
Abstract
Relapse of acute lymphoblastic leukemia (ALL) in the breast is uncommon and often precedes systemic relapse, resulting in poor survival. We report the development of breast involvement of ALL in a 20-year-old woman 32 months after a related allogeneic peripheral blood hematopoietic cell transplantation (PBHCT) in first remission. This extramedullary relapse occurred in the continuous presence of complete donor chimerism. After systemic re-induction chemotherapy and a second PBHCT using donor cells that had been cryopreserved at first transplant, our patient has remained in second complete remission for more than 44 months.
T
Case
An 18-year-old woman presented with abdominal pain and fatigue during her second trimester of pregnancy. She was found to have an abnormal complete blood count with 23% blasts. A bone marrow aspirate and biopsy revealed 73% lymphoblasts that expressed CD10, CD19, CD20, CD34, CD38, CD45, terminal deoxynucleotidyl transferase (TdT) and human leukocyte antigen class II (HLA-DR), consistent with precursor B-cell ALL. Fluorescence in situ hybridization and polymerase chain reaction analyses were negative for BCR-ABL and MLL gene rearrangements, but marrow cytogenetics showed multiple abnormalities, including an addition to chromosomes 1q24 and 21q22 and deletion of chromosomes 7p13-p15, 10q24, and 13q12-q14.
As she had been admitted to the internal medicine service, medical oncology was consulted. She began treatment under the care of medical oncology in accordance with the CALGB 8811 regimen. 6 She gave birth to a healthy daughter at 27 weeks gestation on day 10 of induction and 57 days prior to PBHCT. She received an additional cycle of chemotherapy with intrathecal methotrexate, systemic cyclophosphamide, mercaptopurine, cytarabine, vincristine, and asparaginase. She then underwent an allogeneic PBHCT from her HLA-identical brother after a myeloablative preparative regimen of cyclophosphamide and total body irradiation (TBI). She received a CD34 dose of 5.0×106/kg with a CD3 dose of 1.44×108/kg for her first transplant. Of note, no part of her treatment was delayed due to her pregnancy or delivery. She received cyclosporine and short-course methotrexate for prophylaxis of graft-versus-host disease (GVHD). Her post-transplant course was notable for its prolonged red cell transfusion dependency due to donor-recipient ABO incompatibility (the donor was A positive, the recipient was O positive); she did not have clinical or laboratory evidence of acute or chronic GVHD.
Thirty-two months after PBHCT, at age 20, she presented to her primary care physician with right breast and axillary pain. She was then referred back to medical oncology, which sent her to have a left axilla lymph node biopsy. Flow cytometry of her lymph node revealed extramedullary relapse of ALL, with lymphoblasts expressing the same immunophenotype as in her initial bone marrow at diagnosis. Her bone marrow and cerebrospinal fluid showed no evidence of recurrent ALL, and marrow chimerism studies continued to show 100% donor DNA. A positron emission tomography-computed tomography (PET/CT) scan indicated areas of abnormal fluorodeoxyglucose uptake in bilateral breast tissue, axillary nodes, and supraclavicular nodes.
Her care was then transferred to the pediatric oncology team due to a limited availability of resources in the medical oncology program at that time, including the lack of an active bone marrow transplant program. There she received systemic re-induction therapy with prednisone, doxorubicin, vincristine, and pegylated asparaginase, and also received intrathecal methotrexate. This was followed by one cycle of etoposide and cyclophosphamide and one cycle of high-dose methotrexate, in accordance with the COG AALL01P2 protocol. 7 A follow-up PET/CT scan showed no evidence of abnormal metabolic activity compared to her initial scans (Figs. 1 and 2). She then underwent a second allogeneic PBHCT after a myeloablative preparative regimen of intravenous busulfan and cyclophosphamide, receiving donor peripheral blood stem cells that had been cryopreserved after collection for her initial PBHCT. She received 6.06×106 CD34/kg with 1.75×108 CD3/kg for her second transplant. She once again received methotrexate and cyclosporine for GVHD prophylaxis. Cyclosporine was weaned off by four months post-transplant.
