
Abstract
Purpose:
Self-perceived resilience may enable coping and mitigate poor psychosocial outcomes among adolescent and young adult (AYA) patients with cancer. In order to inform the development of resilience-promoting interventions, we aimed to: (1) describe AYA patient-reported resilience and (2) identify AYA patient-reported contributors and inhibitors of resilience.
Methods:
The “Resilience in Adolescents and Young Adults with Cancer” study was a prospective longitudinal mixed-methods study. Consecutive Caucasian patients aged 14–25 years old enrolled 14–60 days following their diagnosis of cancer and completed one-on-one semi-structured interviews both at the time of enrollment and 3–6 months later. Constant comparative analyses identified salient themes describing modifiable contributors and inhibitors to patient-perceived resilience.
Results:
Seventeen patients (85% of those approached) enrolled in the study. The mean age was 17 years (SD=2.6) and 53% were female. All patient definitions of resilience inferred an ability to handle adversity. Five themes emerged as predominant contributors or inhibitors of resilience: (1) stress and coping; (2) goals, purpose, and planning; (3) optimism; (4) gratitude and meaning; and (5) connection and belonging. Merged analyses suggested that AYA resilience was a balance that may be enabled by promoting certain skills.
Conclusion:
AYA patients with cancer perceive resilience as a balance. Learned skills in stress management, goal-setting, and benefit-finding may empower AYAs during their cancer experience, in turn improving long-term psychosocial outcomes.
T
Positive psychological resources may enable patient coping and mitigate negative outcomes. 17 In this regard, the construct of resilience represents a promising candidate for intervention. It implies an ability to withstand, bounce back, or even bounce forward from adversity18,19; however, defining and measuring resilience in cancer has been challenging.20–22 In non-cancer settings, resilience has been equated with individual characteristics23–25 or evolving processes of adaptation. 26 Family resilience models suggest an additional element of balance—whole families must learn to adapt to the new demands of illness while also attempting to maintain a semblance of new normalcy.27,28 In our previous work, we found that the parents of children with cancer attribute resilience to all of the above (characteristics, processes, and balance), 20 but that individual perspectives are highly subjective. 29 In addition, parent self-perceptions are associated with outcomes: those with low self-perceived resilience have higher rates of psychological distress, poorer social support, and worse health behaviors. 30
Among AYAs with cancer, resilience has been defined as the process of identifying or developing resources to manage stressors and achieve a positive outcome.31,32 To our knowledge, however, patient-reported perspectives of how to promote that resilience have not been described. Because self-perceptions may directly affect outcomes, we aimed to: (1) describe AYA patient-reported definitions of resilience and (2) identify factors that AYA patients believe contribute to or detract from their own resilience. Such information could inform the development of age-appropriate interventions designed to promote whole patient care during and after the cancer experience. 33
Methods
The “Resilience in Adolescents and Young Adults with Cancer” study was a prospective longitudinal mixed-methods study conducted at Seattle Children's Hospital (SCH), where the majority of patients are under 26 years of age. The study was approved by the SCH Institutional Review Board. Eligible patients were 14–25 years of age, English speaking, and diagnosed with a malignant tumor requiring chemotherapy treatment 14–60 days before study enrollment. In order to limit heterogeneity in prior life or current clinical experience, patients older than 25 years of age and those with central nervous system tumors and/or cognitive impairment were excluded.
Consecutive eligible patients were identified from the hematology/oncology inpatient and outpatient clinical services and were approached by their primary medical team to assess their willingness to participate. All interested patients were then approached by study staff. All patients aged 18–25 and parents of children aged 14–17 provided written informed consent. Patients aged 14–17 also provided signed assent to participate in the study. Each patient was offered $50 per interview in compensation for his or her time.
