
Abstract
Purpose:
Survival of children and adolescents and young adults (AYAs) treated for cancer has increased with improved treatments. However, there is still an increased risk of second primary cancer (SPC) in the long term compared with the same-age population, especially related to treatments. The follow-up of this population and the prevention of SPC are important issues. Therefore, this study aimed to review the available literature on cancer risk factors (lifestyle and occupational exposures) in children and AYAs previously treated for cancer in order to identify interventions that might be implemented to improve healthy behaviors in this population.
Methods:
PubMed was searched using the following terms: “cancer[Tiab] AND young adult[Tiab] or teen[Tiab] or childhood[Tiab] AND prevention[Tiab] AND survivors[Meshterm].”
Results:
Twenty-seven articles were included. Children and AYA survivors of cancer have similar risk behaviors to their peers regarding tobacco, diet, and sun exposure. However, they have lower physical activity. Few studies on prevention strategies in this population were identified. Results of available studies remain inconclusive. No publications were found on occupational exposure and risk of second cancer.
Conclusion:
Children and AYAs treated for cancer are a population at risk and require specific effective prevention strategies.
S
Female sex, older age at diagnosis, earlier treatment era, and radiation therapy were associated with increased risk of subsequent neoplasms. Differential exposure to cancer risk factors such as lifestyle (tobacco, diet, physical activity) may also be associated with increased risk of second malignancies, but this has been poorly studied in AYAs. To improve the prevention of second malignancies, the available literature was searched on cancer risk factors (lifestyle and occupational exposures) in children and AYAs previously treated for cancer. This study also reviewed the interventions that can be implemented to improve healthy behaviors in this population. The study focused on cancer risk factors known to be associated with the cancer types having shown an increased incidence in children and AYAs previously treated with cancer: smoking (lung cancer, breast cancer, colorectal cancer, leukemia) 6 ; diet, nutrition, and physical activity (colon cancer, rectal cancer, breast cancer, skin) 7 ; sun exposure (skin cancer); alcohol (breast cancer, colorectal cancer); and occupational exposures (lung cancer, leukemia, skin cancer, bone sarcomas, CNS tumors).8,9
Methods
PubMed was searched until June 2014, with no restriction on the earliest date of the publications, using the terms “cancer[Tiab] AND young adult[Tiab] or teen[Tiab] or childhood[Tiab] AND prevention[Tiab] AND survivors[Meshterm],” and limiting the search to articles in English and French. The search was completed using online data from the Public Health data bank, International Agency for Research on Cancer (IARC) website, and various websites (sanitary, occupational, and environmental agencies) and consensus conferences. The reference lists of related articles were also searched.
The articles (epidemiological studies, intervention studies, and literature reviews) were selected on their summary and further through the full article. Articles dealing with the risk of second malignancies associated with life style factors or occupational exposures as well as articles on cancer prevention strategies for the malignancies seen as second cancers after childhood and AYA cancer were selected. To take into account the substantial variability in the age ranges used by authors across studies and to facilitate the analyses of available publications, a predefined age range for this population was no applied. Articles dealing with second cancers related to genetic predisposition or psychosocial consequences of second malignancies, screening, and surveillance practices were not included. Articles dealing specifically with the risk of second malignancies associated with treatment of a first cancer were also excluded, as extensive reviews of the literature have been published previously on this topic.2,5
Results
Of the 105 articles identified by the search, 27 articles were included of which 14 dealt with behavioral risk factors and 13 with health promotion, including preventing risk factors for second cancers (see Fig. 1). Fifty-seven articles were excluded after reviewing the full publication because they did not match the eligibility criteria. Fifteen of the articles were unavailable through the authors' library or interlibrary services within the review time scope. Fifteen of the articles were excluded after full reviewing by two reviewers (J.C. and S.D.), who considering them to be outside the scope. Table 1 provides a detailed description of the main studies included in our search.
