
Abstract
Purpose:
Cancer-related fatigue in adults has been the subject of considerable recent research, confirming its importance as a common and debilitating symptom, and establishing a number of evidence-based interventions. There has, however, been limited focus on the fatigue suffered by teenagers and young adults with cancer, a group recognized as having unique experiences and developmental needs. We have undertaken a systematic review of the literature to provide a comprehensive overview of studies evaluating fatigue in this younger patient group in order to guide clinical practice and future research.
Method:
We searched MEDLINE, EMBASE, PsycINFO, and CINAHL databases for literature containing data relating to any aspect of fatigue in patients aged 13–24 at cancer diagnosis or treatment.
Results:
Sixty articles were identified, of which five described interventional clinical trials. Cancer-related fatigue was consistently one of the most prevalent, severe, and distressing symptoms, and it persisted long-term in survivors. It was associated with a number of factors, including poor sleep, depression, and chemotherapy. There was little evidence for the effectiveness of any intervention, although exercise appears to be the most promising. Importantly, fatigue was itself a significant barrier to physical and social activities.
Conclusion:
Cancer-related fatigue is a major and disabling problem in young cancer patients. Effective management strategies are needed to avoid compounding the dependence and social isolation of this vulnerable patient group. Future research should focus on providing evidence for the effectiveness of interventions, of which activity promotion and management of concurrent symptoms are the most promising.
C
Cancer-related fatigue is a “persistent, subjective sense of tiredness related to cancer or cancer treatment that interferes with usual functioning.” 8 It is a multidimensional symptom with physical, affective, and cognitive components. The range of perceptions may include a feeling of weakness and inability to perform tasks, decreased motivation and low mood, and difficulty in thinking clearly. 9 It differs from fatigue felt by healthy individuals in that it is of greater magnitude, disproportionate to the level of exertion, and incompletely relieved by rest.
Fatigue appears to be both the most common and the most distressing symptom experienced by adult patients with cancer.10,11 Many surveys suggest a prevalence of over 75%, with rates increasing in conjunction with oncological treatment.12,13 Adult patients report that fatigue is the symptom which has the greatest negative impact on their quality of life. 11
Despite the size of the problem, cancer-related fatigue has traditionally been neglected both in clinical and research terms, with healthcare staff and patients tending to consider it an unavoidable consequence of cancer and its treatment.10,14 However, over the last two decades, a substantial evidence base has been developing in the adult literature. Systematic reviews of research in older adults has shown that—apart from treating reversible underlying causes—the most promising approaches are exercise 15 and psychosocial interventions such as education. 16
Recognition of the particular importance of cancer-related fatigue in younger cancer patients has only emerged over the last 5–10 years. Lack of energy has been shown to be the most common symptom in children with cancer, with children placing emphasis on a sense of physical weakness, associating fatigue with disruption of sleep. 17 TYA cancer patients also appear to suffer from significant fatigue,18–20 unsurprising given that even healthy teenagers and young adults have a propensity to experience fatigue. The developmental need for longer sleep during this important phase of brain maturation is hindered by circadian rhythm shifts and a tendency to develop unhelpful sleep habits.21,22 TYAs perceive fatigue in both cognitive and physical terms. 5 Fatigue is believed to have a particularly negative impact on quality of life in this group, as it hinders many of the key developmental needs of this age, such as autonomy and the formation of close peer relationships. 23 Many TYA cancer patients remain or return to being dependent on their parents at a time when they would have been expecting to achieve independence. It is well recognized clinically that the parents of fatigued TYAs bear a considerable burden.
In one previous review of fatigue in teenagers in cancer published a decade ago,
20
Erikson found there was minimal research focusing on fatigue in this age range. Given the number of articles published since that review, it was decided to systematically appraise the current evidence base with a focus on the TYA age group. The review was designed to be broad to provide a comprehensive overview of studies investigating any aspect of cancer-related fatigue in patients diagnosed or treated for cancer while aged 13–24 years old. The research questions were:
1. What is the prevalence and severity of cancer-related fatigue in TYA patients during and after treatment? 2. What is the impact of fatigue on TYA cancer patients? 3. What is the experience of parents of fatigued TYA cancer patients? 4. What are the correlates of cancer-related fatigue in this patient group? 5. How effective are interventions to manage fatigue in TYA patients?
