
Abstract
Purpose:
This qualitative study aims to characterize the factors that influence access to fertility preservation (FP) resources and services after cancer diagnosis at NCI Community Oncology Research Program (NCORP) minority/underserved community sites, which serve patient populations comprising at least 30% racial/ethnic minorities or rural residents.
Methods:
Phone interviews were conducted from 2014 to 2015 with interested and knowledgeable healthcare providers practicing at NCORP minority/underserved community sites, using a semi-structured interview guide. Data were transcribed, de-identified, and analyzed using qualitative analysis software, Dedoose, to determine the most common themes in access to FP resources and services.
Results:
Interviews were conducted with 10 board-certified physicians practicing at 10 of the 12 NCORP minority/underserved community sites; five respondents identified as oncologists, and five were reproductive endocrinology/infertility specialists (n = 4) or obstetricians/gynecologists (n = 1). Findings revealed highly variable access to FP resources at each site. Notable barriers to FP services were cost, time, provider education, lack of clinical guideline application, and perceptions among healthcare providers that negatively affect the discussion of options and risks with eligible patients.
Conclusion:
Clinical FP guidelines and resources for cancer patients and healthcare providers need to be better integrated into existing cancer networks that serve minority and underserved patient populations. Providers need more education regarding timely provision of FP services to all newly diagnosed cancer patients of reproductive age.
T
Racial and ethnic disparities in oncofertility have also been described,17–20 and are thought to arise from a host of interlinked socioeconomic, cultural, and environmental factors. 21 Cancer patients from racial and ethnic minorities are less likely to pursue assisted reproductive technologies (ART) and have poorer success rates when they do. 19 They are more likely to experience poor or delayed access to services, and may face financial difficulty, harbor mistrust of the healthcare system, and experience racial stereotyping by practitioners.18,19,22 The ongoing controversy regarding whether insurance should cover the cost of FP further complicates the issue.23–25 Remarkably, when such barriers to access are removed, for example in a prior model of the military healthcare system where access to medical services was made widely available, the use of FP technologies was noted to increase fourfold among African American women compared to the general ART population in the United States.19,26
The 2013 American Society of Clinical Oncology (ASCO) clinical practice guideline update on FP for patients with cancer highlights the need to address disparities in FP access. 27 In this context, this study aimed to examine factors that affect access to FP resources and services at NCI Community Oncology Research Program (NCORP) minority/underserved community sites. The NCORP was created in June 2014 to facilitate community-based cancer care delivery and eliminate disparities through a network of 7 research bases, 34 community sites, and 12 minority/underserved community sites. The 12 minority/underserved community sites are distinct within the NCORP network because they represent hospitals, oncology practices, and integrated healthcare systems that serve patient populations comprised of at least 30% racial/ethnic minorities or rural residents. 28 To date, no study has explored issues related to access to FP resources and services in a largely minority-serving, institutional setting. Thus, the NCORP minority/underserved community sites are an appropriate focus for this study. By identifying the factors that either facilitate or restrict access to FP resources and services by cancer patients in low-resource and rural environments, steps can be pursued to improve access and eliminate health disparities in preservation of fertility for newly diagnosed cancer patients.
Methods
Sample recruitment
Telephone operator services were contacted at each of the 12 NCORP minority/underserved community hospitals. A request was made to speak with any healthcare provider(s) responsible for discussing fertility risks and FP services with newly diagnosed cancer patients. The scope of specialty and level of healthcare providers were left to the discretion of the operator. If no provider could be identified, a request was made to speak with administrative and/or clinical research staff within oncology, REI, or gynecology at the institution. An email was forwarded to identified staff members that summarized the study objectives, inviting them to participate and requesting additional information. If no response to the email was received within 2 weeks, up to three follow-up emails and/or phone calls were made. Participants were welcomed to nominate other colleagues at their institution. Using this purposeful sampling strategy, providers who were most likely to be familiar with and interested in the topic of FP were ultimately recruited for participation. All participants provided verbal consent, and the study was approved as exempt by Northwestern University and University of California, Irvine Institutional Review Boards.
Interview format
Interviews were conducted by telephone, using a semi-structured interview script designed by the research team (Appendix 1). All interviews were conducted by one person (M.B.), who worked closely with a qualitative research team member (D.V.) for ongoing guidance and feedback. Responses were audio-recorded.
Data analysis
Audio-recorded data were transcribed verbatim, de-identified, and reviewed by the research team. Data were imported into qualitative analysis software, Dedoose (version 6.0.19), and analyzed using open, axial, and selective coding techniques by at least two research team members (M.B. and D.V.). Coding rules were established, and the first transcript was openly coded to create a code book. Multiple teleconference meetings followed between team members to review and define these codes. This process was repeated for each subsequent transcript, until all data passages were exhaustively coded, resulting in a total of 45 unique codes. Through an iterative, group discussion-based process, these codes were grouped into higher-order categories, which were subsequently consolidated into larger themes. Frequencies of responses were recorded to determine the most common topics (see Table 1). As new codes emerged, two different coders reviewed, discussed, and reconciled information to ensure consistency. Data saturation (the point at which no new codes emerged) was documented and was met by the seventh interview.
Results
Participants
Interviews took place between November 2014 and April 2015, with participants at 10 of 12 NCORP minority/underserved community hospitals participating (response rate of 83%). See Figure 1 for the cancer incidence percentages for racial and ethnic minority populations by NCORP minority/underserved catchment areas. Catchment areas include the state or states served by a single minority/underserved community site. Of the two sites that did not participate in interviews, neither responded to multiple requests and follow-ups, and for one, language may have been a barrier. Telephone operator services at this site were conducted in Spanish only, and identified contacts did not respond to multiple emails requesting participation in the study.