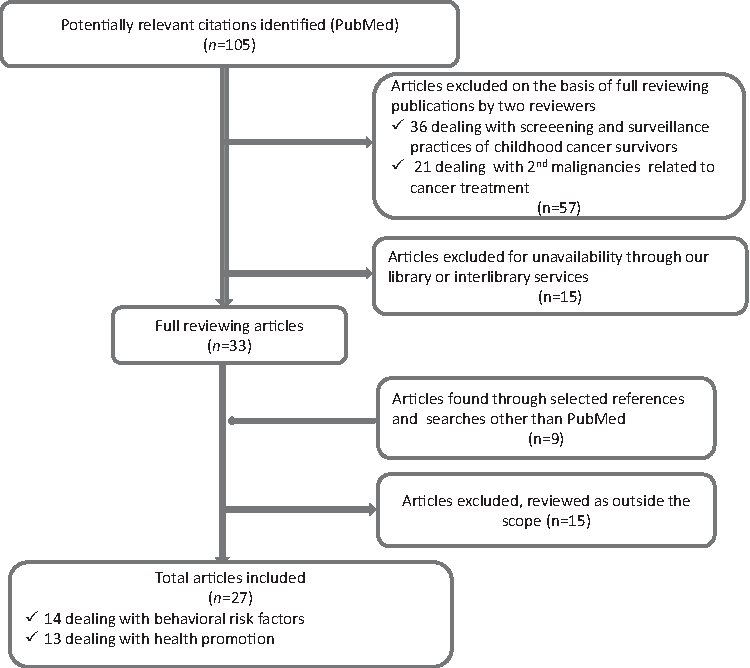
Flow diagram for the search.
The Childhood Cancer Survivor Study (CCSS) is a retrospective cohort study of 14,359 survivors of childhood cancer diagnosed prior to 21 years of age between January 1, 1970, and December 31, 1986, with a longitudinal follow-up of 5-year survivors of childhood cancer treated in 26 institutions in the United States and Canada. Eligible cancer diagnoses included leukemia, central nervous system malignancy, Hodgkin lymphoma, non-Hodgkin lymphoma, Wilms tumor, neuroblastoma, soft-tissue sarcoma, and bone tumors.
Body mass index (BMI) is a measure of body fat based on height and weight that applies to men and women.
AERs, absolute excess risks; ALL, acute lymphoblastic leukemia; CI, confidence interval; HR, hazard ratio; RR, relative risk; SIR, standardized incidence ratio.
Behavioral factors
Overall, 14 publications addressed lifestyle factors, such as smoking, cannabis use, alcohol consumption, sun exposure, physical activity, and nutrition. Four focused especially on AYAs previously treated for cancer.10–13 Three articles focused exclusively on smoking,14–16 and six on physical activity and nutrition.17–22 One publication dealt with sun exposure in AYAs who had previously been treated for cancer. 23
Tobacco
Overall, five studies focused on smoking in young cancer survivors.11,12,14–16 Smoking prevalence in survivors varied between 10% and 29%. Two studies found a significantly lower prevalence of smoking in survivors of AYA cancers compared with the general AYA population.11,12
Kahalley et al. studied factors associated with smoking in 307 adolescents from the CCSS. 14 In this study, the percentages of current smokers (10%) and past adolescent smokers (28%) were similar to those in the general population (9% and 33%, respectively). Factors associated with increased prevalence of recent smoking (having smoked in the week before the survey) were eating disorders (bulimia, anorexia), psychiatric problems (e.g., suicidal behavior), emotional distress, having friends who smoke, and having smokers in their household. Tyc et al. studied the factors associated with starting smoking in 94 preadolescents with cancer and in 190 preadolescents without cancer. 15 In this study, no preadolescents with cancer and only 0.5% of preadolescents without cancer reported current smoking (a non-significant difference). Preadolescents without cancer were more likely to report future intent to smoke compared with preadolescents with cancer (34.1% vs. 14%; p < 0.001). They were also more likely to have a close friend who smoked (16.8 vs. 7.5%, p = 0.03). Preadolescents with cancer had a better knowledge of the risks related to tobacco smoking in general (p = 0.001) and of their own specific risks (p < 0.001). They attributed more value to overall health (p = 0.001). Intent to smoke was significantly associated with age, sex (male being at greater risk), the absence of cancer, having parents or friends who smoke, and perceived vulnerability to tobacco-related illnesses. 15
Regarding cannabis smoking, an Australian study showed that cannabis use was significantly lower among the 153 adolescents treated for cancer than in the age-matched healthy population. 11
Tercyak et al. evaluated the prevalence of three behavioral risk factors (smoking, insufficient physical activity, and non-compliance with recommendations on sun exposure) in adolescents aged 11–22 years of age who had had childhood cancer. Regarding smoking, 50% of the participants smoked, whereas 53% declared not having any of these risk behaviors, 28% declared one of the three risk behaviors, 12% having two of the three risk behaviors, and 7% having all three (see Table 1). 13
Alcohol
Two studies showed significantly lower alcohol consumption among childhood or adolescent cancer survivors compared to the age-matched healthy population.11,12 Compared to their healthy peers, younger survivors (13 to 17-years) less frequently reported alcohol use (odds ratio [OR] = 0.44; 95% confidence interval [CI]: 0.39–0.49); whereas older adolescent survivors (18–24 years of age) more frequently reported alcohol use (OR = 1.5; 95% CI: 1.0–2.2; see Table 1). 11