Qualitative interviews
One-on-one semi-structured interviews were conducted either in clinic or in the patient's hospital room at both enrollment and then again 3–6 months later. The interviews were all done by the same investigator (ARR), who is trained in qualitative methods. The flow of the interview changed over time. While all patients were asked “what does the word ‘resilience’ mean to you?,” interviews early in the study opened with this question, but responses tended to be abstract definitions that did not reflect personal experience. In order to meet our aims, we modified the interview guide mid-study and began instead opening with “how has this [cancer experience] been for you?” Exploratory items queried expectations, beliefs, worries, and concerns about cancer; personal strengths and challenges; sources of support; coping strategies; and quality of life. Each interview then closed with patients' perceptions of the word “resilience,” followed by their advice to future patients (“knowing what you know now, what advice would you give a patient with [same diagnosis] who was diagnosed today?”). No formal intervention other than standard psychosocial supportive care was provided between interviews. Interviews lasted between 30 and 90 minutes each; all were audiorecorded and transcribed verbatim, producing 324 total pages of interview transcripts.
Data analyses
All authors coded all transcripts using a constant comparative analysis to identify salient themes. 34 Participant responses from the first set of interviews (those conducted at the time of enrollment) were openly coded by examining words, phrases, and sentences which, in turn, directed the development of codes with short descriptors (e.g., “vivo codes”). 35 Constant comparative coding was used each time a new topic emerged to determine if it fit into one previously described or warranted a new code of data. Codes were then sorted and compared until data reached a saturation point. 36 This methodology was selected because of the exploratory nature of the study. Inter-rater reliability was assessed during serial team meetings, with any discrepancies discussed as a group until consensus or new coding terms were identified.
A total of 32 original codes emerged from participant responses during the first set of interviews. After these were established, axial coding 34 focused on the primary objective of identifying patient-reported components of “resilience” and revealed five themes that directly contributed to or negatively inhibited patient-reported resilience: (1) stress and coping; (2) goals, purpose, and planning; (3) optimism; (4) gratitude and meaning; and (5) connection and belonging.
This process was repeated with the transcripts from the second set of participants interviews (conducted 3–6 months after enrollment) to identify any emergence of potential new codes and verify continued saturation. Following team discussions of both the first and second sets of transcripts, individual authors re-reviewed and re-coded select transcripts (n=6–15 each) to validate themes and identify selected examples thereof.
Results
Between December 2012 and May 2013, we identified 22 consecutive patients who were eligible for enrollment (Fig. 1). Two were approached for an alternative survey-based study and were therefore not approached for this project. Of the 20 approached, 17 (85%) enrolled and completed the first interview; 15 (75%) also completed the second interview. Data from all patients were included, regardless of second interview participation.

Flow diagram of patient approach, enrollment, and completion of study interviews.
Participants were between 15 and 23 years old (mean=17; standard deviation [SD]=2.6); 53% were female (Table 1); all were Caucasian. Sarcoma was the most common cancer type (n=8), followed by acute lymphoblastic leukemia (n=5), acute myelogenous leukemia (n=2), and Hodgkin lymphoma (n=2).
SD, standard deviation.
Patient definitions of “resilience” varied; however, almost all inferred an ability to handle adversity:
• How I bounce back. • The ability to get through things. • Your resistance against something. • Being open to things. • How you handle something. • How well you rebound from something…being able to fight back. It can be taught. • Being able to find a way to deal with stuff. • It depends on the person and their experiences…it's kinda like exercising. You have to have done it before and…gain some muscle before you run a race…personal strength. • Your ability to come back from something. • When you build up the strength so you know that you can fight. • You can bounce back. • Not breaking down…not giving up…keep moving forward. • Keep going…like, get through everything…you go through a process…it's just like there's steps. • Having a plan…that you come back from it. • There's always good with the bad. It's kind of all a balance. • I don't know what that word means. (Two participants with same response).
Specific comments suggested inherent resistance to stress, learned coping processes, and ultimate recovery from challenging experiences.
Five themes emerged as predominant components of AYA patient-reported resilience (Table 2). These were unchanged from the first to the second interviews and were unrelated to individual-level patient characteristics; however, patients' examples became more descriptive and experience-based over time. Within each theme of the five themes, patients described both contributing and inhibiting components of resilience.
