
Abstract
Purpose:
There is growing evidence about the extent that cancer in adolescents and young adults (AYAs) can interrupt normal developmental trajectories, which places the onus on cancer services to buffer these impacts. This article reports the protocol of a four-stage study that aimed to establish how well Australian cancer treatment services are providing youth-friendly cancer care, that is, quality care that best meets young people's needs. The overall goal of this study is to develop an evidence-informed model of cancer care for this age group.
Methods:
Eligible patients were 15–25 years old and 6–24 months from a cancer diagnosis, and a nominated carer. Stage 1 consisted of in-depth, semi-structured interviews. Qualitative analysis identified the major domains affected by cancer. Stage 2 was the development of a survey tool for AYA and parents to measure these domains, compiled from validated instruments of: psychological distress; post-traumatic growth; quality of life; social support; quality of services, information, and needs; physical, psychological, and social needs; self-management; and experience of care, as well as questions covering additional domains (e.g., fertility preservation). Stage 3 was a national survey of AYAs and parents. This information will inform the development of a program model, to be refined by stakeholder consultation in Stage 4.
Conclusion:
Analysis of these data will inform how well cancer services meet the needs of AYAs and their parents around clinical services and psychosocial supports, the physical environment, and information, with the ultimate goal of informing a program model of AYA cancer care.
C
The experience of cancer can interrupt normal trajectories around family relationships, as treatment typically requires intense support at a time when greater autonomy and independence from family is anticipated. 5 The physical effects of cancer treatment such as body scars, hair loss, weight change, and threats to future fertility can affect body image, self-esteem, and identity.6,7 Existing friendships are harder to sustain, while opportunities to form new relationships that are developmentally characterized by greater intimacy may be compromised. 5 So too protracted cancer treatment, including of late effects, challenges financial independence through disruptions to normative transitions from education to employment.3,8 In addition, the challenge of living with uncertainty around cancer relapse and premature death coincides with a life stage characterized by a high burden of mental disorder.9,10
In contrast to major improvements in cancer survival in younger children and older adults, there has not been the same progress in AYA cancer survival.11,12 This has been attributed to many factors, including cancer types and under-representation of AYAs in clinical trials.11–13 It is also apparent that AYAs with cancer have suboptimal levels of psychosocial well-being, 14 unmet needs for information,14,15 and lack access to peer support.16,17 These factors might reduce engagement with treatment regimens, resulting in the potential for reduced intensity and reduced effectiveness of cancer treatment.9,11,13,18
Notwithstanding the potential for cancer and its treatment to disrupt virtually every aspect of AYA development, an important question relates to what extent health services can buffer these negative experiences. This question arises in the context of growing international appreciation that health services will deliver higher-quality care when better orientated to the developmental needs of AYAs, a concept referred to by the World Health Organization (WHO) as youth-friendly or youth responsive healthcare.19–23
Given the importance of social support in buffering the cancer experience and the extent to which families support young children with cancer, 24 further questions also relate to the extent and nature of support provided by parents when AYAs develop cancer. Australia has experienced a number of reforms around AYA cancer care.25,26 However, surprisingly little evaluation of AYA cancer services or patient and family experiences of AYA cancer care is available to shape future service models. 27 Internationally, with some notable exceptions from recent U.S. studies,17,28,29 there is still a major gap in patient-reported needs and experiences of care across the range of domains pertinent to AYAs. And while parent perspectives have been prominent within the pediatric cancer literature, 24 they have been remarkably absent from the AYA literature, whether in relation to the impact of AYA cancer on parents, parent reports of unmet need, or parent and family well-being.
