
Abstract
Purpose:
The adolescent and young adult (AYA) population is a growing group of survivors, exceeding more than 600,000, at high risk for late effects of cancer-directed therapy. While many guidelines exist for cancer survivorship care, choosing which to use for an AYA cancer survivor is challenging, yet vital, to ensure comprehensive follow-up care.
Methods:
Survivorship care plans (SCPs), including treatment summaries (TS) and follow-up care plans, were created for three clinical vignettes (acute lymphoblastic leukemia, osteosarcoma, and Hodgkin lymphoma). Four sets of guidelines were used, including the Children's Oncology Group Long-Term Follow-Up Guidelines (COG LTFU), National Comprehensive Cancer Network (NCCN) Guidelines for Age- Related Recommendations: AYA Oncology (NCCN-AYA), NCCN Guidelines for Treatment of Cancer by Site (NCCN-Site), and NCCN Guidelines for Supportive Care: Survivorship (NCCN-Survivorship) and NCCN supplemental cancer screening guidelines. The follow-up care plans were compared across guidelines to determine the extent and nature of the similarities and differences concerning AYA cancer survivorship care.
Results:
The guidelines disagree on the link between treatment exposures and late effects, the population to be screened, the screening test to be used, and the time interval of testing. Specific examples of this include screening for cardiac toxicity, breast cancer, and neurocognitive deficits.
Conclusions:
While many guidelines exist for AYA survivorship care, there is discordance among the recommendations. This has significant implications for the long-term follow-up care of an AYA survivor. This study offers solutions to harmonize guidelines in order to ensure comprehensive quality survivorship care for this population.
T
The importance of improved survivorship care has been highlighted both nationally and internationally. The 2006 Institute of Medicine (IOM) Report, “From Cancer Patient to Cancer Survivor: Lost in Transition,” calls for increased surveillance and prevention of late effects, as well as improved intervention and coordination of care. 3 The recent American College of Surgeon's Commission on Cancer (CoC) standard on survivorship care planning responded to these requests. 9 In order to receive CoC accreditation, cancer programs must offer patients survivorship care plans (SCPs) that adhere to the standards laid out by the IOM. While the original standard called for implementation by 2015, the revised standard calls for a phase-in approach by 2019. In order to develop such care plans, however, clinicians need access to a harmonized set of evidence-based guidelines. In 2010, the International Late Effects of Childhood Cancer Guideline Harmonization Group was created, and it issued a report declaring the need to harmonize existing, multiple, survivorship guidelines.10–12
Providing survivorship care to the AYA population is challenging. First, confusion exists on who should follow this patient after completion of therapy. Second, there is uncertainty on how an AYA survivor should be followed for surveillance of late effects, that is, according to which available guidelines, as more than one exists for this population.
While AYAs may have received their primary cancer care in the pediatric setting, their follow-up care, as they age into the realm of adult providers, is uncertain. Do patients remain with their pediatric oncologist for life, or transition eventually to an adult primary care provider (PCP), adult oncologist, or survivorship oncologist? Increasing evidence shows no difference in outcome of follow-up care between oncologists and PCPs,13–16 but there is evidence that PCPs are not often involved in follow-up care. 17 PCPs also report that they prefer to follow survivors in conjunction with an oncologist. 18 However, for the AYA survivor, it is often unclear as to which oncologist would provide this care once the patient is off therapy for many years.
Many providers indicate that access to surveillance guidelines and SCPs are of high importance in providing care.18,19 Similarly, both the National Cancer Policy Board of the IOM and American Society of Clinical Oncology (ASCO) endorse the development and use of evidence-based surveillance guidelines.1,3,20 Published surveillance guidelines have shown some utility in areas of costs and benefits to patient care,21–23 but there are issues of consistency in guideline application. Multiple studies, in which a clinician was provided a clinical vignette on Hodgkin lymphoma to test adherence to Children's Oncology Group (COG) recommendations, have highlighted such issues.18,19,24,25 For example, in the 2009 study by Henderson et al., 34% of pediatric oncologists did not adhere to breast cancer screening guidelines, 43% did not adhere to cardiac screening, and 24% did not adhere to thyroid screening. 24 Similarly, in 2014, Suh et al. found that 90.6% of adult internists did not adhere to breast cancer screening, 85.1% did not adhere to cardiac screening, and 23.6% did not adhere to thyroid screening. 18 The development of SCPs for AYAs is further complicated because among cancer-specific guidelines, there is wide variation in recommendations.
