
Abstract
Purpose:
Childhood cancer survivors (CCS) are at increased risk of metabolic dysfunction as a late effect of cancer treatment. However, pediatric metabolic syndrome (MetS) lacks a unified definition, limiting the diagnosis of MetS in CCS. This study evaluated individual metabolic health risk factors and potential areas for intervention in this at-risk population.
Methods:
This single center, retrospective observational longitudinal study evaluated the metabolic health of all CCS attending an oncology long-term follow-up clinic at a university hospital in Sydney, Australia (January 2012–August 2014). Participants were 276 CCS (52.2% male; mean age 18.0 years; range 6.8–37.9 years), at least 5 years disease free with a broad spectrum of oncological diagnoses. Primary metabolic health risk factors included raised body mass index, hypertension, and hypertransaminasemia. Participants treated with cranial radiotherapy (n = 47; 17.0% of cohort) had additional biochemical variables analyzed: fasting glucose/insulin, HDL/LDL cholesterol, and triglycerides.
Results:
Hypertension was common (19.0%), with male sex (p < 0.01) and being aged 18 years or above (p < 0.01) identified as risk factors. Cranial irradiation was a risk factor for overweight/obesity (47.8% in cranial radiotherapy-treated participants vs. 30.4%; p = 0.02). Hypertransaminasemia was more prevalent among participants treated with radiotherapy (15.6% vs. 7.3%; p = 0.03), and overweight/obese participants (17.6% vs. 8.2%; p = 0.04).
Conclusion:
Metabolic health risk factors comprising MetS are common in CCS, placing this population at risk of premature adverse cardiovascular consequences. Proactive surveillance and targeted interventions are required to minimize these metabolic complications, and a unified definition for pediatric MetS would improve identification and monitoring.
A
Metabolic syndrome (MetS) is a cluster of clinical and biochemical risk factors indicating metabolic dysfunction, which are associated with the development of cardiovascular disease and T2DM. 6 In adults, numerous definitions have been proposed, which include the following parameters: central obesity, dyslipidemia, hypertension, and insulin resistance (IR).6,7 Non-alcoholic fatty liver disease (NAFLD) is postulated as the hepatic expression of MetS and often occurs concomitantly.8,9 Furthermore, components of MetS, notably IR and obesity, are independently associated with increased cancer risk (e.g., breast, esophageal, colon).9–11 In children and adolescents, no unified MetS definition exists, causing inconsistent prevalence data. 10 However, the International Diabetes Federation (IDF) MetS definition, validated for children older than 10 years of age, is widely used: central obesity plus two of hypertension, elevated triglycerides, low high-density lipoprotein cholesterol (HDL-C), and high fasting plasma glucose. 12
Many CCS develop MetS, and a recent review of CCS with acute lymphoblastic leukemia (ALL) revealed that 12–39% had MetS, albeit with inconsistent definitions used. 13 Multiple chemotherapy and radiotherapy agents are known to affect metabolic parameters adversely.14,15 Chemotherapy can impair glucose and lipid metabolism, hormonal pathways, and pro-inflammatory cytokines/adipokines, increasing the risk of endothelial dysfunction, IR, adipose deposition, and weight gain.14,16 Local irradiation can damage pancreatic beta cells, and is associated with a significantly increased risk of diabetes mellitus.17,18 Cranial radiotherapy (CRT) is particularly deleterious to metabolic health via hypothalamic–pituitary axis damage and subsequent endocrine disorders associated with metabolic dysfunction. 19 Furthermore, multi-agent protocols combining chemotherapy and radiotherapy are associated with a higher risk of MetS than single modality regimens.13,20
Obesity is common in CCS, and its etiology is multifactorial.4,21 Cranial and total body irradiation (TBI), chemotherapy, and surgery are all identified risk factors predominantly via hormonal pathway dysregulation. 18 Growth hormone (GH) deficiency secondary to CRT is particularly associated with increased fat mass, decreased lean body mass, IR, and T2DM.14,22 Hypertension is also more prevalent in CCS than in population rates, and a recent study reported a 2.43 increased relative risk for ALL survivors. 4 Although mechanisms leading to hypertension are multifactorial, renal causes are common and often secondary to nephrotoxic chemotherapy, radiotherapy, nephrectomy, and supportive care agents (aminoglycosides, cyclosporin A). 23 Both chemotherapy and radiotherapy can impair insulin sensitivity, and higher fasting glucose and insulin concentrations are reported in CCS compared with age-matched controls. 24 Dyslipidemia in CCS can be secondary to chemotherapy, TBI, or treatment-associated obesity and hormonal deficiencies.25–27 TBI is also associated with NAFLD, and liver irradiation is independently associated with hypertransaminasemia. 25
CCS are at increased risk of MetS components. However, a unified definition of pediatric MetS is still lacking. Therefore, the aim of this longitudinal study was to determine the prevalence of individual metabolic health risk factors in a large cohort of CCS with a broad spectrum of oncological diagnoses.