Methods
Literature search strategy
The literature was searched within MEDLINE, EMBASE, PsycINFO, and CINAHL databases for January 1981 through October 2013. Preliminary searches had suggested that there was no literature of relevance published prior to 1981. The search strategy is detailed in Table 1. Reference and citation searches were also undertaken, with manual searching of all issues of a key journal—the Journal of Adolescent and Young Adult Oncology (issues 1–4 of both volume 1 and volume 2)—as well as the proceedings of the 2012 Teenage Cancer Trust International Conference. Related systematic reviews were searched, including reviews evaluating symptoms experienced by teenagers with cancer, 24 fatigue in lymphoma patients, 25 and interventions for fatigue in children and adults.26,27 Experts in teenage and young adult cancer-related fatigue were also contacted.
Both “adolescent” and “young adult” limiting terms were available in the MEDLINE and CINAHL database searches, but only “adolescent” was available for the EMBASE and PsycINFO searches.
Selection criteria
The key inclusion criteria were that all study participants had malignant disease, and that either the majority were aged 13–24 years old at the time of cancer diagnosis or treatment or the results for this age subgroup were presented separately. Included studies could investigate any aspect of cancer-related fatigue, use any outcome measure, and employ quantitative or qualitative methods. Exclusion criteria included non-English language publication, absence of original empirical data, phase I/II clinical trials, trials involving fewer than 10 patients, case reports, and retrospective case note reviews. Studies of TYA-aged survivors of pediatric cancer were not included.
Quality assessment and data analysis
Gough's Weight of Evidence Framework
28
was employed to assess article quality, relevance, and bias, and to generate an overall judgment about contribution. This framework includes analysis of “fitness for purpose” and relevance to the research question, providing a more applied synthesis of evidence than simply assessing the generic quality of each article. Four scores of “low,” “medium,” or “high” are given for each of the following:
• Weight of Evidence A: The integrity of the evidence in its own terms • Weight of Evidence B: The appropriateness of method for answering the review questions • Weight of Evidence C: The appropriateness of the focus or relevance for answering the review questions • Weight of Evidence D: The overall rating generated by combining the Weight of Evidence A, B, and C scores
All articles, irrespective of relevance and quality, were included, but those rated “medium” and “high” were given greater weight in the analysis.
The searches produced 2388 unique titles that were initially screened by one researcher (AS). After 566 abstracts were reviewed by two researchers (AS and SG), 343 full articles were read by one researcher (AS), who excluded most of them on the basis of the participants' ages. Two researchers (AS and SB) read the remaining articles, with disagreements resolved by discussion. The final number of included articles was 60 (Fig. 1). A narrative synthesis was undertaken in relation to each of the research questions.