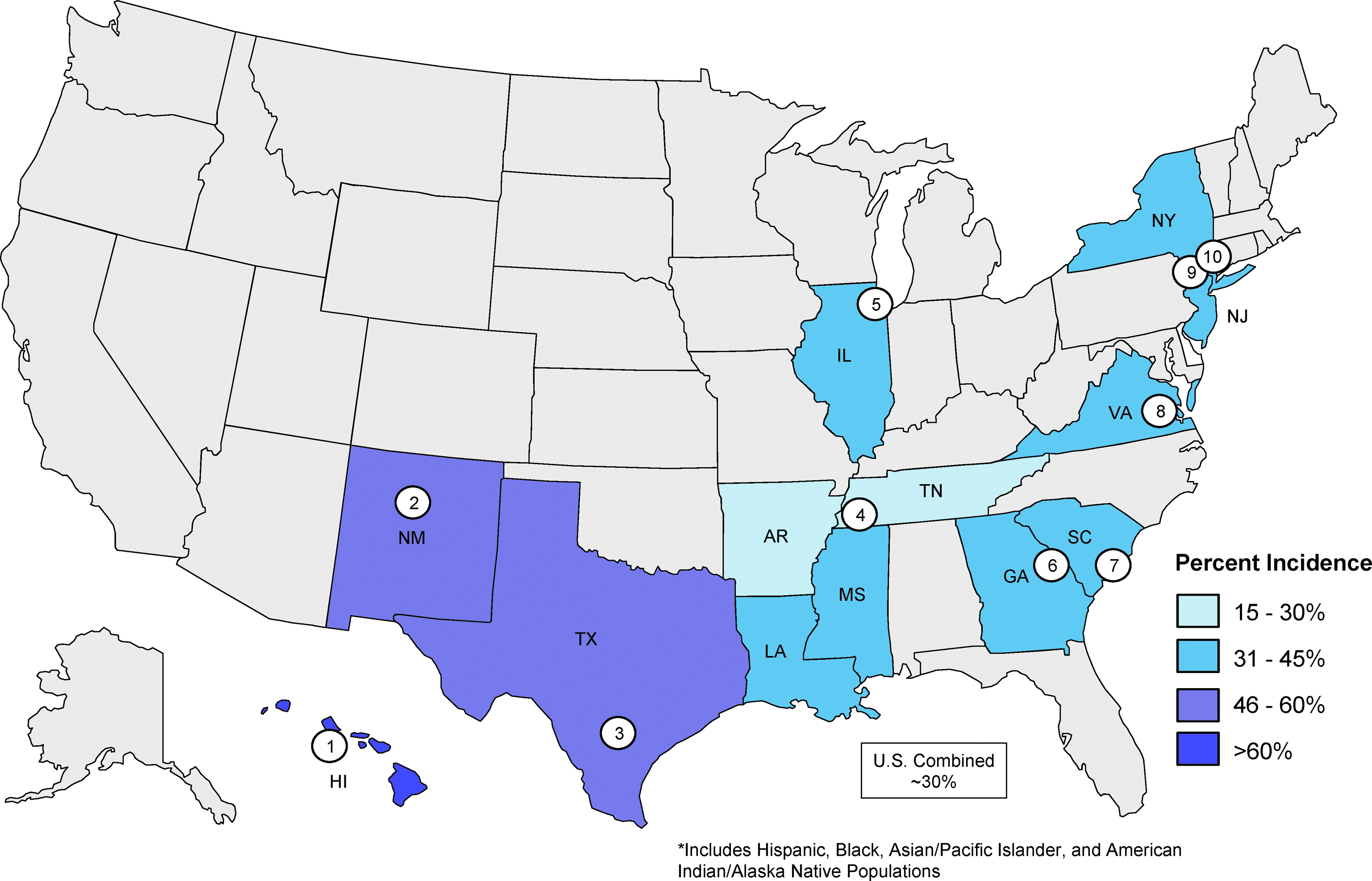
Cancer incidence percentages for racial and ethnic minority populations by NCI Community Oncology Research Program (NCORP) minority/underserved catchment areas. 48 Each minority underserved NCORP hospital that participated in the study is labeled by number: 1, The Queen's Medical Center; 2, University of New Mexico Cancer Center; 3, University of Texas Health Science Center at San Antonio; 4, Baptist Cancer Center; 5, John H. Stroger Jr. Hospital of Cook County; 6, Georgia Regents University; 7, Medical University of South Carolina; 8, Virginia Commonwealth University Massey Cancer Center; 9, Columbia University Medical Center; 10, Montefiore/Einstein Center for Cancer Care. Of note, the Puerto Rico Minority Underserved NCORP is not shown, as cancer demographics could not be obtained. Color images available online at www.liebertpub.com/jayao
Six of the participating sites were identified as university hospitals. Of the subjects recruited, all were board-certified physicians, with the majority representing medical oncology (n = 5) or REI (n = 4), and one affiliated with general obstetrics/gynecology (n = 1). One oncologist had a background in pediatric oncology, and one REI physician identified as a Fellow. The age of the participants ranged from 34 to 61 years. Six participants were female.
Survey results
Six major themes emerged during data analysis, based on the most commonly identified barriers or facilitators of FP in the cancer setting. Selected illustrative responses are provided below, organized by theme. Please refer to Appendix 2 for additional qualitative findings.
Theme 1: Resources
Educational resources
Half of the participants reported having fertility-specific educational resources offered at their sites for patients to review. Of these, few described use of self-created resources, in the form of pamphlets and brochures. One site had its own patient fertility hotline.
Some participants acknowledged referring patients to online educational resources, which included but were not limited to the Oncofertility Consortium, Fertile Hope, LIVESTRONG, or the American Society for Reproductive Medicine (ASRM), though it was unclear if this was done routinely. Few recalled ever referring patients to the free Oncofertility Consortium hotline (FERTLINE). One REI also felt that language used in some informational websites for patients “tends to be geared more towards physicians and practitioners and less toward the patients,” which was perceived to be a barrier to referring patients online.