Overweight, obesity
Seven studies investigated factors associated with unhealthy lifestyle, overweight, and obesity in people who had had cancer as children or AYAs. Three studies reported a relationship between obesity and cancer treatment.20,21,24 Children with acute lymphoblastic leukemia who received a dose of radiotherapy to the brain greater than 20 Gy before 4 years of age had a fourfold increased risk of obesity; this was especially true for women. 24 The risk of obesity in women treated for a brain tumor was higher if they were younger than 4 years old at diagnosis. 20 A review of the literature reported a low rate of physical activity, little motivation to undertake sports, and difficulties meeting nutritional recommendations among childhood cancer survivors. 18 However, the proportion was similar to the healthy age-matched population, with adolescents having a less healthy lifestyle in general (eating at fast-food outlets, decreased physical activity). 22
Sun exposure
Buchanan et al. studied sun exposure in 9298 survivors of childhood cancer, diagnosed prior to 21 years of age, from the CCSS cohort. Compared with the 2950 matched controls (who were siblings of the cases), cancer survivors exposed themselves significantly less to the sun, used significantly less artificial tanning devices, and had used more sunscreen the previous summer. 23
Results from Tercyak et al.'s study showed that 37% of the participants did not follow recommendations on sun exposure. Among the 28% of participants reporting only one risk behavior, non-compliance with recommendations on sun exposure was the most common (17%; see Table 1). 13
Determinants of behavioral risk factors
Overall, five studies investigated factors associated with increased prevalence of behavioral risk factors. Emmons et al. studied the factors associated with starting or quitting smoking in 9709 subjects from the CCSS. 16 Factors associated with a reduced likelihood of smoking were younger age at diagnosis (younger than 10 years old), history of brain radiotherapy, and pulmonary-related cancer treatment. Factors associated with an increased likelihood of smoking were lower education level (below bachelor level), lower annual income (<US$20,000), and not having black skin color. Furthermore, lower education level, male sex, lesser satisfaction with life, and stressful events were associated with excessive alcohol consumption in AYA cancer survivors. 12 Green et al. analyzed the factors associated with obesity in 9284 adults (older than 18 years of age) from the CCSS. Age at diagnosis (between 5 and 9 years old) and radiation dose to the hypothalamus and the pituitary (between 20 and 30 Gy) were significantly associated with obesity. Meeting US Center for Disease Control and Prevention guidelines on vigorous physical activity and a medium amount of cancer-related anxiety were significantly associated with a decreased risk of obesity. Use of paroxetine was significantly associated with an increased risk of obesity compared with other drugs (see Table 1). 17 Buchanan et al. found that factors associated with regular sunscreen use in the past summer in survivors of childhood cancer were female sex, having fair skin, having previously been screened for skin cancer, and being prone to sunburn (see Table 1). 23 Older age and stress were significantly associated with the presence of more than one risk behaviors (smoking, insufficient physical activity and non-compliance with recommendations on sun exposure) in Tercyak et al.'s study. 13
Occupational exposures
Charbotel et al. have recently reviewed occupational carcinogenic agents associated with rare tumors, including the most frequent tumors is children and AYAs. 9 However, the search did not find any study in the literature investigating the risk of relapse or the risk of second malignancies associated with occupational exposures.