Adolescence is defined by the WHO as starting at 10 years of age and finishing at 19 years of age, which is consistent with downward trends in the age of onset of puberty. 22 Increasing attention is being paid to the 10–24-year-old age span of adolescence and young adulthood due to upward trends in the ages at which the key social role transitions from adolescence into adulthood are now achieved (e.g., completion of education) and the appreciation that neurocognitive maturation continues at least to the mid-20s. 22 Cancer service evaluation is complicated by variable age criteria for both clinical services and research. 30 In the United States, the age span of AYA cancer extends up to 39 years,14,30 while in the United Kingdom, clinical services typically span from 13 to 26 years. 31 In Australia, Youth Cancer Services are now designated from 15 to 25 years. 32 As the developmental trajectories and service needs of cancer patients in their late 20s to 30s may differ significantly from younger adolescents, there may be benefits in examining more developmentally homogenous age groups.
Given the extent that social determinants influence the experience of AYAs with cancer and their families, the socio-ecological framework that that has been widely used in pediatric, family-centered oncology care 33 provides a useful model for conceptualizing the AYA within the context of family, peers, and the broader enabling and protective social subsystems. The extent that critical social role transitions in adolescence and young adulthood (such as the passage from education to employment) can be disrupted by cancer also highlights the importance of considering these wider life outcomes within a systemic framework, in addition to the usual targets of supportive care interventions such as emotional distress. 22
The objective of this study was to establish the degree to which Australian cancer treatment services are meeting AYAs' and parents' needs, with the intent of using this information to shape the development of future services for young people with cancer and their parents. Consistent with Australian Youth Cancer Service norms, the age span of interest is defined as 15–25 years, which also enables consideration of a model of care that is appropriate for pediatric, adult, and AYA-specific services.
The goal of this article is to overview the four stages of the study and the major methods of each stage. The study was conducted by a multidisciplinary research team with expertise in clinical, public health, and health service research, medical oncology (pediatric, AYA, and adult), adolescent health and medicine, psychology, sociology, and health policy. An international advisory committee and the Victoria and Tasmanian AYA cancer committee informed the study.
Methods
This was a four-stage study (see Fig. 1). Stage 1 consisted of in-depth semi-structured interviews with young people, parents, and carers. Stage 2 involved development of an AYA cancer survey instrument and an accompanying parent survey. Stage 3 was a national Australian survey of AYAs with cancer and their parents. Stage 4 will be the development of a program model to be undertaken in concert with stakeholder consultation.

Study design.
Stage 1: Qualitative research study
Eligibility criteria
AYAs were eligible if they: (1) had a diagnosis of new or recurrent cancer between 15 and 25 years old; (2) were diagnosed between September 2010 and December 2012; and (3) were 6–24 months from diagnosis at recruitment. The perspective of carers was sought from the parent or carer who had most supported the AYA since diagnosis.
Recruitment strategy
Informed by all chief investigators and associate investigators, six services were selected that provide specialist cancer care to AYAs within pediatric, adult, and AYA services (see Table 1). These were purposefully selected, as they were at different stages of AYA service development, spanned different states, and ensured coverage of urban, regional, and rural settings.
AYA, adolescent and young adult.
Recruitment of AYAs and carers
Ethics approval was obtained at each site to conduct in-depth telephone interviews with AYAs and a nominated carer. Local staff identified AYA meeting eligibility criteria. The research team then contacted potential participants, confirmed eligibility, and, after obtaining verbal consent, sent written consent forms to complete before the interview. At the adult and AYA sites, participants were asked to provide the contact details of the carer who had been most involved in their care. This person was separately contacted and could be interviewed even if the AYA themselves did not participate. At the three pediatric services, parents were the primary contact. The choice of carer was similarly prioritized as the person who had been most involved.
Procedures
Telephone interviews were conducted separately with AYA and parents, digitally recorded, and transcribed. The interviews were undertaken by two experienced researchers who, using an interview guide (available on request), first asked broad, open-ended questions to encourage the participant's narrative, and then used specific prompts around key areas of interest. These prompts (specific to the AYA or parent or carer) related to: the psychosocial impacts for AYA patients, and the factors (e.g., disease/treatment, intrapersonal, and environmental) that affect these outcomes; the psychosocial impacts for parents or carers, and the factors (e.g., disease/treatment, intrapersonal, and environmental) that affect these outcomes; the met and unmet informational and psychosocial needs that AYA patients and parents or carers identify about current cancer services; and the preferences of AYA patients and parents or carers about accessing information and psychosocial supports.