The aim of this paper was to explore how an AYA survivor would be followed for late effect surveillance based on the currently available guidelines. Table 1 shows the four distinct guidelines referencing the AYA age group. A flow diagram (Fig. 1) illustrates how the guidelines referenced one another. This study uses each set of guidelines to develop a SCP for three case vignettes. By directly comparing guideline recommendations, the investigation points to issues in guideline application and consensus for long-term follow-up care for AYA cancer survivors.
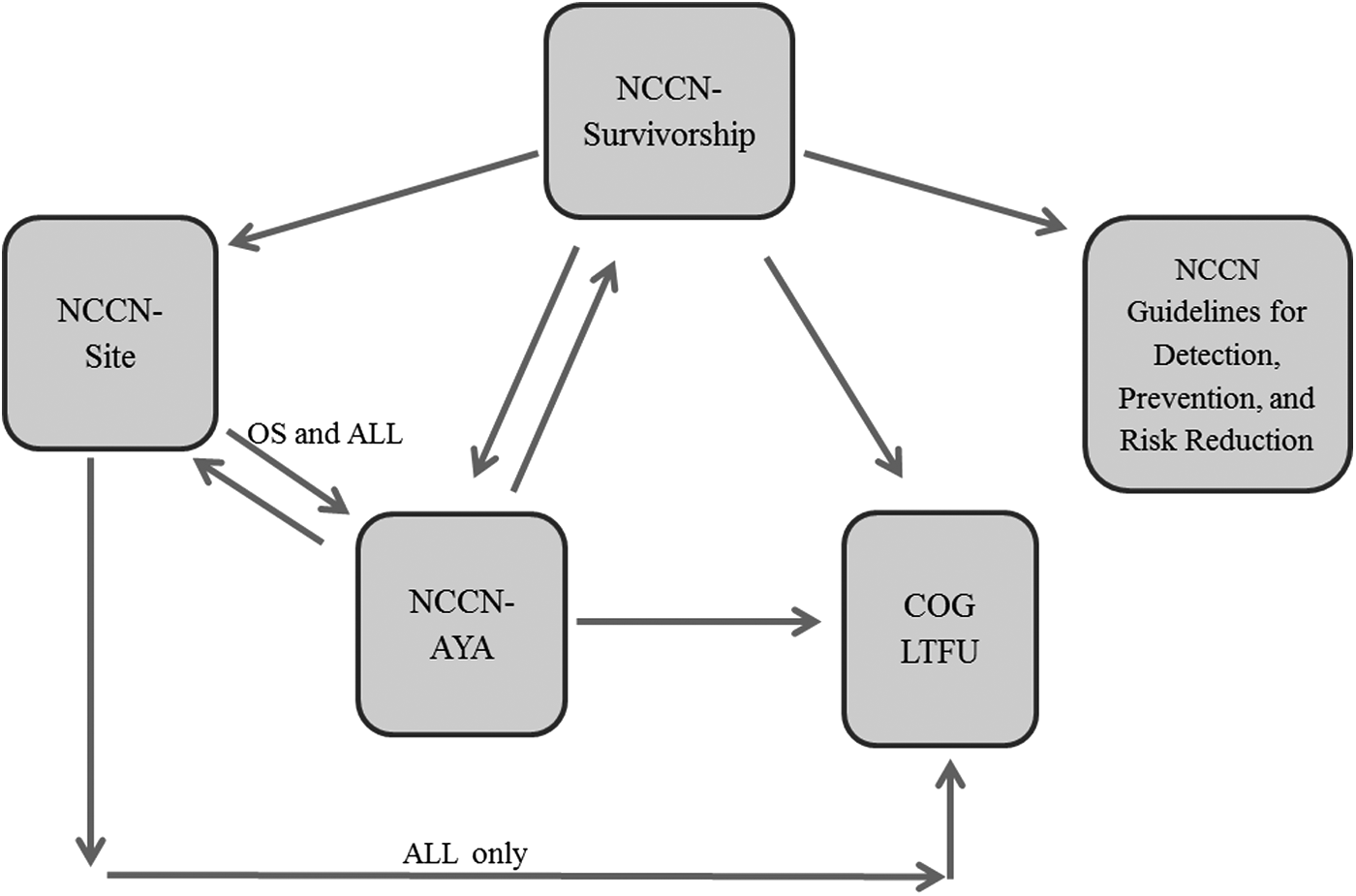
Flowchart of document references. The Children's Oncology Group Long-Term Follow-Up Guidelines (COG LTFU) do not reference the National Comprehensive Cancer Network (NCCN) guidelines. The NCCN-Survivorship guidelines reference all other guidelines (NCCN and COG LTFU). The NCCN-AYA guidelines reference the COG LTFU guidelines and NCCN-Site and NCCN-Survivorship, but not NCCN Guidelines for Detection, Prevention, and Risk Reduction. The NCCN-Site acute lymphoblastic leukemia guidelines reference the NCCN-AYA and COG LTFU guidelines. The NCCN-Site osteosarcoma guidelines reference the NCCN-AYA guidelines only. The NCCN-Site Hodgkin lymphoma guidelines do not reference other guidelines.
