
Abstract
Purpose:
To examine the perspectives of adolescent survivors of childhood cancer during the transition to early survivorship.
Methods:
An exploratory, retrospective qualitative study using a multiple case study research design was conducted with eight adolescent survivors of childhood cancer between the ages of 14 and 17 years old. Adolescents who participated in the study were off treatment for a minimum of 6 months and a maximum of 5 years. Participants completed a demographic questionnaire, a semi-structured individual interview, and a follow-up meeting. Data were analyzed using a template organizing style, immersion/crystallization approach, and cross-case analysis strategies within the context of a pediatric oncology transition conceptual framework.
Results:
Adolescent survivors perceived that their lives changed after treatment completion, but they did not define this time as a “transition.” They identified re-engagement in activities and improvement in or absence of negative residual effects of treatment as indicators of returning to normalcy. Presence of residual effects restricted adolescents' participation in desired activities and reminded them that the impact of cancer and treatment extended beyond treatment completion. Adolescents varied in their perceived need for transition care.
Conclusion:
Adolescents have a unique perspective regarding the transition to early survivorship, providing support for distinguishing them as a distinct subgroup of cancer survivors.
A
To date, few studies have investigated this transition period among adolescent cancer survivors. A qualitative pilot study using focus groups investigated the experiences during the transition to early survivorship of adolescent cancer survivors aged 14–18 years old who were 1–5 years post-treatment completion, as well as their parents and community-based primary care physicians. 3 Findings indicated adolescent survivors were in limbo as they attempted to regain a sense of normalcy and reintegrate into the school setting with peers. Adolescents and parents also perceived a lack of information about the transition process and expressed interest in receiving information about late effects and options to access psychosocial support. Adolescents generally had little knowledge of late effects and believed primary care physicians had limited knowledge of such information. 3 Another exploratory study investigated the identity development of 12 adolescent and young adult cancer survivors 12–20 years old and their perceptions of their physical and mental health during the early survivorship period. 4 Findings revealed survivors recognized that their identity development was significantly impacted by the cancer experience. Adolescent and young adult survivors straddled the line between cancer patient and survivor, often feeling uncertain about their identity, which was further complicated by daily reminders of cancer and adjustment difficulties. 4
Although these studies reveal adolescent and young adult cancer survivors face unique challenges associated with early survivorship, there is limited research regarding this transition period compared to other phases of the cancer continuum. 5 Additionally, there is often no clear distinction between completion of treatment and transition to early survivorship; therefore, it is difficult to acquire an understanding of the transition process itself and distinguish its key features. Further, there has been limited attention given to identifying transition care needs and perceived support that would make this transition successful.
Schumacher and Meleis 6 presented a framework for conceptualizing transitions based on a review of nursing literature. Wilkins and Woodgate 7 maintained the key attributes of transition but tailored content to reflect the transition experiences of siblings of pediatric cancer patients. Antecedents are conceptualized as events that initiate a transition process, which can be categorized as health-illness, developmental, or situational.6,8 Key attributes that define a transition include process, movement, disequilibrium, change, and individual perception. Further, the framework includes process and outcome indicators and consequences associated with healthy and unhealthy transitions (Fig. 1).