Translation resources
Most participants reported having access to readily available, hospital-appointed interpreters and/or translator phones for a variety of languages at their sites. Some sites had consent forms available in Spanish or other non-English language. Few, however, described access to translation services at their facility as poor.
Referral resources
All non-REI participants reported needing to refer patients out to the community for FP access, as no in-house fertility specialists were currently available at their centers. Some identified this fragmentation of services as a barrier: “One challenge is that our reproductive endocrinologists aren't on site. The patients have to make a separate visit to a totally different part of the community.” All participants reported using some form of fertility referral system, usually through personal partnerships with local, private fertility centers. Few were familiar with or had ever used the National Physician's Cooperative (NPC) to refer patients to local fertility specialists.
Theme 2: Health system structure
Program structure
Access to ancillary services was a recurring theme among participants. Some expressed frustration at lack of assistance with fertility discussions and referrals: “Well you're speaking to the team, actually. I don't have a nurse coordinator typically for this so we pretty much—meaning I—have to arrange everything so that makes it a little, you know, cumbersome at times.” One participant described mid-level provider involvement as a facilitator, but very few acknowledged receiving support from trained non-physicians, such as fertility patient navigators, nurse coordinators, or clinical research associates.
Discussion structure
Several participants were able to describe a step-by-step fertility consultation process spontaneously. The process typically involved identifying patients at risk for infertility, discussing infertility risk at a clinic visit, and subsequently referring to a REI. Some REI participants 48 provided additional details on the initial consultation with risk assessment, discussion of options and cost, and the option for continued storage of gametes. One of these FP consultation programs had only been in place for 5 months.
Of those few participants who could not provide a clear step-by-step process for fertility consultation, one was unable to identify any FP program at their center, while three others provided minimal information and could not elaborate much even after probe questions were asked, suggesting lack of structure or consistency of fertility discussions with patients.
Payment structure
Several of the participants perceived the lack of financial coverage for FP for cancer patients as a barrier: “If it was more financially supported by insurance, I think more [patients] would have the opportunity to freeze eggs or embryos. I think more of them would take that opportunity.” A few participants described site-specific discount packages and payment plans as facilitators for FP. Some further reported provision of free IVF medications through partnerships with organizations including LIVESTRONG and Ferring Pharmaceuticals.
Theme 3: Time
Patient time
Half of all participants also reported that they consistently referred or were referred to within 24–48 hours from time of cancer diagnosis. Early discussion about fertility issues with patients was considered a facilitator to successful FP. However, time was also among one of the most commonly cited barriers to successful FP provision. REI representatives in particular perceived late referrals as a detriment to patients' fertility options: “If we had known a little bit sooner, like when they had been diagnosed versus when they were about to start chemo, we would have been able to at least have time for [patients] to have options.” The stress of diagnosis and urgency to start treatment were also described as potential barriers to FP: “Being single, not knowing what their future holds, and the underlying disease, whether it's potentially curable or not, these are more important issues in my opinion.”
Also highlighted were the time limitations of financial aid applications: “While there are organizations like Fertile Hope, which offer financial assistance, and pharmaceutical companies, which offer free drugs, the process to be approved for these is prohibitive. It can take weeks to months to get approval for these financial assistance packages and most patients with cancer want to start treatment yesterday.” Poor access to transportation among patients was further identified as a limitation for scheduling and keeping appointment times.
Provider time
One participant illustrated the challenge of discussing FP with every eligible patient in a clinic setting: “When you see 30 patients a day, you've got a mountain of electronic documentation to do, committees, meetings, so [patients] don't have a lot of discussion time. So in a patient with cancer, [fertility] is probably not going to be one of the higher priority topics.” Outpatient versus inpatient care was also thought to affect how much time a provider could dedicate to a fertility discussion: “On the inpatient service, you have 24-hour services to answer questions and help folks through the process; but on outpatient, patients have only half an hour to obtain the same information.”
Theme 4: Knowledge
Knowledge of guidelines
Several providers acknowledged familiarity with the recently updated ASCO guidelines on FP for cancer patients. However, none was able to provide specifics on guideline recommendations. Some felt these guidelines were not perceived by healthcare providers as a priority:
To have people really pursue these guidelines is challenging because first of all, our oncologists really want to get clinical care going … but also, not enough people know about the oncofertility groups or what's available to patients, and it's just not at the top of everyone's mind. So, I think guidelines are always there, but I mean how many guidelines do people follow in general? There's always a challenge between new guidelines and their actual translation and implementation. But I think, like everything, it's one thing if you have guidelines for something that's not costly, it's another thing if you have guidelines for something that's very cost-prohibitive to implement.
First-line provider education
A majority of participants identified first-line provider knowledge as a major barrier to FP access and a continued challenge to ensuring every newly diagnosed cancer patient of reproductive age receives a discussion about potential fertility risks of cancer treatment: “It's still 100% that first person, first-line provider who needs to address [FP] … doctors are the first challenge.” Regarding ways to improve education, one participant suggested, “Discussing how to get the word out in private practice as opposed to the academic centers may be one avenue of approach to try to fill that gap.”
Theme 5: Interest
Patient interest
Perceptions of patients' interest in pursuing FP were mixed among participants. Some agreed that “it's something that they almost always want to talk about, especially young patients.” Others had different stories: “Sometimes, they feel like ‘I'm too sick … if it's not an immediate issue, I don't want to deal with it.’”
Provider support
Support by providers and comfort level discussing FP was another commonly perceived facilitator to FP access. One theme was the perception among oncologists that offering unattainable services may be unfair: “I do wonder, in general, whether people don't offer it because they think people can't pay, without understanding what their capacity is, or they feel badly because they don't want to offer something that they feel won't be attainable.”
