
Abstract
Adenoid cystic carcinoma (ACC) accounts for only 1% of all malignant head and neck tumors, and rarely affects children or adolescents. We present a 16-year-old female patient who was diagnosed with ACC at 12 years of age. The primary tumor was located in the left parotid gland. Initial treatment consisted of surgical resection and radiation therapy. Less than two years later, she developed recurrent disease in the right cavernous sinus with pulmonary metastases. At the time of this report, she is alive with disease. Both the patient's age and pattern of metastasis are rarely reported in the literature.
A
The preferred treatment for ACC is surgical resection with negative margins. The use of postoperative radiation is common, but its benefit is debatable in the available literature.2,3,6 Disease-free survival at 5 years ranges from 57–65%.1,7 However, ACC can be an indolent malignancy, often with late local recurrence and hematogenous spread of distant metastases.1,2,7,8 Once a patient has recurred, long-term outcomes are dismal, with overall survival rates of 35%, 15%, and 0% at 5, 10, and 15 years respectively. 1 The most common site for distant metastases is the lung. Bone, liver, and brain metastases are also rarely reported.7,8
Case Report
A 12-year-old female presented to her primary care provider with a gradually enlarging lump in front of her left ear over many years and recent development of left-sided jaw pain. Initial computed tomography (CT) scan reported lymphadenopathy without suspicion of neoplasia. However, her pain continued, and magnetic resonance imaging (MRI) 3 months later revealed a 3.4 cm×4.5 cm mass in the left parapharyngeal space with erosion of the mandible (Fig. 1). She underwent a left total parotidectomy, left suprahyoid neck dissection, incision of left submandibular gland, and facial nerve anastomosis using a greater auricular nerve graft. Pathology showed c-Kit positive ACC within the parotid gland with microscopic perineural invasion and positive deep tumor margins. There was a histologic predominance of a cribriform pattern with minor amounts of solid and tubular patterns (Fig. 2). Immunohistochemical staining showed positivity for p53 tumor suppressor gene expression. Adjacent minor salivary glands and lymph nodes were negative for tumor. Metastatic evaluation with a CT of the chest, abdomen, and pelvis were negative for disease. Postoperatively, she underwent 6400 cGy of intensity-modulated radiation therapy to the left parotid and salivary gland.
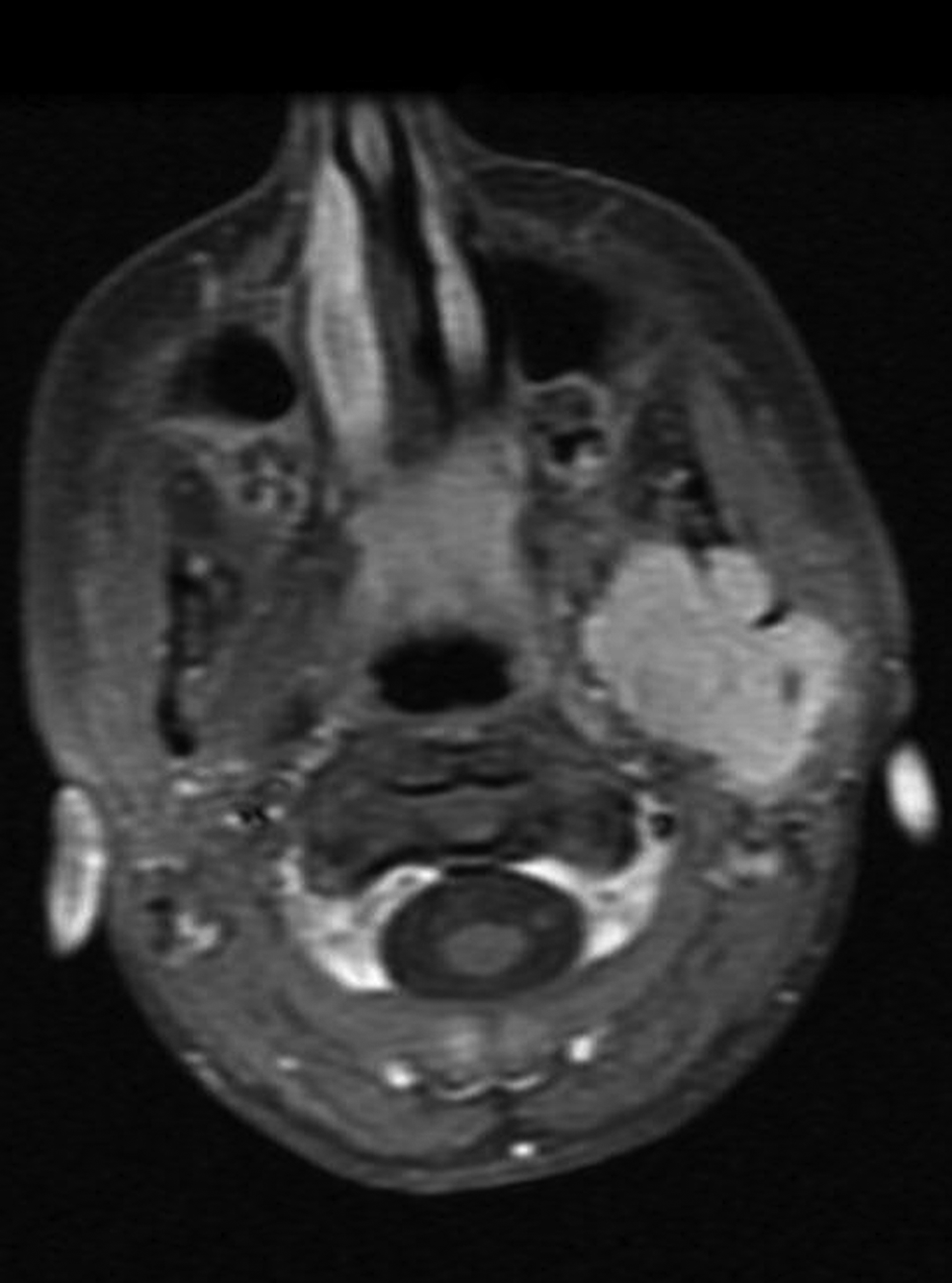
Magnetic resonance imaging performed at initial diagnosis revealing large enhancing salivary gland tumor.