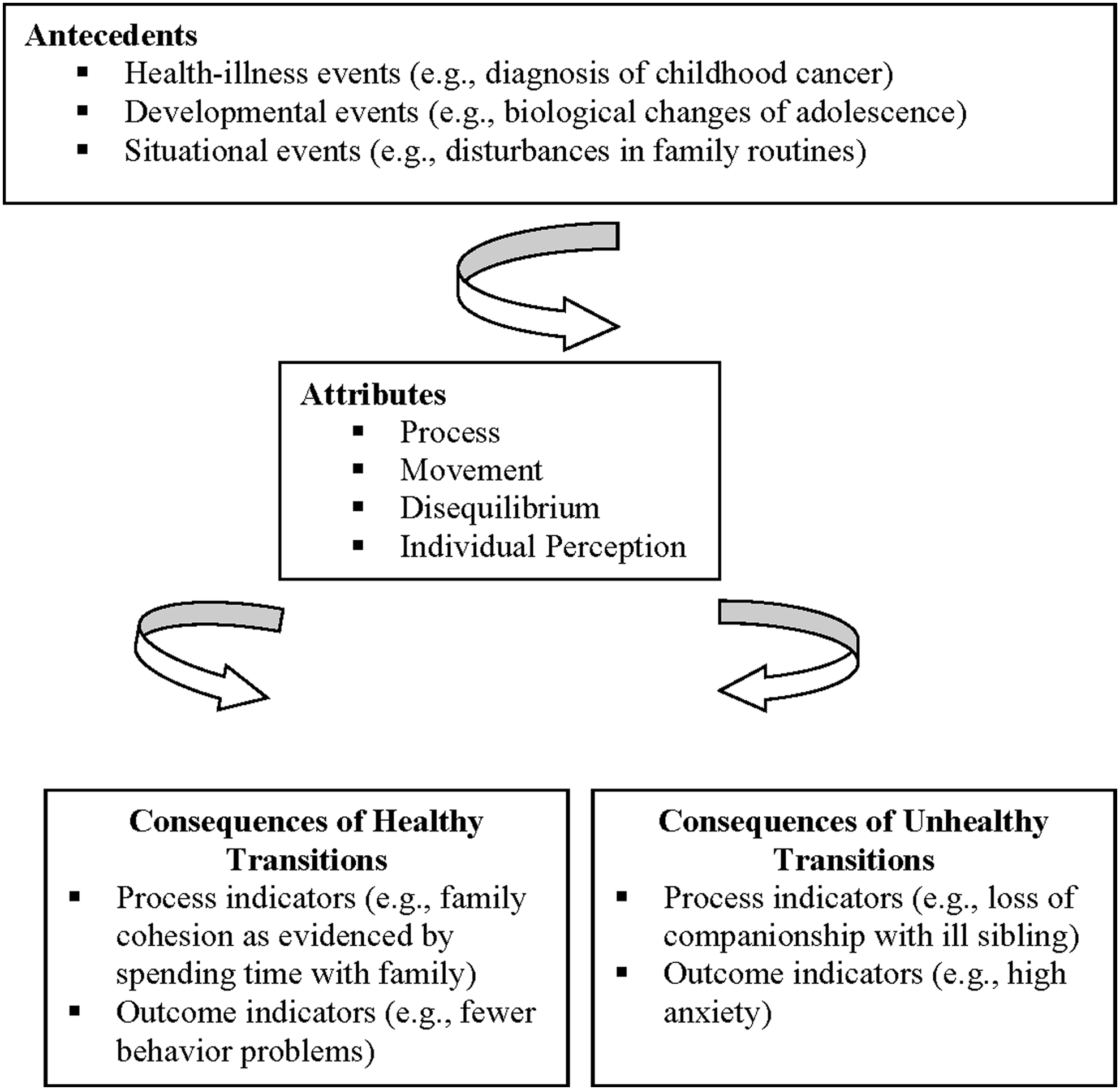
Illustration of conceptual framework for siblings of children with cancer. From Wilkins KL, Woodgate RL. Transition: a conceptual analysis in the context of siblings of children with cancer. J Pediatr Nurs. 2006;21(4):256–65. Reprinted with permission from Elsevier, Inc.
For the purposes of the current study, the key attributes of transition presented in the Wilkins and Woodgate 7 framework were retained and applied to the current study as specified below. The health-illness antecedent event initiating the transition to early survivorship was the completion of treatment. We conceptualized that adolescent cancer survivors would simultaneously undergo transitions triggered by developmental antecedent events.
The purpose of this study was to conduct an exploratory, retrospective qualitative investigation to gain an in-depth understanding of adolescent cancer survivors' individual perceptions and the meanings they assigned to the transition to early survivorship. Another goal of the study was to learn about the state of disequilibrium, or feelings that make an individual feel unbalanced or outside of their “comfort zone,” changes made or experienced by the adolescent in response to the state of disequilibrium, and what support and/or services promoted a healthy transition process. Our specific research questions were:
1. How do adolescent survivors of childhood cancer perceive the transition to early survivorship? 2. What are the challenges faced by adolescent survivors of childhood cancer during the transition to early survivorship? 3. What are the beliefs of adolescent survivors of childhood cancer about the support and/or services that were or would be beneficial during the transition to early survivorship?