Clinical trials
Clinical trial enrollment among minority/underserved community sites was also a topic of interest to the authors, as it could reveal any barriers among providers of the institution to enhance FP-related research actively. Of all sites, only one participant reported having patients currently enrolled in a fertility-related clinical trial. While several participants agreed that clinical research was one driving component of an institution's interest in FP, many barriers to research in a minority/underserved setting were suggested. As one participant described, “The main challenge would be who would take ownership of a trial. Right now, I am the only medical oncologist that is even remotely interested in this, and I am one of three breast oncologists at the institution, so it's a matter of time and who would take over.” Others agreed that among their specific patient population, research was not always a priority: “When you see less affluent folks, they often have more advanced disease, and it's overwhelming having to talk about issues other than the things that they have to do right now to get them started on treatments, and even then, to bring up things that aren't always coordinated can be overwhelming, and I think these issues like the fertility issue then becomes less important as you're trying to prepare these patients for their treatment.”
Theme 6: Perceived patient factors
Socioeconomics
The majority of participants perceived out-of-pocket costs, regardless of insurance coverage, to be a significant barrier to patients' ability to pursue FP options: “It's one thing to be able to get a consult, another thing to be able to get the treatment. And if you have no money, you have no treatment. Once the consult is offered, so what? We send them over to [X institution], but it doesn't change anything except we check off on a list that we feel better that the information was given.”
Ethnicity/race
All participants were further asked about the perceived role of ethnicity/race, culture/religion, and access to FP. Half specifically identified Hispanics and/or African American patients as comprising the greater proportion of their patient population. However, there were mixed responses as to whether ethnicity or race was a barrier or facilitator to FP access. For example, REI providers were less likely than their oncology counterparts to perceive ethnicity and race as a barrier to pursuing FP: “I don't think ethnicity is an issue. Doesn't matter whether they are Caucasian, African American, Hispanic, etc. They have the same interest in pursuing fertility preservation.”
Culture/religion
The participants' responses were further mixed regarding the impact of cultural customs and religious beliefs on use of FP. As one oncologist participant observed, “Sometimes, in minorities, there is a stigma even with their cancer diagnosis … they can't even tell a relative or friend. They'd rather keep everything hidden. So that can make things difficult, with the diagnosis, with treatment, with fertility discussions, which is related.”
One participant found that religious views sometimes pose a barrier to FP. For example, “We have a big Jewish population, and they have very strong views on the importance of having children, but also, for example, masturbation is not allowed.” On the other hand, another participant from REI found religion to be a neutral factor in obtaining FP, in the setting of advanced technology: “Previously, we would have couples with religious objections to freezing large numbers of embryos, which they then potentially wouldn't be able to use … well, with freezing eggs and freezing sperm, that's no longer an issue.”
Education
Some identified patient education as a potential barrier to FP, though this was less common compared with participants expressing provider education as a barrier (n = 6). “I think the higher educated individuals are able to get information easier because they can search on the web and understand at an additional level and self-educate themselves, versus the folks that are less likely to have access … it's harder for them to understand the long-term consequences of their choices.” In contrast, another participant felt patient education was neither a facilitator nor a barrier in the setting of a devastating diagnosis: “Education helps, but nevertheless, I think for a young cancer patient, it doesn't matter how educated they are. As soon as they get a diagnosis and have to deal with set ABCD and the potential side effects of that upfront, that's challenging for any patient.”
Family dynamics
As with other areas, the perceptions of the participants regarding the impact of family on FP access were mixed. One participant stated, “In terms of the family unit, sometimes [our African American and Hispanic patients] don't have the family support that we'd like them to have.” Another perceived that “with our Hispanic population, they are very family-oriented. They really want a possibility for their children to have children in the future. A lot of times the family is involved, and if its money, the family will often do what they can to help the patient, so they have that option in the future.”
Age/sex
Some participants also offered patient age or sex as potential barriers, though less common a theme. From one oncologist: “The folks that are in their 30s or even their late 30s … to me the question becomes more of a philosophical question, where instead of going through all the details of what's involved in fertility preservation, you're talking more about what type of priorities are most important to you, where are you at in considering all this. It can be very overwhelming.” Another participant noted, “I would say we still try to have a discussion with all the females about fertility … because it is so much more complicated and expensive [than for males].”
Disease-related issues
Among less commonly identified barriers were also those relating to a patient's specific disease process, which could lead to skipping FP altogether: “There are concerns, in part, about leukemia and lymphoma. We've sent patients over to [X institution] … and we've had recommendations from them where they wouldn't do ovarian tissue freezing in some young women because they have leukemia.” Syndromic cancer was mentioned, as well as the curability of disease as factors in further determining priorities: “The fertility issue becomes a topic of discussion when [patients] have diseases that are potentially curable.”
Discussion
This qualitative study revealed variations in the provision of FP resources and services for newly diagnosed cancer patients at NCORP minority/underserved community sites. The study also found differences among providers at these sites in terms of the perceived facilitators and barriers to FP. Similar to the Oncofertility Consortium study on NCI-designated Comprehensive Cancer Centers (CCCs), 15 the findings above reveal that the recommendations in evidence-based guidelines for fertility preservation in patients with cancer are not being consistently translated into clinical practice, especially in low-resource, rural settings serving racial/ethnic minorities and socioeconomically disadvantaged patient populations. Given that the Consortium study on FP services in the CCCs was conducted in 2006, it was expected that by the time the ASCO clinical guidelines were updated in 2013, timely discussion of fertility risks and provision of FP options to cancer patients would have been better integrated into the cancer treatment network.