LTFU, Long-Term Follow-Up Guidelines.
Methods
Vignettes
Three case vignettes were created of cancers common in the AYA age group: osteosarcoma (OS), acute lymphoblastic leukemia (ALL), and Hodgkin lymphoma (HL). These cases were adapted from patients previously treated by the authors. Information provided in the vignettes modeled information that would be available on the patient's treatment summary and clinical notes. The cumulative chemotherapeutic and radiation doses were derived from current COG and National Comprehensive Cancer Network (NCCN) protocols.25–30 The complete vignettes are shown in Figure 2.

Three case vignettes: osteosarcoma (OS), acute lymphoblastic leukemia (ALL), and Hodgkin lymphoma (HL).
For each vignette, a SCP, including a treatment summary and follow-up care chart, was created. The treatment summary was generated using only information given in the vignette, with the assumption no follow-up care had been previously performed. The four guidelines were then referenced to create follow-up care charts. This chart, divided by organ system, includes indicated screening tests and their respective time intervals. Recommendations for targeted history questions and specific physical examinations were summarized in the “wellness” category by indicating the need for a yearly history and physical. A literal interpretation of the guidelines to generate the tables was applied in order to simulate how any type of clinician would assess these recommendations. However, it is recognized that clinical judgment is an important part of generating care plans for cancer survivors.
Review of guideline evidence level
Each guideline was also reviewed for the level of evidence used to create each guideline's recommendations. The COG Long-Term Follow-Up Guidelines (LTFU) were scored by a multidisciplinary panel using a modified version of the NCCN categories. 25 Category 1 was defined as “high-level of evidence” derived from high-quality case control or cohort studies. Category 2A and category 2B were defined as “lower-level evidence” derived from non-analytic studies, case reports, case series, and clinical experience. A minimum of a Category 2B score was required for all recommendations in the COG LTFU guidelines. The three NCCN guidelines define their categories by both evidence and consensus that the intervention is appropriate.26–32 Category 1 was based upon high-level evidence with a uniform NCCN consensus of appropriateness. Category 2A was based upon lower-level evidence with a uniform NCCN consensus of appropriateness. Category 2B was based upon lower-level evidence with non-uniform NCCN consensus. Category 3 was based upon any level of evidence with major NCCN disagreement concerning the intervention. The NCCN guidelines state that all recommendations are category 2A unless otherwise noted.
Results
The follow-up care charts are shown in Tables 2–4 for the three vignettes (Table 2 OS, Table 3 ALL, and Table 4 HL). The charts combine all recommended screening tests and frequencies from the COG LTFU, (NCCN) Guidelines for Age- Related Recommendations: AYA Oncology (NCCN-AYA), NCCN Guidelines for Treatment of Cancer by Site (NCCN-Site), and NCCN Guidelines for Supportive Care: Survivorship (NCCN-Survivorship)/NCCN Guidelines for Detection, Prevention, and Risk Reduction (NCCN-DPRR).
Highlighted examples of discordance
As seen in Tables 2–4, the documents disagree on the recommendations for late effect surveillance. Three illustrative examples of discordance are presented. Other discordances noted in terms of late effects, the population to be screened, the screening test to be used, and the time interval of the test were observed. For example, the COG guidelines include screening for reduced bone mineral density, dental abnormalities, and cataracts. Yet, the NCCN guidelines do not include screening for these late effects.