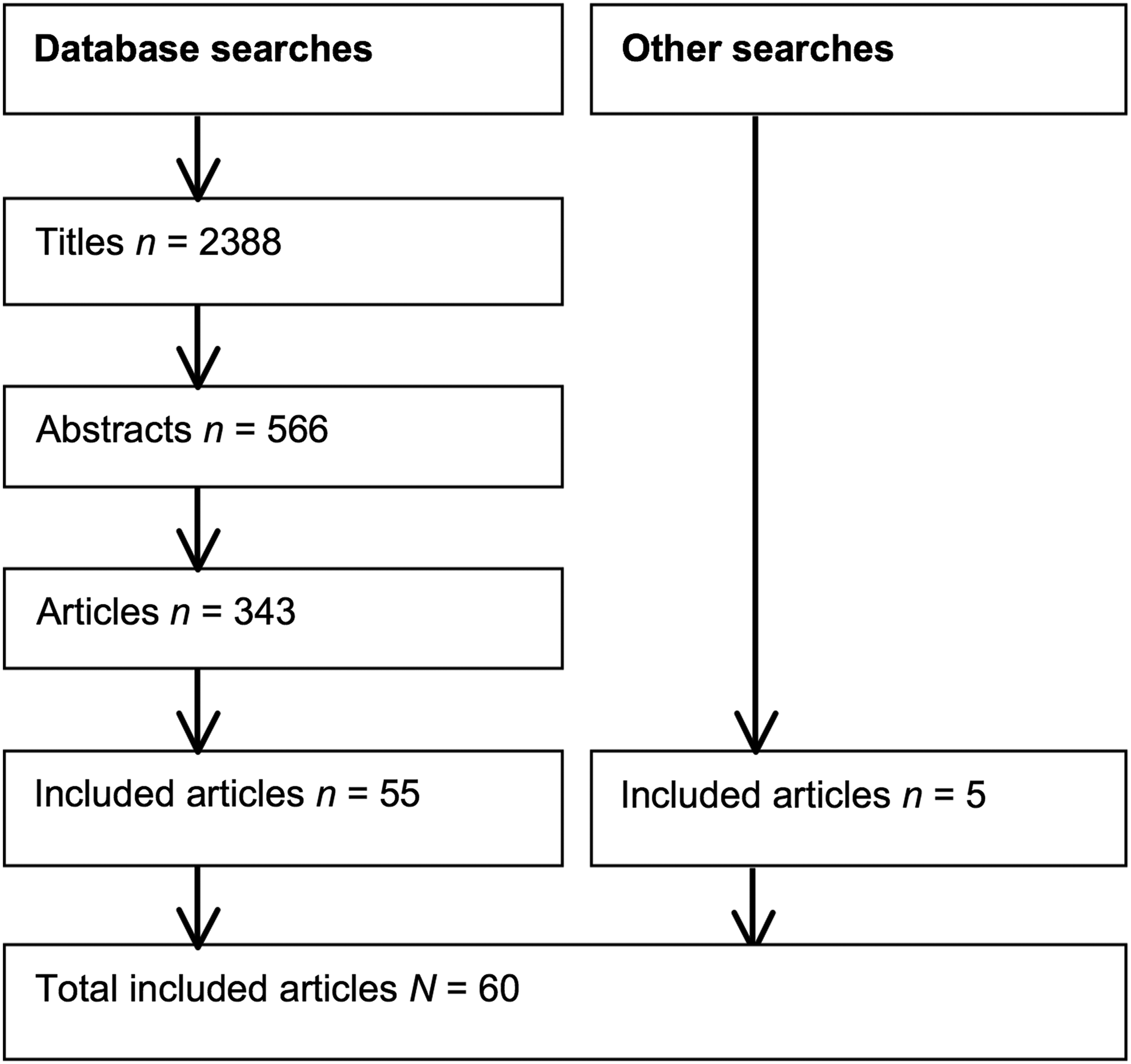
PRISMA flowchart of included articles. Note. Although four pairs of articles and two groups of three articles were publications describing different aspects of the same study's data set, because of the distinct areas of focus, the 60 articles have been viewed as 60 separate studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Results
Description of articles
Thirty-seven of the 60 included articles were from the United States or Canada, eight were from Norway or Sweden, and three were from the United Kingdom. All were published between 1992 and 2013. The 60 articles encompassed a total of 52 separate studies, as four pairs of articles23,29–35 and two groups of three articles36–41 were publications describing different aspects of the same study's data set. It was decided to handle these as different studies, because of their distinct areas of focus. Therefore, for the purposes of this review, the 60 articles were viewed as 60 separate studies.