Prevention strategies to reduce unhealthy behaviors in childhood and AYA cancer survivors
Five articles addressed the problem of prevention of second cancers associated with avoidable risk factors, such as smoking, obesity, and lack of physical activity in children and AYAs who had had cancer.14,15,17–19
Smoking cessation10,25–32
Several studies on smoking cessation were identified. Tyc et al. compared an educational program with follow-up telephone counseling on the risks associated with smoking to standard advice on smoking in 94 pre-adolescents and adolescents who had had cancer. Participants were 10–18 years of age, and mean time from diagnosis was 6.3 years. At 12 months, participants in the intervention group had better knowledge of tobacco, had better perception of their vulnerability, and were less likely to want to smoke (differences not statistically significant). 28
A case-control study of 21 young cancer survivors and 43 controls cancer survivors (age range 13–21 years) looked at the impact of a decision-making and risk-education intervention and showed a marginal significant reduction in smoking among smokers at 6 months after the intervention (see Table 1). 27
No studies on nicotine replacement therapy (NRT) in adolescents with cancer were identified. Recent updates of recommendations propose the use of long-lasting bupropion or NRT in healthy adolescents who have a high dependency on nicotine and who wish to quit smoking. 30 However, recommending their use in children or adolescents who have had cancer seems premature in the absence of safety and efficacy data in this population. 30 Bupropion is contraindicated in people with a history of CNS tumor due to an increased risk of seizures, thereby limiting its usefulness in adult oncology populations. 29
Smith et al. studied the benefit of NRT combined with individual or group behavioral counseling in healthy adolescents. 31 Fourteen percent had stopped smoking at week 8, but only 5% continued to be smoke free at 6 months. Moolchan et al. evaluated the efficacy of different NRTs combined with cognitive–behavioral group therapy. 32 The three groups included (1) active patch (21 mg), (2) active gum (2 and 4 mg), and (3) gum and placebo patch. The proportions of participants who achieved prolonged abstinence at 3 months were 17.6% in the active patch group, 6.5% in the gum group, and 2.5% in the placebo group. The difference was statistically significant between patch and placebo, but not between gum and placebo nor between patch and gum.
Killen et al. performed a randomized clinical trial in 211 healthy adolescent smokers comparing nicotine patch plus bupropion sustained release (150 mg/day) versus nicotine patch placebo. There was no significant difference between both groups, but a majority of adolescents in both groups reduced their consumption to a few cigarettes per day or less and maintained this reduction over time (26-week assessment). 26 The authors explained the lack of difference by a suboptimal dose of bupropion, usually given at 300 mg/day in adults.
Diet, weight, and physical activity
Stolley et al. reviewed the descriptive and intervention studies that included survivors of childhood cancers and a measurement of diet and physical activity. They highlighted that childhood cancer survivors engaged in health-promoting activities at rates comparable to the general population. Authors pointed that the dietary research in childhood cancer survivors is methodologically weak and that behavioral interventions have mostly targeted physical activity. 18
The clinical study of Robien et al. with adult survivors of childhood acute lymphoblastic leukemia (ALL) suggested that in general dietary intake was not consistent with dietary recommendations: 50% of the participants met minimal goals for fruit and vegetable intake, and 50% met minimal goals for dietary fat restrictions. Eighteen percent met recommendations for 30 minutes of physical activity 5 days/week. 19 In the multicentric retrospective cohort study from the CCSS, Green et al. showed that the risk of obesity was decreased among those who met the US Centers for Disease Control and Prevention guidelines for vigorous physical activity (relative risk [RR] = 0.90; 95%CI: 0.82–0.97; see Table 1). 17
Promoting health protective behaviors
In a behavioral health promotion study of 266 childhood cancer survivors aged 12–18 years of age from the St. Jude Children's Research Hospital, Hudson et al. assessed the impact of a multicomponent behavioral intervention on changing health knowledge, health perceptions (perceived susceptibility, perceived seriousness, perceived benefits, perceived barriers), and health behavior practices. In this study, more than half of the participants (52%) did not know that cancer treatments could be associated with a risk of second cancer; 48% of the participants considered this risk as the most concerning potential treatment sequelae (see Table 1). 33 Due to lack of knowledge about the long-term side effects of treatments and about the risk associated with some behaviors, AYAs may not adopt healthy behaviors. New internet technologies (“ehealth”) seem to be useful in promoting healthy behaviors in children and AYAs who have had cancer. 34
Discussion
The aim of this article was to review the available literature on cancer risk factors (lifestyle and occupational exposures) in children and AYAs previously treated for cancer. The article also reviews the interventions that can be implemented to improve healthy behaviors in this population.