Methods
Subjects and study design
This was a single center, retrospective observational longitudinal study, which evaluated CCS attending the Long-Term Follow-Up Clinic (LTFUC) at a pediatric university hospital in Australia. To attend the LTFUC, participants must be disease free for 5 years.
Data were extracted from a dedicated database of all participants attending the clinic between January 1, 2012, and August 15, 2014 (n = 276). Database information was coded by clinicians, and was input by a research assistant (baseline demographics, primary diagnosis/treatment protocol, height/weight/blood pressure [BP], investigations and results, medications and endocrine, renal or cardiac late effects). Six participants attended twice during this period, but data were only extracted from the first clinic visit.
Data collection
Setting
Department of Oncology, The Children's Hospital at Westmead, Sydney, Australia.
Demographics
Date of birth, age at diagnosis/LTFUC, sex, primary cancer diagnosis, treatment protocol.
Clinical data
Height/weight, BP, smoking history, medications. Height/weight were measured using standard anthropometric techniques, with light clothing and shoes removed. Overweight/obesity in adults was defined by World Health Organization guidelines (overweight = body mass index [BMI] ≥25.0, obesity = BMI ≥30.0). 28 For participants younger than 18 years of age, age-/sex-specific International Obesity Task Force BMI tables were used. 29 Blood pressure was measured using the Dynamap® automated system. Elevated readings were repeated after 10 minutes. For participants younger than 18 years of age, elevated BP (hypertension) was defined by the National High Blood Pressure Education Program guidelines (≥95th percentile, age/height/sex specific). 30 In adults, hypertension was defined as a systolic BP ≥130 mmHg and/or diastolic BP ≥85 mmHg, or taking medication for previously diagnosed hypertension. 31
Biochemical data
Fasting blood specimens collected within six months (before/after) LTFUC were included. Participants were instructed to fast prior to specimen collection. Specimens were considered fasting if collected before 11am or documented as fasting. Other specimens were excluded from further analyses. Eighty-eight percent of specimens were analyzed at the institution's clinical diagnostic laboratories. Remaining analyses were performed in other nationally accredited diagnostic laboratories, as participants came from statewide locations. Routinely measured metabolic biochemical parameters were hepatic transaminases (aspartate aminotransferase [AST], alanine transaminase [ALT]).
Cranial radiotherapy subset
Participants treated with CRT and participants with specific clinical indications also had the following parameters measured: glucose/insulin, lipid profiles (total/HDL/LDL-cholesterol, triglycerides), and homeostasis model assessment of IR (HOMA-IR) calculated, where HOMA-IR = fasting plasma glucose (mmol/L) × fasting plasma insulin (mIU/L)/22.5. Results were considered abnormal if outside age-/sex-appropriate laboratory reference ranges. For HDL-C reference ranges, the IDF MetS definition (≥18 years) or American Academy of Pediatrics reference (<18 years) were used.1,32
Metabolic health status
All participants had BMI, BP, and hepatic transaminases measured as primary indicators of metabolic health. Waist circumference was not measured. Thus, the variables collected did not allow a definition of MetS consistent with the IDF definition. 12 Therefore, participants' individual metabolic health risk factors were identified. In all participants, these included: (1) overweight/obesity, (2) hypertension or current antihypertensive mediation use, and (3) hypertransaminasemia (AST and/or ALT). In those treated with CRT, additional risk factors were dyslipidemia and IR/impaired glucose tolerance.