Thirty-six studies were cross-sectional and observational. Of the 24 prospective longitudinal studies, five were interventional clinical trials. Most studies involved only quantitative methods, though seven were qualitative and eight employed a mixed-methods design. Most were rated as medium or poor on Gough's Weight of Evidence Framework. Although 13 were of high quality on Weight of Evidence A (integrity of the evidence in its own terms),17,30,40,42–51 only three were judged to be of overall high quality by Weight of Evidence D.17,30,47
All participants (aside from those in some of the control groups) had a cancer diagnosis. Five studies only recruited patients with lymphoma and/or leukemia,31,32,45,52,53 and one had only patients with extremity bone tumors. 54 All of the remaining studies investigated more than one cancer type. The majority of participants were in the 13–24 years old age range in 46 studies; subgroup data for this age range was presented separately in the remaining 14 papers. The number of patients within each study ranged from 855 to 199, 56 and the median or mean time since diagnosis ranged from 2 months 57 to 20 years. 32
Fatigue was the study's focus and the first outcome measure described in the results for only 18 studies;5,18,19,23,30–32,35,36,42,46,47,50,54,58–61 two of these involved validating symptom measures46,59 and none were interventional. Across the 60 included studies, the most commonly used fatigue outcome measures were the Fatigue Scale-Adolescent (FS-A), 59 the Multidimensional Fatigue Scale (MFS), 62 and the Memorial Symptom Assessment Scale (MSAS 10–18), 63 used in 14,12, and 8 studies, respectively. Eleven studies used a range of other validated fatigue measures, including the Chalder Fatigue Questionnaire, Piper Fatigue Scale, and the Functional Assessment in Chronic Illness Therapy fatigue scale. Eight studies used unvalidated measures, and the remaining seven studies were entirely qualitative in design. Table 2 provides further detail on the more commonly used measures.
Fatigue prevalence
Twenty-four studies investigated the prevalence of TYA cancer-related fatigue (Table 3). Fatigue was measured during treatment in 14 studies, after treatment in five studies, and in a mixed population of patients both during and after treatment in five studies. A “fatigue case” was most commonly defined as fatigue being scored as “present” using the MSAS, a score of anything other than “no fatigue” on a 5-point Likert scale, or a dichotomized score of ≥4 on the Chalder Fatigue Scale. 64
ALL, acute lymphatic leukemia; AML, acute myeloid leukemia; ARM 1, Adolescent Resilience Model study 1; ARM 2, Adolescent Resilience Model study 2; CFQ, Chalder Fatigue Questionnaire; CNS, central nervous system; D1, D2, etc., day 1, day 2, etc.; DXM, dexamethasone; EBT, extremity bone tumor; FACIT-fatigue, Functional Assessment of Chronic Illness Therapy-Fatigue Scale; FS-A, Fatigue Scale-Adolescent; FS-P, Fatigue Scale-Parent; HD, Hodgkin disease; LSS-A, Life Situation Scale for Adolescents; MFS, Multidimensional Fatigue Scale; MSAS (7–12, 10–18), Memorial Symptom Assessment Scale (for 7–12 and 10–18 age range); NORMS, healthy controls; NRS, Numerical Rating Scale; QOL, quality of life; RT, radiotherapy; T1, T2, etc., time point 1, time point 2, etc.; TC, testicular cancer; TRSC-C, Therapy-Related Symptom Checklist-Children; VAS, Visual Analogue Scale; VRS, Verbal Rating Scale.