Screening for cardiac toxicity
Treatment with anthracyclines and radiation increases the patient's risk for cardiac toxicity. 33 Echocardiogram is frequently the screening modality of choice. 34 The COG LTFU guidelines recommend an echocardiogram and electrocardiogram (EKG) at baseline upon entry into the long-term follow-up clinic. Subsequent echocardiograms are based on dose of anthracycline and whether radiation was received. 25 The NCCN-AYA guidelines recommend an echocardiogram every 1–2 years based on anthracycline dose. 27 However, further information on how to calculate the interval based on a dose is not included. The NCCN-Site HL guidelines recommend considering an echocardiogram or stress test at 10-year intervals. 29 The NCCN-Survivorship guidelines recommend an echocardiogram within 1 year of completion of treatment, based on anthracycline dose, radiation exposure, and other underlying risk factors, including hypertension, dyslipidemia, diabetes mellitus, family history of cardiomyopathy or other heart diseases, being older than 65 years of age, and a history of smoking, alcoholism, and obesity. 30 However, the anthracycline dose cutoff indicating the need for an echocardiogram is not listed. If the baseline echocardiogram were normal, a provider would reassess the need for further screening based solely on positive responses from the review of systems questionnaire. In summary, all of the guidelines recommend an ECHO screening based on anthracycline and/or radiation doses. However, specific indications and time intervals differ widely, and are not always listed. These results are displayed in Tables 2–4.
Screening for neurocognitive deficits
Methotrexate has been shown to cause neurocognitive deficits in survivors.35,36 The COG LTFU guidelines indicate methotrexate as a neurotoxic agent, and recommend neurocognitive testing upon entry into the long-term follow-up clinic and then periodically as clinically indicated for patients with evidence of impaired educational or vocational progress. None of the NCCN guidelines indicate methotrexate as a neurotoxin or recommend testing based on methotrexate exposure. The NCCN-AYA guideline recommends neurocognitive testing in patients who exhibit symptoms of impaired educational or vocational progress. The NCCN-AYA guidelines state, however, that “severe neurocognitive deficits are uncommon in survivors of AYA cancer … subtle deficits … may occur with higher-dose cranial radiation” (AYAO-B). 27 The NCCN-Site guidelines do not mention neurocognitive screening at all. The NCCN-Survivorship guidelines include three important symptoms for which to watch: difficulty multitasking or paying attention, difficulty remembering things, and slowed thoughts. 30 A positive response to any three of these symptoms directs the provider to continue through a decision tree to evaluate the need for cognitive testing. In summary, COG LTFU guidelines indicate methotrexate as a potential neurotoxin, and recommend screening on entry into follow-up care. The NCCN guidelines do not indicate methotrexate as a potential neurotoxin, and recommend neurocognitive screening only upon a positive review of systems. These results are displayed in Tables 2–4.
Screening for breast cancer
Chest radiation increases the risk for breast cancer. 37 The COG LTFU guidelines have a section related to cancer screening. 25 The COG LTFU guidelines for breast cancer screening recommend mammograms and breast magnetic resonance imaging (MRI) yearly, beginning 8 years after radiation or at 25 years of age, whichever occurs last, when the patient was exposed to more than 20 Gy of chest radiation. The NCCN-AYA guideline has the same recommendation, only for patients who received radiation before 30 years of age. 27 NCCN-Site HL guidelines recommend mammograms and breast MRI yearly, beginning 8–10 years after radiation or at 40 years of age, whichever occurs first, regardless of radiation dose. 29 NCCN-Site guidelines for OS and ALL did not provide malignancy screening.26,28 The NCCN-Survivorship guidelines link to the NCCN Guidelines for Detection, Prevention, and Risk Reduction. They recommend mammogram and breast MRI yearly, beginning 8–10 years after radiation or at 40 years of age, whichever comes first for women aged 25 years or older. For women younger than 25 years old who have received prior thoracic radiation, the panel recommends breast awareness, counseling, and breast exam starting 8–10 years after radiation therapy. In summary, the majority of the guidelines recommend mammogram and breast MRI screening for chest radiation exposure. However, the specific radiation doses and time intervals differ among the COG LFTU and the NCCN documents. These results are displayed in Tables 2–4.