Smoking and cardiac function
Smoking history was elicited as a key determinant of metabolic health. Echocardiograms were performed (every 1–5 years) in participants treated with anthracyclines due to cardiomyopathy risk. 33 Echocardiograms performed within 18 months of the extracted LTFUC were accepted for analysis. Echocardiograms were performed at numerous sites, as participants came from statewide locations. Extracted variables were left ventricle diastolic dimension (LVDD), left ventricle systolic dimension (LVSD), and left ventricle fractional shortening (FS). If reference ranges were not provided, American Society of Echocardiography guidelines were used for adults. 34 For children, reference ranges were based on a European pediatric database. 35 FS was calculated (if not provided) as: FS = (LVDD − LVSD/LVDD) ×100. If FS was not available, the left ventricle ejection fraction was used as a measure of reduced systolic function.
Statistics
Data were transferred into Excel, and analyzed using SPSS Statistics for Windows v22.0 (IBM Corp., Armonk, NY). Overall relationships were assessed between predictor and outcomes variables (metabolic health risk factors) using multivariate logistic regression models. Binary logistic regression models, Pearson's chi square test, and Student's t-test were further employed to assess specific outcome variables. p-Values were considered significant at 5% (p < 0.05).
Ethics
Ethical approval was granted by The Sydney Children's Hospital Network Human Research Ethics Committee (LNR/14/SCHN/263).
Results
Demographics
Participants were 276 CCS (52.2% male; n = 144). For the majority of participants (64.9%), this was their first or second LTFUC appointment (range 1st–10th). Mean age at primary cancer diagnosis was 5.4 years (range 0.0–17.3 years), and mean age at the extracted LTFUC appointment was 18.0 years (range 6.8–37.9 years). There was no significant difference in age between sexes at diagnosis (p = 0.95) or LTFUC appointment (p = 0.88). More than half of the participants (n = 150; 54.3%) were younger than 18 years of age at LTFU. The distribution of primary diagnoses is shown in Figure 1. Leukemia was the most prevalent (n = 115; 41.7%), followed by lymphoma (n = 37; 13.4%) and sarcoma (n = 36; 13.0%).

Primary diagnosis in a childhood cancer survivor cohort. *“Other” cancers included retinoblastoma (n = 7), hepatoblastoma (n = 5), Langerhans cell histiocytosis (n = 5), nasopharyngeal carcinoma (n = 1), and pleuropulmonary blastoma (n = 1).
Treatment modalities are summarized in Table 1. Almost all participants were treated with chemotherapy (98.6%), more than a third received radiotherapy (39.5%), and more than half of these were CRT or TBI.
Clinical data
Smoking
Of 93% participants (n = 257) with documentation regarding smoking habits, 6.2% self-reported being smokers (n = 16; 10 males), five of whom were younger than 18 years of age.
Overweight and obesity
Of 270 participants (97.8%) with height/weight data available, 89 (32.2%) were overweight/obese. Tables 2 and 3 show the distribution of BMI by age and sex. Rates of overweight/obesity were significantly higher in those aged 18 years or older (n = 53; 43.8%) compared with those younger than 18 years of age (n = 36; 24.2%; p < 0.01). Prevalence of overweight/obesity was comparable between sexes among those younger than 18 years old (males 22.1%; females 26.4%; p = 0.54). However, rates of overweight/obesity were significantly higher in males 18 years old or older (males 52.3%; females 33.9%; p = 0.04) and among participants treated with CRT (47.8% vs. 30.4%; p = 0.02).
Defined using age/sex specific International Obesity Task Force BMI tables, which calculate childhood BMI to correspond to predicted BMI cutoffs at 18 years. 29
BMI = body mass index.