It seems that the behavior of cancer survivors toward a healthy lifestyle is similar to that of the healthy population of the same age, particularly regarding tobacco smoking, diet, and to a lesser extent sun exposure. Although AYA cancer survivors seem to engage in less physical activity than their peers, these results are consistent with previous literature that reported a significantly higher prevalence of current smoking, obesity, and chronic conditions in this population compared with individuals who have no history of cancer. 35
Overall, there are few studies that investigate the risk factors associated with second malignancies, except for long-term side effects of cancer treatments, which are the most important risk factors. However, the increased incidence of second malignancies in this population, of all cancers and in particular of cancers not associated with primary treatment, suggests a potential role of and synergies with other cancer risk factors, such as lifestyle and occupational exposures. The role of the latter in the development of second malignancies remains widely unknown.
Smoking in children and AYA cancer survivors may increase the risk of lung cancer, breast cancer, colorectal cancer, and leukemia. 6 Smoking is one of the most preventable risk factors implicated in cancer development. While survivors of childhood cancer have similar smoking rates to their peers, the former seem to have a better knowledge of the health risks associated with smoking. Tobacco has not only a carcinogenic effect per se, but also enhances radiation effects. For example, smoking has been shown to increase the risk of radiotherapy-induced lung cancer in patients treated for Hodgkin disease. 34 While few studies have assessed the usefulness of smoking cessation programs in young cancer survivors, short-term results are quite disappointing, and there is no long-term evaluation.27,28 The use of NRTs in this population seems premature. 30 This means that it is important to improve our knowledge on the role of tobacco in the occurrence of second malignancies, to implement specific interventions to reduce tobacco consumption, and to prevent young people from starting smoking. 10 This may equally apply to the use of cannabis.
Alcohol consumption appears to contribute substantially to the worldwide cancer burden, although light-to-moderate alcohol consumption has been associated with some benefits related to heart disease, stroke, and diabetes (benefits that are reversed with occasional or regular heavy drinking), as highlighted by Cogliano et al. 36 Alcohol consumption is associated with an increased risk of second malignancy in adults treated for cancers of the upper aerodigestive tract. 37 Even if alcohol consumption seems lower in childhood or adolescent survivors of cancer compared with the healthy age-matched population,11,12 it may contribute to an increased risk of second malignancies. However, no study has specifically evaluated the impact of alcohol consumption on the risk of second malignancy in that population.
Obesity and lack of physical activity are known risk factors for cancers frequently found in childhood or adolescent cancer survivors, such as breast cancer, colorectal cancer, and lung cancer. 37 Furthermore, weight gain associated with cancer-related treatments (steroids or brain radiotherapy) can be amplified by an unhealthy diet and lack of physical activity. 38 However, no studies were found specifically investigating their impact on second malignancies in childhood and AYA cancer survivors. Yet, prevention programs focusing on diet and physical activity have shown long-term efficacy in young people without cancer. 39 It would be pertinent to study the impact of treatment-related weight gain and its active management on second malignancies.
The literature suggests greater proportions of childhood and AYA cancer survivors with appropriate behavior toward UV exposure. However, there is still progress to be made regarding the use of artificial tanning devices. Information on the risk of skin cancer associated with inappropriate sun exposure and artificial UV exposure should be given to these patients.23,40 Such information should also explain the importance of balancing natural sunlight exposure to avoid its damaging effects and meet sun protection guidelines with vitamin D requirements. The latter, produced by natural sun exposure, may have a protective effect against certain types of cancer. 41
Although AYAs are about to enter the workforce in most cases, there are no studies about the impact of occupational exposures on the risk of relapse of the first primary and on the risk of second malignancies. However, some of the tumors that occur in childhood cancer survivors (such as lung and respiratory subsequent primary neoplasms)5,8 are also known to be related to carcinogens present in the occupational environment. According to the periodical cross-sectional French medical survey on exposure to occupational risks (SUMER), young apprentices and young workers are the most exposed to carcinogens at work. 42 Therefore, as a precautionary measure, they should be advised to talk about their medical history with an occupational physician when thinking about their professional orientation. There are no jobs contraindicated in cancers survivors. However, applying a precautionary principle, specific attention should be paid in this population to avoid occupational exposure to carcinogens.