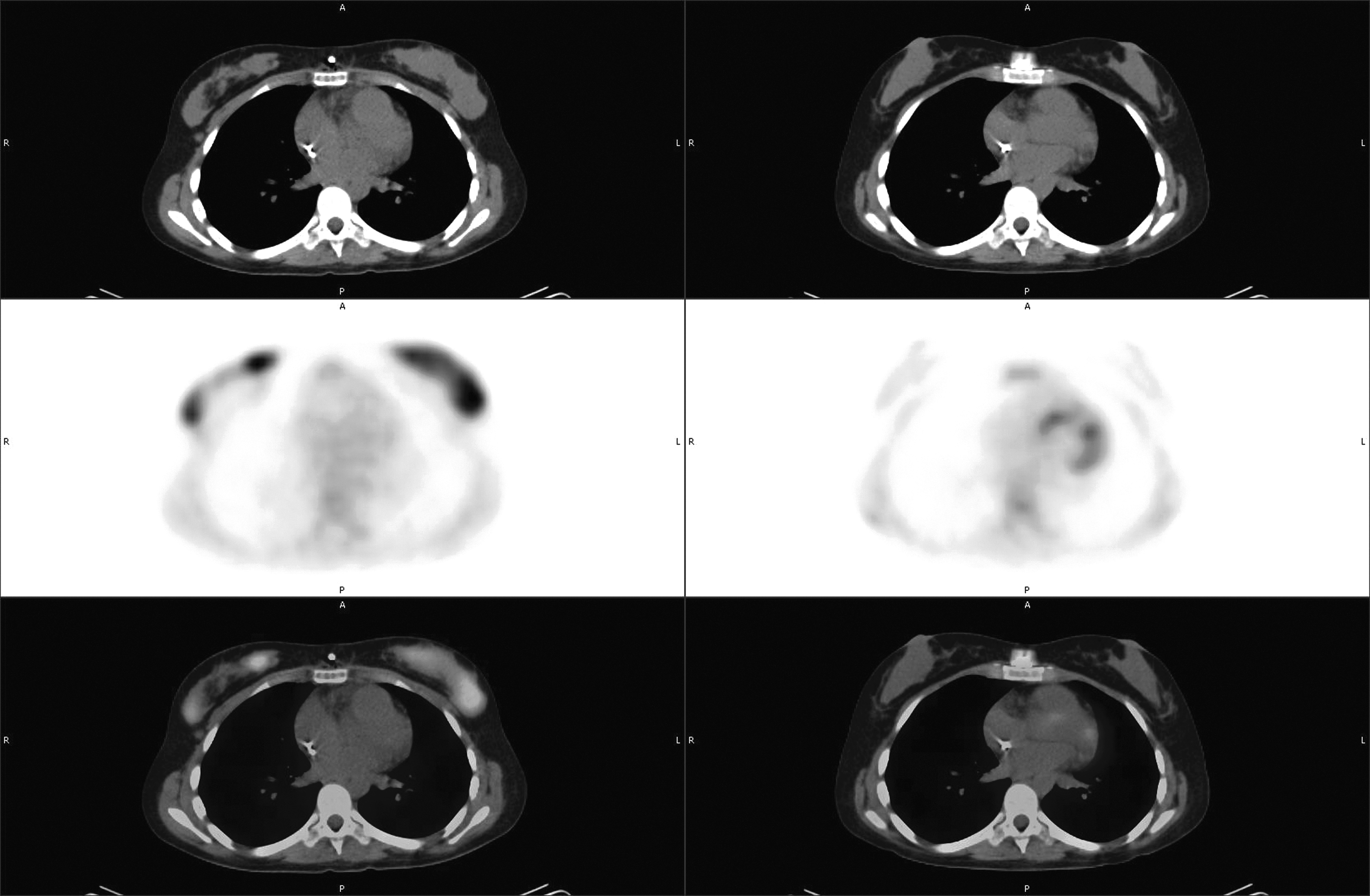
Pre- and post-axial PET/CT. PET/CT, positron emission tomography-computed tomography.