Sample
Interviews were completed with 60 AYA patients and 60 parents and carers (44 mothers, 8 fathers, and 8 carers [all partners]), as shown in Table 1. Thirteen AYAs (3 females) declined to participate (response rate 82%). Six parents declined (response rate 91%).
Analysis
Preliminary content and thematic analyses were conducted by the senior qualitative researcher (S.E.D.) to establish key codes and themes within the data. The primary intent of these analyses was to inform the content of the national survey. Transcripts of interviews were then distributed to the research team for thematic analysis. Each transcript was independently reviewed by two investigators. Thus, three independent assessments of each transcript were produced. This process also identified additional questions and themes that were iteratively explored in subsequent interviews. Identification of key themes was reached by consensus between the three assessors, supported by the team as a group that then identified the priority themes using a series of workshops. Assisted by NVIVO v10 software, 34 detailed qualitative analysis will be performed at a later date, with priority given to understanding how support services and social and physical environments and information best meet AYA and parent needs.
Stage 2: Development of AYA and parent surveys
Survey content
The key themes that emerged from the qualitative interviews informed the content of the quantitative survey and the measures employed. Priority themes were the impact of cancer on relationships, disruption to normal AYA developmental transitions, psychological distress, and unmet needs for many services and supports. For AYAs, the key domains within these themes related to the disruption of family life and the extent of reliance on parents for support, the impact of cancer on well-being and the challenges of accessing various psychosocial supports, the impact of cancer on education and employment, the financial impost of the cancer journey, the impact on peer relationships and the value of informal peer support, challenges around fertility preservation, and widespread challenges around age appropriate services, including the physical environment and information needs. These domains were echoed by parents and carers. The extent of the impact on parents was a critical finding, including disruption to family life, parent well-being, and parent employment. The majority (85%) of carers identified by AYA were parents (even for those managed in adult services). This, together with the evidence that non-parent carers (all romantic partners) identified slightly different challenges, informed the decision to specifically develop a parent version of the survey.
Survey measures
Priority was given to instruments with established reliability and validity and to previously published questionnaires used in AYA cancer research. The study measures, summarized in Table 2, include validated measures of psychological distress, post-traumatic growth, quality of life, social support, quality of services, information, and needs, physical, psychological, and social needs, self-management, and experience of care. Additional questions were specifically developed for some areas, such as fertility preservation. The AYA survey comprised 70 questions in total and took approximately 50 minutes to complete. The parent version paralleled the AYA version. It compromised 79 questions and took approximately 50 minutes to complete.
Measures were slightly modified for an Australian healthcare context, and adapted parent versions were utilized to enable comparisons between AYA and parent surveys.
Stage 3: National survey of AYAs with cancer and their parents
Eligibility criteria
AYAs were eligible if they: (1) were 15–25 years old with a cancer diagnosis made between September 2010 and December 2012; (2) had a first diagnosis of cancer, new diagnosis of recurrence or relapse of cancer, or diagnosis of a second cancer where the first cancer had been previously treated; and (3) were 6–24 months from diagnosis. Exclusion criteria were: (1) poor literacy, cognitive deficit, or being too unwell to complete the survey; and (2) Stage 1 and 2 melanoma (as these are generally managed in non-specialist settings and involve limited disruption to social and educational trajectories relative to other cancer diagnoses). 35 The parent who provided most support to the AYA was sought to interview (carer perspectives were not surveyed).