Methods
Procedure and participants
Three experts from separate academic or medical institutions knowledgeable in pediatric oncology, qualitative methodology, and cancer survivorship reviewed screening and demographic questionnaires and the interview guide. A pilot study was conducted with three adolescent cancer survivors to assess the utility of the semi-structured interview guide and the interview process. Based on the results of the pilot study, revisions were made to the interview guide, including re-ordering and adding questions. The results of the pilot study were used for refining methodology and not for data analysis.
Participants were recruited using purposeful and criterion sampling from a pediatric oncology outpatient clinic at an urban hospital in the Mid-Atlantic region United States. Due to the limited number of participants enrolled at this site, additional participants were recruited at a non-profit cancer organization in the Midwest United States that provides free support, education, and programming for individuals and families impacted by cancer.
Inclusion criteria included: 12–17 years old at the time of the study, diagnosis of cancer other than brain tumor received during childhood at age ≥5 years old, off treatment for a minimum of 6 months and a maximum of 5 years, cancer in remission, no history of relapse, currently attending school in the community, and English as a first language. Individuals diagnosed with a brain tumor were excluded given the sequelae associated with their cancer and treatment. Adolescents diagnosed prior to 5 years of age were excluded due to concerns these individuals would be unable to accurately recall and reflect on their experiences. 2
Recruitment methods included phone contact and flyer distribution. Flyers asked respondents to contact the principal investigator (ADL) directly if they were interested in study participation. The PI called each potential participant and administered the screening questionnaire to verify inclusion criteria. All participants were informed that the study consisted of a face-to-face, semi-structured individual interview and follow-up meeting by phone or in-person. Interviews were scheduled based on participants' day, time, and location preferences. Written consent and assent were obtained prior to the interview. Participating institutional review boards approved this study. Figures 2 and 3 provide detailed information on recruitment and attrition at the pediatric oncology outpatient clinic and non-profit cancer organization, respectively.

Recruitment and attrition at pediatric oncology outpatient clinic.
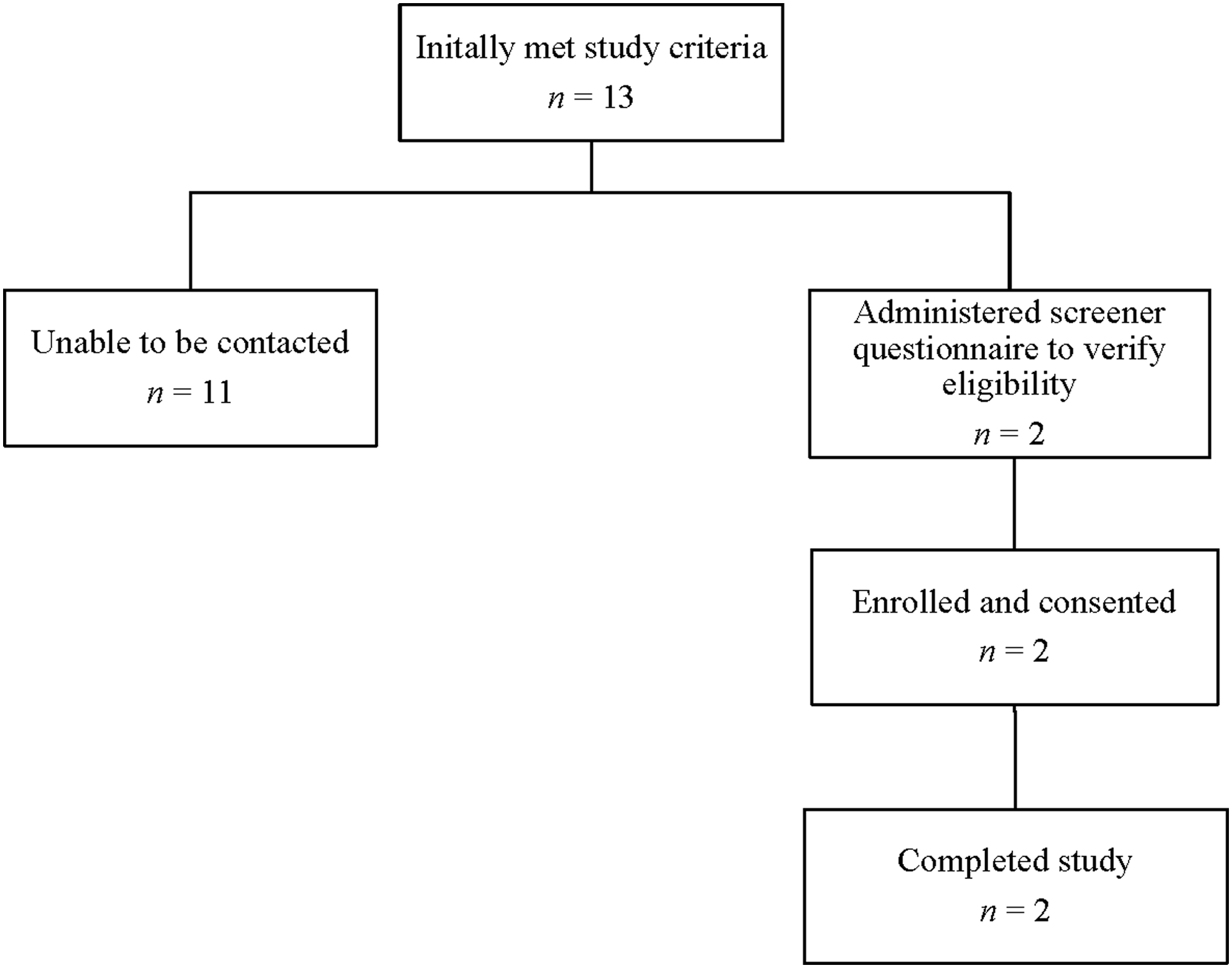
Recruitment and attrition at non-profit cancer organization.
Measures
Demographic questionnaire