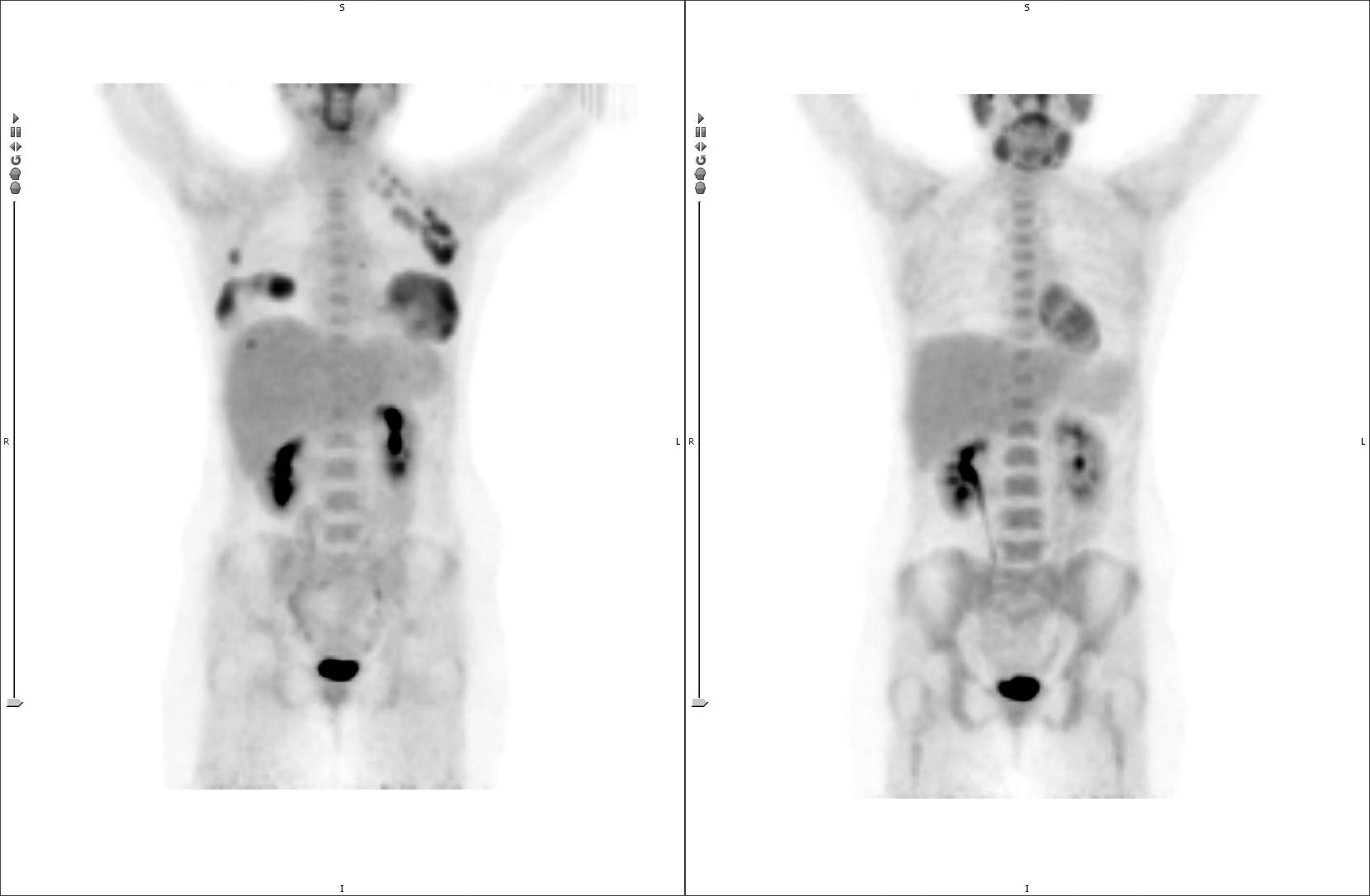
Pre- and post-whole body PET/CT. PET/CT, positron emission tomography-computed tomography.
Six months after her second PBHCT, she developed extensive chronic GVHD with ocular, oral, gastrointestinal, musculoskeletal, and vaginal involvement. Treatment of her chronic GVHD consisted of cyclosporine A, prednisone, and mycophenolate mofetil. More than 44 months after the second PBHCT, the patient has quiescent chronic GVHD, ongoing complete donor chimerism, and no evidence of recurrent ALL. She is raising her healthy 7-year-old daughter, working, and attending college. She continues to be followed by the pediatric oncology team for long-term follow-up care.
Discussion
Our patient has many unique aspects to her case: (1) she was pregnant during her initial diagnosis and treatment of ALL; (2) she had a late breast relapse—almost three years from her first PBHCT; and (3) she developed significant chronic GVHD after her second PBHCT with the same donor cells, despite having 100% donor cell reconstitution prior to her second transplant.