The social context of this study helps identify some significant perceived barriers to FP resources among providers who care for racial and ethnic minority patients with cancer, including lack of access to educational resources and fully informed healthcare providers, lack of access to efficient transportation, inability to afford services, variable levels of family support, and potential hesitance to participate in “non-standard” treatments (i.e., research trials), particularly in the setting of a stressful diagnosis. Many of these issues were also brought to light in prior studies addressing disparities in FP,17–19 and it is important to recognize that many of these issues are applicable to non-minority patient populations as well. For example, according to the ASRM, the average cost of a single in vitro fertilization (IVF) cycle in the United States is $12,400, with many women sometimes needing to complete several cycles before successful pregnancy. This expense can easily become a financial burden for anyone, especially patients already burdened with the high cost and distress of cancer care.
Furthermore, as this study demonstrates, many study participant perceptions were mixed regarding key patient-factor-related themes, such as ethnicity/race, culture/religion, family dynamics, and patient education. Some participants perceived certain patient factors to be barriers, while others shared stories in which those same factors were perceived as facilitators. For example, among the majority of REI participants, many of the issues described above, outside of ability to pay for services, were less likely to be perceived as barriers. This suggests that patients who ultimately received a fertility consultation were generally no different from anyone else in their capability to pursue fertility resources.
Psychosocial studies of young adult cancer survivors of racial and ethnic minority backgrounds have found that this population is highly interested in FP.29–31 One study found that cancer survivors of minority backgrounds expressed greater distress about their ability to have children and were more likely to request help than Caucasian survivors. 29 Despite patient interest, providers acknowledge that their perceptions of a patient's background and his/her ability to afford or follow through with services sometimes dictates whether or not they bring up the topic of fertility.11,32 This implies that many patients may never understand or even hear about risks to their fertility until it is too late. Thus, the largest barrier, perhaps, to minorities and other populations gaining access to FP services may be the perceptions (and sometimes misperceptions) of practitioners regarding their patients' interest in or ability to access FP resources and services. These misperceptions can be addressed by shifting greater focus to educating providers and holding them more accountable for their knowledge of the most updated clinical guidelines, including available professional education and navigation resources provided by groups such as the Oncofertility Consortium, NPC, ASCO, and ASRM. The development of scripts or checklists to guide fertility discussions that take into consideration the issues faced by racial/ethnic minorities and socioeconomically disadvantaged patients may be further warranted. Notably, the need for widespread education of physicians on FP in the cancer care setting was also recognized by the majority of the study participants, and this may be addressed through the addition of relevant teaching curriculums early in the training of healthcare professionals.
One area of need, as demonstrated by the study findings, includes greater use of available patient education resources. As only half of participating NCORP minority/underserved community sites offered any form of pamphlet or brochure to fertility-eligible patients, it is highly probable that many patients leave their clinic visits with unanswered questions, even after discussion of fertility risks. Given one participant's observation that less-educated patients are also less likely to pursue information not already provided to them, it is imperative that sites adopt some form of informational guide on fertility and FP that can be given to their patients. The Oncofertility Consortium and ASRM, as only a few examples, host websites with patient-facing information that can easily be printed as handouts and/or used to augment written materials for patients with Internet access. Few, if any, external educational resources were routinely used by study participants, suggesting a general lack of awareness regarding the wide breadth of available online patient resources.
Another significant theme to emerge from this study was the need for more comprehensive referral services, reduction of fragmentation of services, and better integration of ancillary services in FP in the cancer setting. While the majority of participants acknowledged access to some type of referral system, it is noteworthy that only two had ever used the NPC to refer their patients to fertility specialists. The NPC is a national network of collaborating oncologists and REI specialists that provides practical guidance and referral services to clinical practices interested in providing FP options to their patients. Thus, greater awareness and use of this network by NCORP minority/underserved community sites may help improve access to FP services.33,34
A concern raised by some participants is that patients must seek FP services away from the NCORP institution. This issue is perhaps well addressed by introducing patient navigators or care coordinators—mid-level providers who can guide patients from the time of their cancer diagnosis, to their REI referral, and back to cancer treatment. Increased utilization of patient navigators, which have been shown to be successful in certain programs,35–41 could certainly provide additional opportunities to explain fertility risks, outline FP options, schedule appointments, offer supportive counseling, and, most importantly, help patients navigate the healthcare system. 41 However, successful integration of patient navigator systems, particularly in low-resource and rural care environments, can be challenging given the significant cost and expenses exceeding that of current standing nursing and support staff. One possible solution is to bring more attention to educational interventions, such as eLearning training programs aimed at oncology, gynecology, and/or REI nurses to help facilitate FP discussions with patients. 42 Innovative use of existing nursing and supportive services can be more cost-effective in the long term to address both fragmentation of services and integration of ancillary services, while helping overwhelmed first-line providers better manage time—one of the most commonly identified limitations to FP provision in the cancer setting.
While cost of FP services may not be immediately addressable, the fact that these services are not covered by insurance poses a significant burden to all patients seeking a reproductive future, but especially to financially disadvantaged patients. Currently, only 15 states have enacted some form of insurance mandate for patients facing infertility unrelated to cancer. Yet, no such mandates exist for newly diagnosed cancer patients.43,44 This seems unjustifiable, given that infertility during cancer is often an inevitable, iatrogenic outcome of cancer treatment, and cancer patients have an exceptionally narrow window of opportunity to pursue FP services, which usually closes with commencement of cancer therapy. Furthermore, insurance companies have historically covered treatments for other iatrogenic conditions. Thus, it seems warranted that state and/or federal mandates should be actively developed to facilitate lowering costs of FP services among the cancer patient population as well. Such action would not only help increase FP access among patients of lower socioeconomic backgrounds and those without insurance, but would also encourage more FP-related discussion between patients and their healthcare providers. Indeed, anecdotal evidence suggests that coverage is provided by some insurance companies on a case-by-case basis. For example, the Northwestern University branch of the Oncofertility Consortium has previously appealed and negotiated coverage of FP treatments for many patients. 45 Insurance waiver letter templates are also currently available on the Oncofertility Consortium website. 46 Greater support from healthcare professionals for their patients' rights to a healthy, reproductive future could truly help drive eventually universal coverage of treatment for iatrogenic infertility. Until then, alternatives to alleviate some of the financial burden of FP services include increasing institutional incorporation of discounted programs and payment plans, as well as promoting community and other philanthropic fundraising efforts.