Participants completed a demographic questionnaire after the interview. It elicited commonly reported information, including gender, ethnicity, education level, diagnosis, and type(s) of treatment received.
Interview guide
A semi-structured, open-ended interview guide was used to conduct the initial interviews. The guide included the following components: research questions, leadoff questions, and probes. Questions were based on the conceptual framework, three research questions, and purpose of the study (Table 1). Interviews ranged from 38–96 minutes.
Follow-up meeting
Participants completed individual follow-up meetings by phone or in-person approximately 1 month after their interview. Participants were mailed or emailed a summary of their interview in advance. Member checking, or respondent verification, was conducted, and participants were asked if the interview summaries accurately represented their experiences. Participants were asked additional questions and given the opportunity to provide comments and clarify their interview summaries. Follow-up meetings aranged from 10–38 minutes.
Data analysis
This study utilized an exploratory qualitative methodology using a multiple case study research design. Data from the questionnaires, transcribed interviews, and follow-up meetings were analyzed using a template organizing style (codebook development), immersion/crystallization (I/C) approach, and cross-case analysis strategies.9–11 The PI conducted all interviews and follow-up meetings for consistency purposes. Data were prepared for analysis, transcribed verbatim by an independent party, and reviewed by the PI to ensure accuracy. Two members of the research team (ADL and LJR) independently read two randomly selected interview transcripts, assigned codes that best captured the meaning of text segments, and developed a preliminary code list and codebook.10,12 Another randomly selected transcript was jointly coded to ensure mutual understanding of the codes. Operational definitions were created for each code, and the five remaining transcripts were independently coded using the codebook. Inter-rater reliability was calculated for the remaining interview transcripts and ranged from 80% to 90%. 12 A case report worksheet was completed for each participant to summarize information and to examine whether data converged and triangulation occurred. The I/C process was then used to review the individual case study reports, identify and “crystallize” themes, and establish relationships among themes relative to the conceptual framework and research questions. Finally, a cross-case analysis was conducted to explore commonalities and differences among participants and to formulate overarching findings about the transition to early survivorship. 11 Descriptive statistics were obtained.