While the awareness of cancer risk among survivors of cancer in childhood and adolescence is higher than it is in the general population, a large proportion of the former seems unaware of their increased risk of second malignancies. 33 Various studies emphasize the need to implement specific prevention programs for this population to increase awareness, in particular with regard to the risks associated with certain lifestyle factors and to try to reduce them. 30
While there are no data on the timing of preventive information and interventions, patients request such information from their clinical team.15,43 International and national guidelines on prevention for this population, including screening guidelines, have been published. 44 It is important that this information be communicated and discussed several times throughout follow-up. General practitioners (GPs) have also a key role in providing these guidelines, as less than 20% of adults who have had a tumor in their childhood are followed in a specialized center or by an oncologist. 45 This percentage even decreases over time. Thus, GPs are in the front line to implement prevention and screening procedures and to detect second malignancies for which late diagnosis is a poor prognostic factor. 45 However, GPs often do not feel comfortable following up childhood and AYA cancer survivors, as they lack information on long-term side effects and appropriate follow-up schedules. 45
A recent workshop at the Institute of Medicine emphasized the importance of improving AYA cancer survivorship care based on “a systematic plan for screening, surveillance, and prevention that incorporates risks based on the previous cancer, cancer therapy, genetic predispositions, lifestyle behaviors, and comorbid health conditions should be developed for all AYA cancer survivors.” 46
It may be timely to develop and implement specific prevention approaches in this population, such as lifestyle intervention programs, and to evaluate their benefits, especially since many lifestyles risk behaviors cluster together. 47 The development of evidence-based programs such as those developed and tested by Emmons et al. to address substance abuse among AYA cancer survivors 46 should be encouraged to be widely implemented in other countries.
It seems relevant to study how to improve adherence of children and AYA cancer survivors to these prevention guidelines. Adolescents seem more receptive to messages given by people of their own age. Newer information and communication techniques (such as social networks, games, text messages, or smartphone applications) could be used to deliver the information and some of the interpersonal interactions required. As noted by Elliot et al., health promotion strategies in childhood ALL survivors relate to strategies similar to those applicable to improving healthy behaviors in the general population, and strategies using eHealth technologies are promising. 34 In a recent survey in 25 European countries on more than 25,000 children aged 9–16 years old, 93% surf the internet at least once a week and 60% every day or nearly. They spend at least 1.5 hours per day on the internet. Half of them say “they feel more themselves” in relationships on the net than face-to-face. Adolescents qualify the net as being the first source of information concerning health. 48 Therefore, this technology, with games or online quizzes, may be a good way to convey messages on prevention and healthy lifestyles (cannabis, drug abuse, sexuality, diet, physical activity, etc.).49,50 These tools may be also useful for social support and sharing experiences to reinforce motivation. They are also a great opportunity for new interdisciplinary public health approaches to prevention.
Conclusions and Perspectives
The risk of second malignancies after a childhood or AYA cancer is an important issue in this population and should be addressed in follow-up programs. Appropriate communication between oncologists and GPs is very important in this context. Patients (and their GPs) should have all the information on the course of the disease, the treatment received, the possible late side effects, the follow-up plan, and the screening plan. This plan should be adapted to the individual's risks and the evolution of risky exposures and behaviors.
The present review underscores the need to improve our knowledge on the impact of these behaviors (tobacco, alcohol, diet, and physical activity) on second malignancies and their interaction with the effects related to treatment.
It is important to implement specific prevention strategies in this population and to evaluate these interventions and the factors that could contribute to adhesion to health-promoting messages relying in particular on research on health-risk behaviors that are commonly initiated during pre-adolescence and adolescence and that have importance for adult risk of second primary cancers.
The conclusions of this review may evolve as new data become available.
Footnotes
Acknowledgments
Thanks to Nicole Falette, PhD, Aude-Marie Foucaut, PhD, and Aurélie Danjou, PhD student, for their participation in the review of the manuscript. The research leading to these results has received funding from the European Union's Seventh Framework Programme for research, technological development and demonstration under grant agreement no. HEALTH-F2-2011-261474.
Author Disclosure Statement
No competing financial interests exist.