The heterogeneity of study populations, outcome measures, and definitions of “fatigue case” hindered comparison of prevalence data between studies and prevented meta-analysis. Fatigue prevalence ranged from 7% 47 to 100% 65 during treatment, 9% 50 to 67% 66 after treatment, and between 31% 56 and 100% 67 in the mixed populations. As detailed in Table 3, the prevalence of fatigue and other symptoms were compared on 20 occasions in 10 studies; it was the most prevalent symptom on 11 occasions17,33,34,65,68–71 and the second-most prevalent on six occasions.17,71–73
Two studies—both with survivor populations—included a control group; both used non-contemporaneous controls. Aksnes et al. found a fatigue prevalence of 14% in extremity bone tumor survivors, which was not significantly different from that of age- and gender-matched cases from healthy population surveys (p=0.30). 54 In contrast, Hamre et al. reported a fatigue prevalence of 34% in survivors of Hodgkin lymphoma, compared to 8% in an unmatched healthy control population (p<0.001). 32
Fatigue severity
The severity of fatigue was measured in 32 instances: 20 studies during treatment, five studies after treatment, six studies with a mixed cohort of patients both during and after treatment, and one study that provided data on two separate patient cohorts during and after treatment, respectively. Seven studies reported relative severity of fatigue in comparison to other symptoms: fatigue was most severe in four studies,34,52,68,69 second- 70 and third-most 72 severe in one study each, and fourth-most severe in two studies.40,67 Fourteen different outcome measures were used across these 30 studies. The most commonly used outcome measures were the FS-A, MFS, and MSAS, in nine, eight, and four studies each, respectively. Comparison and synthesis of severity scores was again not possible due to heterogeneity of study populations, methods of reporting the data (for example, absolute score or percentage with score above a defined value), or measures used.
Three studies incorporated a control group, all of which compared fatigue severity in patients during treatment to that in survivors (Table 4). Controls ranged from contemporaneous recruits to unmatched reference data. All three studies showed significantly greater fatigue severity in the cancer groups compared to the controls.
AYA, adolescent and young adult; AYA HOPE, Adolescent & Young Adult Health Outcomes & Patient Experience study; CFQ, Chalder Fatigue Questionnaire; EBT, extremity bone tumor; HD, Hodgkin disease; HRQOL, health-related quality of life; MFS, Multidimensional Fatigue Scale; NORMS, healthy controls; QOL, quality of life; TC, testicular cancer.
Eight studies compared fatigue severity between younger children and teenagers treated for cancer, of which five measured fatigue with both the Fatigue Scale-Adolescent (FS-A) and the Fatigue Scale-Child (FS-C).37,53,60,74,75 The FS-A and FS-C 76 each use 14 age-appropriate questions and are validated for 13–18 and 7–12 year olds, respectively. Fatigue was reported as being more severe in adolescents than in younger children in all but one of the eight studies. 53
Many of the studies that used the FS-A outcome also measured parent reports of fatigue,37,38,47,49,59,60,74,75,77 but patient and parent scores are not directly comparable. One study did directly compare the fatigue scores of TYA patients with proxy scores from their caregivers, and found that their caregivers tended to overestimate their fatigue severity. 30
Fatigue severity was assessed over time in 11 longitudinal studies; all involved participants currently receiving chemotherapy.23,35,37,57,60,68,71,75,77–79 In general, fatigue scores were worse in the two weeks after receiving chemotherapy and then improved until the next cycle. No longitudinal studies investigated fatigue severity over the longer period from treatment into survivorship. One small cross-sectional, observational study of three groups of adolescents during treatment (n=8), 1–2 years after treatment (n=6), and five or more years after treatment (n=8) found that fatigue scores were highest during treatment, lowest during early remission, and higher again during late remission. 18
Impact of fatigue
Twenty-two studies reported the impact of fatigue on patients.17–19,23,33,34,37,39–43,48,55,68,72,73,80–84 Distress caused by fatigue was the most commonly described impact, reported in 11 studies. The MSAS, a scale that allows comparison of the level of distress caused by each symptom, was used in six of these studies.17,33,34,68,72,73 When symptoms were ranked in order of distress, fatigue was in the top half with only one exception. 17 One study reported that distress was correlated with the frequency and severity of fatigue. 34 The remaining five studies used diverse measures of distress,40,43,55,82,83 and fatigue was one of the top four most distressing conditions in four of these studies.40,43,82,83