Results
Demographic characteristics are reported in Table 2. The sample consisted of five male and three female adolescent survivors of childhood cancer with an average age of 16 years old (standard deviation [SD]=1.13; range: 14–17). All participants were from Caucasian, non-Hispanic backgrounds. Five were diagnosed with leukemia and the remaining participants were diagnosed with lymphoma, with an overall mean age at diagnosis of nearly 13 years old (SD=1.81; range: 9–15). Their mean age at treatment completion was 14 years old (SD=1.69; range: 12–16), and half of the adolescents were between 2.5 and 3 years post-treatment completion. At the time of the study, all of the participants attended high school and were in grades 9–12. The participants had varied educational experiences during treatment and early survivorship. These placements were primarily dictated by a combination of factors, including type of cancer diagnosis, treatment regimen, treatment side effects, medical team recommendations, and family preferences.
Combination of community, hospital, homebound, and internet.
The themes related to each research question fell into three categories: perceptions of early survivorship, perceived challenges associated with early survivorship, and beneficial support/services during early survivorship. A total of eight themes were identified (Table 3). The following terms are used to communicate how many adolescents endorsed a particular theme: “few” (1–2), “some” (3–4), “many” (5–6), and “majority” (7–8).
Category 1: Perceptions of early survivorship
It's not a transition, let's get back to normal
The majority of adolescents indicated the word “transition” was not applicable as it represented a more significant change then what actually happened in their lives. A few participants suggested that a “transition” would be more akin to transferring from middle school to high school. Adolescents described this shift to early survivorship in a variety of ways, including: “closing a chapter and moving on,” “moving on to the next stage,” “stepping back into the story or page of a book,” and “continuation of the journey.” The majority of adolescents focused on the concrete goals of finishing treatment, moving on with life, and returning to normalcy.
My approach to life after treatment
The majority of adolescents in the study did not engage in a tremendous amount of forethought or planning about what life would be like after they completed treatment. They handled things as they came and did not necessarily think about their approach to returning to normalcy. The majority of adolescents tended to focus on more tangible events, such as treatment completion, before shifting their focus to the future and life after treatment.
Signs that I'm making my way back to normal
The improvement or absence of treatment residuals and re-engagement in activities and roles served as signs, or indicators, that life was getting back to normal for the majority of adolescents. Adolescents reported improvements in and/or absence of treatment residuals, such as decreased frequency and length of follow-up appointments, lessening or disappearance of treatment side effects, and central line removal. They also described activity-based signs that life was getting back to normal, such as attending school on a more regular basis, re-establishing social relationships and roles, returning to previous academic performance, and participating in extracurricular activities. There were individual differences in the types of signs reported, which were influenced by adolescents' personal interests, motivations, and cancer history/treatment.
Feeling more comfortable with time
All of the adolescents reported feeling more physically and emotionally comfortable as time since treatment completion increased, which facilitated meaningful movement through the early survivorship phase. They described feeling increasingly comfortable over time as they were able to re-engage in familiar activities, observe improvements in their physical appearance, develop insight about their physical status, and realize that follow-up appointments were becoming less frequent and stressful. This growing awareness developed at different points for these adolescents.
Category 2: Perceived challenges associated with early survivorship
Signs that life is not back to normal just yet
Although ending treatment signified an important accomplishment, the majority of adolescents were challenged to juggle a complex combination of physical limitations and continued disruption in their daily lives. They expressed awareness that their journey was not over, as many reported coping with residual effects of treatment, such as compromised immune function; decreased energy, endurance, and stamina; presence of central line; follow-up medical appointments/procedures; and continued treatment side effects. The majority of adolescents experienced some type of activity restriction. Although these restrictions were not permanent for these adolescents, their presence required them to adapt and seek out alternative or modified activities.