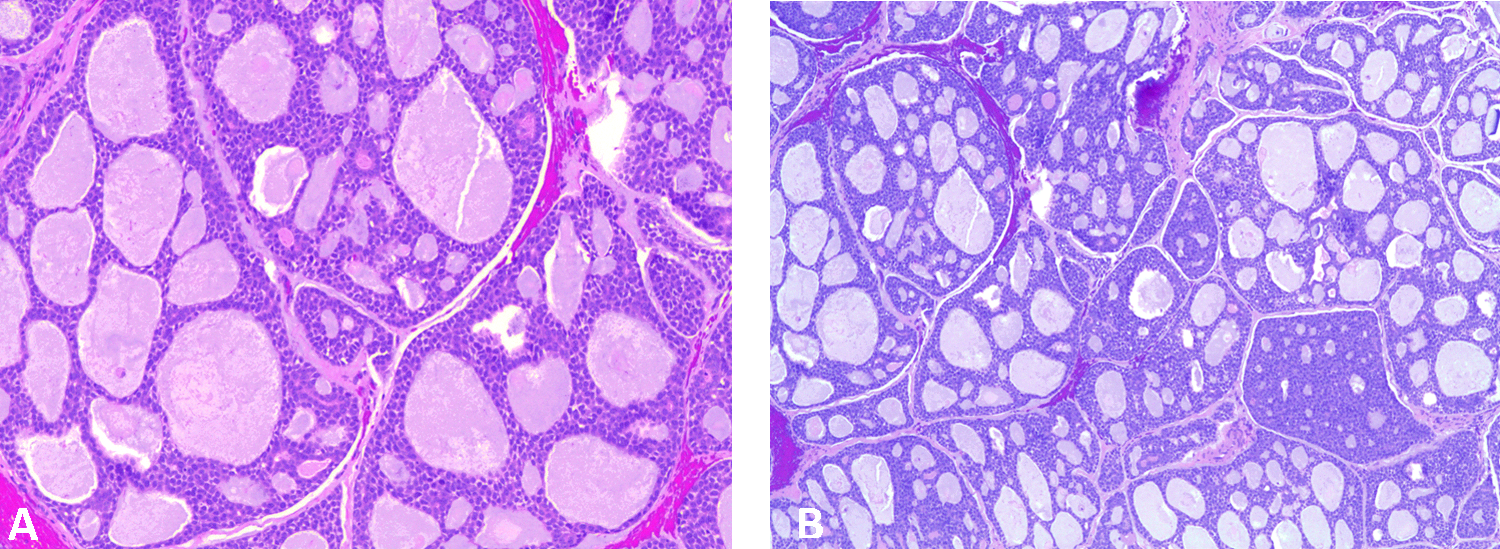
Hematoxylin and eosin stain of salivary gland tumor at diagnosis in
Seventeen months after diagnosis, there was radiographic evidence of locally recurrent disease. An image-guided fine needle aspiration confirmed recurrent ACC with similar histologic features and cribriform predominance. Exploratory surgery with multiple biopsies did not show any malignant components. Four months later, surveillance face and neck MRIs revealed a contralateral right cavernous sinus mass measuring 1.6 cm×1.2 cm×2.7 cm (Fig. 3); biopsy confirmed ACC. Again, this tumor had a cribriform predominance with minimal solid component. The patient underwent proton beam radiation therapy for local control of her cavernous sinus metastasis, which showed subsequent reduction in size. Unfortunately, CT of the thorax revealed multiple asymptomatic pulmonary nodules measuring up to 7 mm in diameter, presumed to be progressive metastatic disease.

Magnetic resonance imaging performed for routine surveillance revealing left cavernous sinus biopsy-proven adenoid cystic carcinoma.