The second-most frequently described impact of fatigue was that it was a barrier to physical activity or exercise, which was reported in six studies.18,23,42,80,81,84 Fatigue was the first- 80 and second-most 84 significant barrier in one study each. Being unable to take part in exercise led to frustration and loss of confidence, with parents becoming “overprotective” and preventing their adolescents from taking part in activities that demanded energy. 42 Four studies reported fatigue as a barrier to other social activities,18,23,42,48 including returning to school. 48 A negative impact on affective state, mood, or anxiety was described in three studies.19,23,37
Experience of parents
Although 10 studies collected parent proxy reports of fatigue severity,30,37,38,47,49,59,60,74,75,77 none investigated the experiences of parents of adolescent teenagers or young adults with cancer-related fatigue. Parent proxy reports of fatigue severity correlated more closely with those of their children for parents of cancer patients than for parents of healthy controls, which was attributed to the cancer patients' parents being “physically closer” and “more attuned to the needs” of their children.30,59,61 However, cancer patients' parents appeared to be less adept than the patients themselves at perceiving changes in fatigue over time.60,77 One study collected staff proxy reports of patient fatigue as well as parent proxy reports, and found that staff reports correlated less tightly than parent reports with patients' self-reported fatigue. 59
Fatigue correlates
Factors correlating with the presence or severity of fatigue were reported in 27 studies, including five of the six scoring highest on the Gough's Weight of Evidence Framework.30,38,47,49,51
Eleven studies highlighted an association between fatigue and physical symptoms, including poor sleep,35,37,57,61,74,75 being part of a symptom cluster,33,70,73 and nausea.29,61 Almost all participants in the three studies that examined symptom clusters were receiving chemotherapy;33,70,73 although there was no consistency in the specific symptoms found to cluster with fatigue, the symptoms tended to be chemotherapy-related. While receiving chemotherapy23,36,44,47,60,66 or dexamethasone 45 both correlated with increasing fatigue, the evidence for a correlation between fatigue and hospital admission47,60,72 or anemia46,60 was conflicting. Even though patients associated fatigue with “doing too many things” or “being too active,”5,23 there was a correlation between improved performance status and lower fatigue scores.46,78
Depression or low mood correlated with fatigue in five studies;30,38,59,61,85 negative affect, 29 global distress, 72 anxiety,33,73 and non-specific psychological conditions44,72 were identified as correlates in a further five publications. Consistent with the link with physical and psychological symptoms, a high correlation with poor quality of life or satisfaction with life was reported in four studies.23,30,66,85
Although some of these correlations are intuitively likely to represent causal relationships—such as the relationship between fatigue and poor sleep quality—no studies addressed causality. However, one longitudinal study that observed a predictable fluctuation in fatigue during chemotherapy regimens of varying frequency 23 and a study involving planned periods on and off dexamethasone 45 both suggested causal relationships with fatigue.
Interventions to manage fatigue
Table 5 details the five interventional trials for TYA cancer patients in which fatigue was used as an outcome measure.43,74,79,86,87 Fatigue was not stated to be the primary outcome measure in any of the five. Three studies were uncontrolled79,86,87 and three were feasibility studies.74,79,87 Four involved evaluation of a structured activity intervention, and one investigated a self-care coping intervention. All of the interventions were standardized with a degree of individualization in accordance with each patient's exercise capacity. Two uncontrolled trials found a statistically significant benefit from their interventions,79,86 which involved intensive structured exercise in a gymnasium at weekly intervals for more than two months. The remaining two physical activity intervention studies involved bringing portable gym equipment to the patient's hospital room and did not find any significant effect.74,87 The self-care coping intervention was also ineffective. 43
FS-A, Fatigue Scale-Adolescent; FS-C, Fatigue Scale-Child; FS-P, Fatigue Scale-Parent; FS-S, Fatigue Scale-Staff; MFS, Multidimensional Fatigue Scale; PedsQL, Pediatric Quality of Life Inventory; PFS, Piper Fatigue Scale; QLI, quality of life index; QOL, quality of life; SDS, Symptom Distress Scale; SCT, stem cell transplant; T1, T2, etc., time point 1, time point 2, etc.; VRS, Verbal Rating Scale.