It is not the focus of life, but the idea of relapse is there
Adolescents expressed a variety of concerns related to relapse, such as receiving unfavorable scan/test results, fearing that symptoms post-treatment may be a sign of relapse, and having to repeat treatment. Some adolescents adopted coping strategies, including avoiding excessive thoughts of relapse, citing positive information from their medical team or examples of peers who have survived, and avoiding cancer-related information that might induce anxiety. Thoughts and concerns associated with potential relapse tended to be greater at the time of treatment completion and lessened over time.
Category 3: Beneficial support and services during early survivorship
My need for support and/or services
Adolescents varied in their perceived need for support during the early survivorship period. Some adolescents welcomed the support they received and thought it was helpful and adequate, whereas others did not perceive a great need for support and preferred to proceed independently. A few adolescents mentioned they were not interested in hearing information about potential late effects, as it would have created unnecessary anxiety or suggested survivorship was a “big deal.” None of the adolescents voiced concerns they did not receive adequate information or support from their healthcare team.
What my healthcare team told me
The majority of adolescents indicated information related to early survivorship was conveyed to them verbally and, in one case, with printed materials. Some of this information was perceived as useful, while others deemed it unnecessary or unwanted. Physicians, nurses, and child life specialists were identified as those who provided information. Discussions pertained to a variety of topics, including physical capabilities/limitations to be aware of post-treatment, engaging in healthy lifestyle behaviors, sleeping well, minimizing risk of infection, pacing oneself during activities, follow-up schedule details, odds of relapse, and to have fun and enjoy life.
Discussion
The findings of the current study suggest that adolescent cancer survivors perceived change was occurring after treatment completion, but did not necessarily define it as a “transition.” Research has found that some childhood cancer survivors strive to return to their lives prior to their cancer diagnosis, while others believe cancer has significantly altered their life to the point that they must establish a “new normal.”13,14 The majority of adolescents in this study described a subtler change, with a focus on returning to their life prior to cancer. They employed strategies during early survivorship such as “in the moment thinking,” facing challenges as they arose, and not looking too far ahead into the future, which likely represents a combination of typical adolescent development within the context of the cancer experience. These strategies also may have been used as a means to protect oneself against worry and distress. These findings speak to the importance of assessing the impact of developmental level and maturation on transition perceptions, approaches, and transition planning. This population presents unique challenges for medical providers given the importance of assessing adolescent/family readiness to receive survivorship information while providing necessary and, at times difficult, information relevant to the adolescent perspective. To assist with this process, it may be beneficial to have adolescents develop short-term early survivorship goals that align with returning to normalcy while parents can be supported in developing short- and long-term goals. Adolescents may be asked to define what terms such as “transition” and “normality” mean to them, with an understanding that their answers may change across the lifespan. Medical providers can present survivorship information and materials in a way that is related to adolescents' goals. Survivorship information can be distributed over time with periodic review to reinforce information as the adolescent continues to mature.
The presence, improvement, and absence of treatment residuals and re-engagement in activities and roles provided adolescents feedback on their progression through early survivorship. For the majority of the adolescents, treatment residuals affirmed the notion that treatment completion does not necessarily equate to a life free of cancer. Research suggests that adolescent cancer survivors are aware of the presence of long-term treatment side effects and recognize the negative impact they have on their life post-treatment. 15 It also has been shown that the post-treatment journey is highly variable among cancer survivors, and treatment effects differ in type, severity, and duration. 16 As such, treatment residuals can manifest themselves in various ways over the course of a survivor's lifespan, which may reflect individual differences in transition experiences. This provides support for taking a systematic, individualized approach to transition planning that considers a patient's characteristics, diagnosis/treatment history, and associated sequelae.