Relapse of pediatric ALL is approximately 20% overall, with about one-third of those relapses occurring in extramedullary locations.8,9 However, most pediatric ALL patients are treated only with initial chemotherapy, not with hematopoietic cell transplantation (HCT).8,9
The breast is a rare extramedullary relapse site in pediatric ALL, limited to a few published case reports, with the majority of breast relapses occurring after HCT.10–13 Most cases were reported in adolescent girls, while the majority of adult ALL cases are in women less than 30 years of age.4,14,15 The largest review of breast involvement in acute leukemia to date was in 2006 by Cunningham, who reported 153 total cases, including 46 in patients with ALL ranging in age from 1 to 60 years old, 90% of which occurred in women less than 50 years old, and 74% occurred in women less than 30 years old. 4 Of the cases with breast leukemia relapse following HCT, 86% were women 10–29 years old. Fourteen women relapsed post-HCT and generally had very poor outcomes. They had received a variety of treatments, including radiation, chemotherapy, donor lymphocyte infusion, and a second HCT. Unlike our patient, who was in remission for 32 months after HSCT, these patients had very short post-transplant remissions—all less than 24 months. 4 Another review by Surov et al. reported 133 women and girls with acute leukemia, of which 35 had ALL. The age range of these women was 1–80 years old, with a median age of 33. The majority of cases of breast involvement occurred after HCT. 15 As in the Cunningham review, patients with breast involvement did poorly with a survival of 28%; however, the authors did not distinguish between the different types of acute leukemia (ALL versus acute myelogenous leukemia), making it difficult to draw any meaningful conclusions of outcome specifically with ALL of the breasts. 15
Interestingly, in women with breast leukemia, if pregnancy is associated with their initial diagnosis of ALL, there is an increased incidence of secondary breast leukemia found, as was the case in our patient.4,14 Pregnancy during treatment of acute leukemia can be difficult due to a multitude of potential complications, including disseminated intravascular coagulation and pancytopenia, which then complicate treatment of the mother and safety of the fetus, as anemia decreases oxygen and nutrient exchange to the fetus during pregnancy. 16 There are also questions regarding the safety of chemotherapy administration and its effects on the growing fetus, as most chemotherapy agents cross the placenta. The greatest risk of side effects appears to be in the first trimester.16,17 Our patient was entering her third trimester at the time of diagnosis and gave birth shortly after induction began, so she did not require any modifications to her treatment.
While secondary breast leukemia may be more common in patients initially pregnant at the time of diagnosis, the breast has not historically been considered a sanctuary site. Sanctuary sites have been identified as common areas of EM relapse because they are protected from initial systemic chemotherapy due to an anatomic or physiologic barrier. 18 One thought is that the breasts may not have a specific barrier protecting them from chemotherapy, but instead may be a more favorable tissue for acute leukemia recurrence.4,19 However, although more cases of breast leukemia have been reported in recent years, the predilection of acute leukemia for breast tissue is still unknown. As our patient received TBI as conditioning prior to her first PBHCT, her breasts did receive treatment, and thus should have been a less likely area of relapse. Lee et al. focused on the protective effects of GVHD on sites of leukemia relapse in both lymphoblastic and non-lymphoblastic leukemia and concluded that GVHD did have a protective effect on bone marrow relapse, but had less of one on EM relapse, and extrapolated this to mean that there was less graft-versus-leukemia (GVL) effect in these EM sites, including the breasts. 20 Our patient did not show evidence of acute or chronic GVHD after her first transplant, which should not have favored an EM relapse.
GVHD has been reported after second transplants with the same donor even if it was absent after the first transplant. 21 What is notable about our case is that our patient remained fully engrafted (complete donor chimerism) with her brother's donor cells before her second transplant and received a cryopreserved aliquot of the same cells that were collected before her first transplant. Although allogeneic sibling transplants are typically done with fresh rather than cryopreserved cells, our patient was fortunate to have additional cryopreserved cells, as her brother was not available for a second donation. Our patient received GVHD prophylaxis, as it is standard of care for allogeneic SCT, though because our patient received the same cryopreserved cells in her second PBHCT when she was fully engrafted with her brother' cells, one could argue that GVHD prophylaxis was not necessary. Even though she essentially received an autologous SCT, she developed GVHD in her second transplant, which is unusual. It is plausible that the longer remission after her second PBHCT was due in part to a GVL effect associated with her chronic GVHD.
Conclusion
Our case illustrates many complications unique to the population of adolescents and young adults with cancer. As our patient was a young adult, either pediatric or adult protocols may be utilized for care. Another challenge unique to young adults was our patient's pregnancy during her initial ALL diagnosis and treatment. Lastly, she developed an EM relapse in breast tissue, a complication rarely seen in the pediatric population. Despite the complexities of her initial diagnosis and recurrence, she remains in remission. Her case contributes to the knowledge base of adolescent women with EM relapse of ALL in breast tissue and reaffirms the importance of aggressive treatment to improve outcome, as women with breast leukemia have a poor prognosis, especially if treated conservatively.
Footnotes
Author Disclosure Statement
No competing financial interests exist.