Recruitment strategy
While planning this study, another Australian study of 14–19 year olds reported a response rate of only 7.8% using cancer registries for recruitment. 36 Delays in cancer registration, together with that low response rate, influenced the decision to recruit from leading cancer care sites. Twenty-one public hospitals were identified that provide the majority of AYA cancer treatment in each state, 17 of which agreed to participate (see Fig. 2). Recruitment was also undertaken through a national network of peer support groups for AYAs with cancer run by CanTeen.
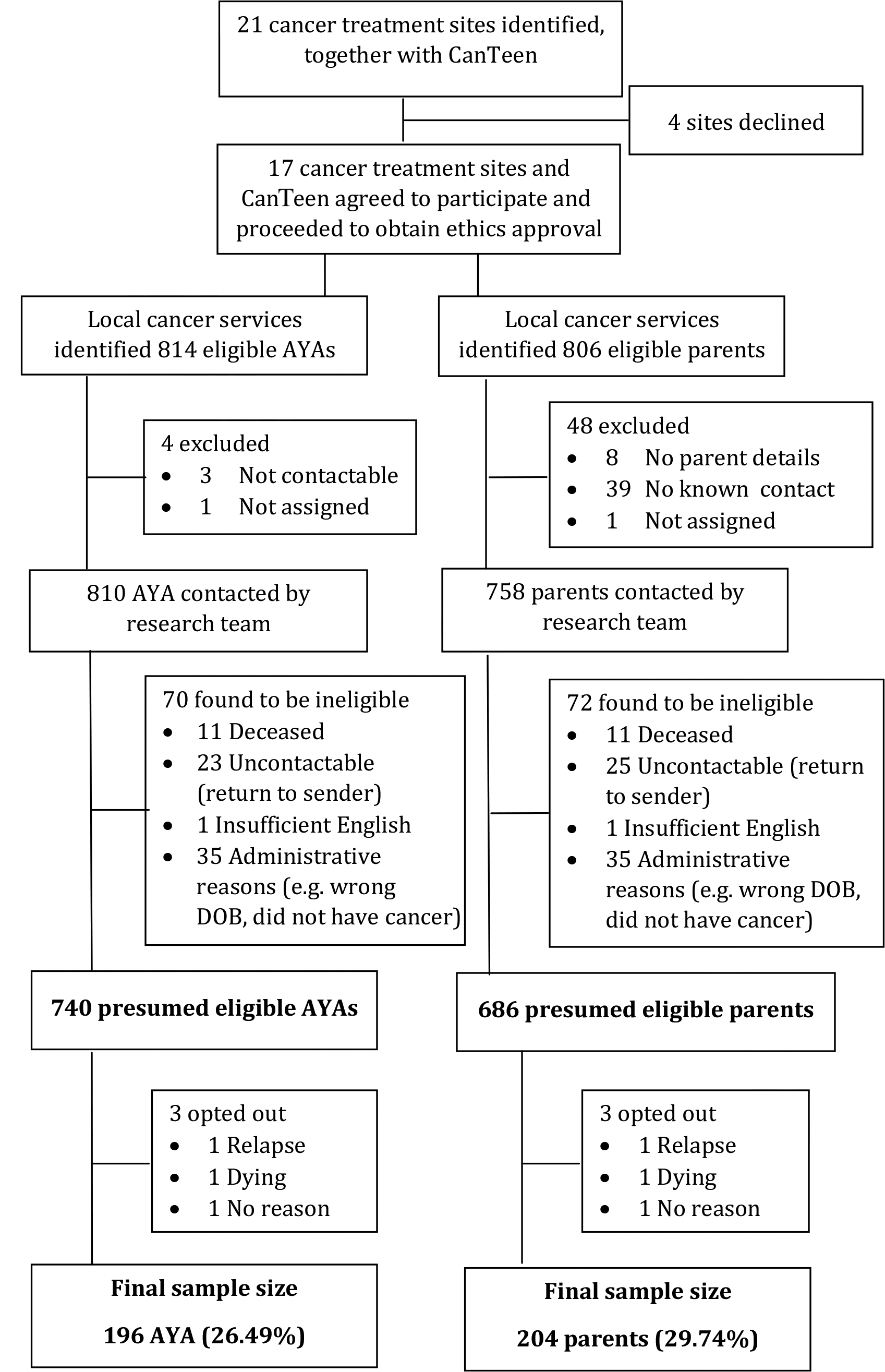
Flowchart of recruitment for national survey (Stage 3).