While the lack of active clinical trials among NCORP minority/underserved community sites was disappointing, it was also expected. Encouraging more providers to participate in FP clinical trials can certainly facilitate collaborative research across oncofertility and REI disciplines, which can further facilitate uptake of effective, evidence-based FP practices into routine cancer patient care. 47
This study is not without limitations. Ten of the 12 minority/underserved sites are represented in this interview process, yielding a response rate of 83%. Some might argue that because only one individual participated from each site and because all participants were physicians, this study's conclusions are limited, perhaps even biased. However, the sample size obtained and the provider level of the participants involved are noteworthy findings, in and of themselves, as they point to several barriers to the progression of FP services at minority-serving cancer centers. First, the majority of telephone operator services at these centers were unaware about which department had information on FP provision for cancer patients, which underscores how poorly integrated FP still is within these cancer care networks. Administrative and clinical directors were furthermore contacted at every location for assistance, but many took weeks and often months to respond to telephone calls and email correspondence, primarily due to difficulty identifying FP-knowledgeable contacts for participation. Some site directors never responded at all. Several attempts were made to recruit multiple interviewees at each site, but in the end, the research team's efforts were challenged by not only a lack of FP awareness at these sites but also a lack of structure, including access to ancillary services. The physicians participating in this interview process were ultimately identified by their institutions as the key individuals driving awareness of FP among their respective minority/underserved populations. While there was certainly interest among this group, as a whole, to expand FP services within their communities, the majority agreed that their efforts were limited by time and sparse resources.
Therefore, the authors propose that the sample size of this study reflects an unmet need rather than a flaw in study design. In fact, it is significant that data saturation during the course of our research was documented and was met by the seventh interview (as determined by two different coders), which suggests that n = 10 sufficed to meet the objective of this qualitative study. The authors predicted that there would be several gaps remaining in the fluid translation of FP bench work to bedside, particularly among populations with limited access to care. This is the first study to examine Oncofertility in the NCORP minority-underserved setting and serves as a meaningful start to exploring further how to improve access nodes among minority/underserved cancer patients seeking FP. Raising greater awareness about the obstacles ahead can only help to bolster efforts to one day enable successful FP for this patient population.
Conclusion
This study found several variations in the FP resources and services provided to patients with cancer at NCORP minority/underserved community sites. In the sample of physicians at these sites, numerous perceived barriers to FP were identified within minority and underserved patient populations that could be addressed to improve patient access and reduce disparities. To improve provision of FP resources among racial and ethnic minority populations and all populations in general, greater emphasis needs to be placed on promoting provider education, offering educational resources to patients, using more comprehensive referral services, reducing fragmentation of services through better integration of ancillary services, and increasing opportunities for related clinical research. Given that future fertility has become a significant survivorship issue for young cancer patients, it is important that FP resources and services be better integrated into cancer care such that all eligible patients receive information about fertility risks of their cancer treatment and are provided a fertility consultation, if desired.
Footnotes
Acknowledgment
The authors thank Stacey Tobin, PhD, for scientific editorial assistance for this manuscript.
Author Disclosure Statement
No competing financial interests exist.
Qualitative Findings
| Theme | Excerpt |
|---|---|
| Resources | |
| Educational | “Actually, the only pamphlet that we have right now, that we've been using, is the one that came to us through Oncofertility.” |
| “We have a separate [information brochure] for females and males, and it talks about the different options and then at the bottom gives them a phone number either for questions or to make an appointment.” | |
| “If they have an iPhone, I'll refer them to the iSaveFertility app. If they have a computer, then we'll refer them to myoncofertility.org.” | |
| “We don't leave pamphlets with patients, although it's not actually a bad idea.” | |
| “I think [a handout] helps a lot because it takes the mystery out of it. The person and their family have something tangible to take home and use to address any questions they want to go through again.” | |
| “Informational websites for patients tend to be geared more toward physicians and practitioners and less toward the patients.” | |
| “[We have] nothing unique to our center. We provide already available resources through the Society of Assisted Reproductive Technology, ASRM, and Fertile Hope.” | |
| Translation | “At the hospital, we have multiple Spanish translators because Spanish is a predominant language here … personally I prefer the translator in the room. That's my prejudice because I can get more visual clues of how patients understand the information.” |
| “If they speak French, then I can speak French to them perfectly. But if they speak Spanish … too bad.” | |
| “We usually ask them to bring a family member or relative. Sometimes, there are translation services provided by the community … but it's something that has to be arranged ahead of time.” | |
| “So a lot of us can actually speak Spanish to our patients, and if for some reason, there is some language that we can't speak, we do have translator phones.” | |
| “We have onsite translators available for most languages, in person, from Arabic, to Spanish, to Chinese, and Cantonese. We also have written consents in English, Arabic, and Spanish.” | |
| Referral | “The oncologist has to be prepared to make a referral to an oncofertility specialist because that's not their area of specialty. So they have to be equipped with all the proper referral lines.” |
| “We send an email to our colleagues at an associated clinic because we don't have anyone at our academic center that sees the patients.” | |
| “We have a few fertility specialists here that we work with very closely and they seem like they are very receptive to our patients … they know that we need to possibly start treatment right away.” | |
| “I've got these guys that will see patients for me instantly. They don't belong to my hospital ownership-wise, but they work about 100 yards away from me.” | |