While this table shows only selected exemplary quotes for each theme, quotes are presented in their entirety in the online appendix (Supplementary Appendix can be found online at www.liebertpub.com/JAYAO).
Theme 1: Stress and coping
“Get through the stress…stay calm…don't panic.”
All patients endorsed needing to learn how to handle the stress of a cancer diagnosis, including its treatment and associated life changes. Patient-reported stress management and coping strategies varied. For example, some relied on pre-existing personal strength (“I've always thought I've been a strong person and just got through things”), while others relied on the simple passage of time (“just wait it out”). Some reported pre-existing or newly-developed skills such as guided imagery (“I've learned to imagine my happy place”), mindfulness (“you have to be aware of what's happening and what's going on in your mind and body…it's good to plow through it, but every now and then, step off the plow and look”), talking to parents or peers (“It would help to vent to someone else about it”), journaling (“journaling your feelings really helps”), or practices that varied by circumstance (“I've just sat down, taken a deep breath and said, ‘okay, let's do this,’ and other times I've screamed and punched my car. Whatever works.”).
In contrast, overwhelming stress, worries, and exhaustion inhibited patients' abilities to cope. Almost all patients associated cancer with possible death, and patients who dwelt on this fear reported feeling less resilient (“You get stuck worrying. It's just terrifying, you know?”). No patient reported that the stress or worry was constant. Rather, patients described periods of higher and lower stress that made immediate coping harder or easier, respectively.
Theme 2: Goals, purpose, and planning
“Try to have goals…the days you feel lost, like, you don't feel you can keep going? Picture those goals and have that help you to be strong and resilient.”
Almost all patients described a need to look forward to something, and many identified specific goals or plans (“Having something to work for, having that vision is really helpful…To see where I wanna be after this whole thing.”). These plans were sometimes simple. For example, one patient focused on her hobby of horseback riding; she said thinking about riding in the future enabled her to be resilient now. Several patients described looking forward to returning to school and some identified long-term career or personal goals such as becoming a nurse, advocating for other kids with cancer, or getting married.
“Not knowing what to expect” was cited as a particularly difficult aspect of the cancer experience. To many participants, the associated inability to plan for the future provoked anxiety and, in turn, inhibited self-perceptions of resilience (“How do you know what to overcome when you don't know what is coming?”). This was particularly true at the beginning of their cancer treatment. Once they gained personal experience with medical practices, they felt more knowledgeable (“At first I thought, ‘okay, my life is ruined’…but, it isn't as bad as I thought it would be.”).
Theme 3: Optimism
“Resilience is trying to keep the positives…you just gotta stay positive.”
Almost all patients reported that “staying positive” and/or “learning to find positives in the negatives” was a critical component of coping and, in turn, resilience. Likewise, much akin to the inhibitory nature of overwhelming stress, being “stuck in the negative” was seen as a barrier to resilience.
When asked probing questions about how to be positive, many patients described a concerted effort to identify new life perspectives, as one patient explained:
“The positives of cancer…it's a weird concept, you know? Not many people think about it and not many people see it, obviously, because it's like, not a positive time, physically and emotionally in your life. But you have to make it positive…Like, growing closer to family, closer to friends, seeing who's really my friends…I won't remember every stomach ache, but I will remember every friend that came and visited me…It's hard to be happy and have cancer at the same time, but I promise it's possible because I'm doing it.”
Theme 4: Gratitude and meaning
“The way you look at things, the way you look at life, your perspective, is really changed. You're not invincible. You can get sick and you can get hurt. And it makes you appreciate things. Stuff that's important, you know?”
As patients described methods to remain optimistic, they often went on to describe things for which they were grateful (e.g., relationships, periods of comparative physical wellness, new perspectives). Likewise, they often reported searching for and finding meaning in their cancer experience. For example, one patient said, “I think…God gave me this so I could see the suffering, so I could really understand, so I'd kinda know what I wanna go into [for my career].”