Blood pressure
Blood pressure was recorded for 97.4% participants (n = 269), of whom 19.0% (n = 51) had hypertension (70.6% male, 66.7% ≥ 18 years of age, 51.0% overweight/obese). Two participants with hypertension were taking antihypertensive medication (3.9%). Factors associated with a significant risk of hypertension were male sex (p < 0.01), older age (hypertension prevalence in participants <18 years 11.3% vs. 28.7% in those ≥18 years old; p < 0.01) and overweight/obesity (p = 0.045). Radiotherapy exposure was associated with an increased prevalence of hypertension, which was not significant (24.8% vs. 14.7%; p = 0.20). Of the 11 participants younger than 18 years old with hypertension, four were overweight/obese, one had a single kidney, and two had had a partial nephrectomy.
Biochemical data
Hepatic transaminases
Hepatic transaminases were available for 96.7% (n = 267) of participants of whom 10.9% (n = 29) had hypertransaminasemia. Prevalence was higher in participants treated with non-cranial radiotherapy (15.6% vs. 7.3%; p = 0.03) and the overweight/obese (17.6% vs. 8.2%; p = 0.04).
Lipid profiles
Lipid profiles were available for 26.1% of participants (n = 72), which included profiles for 97.8% (n = 46) of participants treated with CRT. Biochemical dyslipidemia was identified in 50.0% (n = 36); 19 had elevated LDL-C, 21 low HDL-C, and 13 elevated triglycerides. Four participants were taking statins for hypercholesterolemia.
Glucose metabolism