Discussion
This review provides evidence that fatigue is one of the most prevalent and severe symptoms experienced by teenagers and young adults suffering from cancer, occurring in the majority of patients and particularly prevalent during cancer treatment. This finding is consistent with evidence in adults with cancer, for whom fatigue is now accepted as the most prevalent symptom. 11
There were no studies comparing TYA patients' fatigue with that of older adults with cancer. However, a number of publications compared fatigue in TYA patients to that in young children, with fatigue being more severe in the TYA population. This is consistent with the developmental sleep changes of adolescence. Healthy teenagers tend to develop fatigue and daytime sleepiness related to inadequate sleep. 21 At this age, longer sleep is needed, yet shifts in circadian rhythms result in later bed times; the amount of time spent sleeping is further limited by unhelpful sleep habits, such as caffeine consumption and social engagements. 21 Controlled studies have shown that fatigue in teenaged and young adult cancer patients is even higher than that in healthy controls.30,32,51,54 The dual risk factors for fatigue development—having cancer and being within or soon after the teenaged years—appear to combine to create a particularly significant problem in this vulnerable patient group.
Cancer-related fatigue is not only present during or soon after treatment: several studies of TYA cancer survivors showed long-term continuation of fatigue many years after cancer diagnosis and treatment.32,52,54 Given that TYA cancer patients have an approximately 80% five-year survival rate, 6 this means that large numbers of young people are contending with ongoing morbidity while attempting to rebuild their lives after a cancer diagnosis.
Not only is fatigue prevalent, severe, and persistent, there is consistent evidence that fatigue causes significant distress, with a negative impact on quality of life. Fatigue may be a particularly distressing symptom in teenagers and young adults because of its impact on functioning at an age when independence and social interactions are high priorities. The inherent social isolation resulting from the diagnosis of a serious disease at a young age that can require years of burdensome treatment is further compounded by the presence of fatigue. The level of distress may also reflect the developmental stage of teenagers and young adults, who are more able than children to understand the significance of their symptoms and underlying cancer, yet may be less able to control and rationalize their emotions than older adults.
Despite the increasingly strong and consistent evidence base confirming the magnitude of the problem, there are no published studies evaluating interventions whose primary aim is to treat or prevent fatigue. The few interventional studies to date are mostly uncontrolled or feasibility studies investigating physical activity. Exercise is recognized as an effective treatment in adults with cancer-related fatigue. The presence of fatigue hinders activity, which then leads to deconditioning (or loss of “fitness”). This in turn worsens the fatigue, so leading to a vicious cycle that perpetuates the symptom. Exercise or activity is believed to work, at least in part, by preventing deconditioning and the development of this vicious cycle. Although two of the four physical activity interventional studies did report significant findings, both were uncontrolled. Given the well-established placebo effect that occurs with subjective symptoms such as fatigue, 88 the strength of existing evidence for intervention effectiveness in the TYA age group is, as yet, poor.
In the context of physical activity being the only intervention for fatigue with any—albeit limited—supporting evidence in the TYA literature, a significant finding of this review is that fatigue itself is a key barrier to activity. There is mounting evidence that resting is perceived by patients, parents, and healthcare professionals as the best approach to managing fatigue. Studies have found that young patients feel that “being too active” or “doing too many things” may worsen fatigue;5,23 that parents encourage rest; 42 and that in a mixed child and teenage population, healthcare professionals' most commonly recommended treatment for fatigue was rest and relaxation. 89
There is evidence that activity levels tend to decline during the teenaged years due to conflicting priorities, fear of injury, and a sense of embarrassment. 90 It is conceivable that TYA cancer patients may be particularly prone to such decline in activity; there may be perceived increased vulnerability to injury, and disease- or treatment-related bodily changes that could potentially cause self-consciousness. 90 Cancer-related fatigue, in combination with these normal teenage inhibitions, can therefore present a formidable barrier to activity, paradoxically the very intervention that appears to have the greatest potential to improve their fatigue. Furthermore, at this formative age, life-long habits are developed. Maladaptive behaviors such as inactivity are therefore even more likely to persist, perpetuating fatigue and its associated disability and adverse psychosocial sequelae long-term.
