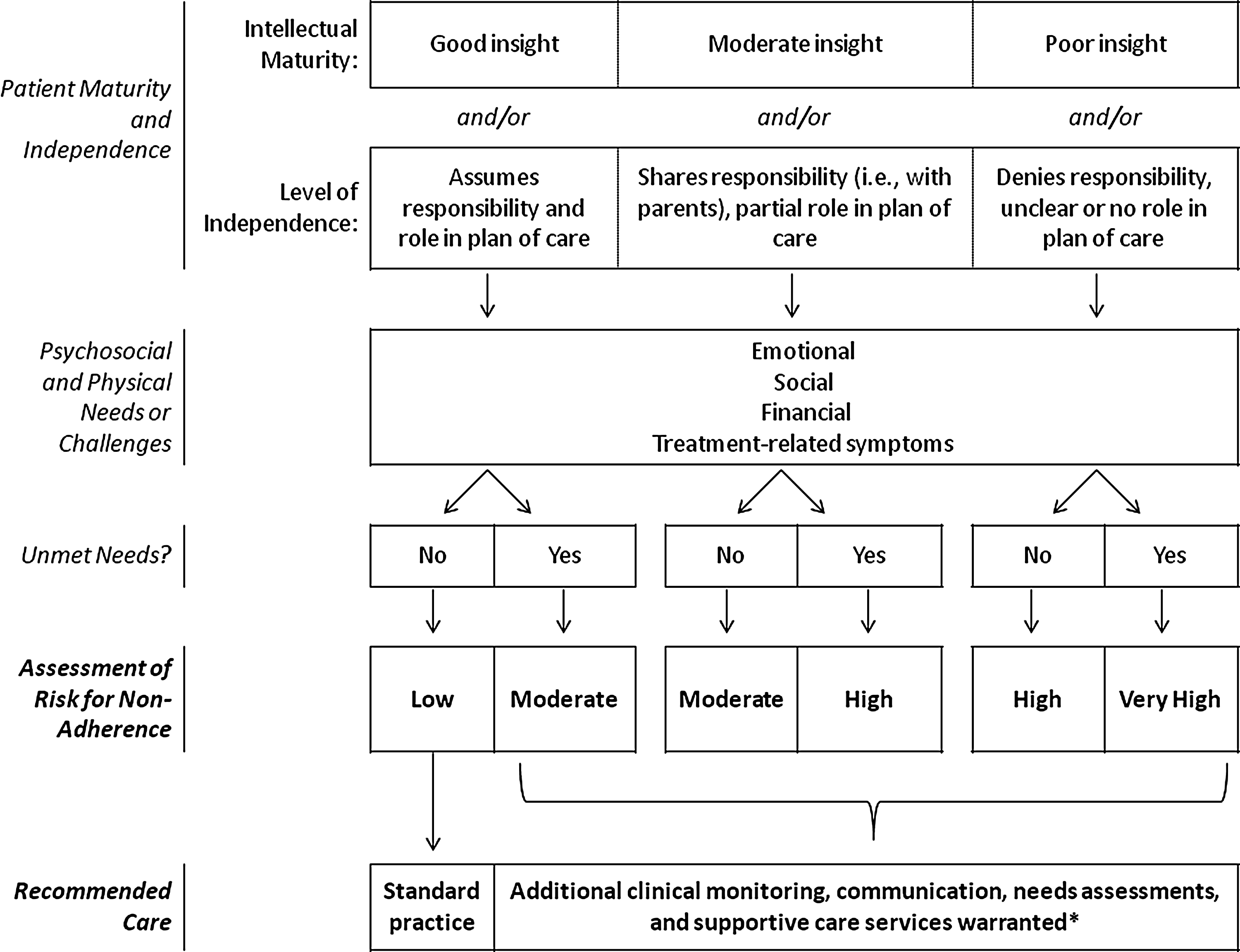
Proposed algorithm for flexible risk assessment of adherence among AYA oncology patients. *Suggested additional supportive care services depend on identified needs and may include referrals to social work, palliative care, child life, psychology, psychiatry, or chaplaincy. AYA, adolescent and young adult.
To assess the risk for non-adherence in AYAs accurately, providers must first form developmentally appropriate expectations regarding a patient's intellectual maturity and independence. For example, it might be unreasonable for providers to expect a 15-year-old patient to assume full responsibility for his cancer treatment; even older patients may lack insight into how their cancer diagnosis and treatment should affect their day-to-day choices. Providers should also consider patients' prior history of adherence as an indication of their level of independence. Second, to help patients effectively meet the demands of their treatment, the healthcare team should formally assess needs and challenges, and then direct patients to available resources (Table 1). Healthcare providers can promote adherence by recognizing and treating emotional stressors (e.g., distress or anxiety), by encouraging or identifying social support networks, by enabling important milestones to be met, and by providing resources for patients with financial hardships (e.g., medical insurance, job security, or transportation costs). Optimizing supportive care strategies to minimize treatment-related symptoms may maximize a patient's overall coping ability and potentially improve adherence. Continued unmet needs suggest greater risk; patients may not be able to prioritize their treatment over those needs. Using the approach described here, few AYA patients would be considered as “low-risk” for non-adherence. The majority of AYAs would benefit from additional clinical monitoring, communication, ongoing needs assessments, and supportive care services to enhance the therapeutic alliance and ultimately achieve better outcomes.
AYA, adolescent and young adult.
Summary
Although adherence is a topic of considerable interest in AYA oncology, current approaches to assessment and management of adherence fail to address the unique developmental needs of AYA patients. We propose that innovative and flexible assessments of AYAs' risk for non-adherence should include consideration of patient maturity and insight, as well as psychosocial needs. Further refinement of such tools should be a priority for health services researchers specializing in AYA oncology. Careful assessment of AYAs' risk for non-adherence will enable constructive collaborations between patients and providers, promote the use of innovative and individualized interventions to support AYA adherence, and ultimately contribute to superior outcomes among AYAs with cancer.
Footnotes
Acknowledgment
ARR was supported by the Ruth L. Kirschstein National Research Service Award T32CA009351.
Author Disclosure Statement
No competing financial interests exist.