Recruitment of AYAs and parents
Ethics approval was obtained from 17 hospitals in five states to survey AYAs treated for cancer and their parents. Each participating hospital also required separate research governance approvals. Approval was also obtained from the ethics committee of CanTeen.
Procedure
Potentially eligible participants were identified by local staff and sent a survey package from their cancer service. AYA and parent versions were prepared in separate envelopes that contained: (1) a letter of explanation from the senior clinician at the main cancer center; (2) a copy of the survey with a prepaid return envelope to the research team; (3) an online link to complete the survey via the internet; and (4) information about telephone completion.
Parent information was available at 10 sites. When the patient was younger than 18 years of age, the AYA and parent packages were mailed in one envelope addressed to the parent. The parent information letter requested that the parent pass the survey package on to the AYA for completion if they were willing for their son or daughter to be involved. When the AYA was older than 18, separate survey packages were mailed directly to them and to their parent. Parent contact details were generally not available at seven adult hospitals, including those with emerging AYA services, or from the CanTeen database. In these instances, packages were directly mailed to the AYA. In addition to the parent survey, a letter asked the AYA to pass the survey on to the parent who had most cared for them during their cancer treatment.
Written consent was required from AYAs and parents using a tick-box question at the start of the survey. Follow-up procedures varied slightly according to local ethics requirements. At the majority of sites (n = 15), when opt-out notification was not returned within 3 weeks, contact details were provided to research staff who undertook follow-up activities. AYAs and parents were sent a further survey package, and up to five telephone calls were made over several weeks. CanTeen staff sent one email reminder to potential AYA participants, with a link to the online survey. Reminders were unable to be sent to parents recruited through CanTeen due to the absence of contact information.
AYA and parent sample
Figure 2 shows the number of AYAs and parents sent surveys. Surveys were returned from 196 eligible AYAs and 204 eligible parents, of whom 126 were matched familial pairs or dyads. No consistent information is available on non-responders.
Sample characteristics
Table 3 summarizes the demographic characteristics of the AYA sample. The mean age at diagnosis was 19.9 years (21.6 years at time of survey). Sixty-four percent of participants lived in metropolitan cities, and 49% resided in Victoria. Almost three-quarters of the sample (72%) lived with their parents, or 91% of 15–19 year olds and 57% of 20–25 year olds. Fifty percent were studying part or full time, 47% were working part or full time, and 17% were unemployed.
Percentages use total number of responses as denominator (otherwise n = 196 is used as the denominator).
Totals are for number of responses due to a “tick all that apply” question type.
Table 4 summarizes the cancer and treatment characteristics of the AYA sample. The most common cancer types or groups were malignant hematological conditions (leukemias), Hodgkin's lymphoma, and sarcoma. Thirty-nine percent of respondents reported spending more than 1 month as an in-patient. Eighty-three percent of respondents underwent chemotherapy. Sixteen percent had experienced relapse of cancer. The majority (81%) were off-treatment. The main cancer treatment sites, shown in Table 5, were based in capital cities or large regional cities or towns. The majority (86%) of these sites were adult hospitals.
Percentages use total number of responses as denominator (otherwise n = 196 is used as the denominator).
Totals are for number of responses due to a “tick all that apply” question type.
Hospitals in Tasmania, Australian Capital Territory and Northern Territory were not invited to participate as the great majority of AYAs with cancer in these jurisdictions access tertiary treatment through cancer centers in other states.