Adolescents in the current study varied in their perceived need for support and/or services related to the transition to early survivorship. Some adolescents were receptive to advice while others did not want any information as it created unnecessary anxiety and suggested that the transition represented a significant change. The majority of adolescents were content with the information, or lack thereof, they received. Further, none of the adolescents independently sought out information related to the transition. Consistent with findings in the extant literature, these particular adolescents may have wanted to preserve a neutral or positive state of mind as they transitioned to early survivorship. 17 Adolescents did not report receiving any formal type of support, such as a transition conference or a survivorship care plan. The lack of formal supports or services to facilitate these adolescents' transition to early survivorship is consistent with research suggesting limited transitional care planning interventions. 5 The most salient type of support identified by the majority of adolescents was social support from same-age peers and other cancer survivors across school, community, hospital, and camp settings. This finding likely reflects adolescents' desire to seek out peer relationships, particularly with those who are similar or can relate to their experiences, suggesting that opportunities for social interaction may be useful during early survivorship. Further, adolescents in the current investigation also varied in the types of support they were interested in receiving after treatment completion. This particular finding speaks to the importance of recognizing individual differences in support preferences, which again suggests the need for individualization of transition planning rather than a “one size fits all” approach. A more formal plan or set of guidelines may be more useful to professionals and caregivers with a more indirect impact on patients.
In practice, a tiered public health approach, such as the Pediatric Psychology Preventative Health Model, 18 may hold great promise in the delivery of transition services given the emphasis on targeted intervention based on need, level of distress, and individual risk factors. Given the importance of individual differences, it is likely that adolescent cancer patients and survivors will vary in their need for transition support and intervention to successfully navigate the transition to early survivorship. Further, this model can be used to develop a tiered system of transition service delivery based on need and risk level to maximize positive transition outcomes in a cost-effective manner.
Regarding the conceptual framework, the completion of treatment represented a health-illness antecedent event. Although this event unfolded at different times under various conditions for each adolescent, it was generally perceived as a phase of their life that was completed. Some adolescents experienced specific situational events, such as starting high school or middle school, in tandem with treatment completion. The presence of multiple antecedents added an additional layer of complexity, further defining the transition process. Although adolescents in the current study did not identify early survivorship as a transition, their experience included many key attributes of a transition. For example, adolescents' perceived movement as they returned to a sense of normalcy and experienced a state of disequilibrium characterized by feelings of uncertainty about the future, fear of relapse, and continued presence of treatment residuals or disruption in activities and/or roles. The degree of disequilibrium experienced by the adolescents was variable, and appeared to be related to factors such as type of diagnosis, intensity of treatment regime, and severity/persistence of treatment residuals. Their individual perceptions of the transition to early survivorship were a hallmark of this study. Each adolescent shared his or her perspective, assigned meaning to the cancer experience, and was able to reflect on the impact (or lack thereof) that cancer had on his or her life. They focused on returning to a sense of normalcy and recognized concrete signs that provided feedback about their progress or lack thereof in returning to normalcy.
The study's findings extend previous research, although there are limitations. The findings may not be representative of the experiences of adolescent cancer survivors from different geographic locations and cultural backgrounds, nor of those with different cancer diagnoses, such as brain or solid tumors. Recall bias is important to consider, as adolescents were asked to answer questions regarding their past experiences with varying lengths of time since treatment completion. There was a lack of cultural, ethnic, and socioeconomic diversity in the current sample. Selection bias must also be considered because patients who agreed to participate in research may have had significantly different experiences than those who declined participation. Further, there may be differences in participant characteristics based on recruiting from a non-profit community organization providing supportive care versus an urban hospital where patients receive follow-up medical care. Lastly, social desirability is a potential limitation, as adolescents may have described their experiences in a socially desirable manner or withheld information to create a positive image during the interviews and follow-up meetings. 19
Conclusion
The findings of the current study revealed that adolescent cancer survivors have unique perspectives of the early survivorship period, specific challenges during this time, and varying needs for transition support. Results lend support to distinguishing adolescents as a distinct subgroup of cancer survivors. Practical implications were discussed that may promote positive transition experiences for adolescent cancer patients and survivors.
Footnotes
Acknowledgments
The authors would like to thank Katherine Griffin, RN and Kathy Maxwell, LISW-S for their assistance. We are also grateful to the participants for sharing their experiences.
Author Disclosure Statement
No competing financial interests exist.