| “It's very rare for a patient in our population to get an oncofertility referral or to get any treatment. The best thing we have available right now is if there's a patient who has this interest, we can refer them to the Oncofertility Consortium.” | |
| Structure | |
| Program | “We don't have a navigator. I'm it.” |
| “We don't have a fertility specialist in house.” | |
| “Anything that makes it easier on the patient makes it easier on the treatment team, too.” | |
| “We have a navigator who is responsible for communication with patients, and we have an IVF nurse who deals with scheduling appointments and retrievals. | |
| “I have an NP [nurse practitioner] that works with me in the Late Effects clinic and she is also getting training in fertility preservation, and there was someone else here before, and she would actually be the one who would go and talk to almost all of the males.” | |
| “[Nurses] have a care plan for all the cancer patients. One of the items on that care plan is fertility preservation, so if it hasn't been brought up previously it's usually caught by the nurse practitioner during development of the care plan.” | |
| “At the cancer center itself, there are more resources. There are navigators and staff that we don't have here at the private office.” | |
| “Whoever sees that patient first, if that's surg onc, rad onc, or med onc, whoever that person is, addresses [the patients'] desire for fertility if we think they are going to be at risk due to potential need for chemotherapy.” | |
| Discussion | “[Discussion] depends on the cancer diagnosis and potential treatment.” |
| “For fertility preservation, really at the time of diagnosis is the best time [for discussion].” | |
| “I don't think there's a discussion. If there's any discussion about fertility preservation, it would have to be after a referral is made.” | |
| Payment | “If insurance covered [fertility preservation], that would completely change things. I mean the financials are really a problem.” |
| “[Insurance] plays a huge role because most patient in the state do not have insurance coverage. Although we do have some reduced fee options for some patients with medical indication to freeze eggs, it's still cost-prohibitive for a large portion of patients.” | |
| “We provide a 60% discount for our fertility preservation patients and also provide free medication applications.” | |
| “When we had the sperm bank that would basically not charge our patients, that made things so much easier. So it's been very unfortunate that that's changed.” | |
| “We've really overcome a lot with our plans and policies that we have in place both for tissue freezing and for egg and embryo freezing … which we think is very competitive. For the tissue freezing patients, they often pay nothing up front. We bill the insurance first. If they pay for the surgery, great. If they don't, then the hospital works with them.” | |
| “To my understanding, fertility preservation is not covered under any type of insurance program. Or not covered enough to be able to make it a reality for patients with insurance.” | |
| “We are trying to get a law passed here in [state] where cancer patients undergoing treatment that can cause fertility issues will be allowed to at least get an initial consultation and maybe even collection paid for by insurance.” | |
| Time | |
| Patient | “Besides the finances is the timing. Obviously, options will sometimes depend on how much time we get until they want to do preserving and that will determine whether we can do egg or embryo freezing or tissue freezing.” |
| “A lot of times, the oncologist won't send the patients to me because they don't want to delay the treatment for two weeks and they want to start right away. I'll let them know that they don't have to delay … we can do the two concomitantly.” | |
| “The process would be made easier by providing information as soon as possible after diagnosis of the patient. Certainly listening and understanding where they are during the treatment and what their goals are for the future [also helps].” | |
| “If they're on Medicaid and they only get around by bus, they're not going to get fertility counseling. I mean, they just can't make it. They've got to schedule it, and it's tough.” | |
| “In the stress of diagnosis, this topic may sometimes be overlooked. Especially in the younger patients.” | |
| “I think some people are less comfortable about talking about fertility stuff before they're even able to offer a treatment plan, which doesn't always make sense because I always think if you're going to treat anyway and we're [going to] say everybody should sperm bank, then it really doesn't matter what the treatment plan is.” | |
| “If you can tell that they're barely going to make their treatment appointments because they have no transportation you might say well there's no point in discussing because they don't have the personal or ancillary resources to get there.” | |
| “Sometimes the transportation can be a barrier … to be able to get to appointments … to talk to a fertility specialist.” | |
| Provider | “For pediatric oncology, the culture is still to start treatment pretty quickly … even in Hodgkin's disease where I think there is the most likelihood to be willing to wait, it still depends on where the disease is.” |
| “That's our goal, [to see the patient] within 48 hours of the time that we are notified.” | |
| “You don't really have enough time for the most part … it's really a challenge.” | |
| Knowledge | |
| Guidelines | “I don't refer back to them, I can't remember the details, but I'm sure they were pretty reasonable.” |
| “I guess I don't know them off the top of my head.” | |
| “It still doesn't help us in a sense because insurance doesn't cover [fertility preservation] anyway, but I think it makes people think a little differently about it.” | |
| “I saw the guidelines. They didn't change that much since the 2006 guidelines. I think some of the wording was a little different … but I don't know if it's followed through in clinical practice.” | |
| “We actually took a survey of a lot of CCOG members to see if they read them and some of the different recommendations, and we're actually going to submit it for publication.” | |
| “We have more awareness and certainly oncologists need to make patients more aware.” | |
| “Probably the biggest issue is education of the oncologists to let them know that there are resources available including the specifics of what our process is for the patient.” | |
| First-line provider | “In my experience, being at different institutions during the last year and a half, a lot of physicians seeing young cancer patients, who have been in practice for years and years, really didn't think [fertility preservation] was relevant and didn't think it was important to discuss initially with patients.” |
| “I think, right now, one big hurdle is the hematology/oncology world themselves … they're just not always getting the word to their patients.” | |
| “I think if the provider is comfortable talking about it, has knowledge about the topic, and makes the conversation move smoother, in contrast to a provider who really doesn't know any options … that creates a lot of ambiguity in the conversation and patients don't know what to think or make of that.” | |