Ethics approval was obtained from this site but data collection did not proceed.
One survey was returned which did not specify the main cancer site. While added here, the data were not analyzed further.
Characteristics of the parent sample
The demographic details of the 204 parent respondents, largely mothers, are shown in Table 6. Three-quarters lived with their child or children, and two-thirds also lived with their partner or spouse. Approximately 70% of parents were born in Australia. Sixty percent had obtained a tertiary level of education. Sixty percent lived in metropolitan areas.
Percentages use total number of responses as denominator.
Totals are for number of responses due to a “tick all that apply” question type.
Data analysis
De-identified hardcopy, online, and telephone survey responses were entered into the research database software RedCap™. 37 Each AYA and parent entry had an individual participant code and a family code to enable familial pairs to be linked for analysis. Data will be exported from RedCap™ to STATA v13 quantitative software for analysis. 38 Descriptive statistics will be calculated for individual survey questions. This initial analysis will provide prevalence data for AYA and parent met and unmet informational and clinical service needs, level of distress (depression, anxiety, and post-traumatic stress symptoms), quality of life, social support and impact of cancer upon practical, educational, vocational, and family relationships. With respect to experience of care data, descriptive statistics will be used to examine self-reported informational and clinical needs and to identify areas of improvement for services. Bivariate analysis of the effects of independent variables (e.g., sex, age at diagnosis, hospital type) on healthcare experiences will be undertaken using chi-square and Fisher's exact tests. Linear regression models will be utilized to examine associations between demographic factors (e.g., age, sex), illness (e.g., treatment intensity, time in hospital), and psychosocial variables (e.g., social support, other life stressors) on outcome measures. Outcome measures will include post-traumatic stress symptoms, distress (anxiety and depression), and quality of life. Regression models will be separately conducted for AYAs and parents. Univariate analyses will be conducted for each of the independent variables; standard multiple regressions will then be conducted utilizing the significant predictor variables (p < 0.05) from the univariate analyses. Analysis of data from family dyads (n = 126) will also be undertaken. Pearson's coefficient and paired sample t-tests will be utilized to examine associations between family dyads. Regression modeling will be utilized to examine outcomes for family dyad data, and general estimating equations will be utilized to correct for the correlation between parent and AYA data.
Stage 4: Model development and stakeholder consultation
In response to the identified needs and experiences of AYAs and parents, the research group will engage with various stakeholders, including AYAs, parents and carers, healthcare professionals, government representatives, and philanthropic groups to refine a model of care that can deliver an appropriate level of psychosocial and practical support to AYAs with cancer. This will involve: developing a model of cancer care based on the elements of need identified by AYAs and parents; conducting a series of consultation forums with stakeholders around Australia with the goal of seeking feedback, especially about the local feasibility and utility of the model; and refining the model, documenting the guiding principles that shaped the best-practice model.
A qualitative methodology will be used for this stage; focus groups, interviews, and stakeholder consultations will be audio recorded and transcribed for further analysis. NVIVO v10 will be utilized to undertake thematic analysis of consultations that will be used to inform the final model of care.
Discussion
This four-stage study of AYAs with cancer and their parents will provide rich data to help us to understand better the impact and experience of cancer on 15–25-year-old Australians and their parents. Given that the domains that were included in the national survey (Stage 3) arose from a qualitative study of AYA and carers (Stage 1), a strength of the study is the extent to which it is embedded in the experiences of consumers. The relatively large sample size of AYA within a tightly defined age span is an additional strength of both the qualitative and quantitative stages, given that this period spans an especially dynamic period of human development. This study will provide the opportunity to explore the perspectives of parents, who have been largely missing from AYA research. The high proportion of AYAs living at home reinforces the significance of parent perspectives, which will be augmented by analysis of the 126 family dyads within Stage 3.