Specific negative emotions seemed to inhibit this process and consequential perceptions of resilience. One particular example was shame, which was often associated with the physical stigmata of cancer treatment, and seemed to disable participation in routine activities (“With the [feeding] tube, I won't be able to go to school anymore. It's hard enough without any hair. And then people are looking at you…with the tube that'd be too much.”). In other cases, shame was suggested by general comments about being labeled a cancer patient (“It makes me feel less of a guy, less of a man.”). In all cases, shame and other negative emotions made patients feel more vulnerable, more socially isolated, and less resilient.
Theme 5: Connection and belonging
“What's really helped me get through it is having a really good support system.”
In addition to themes that underscored individual differences and skills, every patient also described the need for social support, connection to others (e.g., family, peers, other cancer patients), or a sense of belonging. Feeling different, on the other hand, was repeatedly cited as a barrier to resilience: “It helps to be around other people, for me to cope,” one patient said, “but only when they don't treat me differently. Like, my family doesn't treat me differently, but other people, my friends, they do and that makes it harder.” Similarly, patients said that feeling abandoned and/or isolated was particularly difficult: “My best friend hasn't called me. I see him posting this stuff about, like, his girlfriend [on Facebook], but he lives down the road and doesn't even care about me…It's like, ‘really, dude? Your best friend? Come on, make an effort.’ It makes me sad.”
Merged themes
Taken together, the above themes suggest a delicate balance—specific components can positively or negatively impact patient-reported resilience (Fig. 2). For example, patients who are able to manage stress, set goals, stay positive, or find meaning seemed to consider themselves resilient, but in periods of high anxiety or transition (e.g., when they did not know what to expect), they felt their resilience lessened. Likewise, patients who perseverated on negative experiences or who could not create meaning or purpose tended to perceive themselves as less resilient. No patient believed resilience was static; rather, patients reported that their potential for resilience (“the balance”) shifted with particular moods, experiences, perspectives, and skills. Perhaps most importantly, all patients suggested that they could learn to shift that balance toward higher self-perceived resilience.
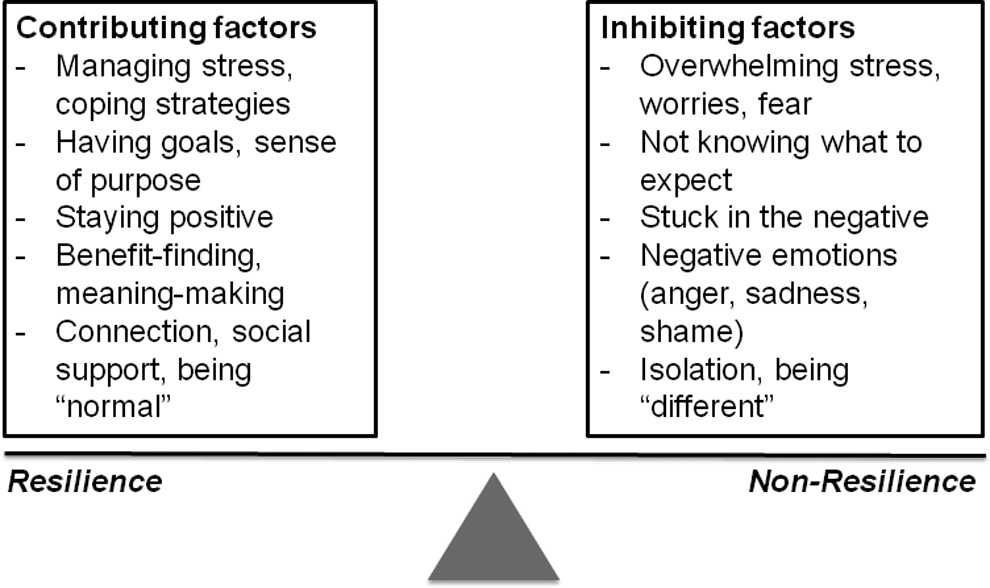
The balance between adolescent and young adult cancer patients' self-reported contributing and inhibiting factors of resilience. Potential interventions could translate these into teachable skills or programmatic support aimed at tipping the scales toward resilience.