| “Newer co-treatment with drugs like tamoxifen, Letrozole, and Lupron makes the oncologist more comfortable [to send patients with endometrial or breast cancer], since they know that the estrogen level will be kept at physiologic levels.” | |
| Interest | |
| Patient | “If you're sophisticated, educated, and this is a concern, you can get it addressed. And you drive your car and you show up at your doctor's visit.” |
| “I think for folks that are very young, like in their 20s, they are more interested in pursuing counseling regarding their fertility.” | |
| “They're usually very interested in it, especially because we have a large Hispanic population and families are important.” | |
| Provider | “I think it's pretty physician dependent because some of the peds heme/onc are really interested in fertility preservation and so I've talked to them a lot and worked with them a lot, so I think that's why we get a lot of referrals from them.” |
| “The provider has to open to this as a viable push for the patient, and the provider has to acknowledge that this is part of the care and that if it takes an extra week or two to get started on treatments, that's not going to change the patient's overall long-term benefits from the treatments.” | |
| “A lot of providers don't think it's important, so I think educating the provider is the biggest challenge/barrier so they in turn can empower, educate, and inform their patients. That's the challenge I have seen probably the most at my institution.” | |
| “As the oncologist, we try to be very supportive with all the decision making. And once they decide, we support their decision.” | |
| “I think if [primary providers] could just mention it or you know, give out one of our flyers, so at least the patient knows we are a resource, even if they don't have a lot of time to talk about it … if they just get them in contact with this us, then we can at least get the ball rolling for the patient. But it's hard for us if we don't know the patients are out there.” | |
| “You want the treating physician to be open-minded and to be supportive. I've never seen someone that's not.” | |
| “The real big [question] is does the doc have much of interest in the subject? They say ultimately it's the doc who decides. Well, if the doc doesn't care, nobody gets referred.” | |
| Clinical trials | “I didn't know that there's a need for it.” |
| “We have none going on right now. I can say that with certainty because I'm the research director.” | |
| “We actually had a multicenter study set up through one of the CCOPs but they lost their funding. So right now we're trying to get funding … we'd love to be involved in the clinical trials. We just haven't been given the opportunity.” | |
| “No, but we are very interested in it … our program is only 5 months old.” | |
| “We have some things in the works and trials are being designed.” | |
| Perceived patient factors | |
| Socioeconomics | “[Fertility preservation] can get quite expensive, particularly for young people who may not even have a career. Also the cost of storage …19-year-old [patients] may not be ready to have kids until they're in their 30s, so that's a lot of years to store something and [can be] expensive.” |
| “Patients in the lower financial brackets are less likely to be able to afford the process, even if they wanted to.” | |
| “I think it's perceived, especially by the oncologist, as unfair to even present something like this to the patient knowing that these facilities and programs are available, but not to [the patient], because it's not in financial reach.” | |
| Ethnicity/race | “Rich, white people get fertility referrals, because they want it.” |
| “I would say 60% of our practice is Black … most are in the lower socioeconomic class. They aren't going to make it and show up [to appointments], so it's a challenge even at the best of times. So, they don't ask, [and] they don't get a lot of referrals to fertility preservation doctors.” | |
| “We see a lot of African Americans, we see lower educated patients … certainly lower socioeconomic status, probably more than in other places.” | |
| “It takes about three Black people to get one consent signed … maybe it's a cultural thing, but they don't want to participate in studies. They don't want to be guinea pigs. I've seen that so many times—‘just give me the standard treatment, doc.’” | |
| Culture/religion | “Culturally, the only [challenge] really that I've seen is more so [from] the spouses than the patients themselves, where sometimes we don't get cooperation by virtue of not getting a semen analysis if we need it; [disagreement between couples] if they're going to do an embryo freezing.” |
| Education | “I think it's easier for [patients] when they have looked it up a little and have a little more background knowledge on the subject.” |
| “There's a level of sophistication needed. A lot of patients don't understand … you can talk to them, write it down, and they'll still scratch their head.” | |
| “Possibly, another area of approach would be to try to get the word out either through the media or through local sources too, to let people know that these services are available.” | |
| Family dynamics | “Usually if the patient is very young like in their early 20s, usually their parents are involved, too. And they're thinking about grandkids … which makes it a little easier. And if they're single … they get treated when more people are involved, like a spouse or parents. So family support is important.” |
| “It may not be true, but I think there's a segment of society in which the undereducated have more children at a younger age, and that segment may be less likely to want fertility issues addressed because they already have children. And they may or may not have ever had a spouse that can be financially or emotionally supportive.” | |
| “My experience here down in the South is that people aren't as interested in fertility preservation, and I have no idea if that's because our patients have children younger because a lot of our patients have already had children by the time they are even in their 30s getting diagnosed.” | |
| “If they have six kids already, [fertility preservation] is probably not a big issue.” | |
| Age/sex | “Maybe there is a little prejudice there. Someone in their 40s, we may not necessarily talk about fertility treatment, but maybe we should. But for someone in their 20s or 30s, I definitely bring it up.” |
| “The feasibility—it's almost impossible to get eggs from prepubertal girls and sperm from a prepubertal boy, so in those cases, we are talking about freezing testicular tissue and freezing ovarian tissue, both of which are still considered experimental.” | |
| “Males have mostly bought on with the sperm banking, but I think it doesn't always get discussed … for females, it still feels like it's such a huge effort, and again, I think it's the financial and timing delay that are most problematic.” | |
| Curability of disease | “If someone has a large mediastinal mass, nobody is going to be comfortable waiting.” |
| “To think they may have some syndromic cancer, like Lynch syndrome or a BRCA1 or 2 mutation, [patients] may not want to harvest their eggs or donate sperm. They say, well, there's a 50% chance that I'll transmit this, and I don't want to do that.” | |