High participation rates were seen in Stage 1. In Stage 3, the number of potential participants identified across national survey sites was less than predicted. To some extent, this is explained by the lack of participation of four large public hospitals, including a children's hospital from NSW and West Australia and a large adult hospital in NSW. While recruitment of young people for any research is challenging, 39 additional difficulties resulted from the inadequacy of a number of local department and hospital databases. For example, the information was inaccurate (e.g., diagnosis) at some sites, which meant that surveys were sent to people without cancer. At other sites, hospital databases did not allow searches by date of diagnosis, resulting in all appropriately aged patients with an outpatient appointment during the study period being sent a survey, regardless of diagnosis. Due to lack of parent contact data, AYAs at eight sites were asked to forward the survey to their parents. The number of eligible AYAs was considered as the parent denominator, but it is not known how many of these parents received a survey. Thus, as with the AYA survey, the denominator is likely to be an overestimate, but it was not possible to obtain a more accurate figure. Sites with clinic coordinators generally had access to more accurate, detailed, and up-to-date databases. This suggests that investing in these roles, as well as clinical databases, should be considered core infrastructure for clinical research. Introduction of electronic medical records can also be expected to increase clinical accuracy and reduce the burden of research. Ensuring that adult sites routinely record carer contact data, as occurred in pediatric sites, would aid recruitment in future studies of this type.
This study will enable exploration of many key aspects related to the impact of cancer diagnosis and treatment and the experiences of care for young people and their families. The use of validated measures will facilitate descriptive analyses of psychological distress, quality of life, social support, psychosocial needs, and self-management that will inform the model of care in relationship to the types of services that might be anticipated to be required. A wealth of wider data will also inform the model of care that will be developed in Stage 4 of this research for AYAs and parents. This includes patient experience data, where measurement of both met and unmet need will help prioritize AYA and parent needs. The national survey will also provide rich data about fertility preservation, including aspects of professional communication, prevalence of uptake, and barriers to use, which will be augmented by the depth of qualitative data about fertility, sexuality, and body-image disturbance. Due to cross-sectional data, it will not be possible to attribute causality of the quantitative findings to cancer. However, triangulation of the qualitative and quantitative data will provide a robust, comprehensive, and rich resource to inform a model of care for this group.
In conclusion, this four-stage project will enable us to understand better the experiences and service needs of a tightly defined age range of AYAs with cancer and their carers. The mixed methods provide rich qualitative data, along with quantitative data from a large national survey using validated measures. This novel information will be used to identify the major elements required within a model of care that has the intent of buffering the highly disruptive aspects of a cancer diagnosis and its treatment on AYA and their parents.
Footnotes
Acknowledgments
We wish to acknowledge the generosity of the Australian young people and their families who participated in this study, as well as the members of the Victorian and Tasmanian Adolescent and Young Adult Cancer Advisory Committee for their many contributions. Ms. Tarnya Hotchkin is warmly acknowledged for her contribution to data collection, as are the staff at each clinical site for their generous assistance with recruitment. Ms. Sharon Bowering, Dr Pandora Patterson, Associate Professor Wayne Nicholls, and Professor David Thomas are gratefully acknowledged for their contributions, as are the members of the international advisory committee. This project was funded from 2011–2013 by a grant (APP1010977) from Cancer Australia in association with Beyondblue and CanTeen through the Priority-driven Collaborative Cancer Research Scheme to support research that reduces the impact of cancer on the community and improves outcomes for people affected by cancer. Additional funding has been gratefully received from the ONTrac at Peter Mac Victorian Adolescent and Young Adult Cancer Service, the Victorian Department of Health (Cancer Strategy and Planning, Department of Health), the Royal Children's Hospital Foundation and Redkite. Dr. McCarthy is funded via a Murdoch Childrens Research Institute Career Development Award. The Murdoch Childrens Research Institute is supported by the Victorian Government's Operational Infrastructure Support Program.
Author Disclosure Statement
No competing financial interests exist.