Discussion
In this prospective mixed-methods study, we found that AYAs recently diagnosed with cancer predominantly associated their present (and potential) resilience with personal resources and learnable skills: stress-management, goal-setting, positive-reframing, and benefit-finding. Social support and maintenance of connections with family and peers were also critical. These factors were consistent across both interview points. Perhaps most notably, patients endorsed a sense of balance between contributing and inhibiting factors of resilience, indicating that promoting resilience contributors could “tip the scales” toward more positive coping and adjustment.
Coping and adjustment to the cancer experience, in turn, may be key predictors of long-term psychosocial outcomes among AYAs.37–41 Early interventions designed to promote positive psychological resources have shown promise in adults with cancer,42–46 healthy AYAs,47,48 and AYAs undergoing hematopoietic stem cell transplant for malignancy. 49 We have previously shown that self-perceptions of personal resources mediate these associations. 30 For this reason, understanding AYA patients' longitudinal needs and perspectives is imperative.
Unfortunately, one limitation of our study is that we lacked patient diversity: this study was conducted at a single institution among only English-speaking patients, and all of our participants were Caucasian. As such, we were unable to determine if resilience factors reflected racial or cultural differences. Similarly, our consecutively-enrolled patients were predominantly those with sarcoma, a distribution of diagnoses that is not typical of AYAs with cancer 4 and may therefore misrepresent the larger population.
An additional limitation is that our interview guide changed over time. Initially, we lead with a query to define “resilience,” but many patients responded with abstract (and perhaps less personal) responses. As we changed our approach, responses became more thoughtful. We were reassured, however, that the underlying implications of those responses (e.g., that resilience represented an ability to handle adversity) were unchanged before and after our modification.
We included multiple coders of diverse backgrounds (e.g., medicine, nursing, social work, and psychology) in order to represent a breadth of experiences; however, these experiences may have biased the development of our a priori coding schema. Finally, we did not include objective outcome measures or surrogate markers of resilience, nor did our study include assessments of ultimate psychosocial outcomes. As such, we cannot determine if our identified factors of resilience are truly associated with long-term patient functioning.
Our goal was to create a platform for the development of interventions that can then be tested in prospective clinical trials. Based on our findings, we believe that targeting individual resources and/or social support networks has potential. One challenge, however, will be how, when, and with whom to integrate such interventions into clinical care. AYA patients in this study endorsed needing the same critical skills at both the beginning of and later in their cancer experiences, suggesting that early interventions may be more valuable; however, they may be less feasible as newly diagnosed patients are also integrating a new vocabulary of medical terms and the demands of their illness. Likewise, which patients may benefit the most and how to include family members is unclear.
With this in mind, we have developed and are currently pilot testing a resilience-based intervention for AYAs with cancer at our center (“Promoting Resilience in Stress Management” [PRISM]).50,51 This intervention teaches four AYA-endorsed resilience-contributing skills: stress management, goal-setting, meaning-making, and benefit-finding. Future studies will test the intervention's efficacy.
Conclusion
Promoting resilience among AYAs with cancer has the potential to improve psychosocial outcomes; however, patient-reported factors of resilience have previously not been well described. Our findings suggest that AYAs perceive a balance of contributing and inhibiting factors of resilience during their cancer experience, and that many of these revolve around learned (or teachable) skills. Novel interventions that promoted these skills have the potential to improve patient outcomes and long-term survivorship.
Footnotes
Acknowledgments
We would like to thank the patients and families who participated in this research project, with special thanks to Daniel Mar for his perspectives, interpretations, and inspiring degree of resilience. We also thank Leah Kroon, RN, MN, CNS, for her perspective and contributions to our coding development, as well as James (“Devon”) Crouch and Victoria Klein for their assistance transcribing hours of patient interviews.
ARR and this project were funded by a St. Baldrick's Fellow award, a Young Investigator award from CureSearch for Children's Cancer, and a Clinical Research Scholar Award from Seattle Children's Hospital's Center for Clinical and Translational Research.
Disclaimer
Any opinions, findings, and conclusions expressed in this material are those of the authors and do not necessarily reflect those of the funding organizations.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.