At the time of this report, the patient is well, attending school, and exhibiting excellent quality of life. However, routine disease surveillance recently showed a recurrence in the right cavernous sinus at the periphery of the previous radiation field. The upcoming treatment plan includes surgical resection to prevent growth with symptom development. She has had minimal change in the size and number of pulmonary nodules.
Discussion
Our patient's younger age at presentation and metastatic site in the contralateral cavernous sinus are atypical features of ACC, warranting this report and review of the literature. ACC is a rare form of cancer typically seen in older adults. Data reported from the Surveillance, Epidemiology and End Results (SEER) Program for 1973–2008 showed 81.8% of patients with major salivary gland ACC were 40 years of age or older. 9 In our review, we found only a small number of reports of ACC occurring in patients under 20 years of age. Dagher et al. reported an 11-year-old male diagnosed with ACC in the lacrimal gland. The patient underwent radical exenteration of the left orbit. 10 Galliani et al. reported a 6-year-old female diagnosed with cribriform predominant ACC of the lacrimal gland with perineural spread; the patient underwent orbital exploration for diagnosis. After 18 months, she had a local recurrence undergoing a radical orbitotomy and was disease-free at 32 months from diagnosis, though one could argue this is too short a follow-up to make conclusions regarding her likelihood of long-term survival. 11 Shields et al. reported a 9-year-old boy diagnosed with cribriform predominant ACC of the lacrimal gland and treated with orbital exploration, followed by orbital brachytherapy. At the time of publication, the patient was 1 year post-diagnosis and disease-free. 12 It is interesting that case reports in pediatric and young adult populations largely represent ACC of the lacrimal gland rather than salivary or parotid glands, as in our patient. In SEER data from 1973–2008, 29% of orbital ACC occurred in patients under 40 years of age, in comparison to only 15.2% of patients with major or minor salivary gland ACC. 9 Our patient's presentation in the parotid gland is more typical of disease in older adults.1,3,9
Locoregionally invasive disease and distant metastases via hematogenous spread are not uncommon in ACC. However, in our patient both the timing and location of recurrence are of interest. Oplatek et al. reported a single institution retrospective review of 99 patients with ACC of the head and neck and a mean age at diagnosis of 54 years (range: 20–83). Fifty-three percent of patients suffered recurrence with a mean time to recurrence of 63 months, albeit with a wide confidence interval. 2 Another single institution retrospective review of 196 patients diagnosed between 1939 and 1986 with ACC of the salivary glands and a minimum follow up time of 10 years. The authors reported that distant metastases occurred at a median of 3 years, with the range of recurrence (local and distant) to be from 1 month to 19 years. 13 Our patient had her first recurrence at 17 months post-diagnosis.
Even rarer is our patient's metastasis to the contralateral cavernous sinus. Amit et al. retrospectively analyzed 489 patients treated for ACC in nine cancer centers. Only seven patients (1.4%) developed brain metastasis, compared to any distant metastasis in 111 patients (22%). 14 Cavernous sinus metastases have been reported in the literature in only two other younger patients. Huang and Lee reported a 25-year-old female with a right intranasal primary ACC with perineural spread into the ipsilateral cavernous sinus at diagnosis. 15 Kaur et al. reported a 32-year-old male whose primary tumor was on the right hard palate subsequently developed extensive bilateral head and neck disease, part of which originated from the dura and extended into the left cavernous sinus. 16
Typically, cavernous sinus and other intracranial metastases are a result of perineural invasion. However, our patient's contralateral spread seems an unlikely location for metastasis by nerves without detectable disease in the ipsilateral sinus or skull base. There is only one similar report in the literature—that of a 69-year-old male with a history of right parotid ACC presenting less than 1 year after diagnosis with a left-sided frontal lobe mass involving the frontal bone, dura, and brain parenchyma, confirmed to be ACC. Gelber et al. presumed the mechanism of contralateral spread to have been hematogenous as opposed to the more typical perineural spread of ACC. 17
Our patient presents multiple risk factors for disease progression and a poor chance for cure: her age at diagnosis was young, time to recurrence was relatively short, and her primary tumor had perineural invasion of the facial nerve at diagnosis and expressed the p53 tumor suppressor gene. Garden et al. reported retrospectively on 198 ACC patients treated at a single institution between 1962 and 1991, and concluded that perineural invasion involving a major nerve carries a higher risk of treatment failure. 18 This finding was confirmed by another review evaluating prognostic factors in 160 ACC patients. 19
Our patient's pathology has consistently shown a cribriform predominance as opposed to a solid tumor type. Multiple reports have found a >30% solid tumor histology to be a poor prognostic indicator.19–21 Less understood but potentially important in tumor aggression is the presence of p53 tumor suppressor gene expression. 22 Further investigation is required to determine how expression of p53 or other molecular markers may be important in the prognosis and classification of ACC.
Conclusion
In conclusion, we present a unique case of ACC occurring in an adolescent patient with spread to the contralateral cavernous sinus, as well as more typical hematogenous spread to the lungs and local perineural invasion. Despite multiple recurrences, disease progression, and overall poor prognosis for long-term survival, the patient remains asymptomatic with excellent quality of life with the use of surgical control and radiation therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.