Glucose/insulin profiles were available for 22.5% of participants (n = 62), which included 97.8% (n = 46) of participants treated with CRT. Twenty participants (30.8%) had a HOMA-IR >3, indicating IR. Six participants had previously diagnosed diabetes mellitus (type 1: n = 1; type 2: n = 5), and one participant had IR and impaired glucose tolerance. Six participants were treated with a single hypoglycemic agent (metformin: n = 4; gliclazide: n = 1; insulin: n = 1), and one was treated with gliclazide and combined metformin/sitagliptin.
Metabolic health status
Almost all participants (n = 257; 93.1%; 53.5% male) had BMI, BP, and hepatic transaminases measured as primary indicators of metabolic health. Of these, 33.1% (n = 85) had one metabolic risk factor (hypertension, increased BMI, raised hepatic transaminases). Two risk factors were identified in 12.5% (n = 32), and 2.7% (n = 7) had three identified risk factors. All participants with three risk factors were males who were older than 18 years of age. The number of participants with two or more risk factors was significantly higher in males (19.7% vs. 10.0%; p = 0.03) and among participants treated with CRT (26.1% vs. 13.0%; p = 0.04). For participants treated with CRT, when dyslipidemia and IR/impaired glucose tolerance were included for analysis, more than 80% had at least one identified risk factor, and 43.5% had two or more risk factors (Fig. 2).
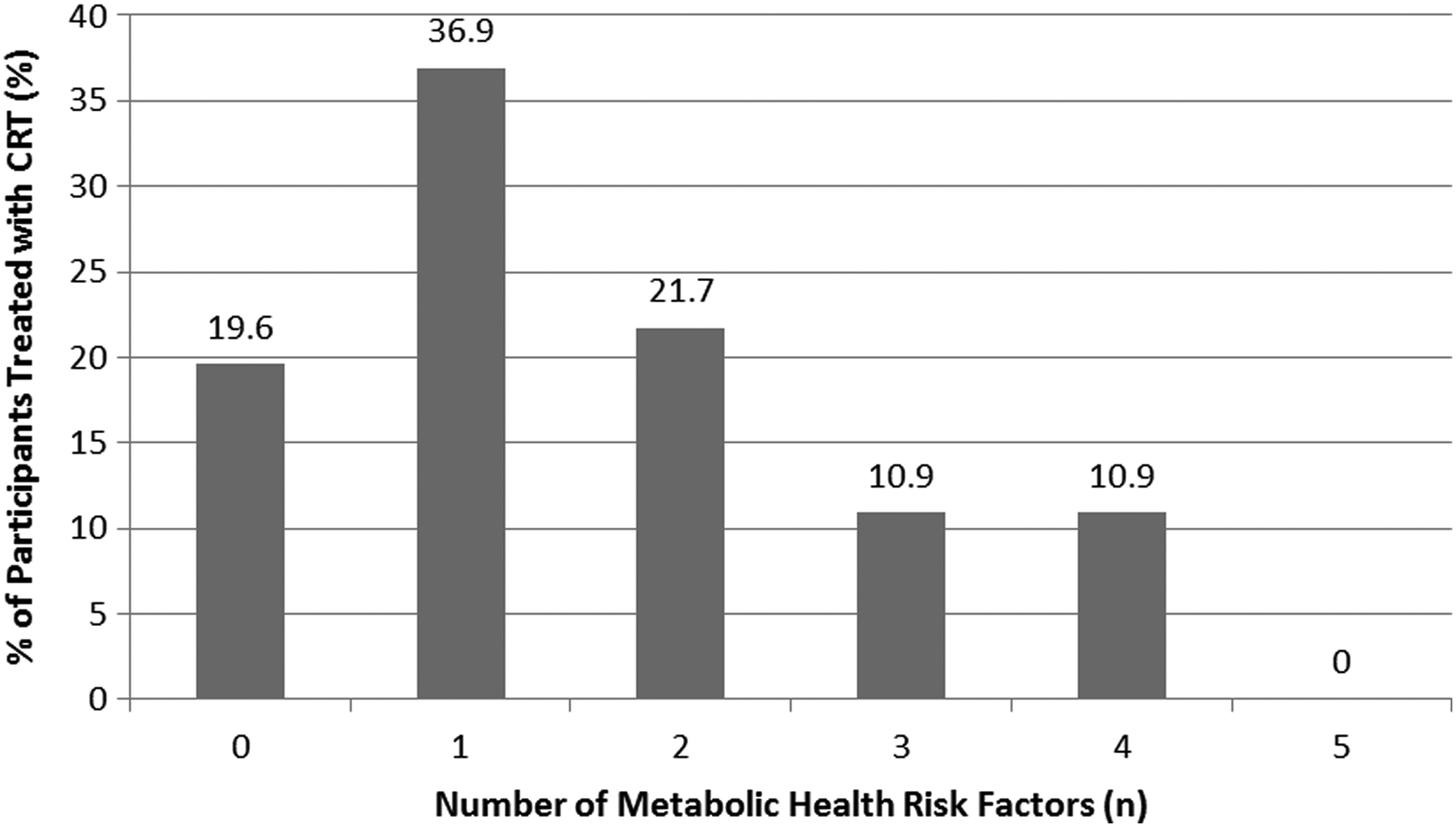
Number of metabolic health risk factors in participants treated with cranial radiotherapy (CRT).
Cardiac function
Among the 239 participants requiring echocardiographic surveillance, 189 had echocardiograms performed within 18 months of the LTFUC. Of these, 19.0% (n = 36) had an increased LVDD, and 4.8% (n = 9) had depressed systolic function, or were on treatment for previously diagnosed decreased systolic function.