Level of evidence used for guideline recommendations
In the COG LTFU guidelines, screening for cardiac toxicity, neurocognitive deficits, and breast cancer all received a category 1 score. A category 1 score was defined as “high-level of evidence” derived from high-quality case control or cohort studies. In the NCCN guidelines, screening for these same late effects all received a category 2A score or higher. A category 2A score was based upon lower-level evidence with a uniform NCCN consensus that the intervention was appropriate.
Discussion
The aim of this study was to determine how an AYA patient, now 5 years from cancer directed therapy, would be cared for in long-term follow-up. In so doing, the difficulties facing clinicians creating SCPs for AYA cancer survivors were illuminated. While many guidelines exist, it is not always clear which guidelines to use, especially when following AYAs, a group that crosses the pediatric and adult spectrum. As seen in Figure 1, the guidelines were difficult to navigate. There was uncertainty as to which to access first, and which to reference when discrepancies arose. When applied literally and compared next to one another, as seen in Tables 2–4, the guidelines differ on the link between treatment exposures and late effects, the screening test to be used, and the time interval of the test. When examined globally, the documents disagree on which patients are at risk for late effects. COG LTFU deems every patient with a treatment exposure as at risk for late effects, whereas the NCCN-AYA screens high-risk patients who received higher doses of chemotherapy and/or radiation, NCCN-Site provides late effects surveillance for only HL, and the NCCN-Survivorship guidelines define those with a positive review of systems combined with other health risk factors as at risk for late effects. Finally, the guidelines were cumbersome to use. This has significant implications for the long-term follow-up care that an AYA will receive.
The most significant problem was the discordance among documents. One reason for this is the discrepancy between evidence scoring for guideline recommendations. The COG LTFU and NCCN committees disagree on the strength of the evidence for cardiac screening, neurocognitive screening, and breast cancer screening. Perhaps this is because much of the research on late effects is retrospective and cross-sectional. Patient-reported retrospective data does not capture asymptomatic patients. Many patients with late effects, including cardiomyopathy, kidney disease, and breast cancer, can be asymptomatic and unaware of the problem unless screened. However, current prospective data also has their limitations. Prospective studies, such as the St. Jude Lifetime Cohort Study, enroll patients who are 10-year survivors. At this point, many patients already have at least one chronic health condition. 6 A lack of early, prospective data results in a lack of knowledge on the timing of late effects post-treatment. Finally, evidence is just starting to develop on which subgroups within a treatment exposure are at higher risk for certain late effects.38,39
Lastly, it is important to recognize that differences in guidelines may result from perspective differences between COG, a pediatric organization, and NCCN, which deals with a primarily adult population. Often, survivorship care is more prevalent in pediatrics because patients stay with their oncologist longer than adults do, who typically return more quickly to their PCPs. Additionally, late effects of treatment seen in children may be more salient to a pediatrician, whereas an adult provider may not recognize the late effect as attributable to treatment because of competing risk. Moreover, pediatricians may consider their patients to have a greater absolute risk from late effects, prompting pediatricians to perform more screening compared with their adult counterparts.
In summary, there are major discrepancies among the four sets of guidelines. Until a comprehensive AYA-related cancer survivorship guideline for long-term follow-up care is developed, the authors recommend that clinicians reference the COG guidelines. The COG guidelines are the most comprehensive and are referenced by the NCCN guidelines for surveillance recommendations. The current findings support the call for harmonization among guidelines. Further work is necessary to develop a comprehensive AYA-related cancer survivorship guideline for long-term follow-up care. Guidelines need to be easy to use and supported by both pediatric and adult providers in order to ensure strong implementation and adherence. To do this, strong evidence is needed to support late effects surveillance. There are two specific ways that this can be accomplished. The first is a new model of survivorship care that provides the patient with a SCP and surveillance immediately at the end of active treatment, rather than waiting for 2–5 years post-therapy. 40 The second is development of a database utilized by a large number of oncology programs. This database would allow physicians to enter the cumulative doses of chemotherapy and radiation immediately at the end of therapy and then subsequently the late effects that develop on a yearly interval. This database would foster prospective research evaluating the timing of late effects, groups at highest risk, and unknown late effects of new targeted therapy agents. It would also provide the evidence to modify guidelines further based on current treatment protocols. Over time, new evidence will inform us on the appropriate amount of screening for each cancer survivor based on the patient's cancer history and treatment exposure.
Footnotes
Acknowledgment
We would like to thank Ruth Ann Weidner for taking the time to review our manuscript.
Author Disclosure Statement
No competing financial interests exist.