Strengths and limitations
The main strength of this review is its breadth: studies were eligible if they investigated any aspect of cancer-related fatigue in TYA-aged patients, and even those with only a subgroup of patients aged 13–24 were included. The database search strategy was effective, with five articles found from other searches. The included studies, however, were heterogeneous and of relatively low quality, limiting the strength of the findings. Although experts in the field were contacted, literature not formally published in the form of journal articles (so-called “gray” literature) may have been missed. Exclusion of articles not in English may also have led to the omission of relevant articles.
Implications for clinical practice
Clinicians should be aware of the prevalence and severity of fatigue in TYA cancer patients, as well as the significant distress it causes. It is possible that a degree of therapeutic nihilism has developed due the lack of clearly effective pharmacological interventions for fatigue. 91 Simply inquiring about the presence of fatigue in each clinical encounter may in itself be helpful, as this can openly acknowledge the problem and provide the possibility for peer and professional support.
Although the evidence base for exercise interventions is very limited, it is clear that encouragement of physical activity is likely to be helpful. In adults, it is well established that exercise improves cancer-related fatigue.15,92 The wider benefits of keeping active during and after cancer treatment include increased well-being, functioning, and quality of life, as well as reduced cancer recurrence and mortality.93–96 Clinicians, potentially lacking the time and knowledge to counsel TYA cancer patients about physical activity, should develop the skills to educate and address any misconceptions of TYA patients and their parents about the benefits of activity, should including confirming its potential to ameliorate rather than—as intuitively expected—worsen fatigue.
The correlation between fatigue and concurrent symptoms, such as poor sleep, is consistent with the evidence in adults that the management of sleep disorders 97 and other symptoms 98 can improve cancer-related fatigue. Rigorous control of concurrent symptoms, including education about sleep needs and habits in adolescence, may have a positive impact on fatigue.
Implications for future research
This review has revealed many gaps in the literature. Further prevalence studies are needed with concurrent controls, using a longitudinal design to evaluate changes in fatigue and fatigue-related distress within a cohort from treatment into long-term survivorship. It would be valuable to compare fatigue severity and associated distress in TYAs and older adults. Future studies could usefully attempt to establish the directionality of relationships between fatigue and other factors Determination of factors that cause, rather than are simply associated with, fatigue could helpfully guide fatigue management. Evidence for this review came from only five countries; further global research into TYA cancer-related fatigue is needed.
Use of dexamethasone in the TYA population appears to worsen fatigue by reducing sleep efficiency and increasing night-time wakenings. 45 Conversely, in adults, this drug may improve fatigue. 99 This conflicting evidence may indicate a genuine difference in the reaction to steroids of adolescents compared to older adults, and is worthy of further exploration.
Current research has established that cancer-related fatigue is a prevalent and distressing symptom in TYA cancer patients. It is essential that future research now focus on the development of interventions to manage fatigue, in order to limit the long-term suffering of this already vulnerable and burdened group of cancer patients. Physical activity—including determining its optimal forms and frequency—is a key research priority, as is assessing the impact of improving sleep hygiene and concurrent symptom control. Research considering parents' perspectives and experiences is also needed given that parental protectiveness may hinder the physical activity that could help ameliorate a TYA patient's fatigue. A deeper of understanding of parents' views and attitudes could facilitate meaningful education of parents that, in turn, effectively increases the activity of TYA cancer patients.
Conclusion
The fatigue experienced by teenagers and young adults with cancer is prevalent, persistent, and distressing. It has a negative impact on quality of life and social functioning that is particularly problematic at this formative age. The magnitude of the problem is established—it is now time to intervene.
Footnotes
Acknowledgments
SB and AS were funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East of England at Cambridgeshire and Peterborough NHS Foundation Trust.
Disclaimer
The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Author Disclosure Statement
No competing financial interests exist.