Discussion
Metabolic health risk factors comprising MetS are common in CCS. As childhood cancer survival rates continue to improve, the premature development of adverse cardiovascular consequences will inevitably increase. The subsequent shift away from cancer recurrence as the major cause of morbidity and mortality in CCS has significant implications.36,37 As such, optimizing interventions to prevent, stabilize, or mitigate these metabolic complications is paramount. 2 Principal modifiable metabolic risk factors are smoking, overweight/obesity, and hypertension. Due to the high risk of secondary malignancy and cardiometabolic disease in CCS, smoking is strongly discouraged, consistent with low reported smoking rates in this study: 6.2% in comparison to national rates (16% for those aged 18–24 years). 38
Overweight/obesity rates were comparable to national data in participants younger than 18 years old (24.2% in cohort vs. 20.9–31.3% for those aged 5–17 years old) and participants aged 18 years of age or older (43.8% vs. 46.0% for those aged 18–34 years). 39 However, total overweight/obesity rates rose significantly among CRT-treated participants (47.8% vs. 30.4%), consistent with other studies. 4 Cranial irradiation doses ≥20 Gy are associated with a significantly increased risk of obesity via damage to hypothalamic centers regulating hunger, satiety, energy expenditure, and leptin pathways.13,40 Females and children younger than 5 years of age are at greater risk.18,41 GH is particularly sensitive to CRT, and isolated deficiency occurs at lower doses (18–24 Gy) compared with other hormonal deficiencies (>30 Gy).14,42,43 Sex hormone deficiencies secondary to central or gonadal damage also promote obesity, and high-dose corticosteroids are obesogenic by increasing energy intake and decreasing lean body mass.14,44 Radiotherapy and chemotherapy additionally induce muscle and nerve injury causing physical inactivity. 45 While not routinely performed in this study, waist circumference in addition to BMI should be measured in CCS as a superior indicator of central obesity and predictor of cardiometabolic risk. 46
Hypertension imparts a significant disease burden in CCS, as almost one-fifth treated with nephrotoxic therapies develop (secondary) hypertension. 47 In this study, hypertension rates were significantly higher than population rates; for participants younger than 18 years of age, 11.3% had hypertension versus childhood population rates of 3.6% (3–18 years; p < 0.01). For participants 18 years of age or older, 28.7% had hypertension compared with national data (7.5% for 18–34 years; p < 0.01).39,48 Hypertension risk is compounded by increasing obesity rates and associated primary hypertension.49,50 Physicians are often reluctant to initiate antihypertensive medication in young people, as typified by low prescribing rates (3.9%) in this study. Given the interplay of metabolic risks in CCS, prompt pharmacological intervention is recommended. 20
NAFLD is the most common cause of chronic liver disease.8,9 Hypertransaminasemia is the most frequently associated biochemical abnormality, which in this study was more prevalent in overweight/obese participants. 51 Notably, normal transaminases or BMI do not exclude NAFLD, as demonstrated in a study of bone marrow transplant recipients, which diagnosed NAFLD by liver ultrasound in 37% of males and 48% of females.51,52 As such, abdominal ultrasound should be considered in addition to routine hepatic transaminases and lipid profiles for NAFLD surveillance.
Cardiomyopathy, while not a metabolic risk factor, further increases adverse cardiovascular event risk. 18 Although no significant association was demonstrated between anthracycline exposure and echocardiogram abnormalities, this may reflect that the time needed for echocardiogram abnormalities to appear is greater than that allowed by the study follow-up period.3,53
The lack of a unified childhood MetS definition impairs the ability to compare metabolic health data across studies. Limitations to a unified definition include variability in insulin sensitivity, body composition and BP during pubertal growth and development, and a paucity of long-term outcome data. 10 Furthermore, parameters indicating metabolic dysfunction in adults, such as BP and lipid profiles, are often initially normal in young people, albeit travelling along higher percentiles. 10
Study strengths include the utilization of a detailed clinical database with data collected from biomarker analysis, imaging, and face-to-face consultation. Due to the retrospective nature of this study, data on glucose/insulin/lipid profiles were primarily only available for participants treated with CRT (17.0%), and waist circumference was not measured. Limitations meant complete indicators of metabolic health could not be reviewed in all participants or data could not be analyzed in accordance with the IDF MetS definition. 12 Future studies should include prospectively collected data encompassing all IDF MetS parameters.
Conclusion
Premature cardiovascular disease will cause significant disease burden in CCS. Future studies should seek to understand better the characteristics that predispose CCS to adverse metabolic health consequences. An internationally accepted definition for pediatric MetS may rationalize metabolic health risk factor identification and promote early intervention in this at-risk population.
Footnotes
Acknowledgments
The assistance of staff of the Academic Department of Adolescent Medicine, the Long-Term Follow-Up Clinic, Department of Oncology, and the Institute of Endocrinology & Diabetes at The Children's Hospital at Westmead is gratefully acknowledged. Dr. Liz Barnes from the Kid's Research Institute at The Children's Hospital at Westmead provided statistical support. Human resources were provided by Linköping University, Sweden.
Author Disclosure Statement
No competing financial interests exist.